
Discovering Expected Activities in Medical Context Scientific Databases
Daniela D’Auria and Fabio Persia
Dip. di Ingegneria Elettrica e Tecnologie dell’Informazione, University of Naples ”Federico II”, Naples, Italy
Keywords:
Activity Detection, Scientific Databases, Cricothyrotomy Simulator, Medical Simulator.
Abstract:
Reasoning with temporal data has attracted the attention of many researchers from different backgrounds
including artificial intelligence, database management, computational linguistics and biomedical informatics.
More specifically, activity detection is a very important problem in a wide variety of application domains such
as video surveillance, cyber security, fault detection, but also clinical research. Thus, in this paper we present a
prototype architecture designed and developed for activity detection in the medical context. In more detail, we
first acquire data in real time from a cricothyrotomy simulator, when used by medical doctors, then we store
the acquired data into a scientific database and finally we use an Activity Detection Engine for finding expected
activities, corresponding to specific performances obtained by the medical doctors when using the simulator.
Some preliminary experiments using real data show the approach efficiency and effectiveness. Eventually, we
also received positive feedbacks by the medical personnel who used our prototype.
1 INTRODUCTION
Reasoning techniques are very essential in many ap-
plication domains, such as video surveillance, cyber
security, fault detection, fraud detection and in clin-
ical domain, as well. In all cases, temporal infor-
mation is crucial. For instance, for what the clinical
research concerns, investigating disease progression
is practical only by definition of a time line; other-
wise, possible causes of a clinical condition have to
be found by referring to a patient’s past clinical his-
tory. In (Zhou and Hripcsak, 2007), the basic con-
cepts of temporal representation in the medical do-
main have been described in order to include: cat-
egory of time (natural, conventional, logical), struc-
ture of time (line, branch, circular, parallel), instant
of time vs. interval, and, absolute time vs. relative
time. Anyway, this is still a challenging and active
subject of research. The main goal of (Safari and
Patrick, 2013) consists in creating a special purpose
query language for clinical data analytics (CliniDAL)
to place in any clinical information system (CIS) and
answer any answerable question from the CIS. In
more detail, a category scheme of five classes of in-
creasing complexity, including point-of-care retrieval
queries, descriptive statistics, statistical hypothesis
testing, complex hypotheses of scientific studies and
semantic record retrieval have been designed to cap-
ture the scope encompassed by CliniDAL’s objectives
(Patrick and Cheng.Y., 2013). However, a review of
temporal query languages reflects that the importance
of time has led to the development of custom temporal
management solutions, which are mostly built to ex-
tend relational database systems (for instance, T4SQL
(Combi et al., 2007)). Many efforts in the relational
database field have been conducted for developing ex-
pressive temporal query languages; nevertheless, they
still suffer from two issues: firstly, they are only ap-
plicable to structural relational databases; secondly, it
is difficult for hospital staff with poor IT skills to ap-
ply them. On the other hand, in most ontology based
approaches composing queries can be difficult due to
a complex underlying model representation and lack
of expressivity.
In other contexts, such as video surveillance, cy-
ber security and fault detection, the reasoning tech-
niques using temporal information are broadly used
for activity detection. Thus, several researchers have
studied how to search for specifically defined patterns
of normal/abnormal activities (Hongeng and Neva-
tia, 2001). Vaswani et al. (Vaswani et al., 2005)
study how HMMs can be used to recognize complex
activities, while Brand et al. (Brand et al., 1997)
and Oliver et al. (Oliver et al., 2002) use coupled
HMMs. Hamid et al. (Hamid et al., 2003) use Dy-
namic Bayesian networks (DBNs) to capture causal
relationships between observations and hidden states.
Albanese et al. (Albanese et al., 2007) developed a
stochastic automaton-based language to detect activ-
ities in video, while Cuntoor et al. (Cuntoor et al.,
446
D’Auria D. and Persia F..
Discovering Expected Activities in Medical Context Scientific Databases.
DOI: 10.5220/0005146504460453
In Proceedings of 3rd International Conference on Data Management Technologies and Applications (KomIS-2014), pages 446-453
ISBN: 978-989-758-035-2
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

2008) presented an HMM-based algorithm. In con-
trast, (Albanese et al., 2014; Albanese et al., 2011)
start with a set A of activity models (corresponding
to innocuous/dangerous activities) and find observa-
tion sequences that are not sufficiently explained by
the models in A. Such unexplained sequences reflect
activity occurrences that differ from the application’s
expectations.
Other relevant works exploiting an events se-
quence definition are (Boselli et al., 2014a) and
(Boselli et al., 2014b): in particular, (Boselli et al.,
2014a) automatically identify cleansing activities,
namely a sequence of actions able to cleanse a dirty
dataset, which today are often developed manually by
domain-experts, while (Boselli et al., 2014b) describe
how a model based cleansing framework is extended
to address integration activities as well.
In this paper, we present a prototype architecture
designed and developed for activity detection in the
medical context. The context of use is very con-
crete and important, as it is represented by a cricothy-
rotomy simulator built by the BioRobotics Labora-
tory of the University of Washington, Seattle (USA)
(White et al., 2014; White et al., 2013; White et al.,
2012a). Such a simulator is very relevant in the surgi-
cal robotic field, as it is very useful for helping med-
ical doctors when they are performing a cricothyro-
tomy. Our main aim consists in making the medical
doctors able to have a very fast feedback about their
performances when using the simulator, that is very
essential for this kind of applications. In order to do
that, we first acquire data in real time from the simu-
lator, when used by medical doctors, then we store the
acquired data into a scientific database and finally we
use an Activity Detection Engine for finding expected
activities, corresponding to specific performances ob-
tained by the medical doctors when using the sim-
ulator. Thus, we model the expected activities with
stochastic automata (Albanese et al., 2014; Albanese
et al., 2011) and exploit the activity detection algo-
rithms presented by (Albanese et al., 2013), as tem-
poral information is essential.
The paper is organized as in the following. Sec-
tion 2 briefly describes the context of use of our pro-
totype architecture, which is the cricothyrotomy simu-
lator designed by the University of Washington, Seat-
tle. Section 3 shows the model used for activity detec-
tion, while Section 4 describes the architecture of the
developed prototype. Section 5 presents some prelim-
inary experiments using real data. Eventually, Section
6 discusses some conclusions and future work.
2 CONTEXT OF USE: A
CRICOTHYROTOMY
SIMULATOR
Modern airway protocols involve many techniques
to restore ventilation including bag-mask-ventilation,
placement of a laryngeal mask airway, and intubation
with or without videolaryngoscope. In cases where
conservative measures fail or when contraindicated,
the only methods remaining to re-establish ventilation
may be surgical. In the developing world where de-
vices such as the videolaryngoscope may not be avail-
able, accurate knowledge and training in the creation
of a surgical airway may have a significant impact on
patient outcomes.
A cricothyrotomy is a life-saving procedure per-
formed when an airway cannot be established through
less invasive techniques. Although performing such
a procedure seems relatively straightforward, studies
have shown that those performed in the pre-hospital
setting were mostly unsuccessful (Wang et al., 2011).
A review of 54 emergency cricothyrotomies found
that the majority of the procedures performed in the
field were unsuccessful or resulted in complications
(King et al., 2012). A military team identified gap ar-
eas in the training of cricothyrotomy in emergency sit-
uations; these included lack of anatomical knowledge
including hands on palpation exercises, poor anatomy
in medical mannequins, and non-standard techniques
(Bennett et al., 2011).
Most of the unsuccessful attempts were due to
inaccurate placement, and incorrectly identifying
anatomy. If the anatomy is not properly identified,
it is unlikely that the procedure will be successful.
Further, a large review of emergency airway cases
found that emergency cricothyrotomies performed by
anesthesiologists were successful in only 36% of in-
stances (Cook et al., 2011). Although many reports
suggest that the success rate of surgical airway place-
ment is low, publications from advanced centers with
extensive training for airway protocols including sim-
ulation show that pre-hospital cricothyrotomy success
rates can be as high as 91% (Warner et al., 2009).
Studies such as this suggest that with adequate train-
ing, the success rate of cricothyrotomy can be dramat-
ically improved. Thus, an improved method of train-
ing needs to be provided for this rare, but life-saving
procedure.
For such reasons, the BioRobotics Laboratory
of the University of Washington, Seattle (USA) de-
veloped a low-cost cricothyrotomy simulator (White
et al., 2014; White et al., 2013; White et al., 2012a)
from readily available components that is equipped
with inexpensive sensors. The simulator emphasizes
DiscoveringExpectedActivitiesinMedicalContextScientificDatabases
447
the palpation and the correct identification of anterior
cervical anatomy and has the ability to record the con-
tact location of instruments on the trachea model dur-
ing the full duration of the simulated procedure.
2.1 Simulator Design
The trachea model is disposable and is replaced af-
ter each procedure. To minimize costs, the trachea
is made of cardboard with fixed size and dimension
according to the trachea of an average adult. Foam
strips were cut for the cartilaginous tracheal rings and
were attached on the trachea with appropriate spac-
ing. The thyroid and cricoid cartilages are permanent
parts made of ABS plastic, using a 3D printer. These
components are fixed onto a wooden base, and firmly
support the trachea model. Conductive foils are used
as low-cost sensors to detect six critical landmarks
(identified by A-F letters) that providers might con-
tact during the procedure. The conductive foils cover
landmarks on the trachea model. Only one of these six
landmarks, the cricothyroid membrane itself, is the
correct area to contact and make an opening. Other
landmarks like the posterior tracheal wall and lateral
locations into the tracheoesphageal grooves should be
avoided during the procedure.
The model is fitted with an Arduino Uno micro-
controller board based on the Atmel Atmega 328 mi-
croprocessor with a mounted 8x8 LED matrix-based
display for user interface capability. The microcon-
troller records the contact data of the instruments
(scalpel, tracheal hook, and hemostat) onto the six
conductive foils, as each instrument is wired. Dur-
ing the procedure, when a closed circuit is detected
between the instrument and a patch of foil, the event
is recorded and labeled with the time in milliseconds.
Breaking contact is similarly recorded. Traditional
matrix scanning techniques are used by the microcon-
troller to detect connections between the instruments
and the foil patches. A minimum time (20 millisec-
onds) between contacts was used to debounce the in-
puts to the microcontroller. The resulting data was
later low-pass filtered with a cutoff frequency of 10
Hz in accordance with general human reaction time.
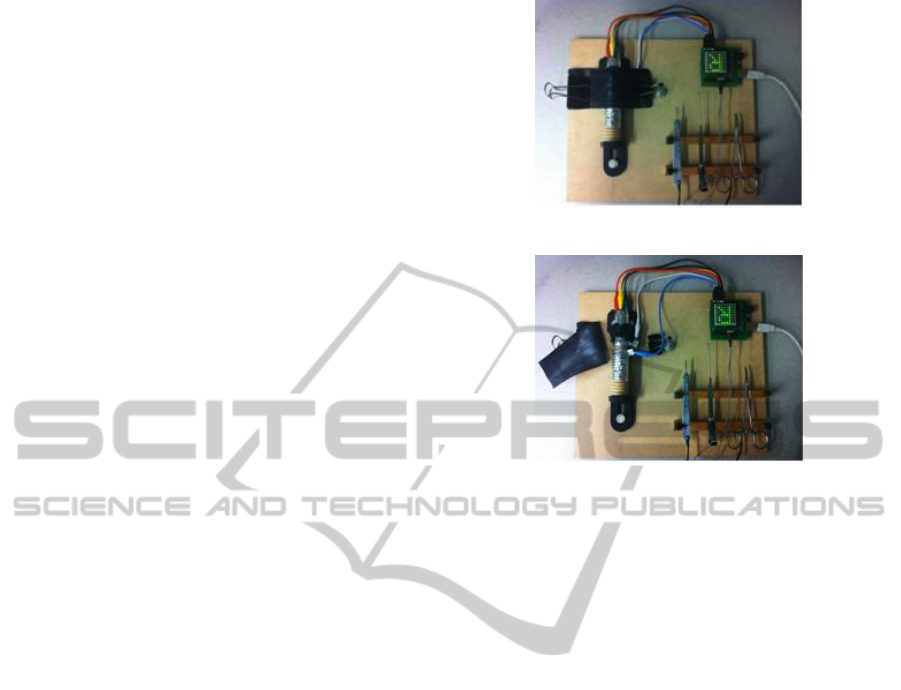
The simulator’s design is shown in Figure 1.
Moreover, the design was optimized for materials
that are low-cost, widely available and simple to as-
semble. The total cost of the simulator was less than
$50, which has a lower price compared to existing
commercial simulators.
(a) Trachea model is covered with in-
ner bicycle tube as human skin.
(b) Six different landmarks repre-
sented by conductive foils and tools
(scalpel, hook and forceps) are con-
nected to microcontroller for data
collection.
Figure 1: Low-cost cricothyrotomy simulator.
2.2 How to Use the Simulator
Medical doctors who want to use the simulator are
firstly forced to watch a video tutorial published by
the New England Journal of Medicine (James and
Pacheco-Fowler, 2008; White et al., 2012b). After
watching the instructional materials, they are allowed
to perform the procedure on the simulator following
the instructions below:
• Step 1: Palpate the cricothyroid membrane. Im-
mobilize the larynx with the non-dominant hand
and perform the procedure with the dominant
hand.
• Step 2: Incise the skin (bicycle inner tube) verti-
cally after palpating the cricothyroid membrane.
• Step 3: Incise the cricothyroid membrane on tra-
chea model horizontally (1 cm length).
• Step 4: Insert the tracheal hook into cricoid carti-
lage.
• Step 5: Insert the hemostat and to expand the air-
way opening vertically and horizontally.
• Step 6: Insert the endotracheal tube.
As these steps were performed, all the data (con-
tact locations on trachea model, instruments informa-
tion, contact duration and total time) were recorded
DATA2014-3rdInternationalConferenceonDataManagementTechnologiesandApplications
448
by the microcontroller; procedures were also video-
recorded for analysis.
Thus, after the description of the used cricothy-
rotomy simulator, the importance of temporal infor-
mation is definitely clear. The following sections de-
scribe how our prototype has been designed and de-
veloped for helping medical doctors when they are us-
ing the simulator.
3 MODELING EXPECTED
ACTIVITIES
This section describes the model that we have defined
in order to derive a formal definition of Expected Ac-
tivity for medical context. We use the temporal proba-
bilistic graph proposed by (Albanese et al., 2014; Al-
banese et al., 2011), so that the elapsed time between
observations also plays a role in defining whether a
sequence of observations constitutes an activity, dif-
ferently from what happens in other models, such as
Hidden Markov Chains. We assume the existence of a
finite set S of action symbols, corresponding to atomic
events that can be detected by the Arduino microcon-
troller board, as described in Section 2.
3.1 Basic Definitions
An Expected Activity is a labeled directed graph A=
(V ,E, δ, ρ) where: (i) V is a finite set of nodes la-
beled with action symbols from S; (ii) E ⊆ V × V is
a set of edges; (iii) δ : E → N
+
associates with each
edge hv
i
,v
j
i an upper bound of time that can elapse
between v
i
and v
j
; (iv) ρ : E → (0,1) is a function that
associates a probability distribution with the outgoing
edges of each node, i.e. ∀v ∈ V
∑
hv,v
0
i∈E
δ(hv, v
0
i) = 1;
(v) there exists an initial node I in the activity defini-
tion, i.e. {v ∈ V | @ v
0
∈ V s.t. hv
0
,vi ∈ E} 6=
/
0 ; (vi)
there exists a final node F in the activity definition,
i.e. {v ∈ V | @ v
0
∈ V s.t. hv,v
0
i ∈ E} 6=
/
0.
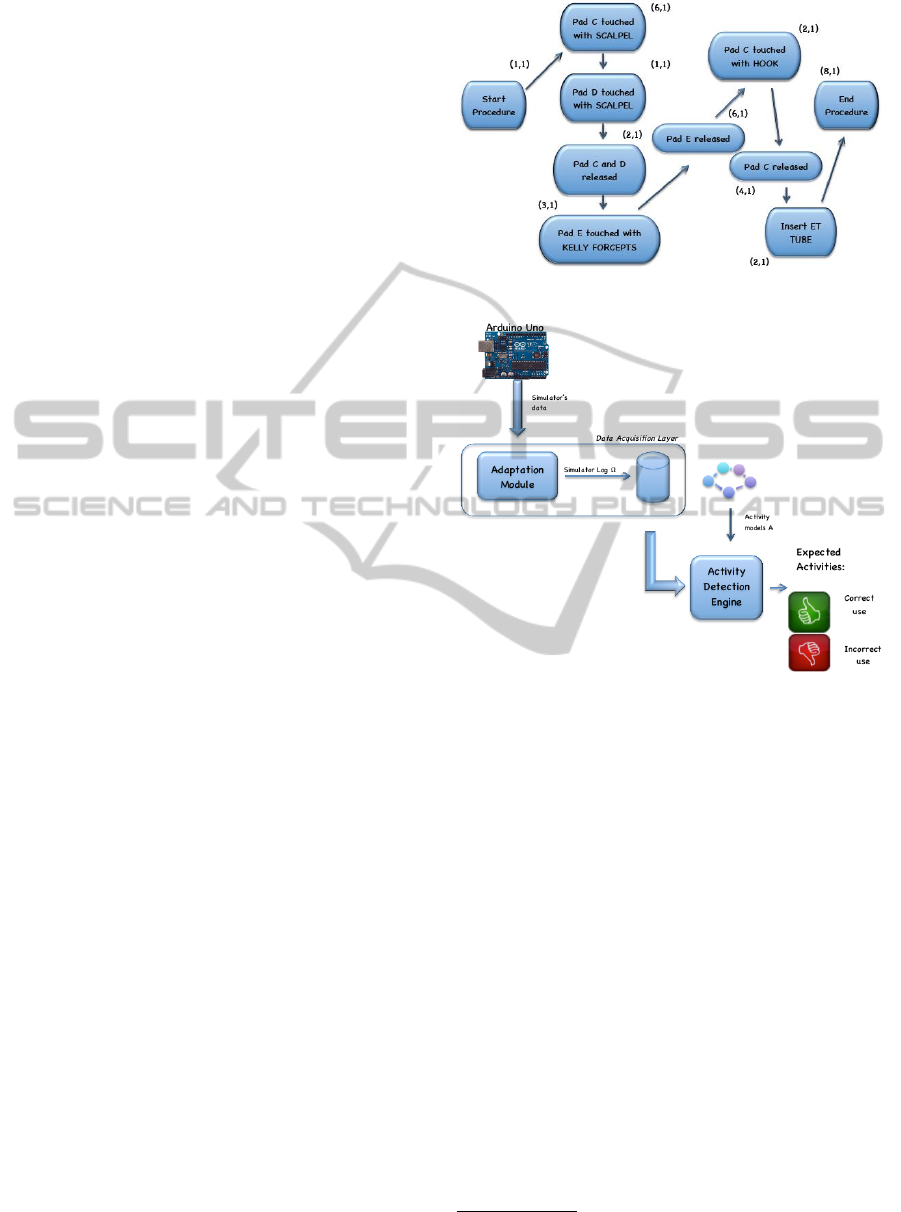
We assume the existence of a finite set S of ac-
tion symbols representing particular interactions (for
instance, Pad C touched with SCALPEL, PAD C re-
leased) between medical doctors and the simulator.
Figure 2 shows an expected activity model represent-
ing simple interactions between a medical doctor and
the cricothyrotomy simulator.
Then, we define an instance of an expected activ-
ity as a specific path in A from the initial node to the
end node.
An instance of an Expected Activity (V, E, δ, ρ) is
a finite sequence hv
1
,...,v
m
i of nodes in V such that:
(i) hv
i
,v
i+1
i ∈ E for 1 < i < m; (ii) {v | hv,v
1
i ∈ E} =
0, i.e. v
1
is the start node I; (iii) {v | hv
m
,vi ∈ E} = 0,
Figure 2: An example of Expected Activity Model.
Figure 3: System Architecture.
i.e. v
m
is the final node F. The probability of the
instance is
∏
m−1
i=1
ρ(hv
i
,v
i+1
i)
.
We work with sequences of time-stamped events.
Let us assume that the number of observable events in
our domain is finite, each event can then be associated
to a different action symbol in the set S. We define an
observed event as a pair ω = (s,ts), where ω.s is the
action symbol associated to the event and ω.ts is the
time stamp at which s was observed.
We call a Simulator Log Ω a finite sequence of log
entries ω
i
.
Now, we are in the position of defining the concept
of Activity Occurrence.
Let Ω be a Simulator Log and A=(V, E, δ, ρ) an
Expected Activity. An occurrence of A in Ω is a se-
quence h(ω
1
,v
1
)...(ω
m
,v
m
)i where: (i) hω
1
,...,ω
m
i is
a subsequence of Ω such as ω
i
= (ω
i
.ts,ω
i
.s), ω.s
being an action symbol from S and ω.ts the associ-
ated time-stamp; (ii) hv
1
,...,v
m
i is an instance of A;
(iii) v
i
= ω
i
.s for 1 < i < m
1
; (iv) ω
i+1
.ts − ω
i
.ts ≤
1
v
i
refers both to the node v
i
in A and the action symbol
s
i
labeling it
DiscoveringExpectedActivitiesinMedicalContextScientificDatabases
449
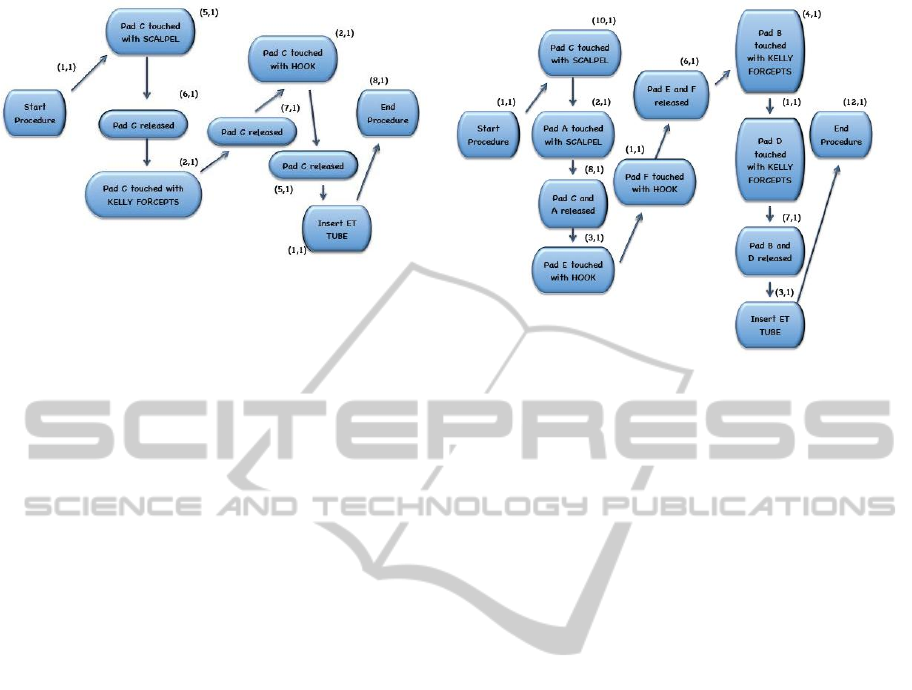
Figure 4: Expected Activity Models.
δ(hv
i
,v
i+1
i) for 1 < i < m.
The probability p(o) of the occurrence o should be
the probability of the instance hv
1
,...,v
m
i. Of course,
shorter activities usually have higher probabilities.
Therefore, since we compare occurrences of different
activity models despite their different lengths, we in-
troduce the relative probability p
∗
(o) = p(o)/p(max).
When computing p
∗
(o) for a given occurrence o, we
consider p(max) as the highest probability of any in-
stance of A when ignoring each instance’s self-loops.
Thus, once we have given the previous formal
definitions for defining our expected activity model,
we can describe the proposed architecture for find-
ing expected activities in medical context scientific
databases in section 4.
4 THE PROPOSED
ARCHITECTURE
The theoretical model has been exploited to develop
a framework for the detection of expected activities
in medical context scientific databases. The structure
of the system is based on a modular architecture, as
shown in Figure 3, which allows the medical doctors
to get a very fast feedback about their performances
when using the simulator.
The following subsections describe the single
components of the overall system architecture.
4.1 The Arduino Microcontroller Board
As also mentioned in section 2, the Arduino micro-
controller board allows us to capture in real time
the contact data of the instruments (scalpel, tracheal
hook, and hemostat) from six different landmarks of
the simulator. In such a way, this component records
the series of time-stamped events, corresponding to
the medical doctors’ interactions with the simulator.
In more detail, events are defined as the start and end
times of contacts between specific instruments and
surfaces on the anatomical model. Other types of
events are defined in terms of readings from different
sensor types. Thus, events are represented by a se-
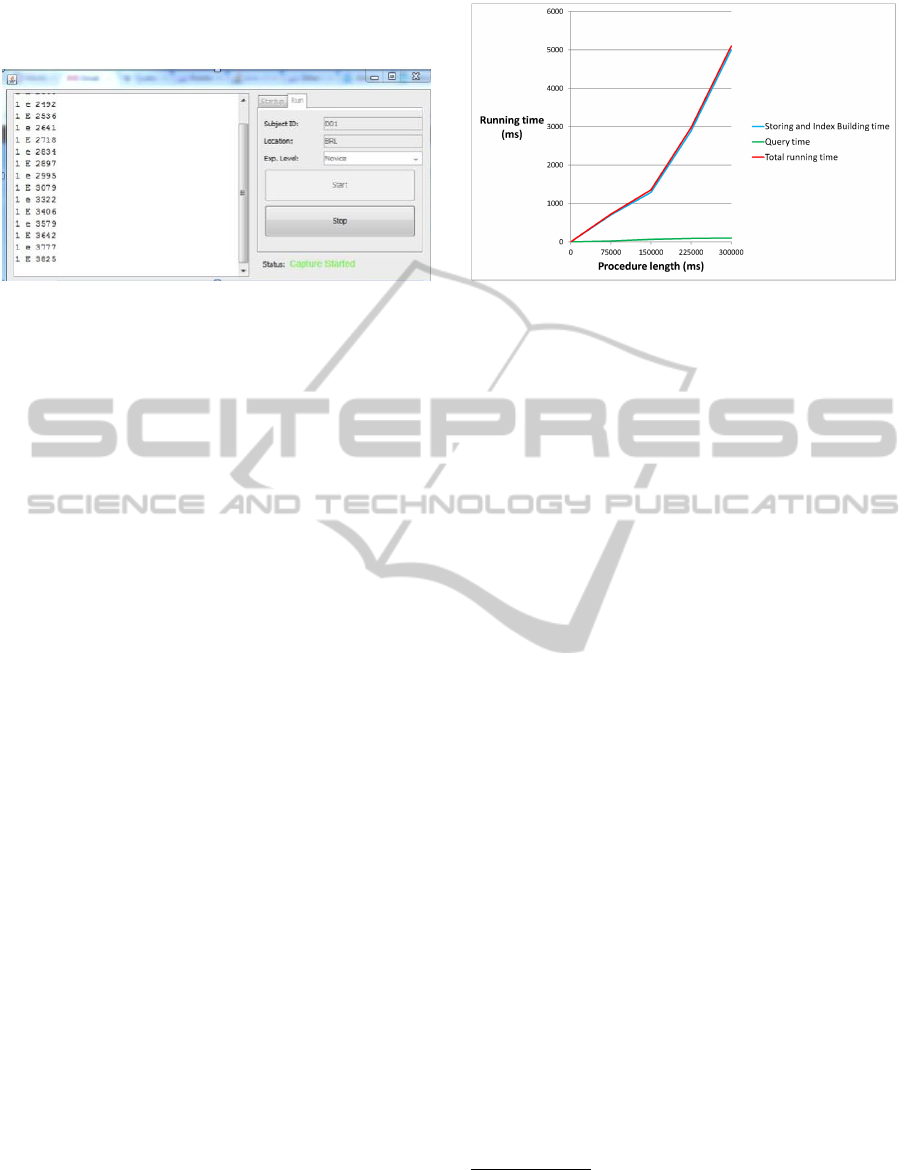
ries of symbols (ASCII characters). An excerpt of the
captured data is shown in Figure 5. Data are encoded
as follows:
• The first single digit number indicates the instru-
ment (1 means Scalpel, 2 Hemostat and 3 Tra-
cheal Hook).
• The character indicates which foil patch is
touched: upper-case for making contact and
lower-case for breaking contact. In more detail, A
means Posterior tracheal wall, B the Right lateral
trachea and cricothyroid membrane, C the Mid-
line cricothyroid membrane (correct placement of
incision), D the Left lateral trachea and cricothy-
roid membrane, E the Cricoid cartilage and F the
Cartilaginous ring of lower tracheal wall.
• The last number is the time in milliseconds.
Then, the data captured in this way represent the
input of the Data Acquisition component.
4.2 The Data Acquisition Component
The Data Acquisition component includes an Adapta-
tion Module that converts the data captured using the
Arduino in a format suitable to the detection frame-
work (i.e. the Simulator Log): it also saves them into
a scientific database, which is able to store personal
DATA2014-3rdInternationalConferenceonDataManagementTechnologiesandApplications
450
information about the medical doctors who are using
the simulator as well.
Figure 5: Data captured using the Arduino Microcontroller
Board.
4.3 The Activity Detection Engine
The Activity Detection Engine takes as inputs time-
stamped user data collected in the Simulator Log and
a set of activity models to find the activity occurrences
matching the known models. Such models have been
previously defined by domain experts who have clas-
sified them in two different categories: the good activ-
ities, corresponding to a correct use of the simulator
and the bad activities, corresponding to an incorrect
use of the simulator. Figure 4 shows two model ex-
amples of a good activity (at left), corresponding to
an excellent performance of the medical doctor and
a bad activity (at right), corresponding to a very bad
performance.
Expected activity occurrences in a data stream
are efficiently detected using tMagic (Albanese et al.,
2013), which allows to solve the problem of find-
ing occurrences of high-level activity model in an ob-
served data stream. As a matter of fact, they propose
a data structure called temporal multiactivity graph to
store multiple activities that need to be concurrently
monitored, corresponding to our knowledge base of
good and bad activities. They then define an index
called Temporal Multiactivity Graph Index Creation
(tMAGIC) that, based on this data structure, examines
and links observations as they occur. Finally, they de-
fine an algorithm to solve the evidence problem that
tries to find all occurrences of an activity (with proba-
bility over a threshold) within a given sequence of ob-
servations. In this way, we are able to find all the Ex-
pected Activities matching the activity models of our
knowledge base in a certain sequence of observations,
allowing medical doctors to get a very fast feedback
about their performances when using the cricothyro-
tomy simulator.
Figure 6: Framework Running Times.
5 PRELIMINARY
EXPERIMENTAL RESULTS
This section shows a preliminary experimental evalu-
ation of our framework. We present the experimental
protocol for evaluating our framework in terms of ex-
ecution time scalability, detection accuracy and user
satisfaction.
5.1 Evaluating Execution Time
We decided to measure
2
the execution time of our
framework for detecting Expected Activities in the
worst case (at least one action symbol for each mil-
lisecond) when varying the length of the Simulator
Log and using the previously defined set of known ac-
tivity models. In more detail, the maximal length of
Simulator Log considered has been 5 minutes, since a
longer procedure would cause the death of the patient.
The time for acquiring data using the Arduino micro-
controller can be considered as negligible. Thus, the
Total Running Time is given by the sum of the Storing
and Index Building Time (higher value) and the Query
Time (lower value), as shown in Figure 6. However,
the obtained Total Running Time can be considered
low even if we are considering the worst case.
5.2 Accuracy Results
100 medical doctors participated in a trial and used
the simulator with our additional framework. The
classic Precision and Recall metrics have been used
2
All experiments presented in this Section were con-
ducted on a machine running Mac OS X 10.9.1, and mount-
ing a 2GHz Intel Core i7 processor with a 8 GB, 1600 MHz
DDR3.
DiscoveringExpectedActivitiesinMedicalContextScientificDatabases
451
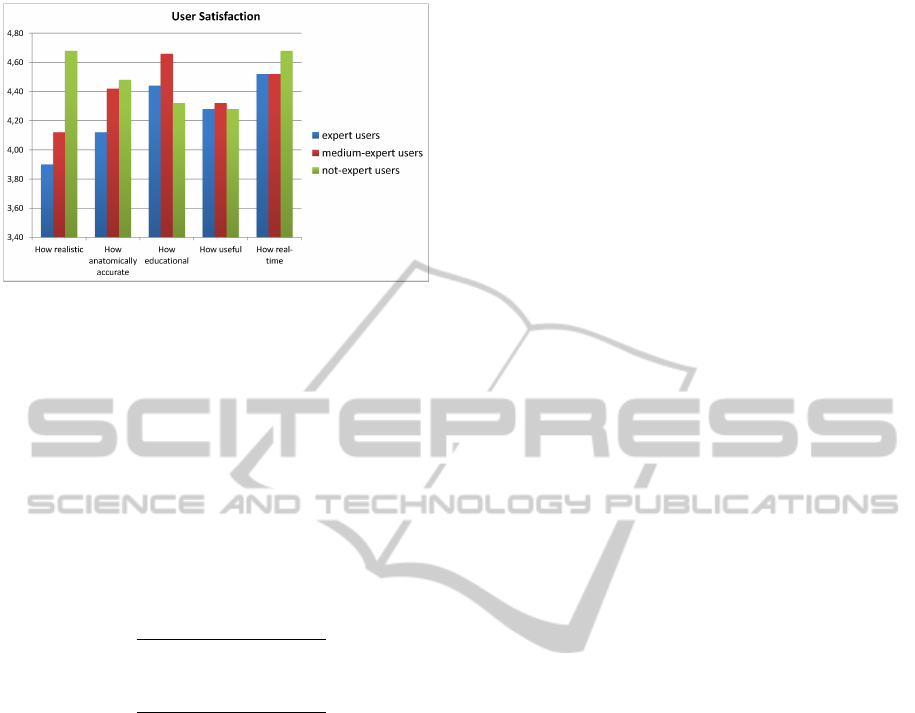
Figure 7: User Satisfaction.
to compute the accuracy (Albanese et al., 2014; Al-
banese et al., 2011), by comparing the Expected Ac-
tivities discovered by our framework with a ground
truth defined by experts who watched the recordings
of the medical doctors’performances several times.
We use {A
a
i
}
i∈[1,m]
to denote the Expected Activi-
ties returned by our framework and {A
h
j
}
j∈[1,n]
to de-
note the activities flagged as expected by human an-
notators. Precision and recall were computed as fol-
lows:
P =
|{A
a
i
|∃A
h
j
s.t. A
a
i
≈ A
h
j
}|
m
(1)
and
R =
|{A
h
j
|∃A
a
i
s.t. A
a
i
≈ A
h
j
}|
n
(2)
We achieved an average Precision of 81% and an
average Recall of 98%, that can be considered a very
encouraging result.
5.3 User Satisfaction
After completing the procedure, the medical doc-
tors, classified in three different categories (expert,
medium-expert and not expert users), filled out a
questionnaire to report their level of training, expe-
rience and their impressions of the simulator. Each
subject was asked to answer 5 questions about the
simulator (How realistic, How anatomically accurate,
How educational, How useful, How real-time) using
a 5-point Likert scale. As we can see in Figure 7, sub-
jects (especially not-expert users) expressed positive
opinions about their experiences with the simulator.
6 CONCLUSIONS AND FUTURE
WORK
This work presented a framework for activity detec-
tion in the medical context. We started acquiring data
from a cricothyrotomy simulator, when used by medi-
cal doctors and we then stored the captured data into a
scientific database. Finally, we used some stable ac-
tivity detection algorithms for discovering expected
activities, corresponding to specific performances ob-
tained by the medical doctors when using the simu-
lator. Some preliminary experiments showed encour-
aging results concerning efficiency, effectiveness and
user satisfaction.
Future work will be devoted to enlarge our exper-
imentation and to plan to integrate the prototype in
more complex and thorny applications by adding new
functionalities and, if necessary, additional layers to
the overall system architecture. For example, a po-
tential application of this tool could consist in mon-
itoring the performance of medical personnel in real
time and detecting potential safety hazard in advance,
for instance, using machine learning techniques and
observations learned during the training of medical
personnel. Moreover, data mining techniques could
be used in an offline setting to analyze in detail the
medical doctors’performances.
REFERENCES
Albanese, M., Molinaro, C., Persia, F., Picariello, A., and
Subrahmanian, V. (2014). Discovering the top-k unex-
plained sequences in time-stamped observation data.
IEEE Transactions on Knowledge and Data Engineer-
ing, 26(3):577–594.
Albanese, M., Molinaro, C., Persia, F., Picariello, A., and
Subrahmanian, V. S. (2011). Finding ”unexplained”
activities in video. In Proceedings of the Twenty-
Second International Joint Conference on Artificial
Intelligence - Volume Volume Two, IJCAI’11, pages
1628–1634. AAAI Press.
Albanese, M., Moscato, V., Picariello, A., Subrahmanian,
V. S., and Udrea, O. (2007). Detecting stochastically
scheduled activities in video. In Veloso, M. M., editor,
IJCAI, pages 1802–1807.
Albanese, M., Pugliese, A., and Subrahmanian, V. S.
(2013). Fast activity detection: Indexing for tempo-
ral stochastic automaton-based activity models. IEEE
Trans. Knowl. Data Eng., 25(2):360–373.
Bennett, B., Cailteux-Zevallos, B., and Kotora, J.
(2011). Cricothyroidotomy bottom-up training re-
view: battlefield lessons learned. Military Medicine,
176(11):1311–9.
Boselli, R., Cesarini, M., Mercorio, F., and Mezzanzanica,
M. (2014a). Planning meets data cleansing. In Pro-
DATA2014-3rdInternationalConferenceonDataManagementTechnologiesandApplications
452

ceedings of the Twenty-Fourth International Confer-
ence on Automated Planning and Scheduling.
Boselli, R., Cesarini, M., Mercorio, F., and Mezzanzan-
ica, M. (2014b). A policy-based cleansing and in-
tegration framework for labour and healthcare data.
In Holzinger, A. and Jurisica, I., editors, Interactive
Knowledge Discovery and Data Mining in Biomedical
Informatics, volume 8401 of Lecture Notes in Com-
puter Science, pages 141–168. Springer Berlin Hei-
delberg.
Brand, M., Oliver, N., and Pentland, A. (1997). Coupled
hidden markov models for complex action recogni-
tion. In Proceedings of the 1997 Conference on Com-
puter Vision and Pattern Recognition (CVPR ’97),
CVPR ’97, pages 994–999, Washington, DC, USA.
IEEE Computer Society.
Combi, C., Montanari, A., and Pozzi, G. (2007). The t4sql
temporal query language. In Silva, M. J., Laender, A.
H. F., Baeza-Yates, R. A., McGuinness, D. L., Olstad,
B., Olsen, . H., and Falco, A. O., editors, CIKM, pages
193–202. ACM.
Cook, T., Woodall, N., and Frerk, C. (2011). Major com-
plications of airway management in the uk: results
of the fourth national audit project of the royal col-
lege of anaesthetists and the difficult airway society.
part 1: anaesthesia. Fourth National Audit Project,
106(5):617–31.
Cuntoor, N., Yegnanarayana, B., and Chellappa, R. (2008).
Activity modeling using event probability sequences.
Image Processing, IEEE Transactions on, 17(4):594–
607.
Hamid, R., Huang, Y., and Essa, I. (2003). Argmode - ac-
tivity recognition using graphical models. In Com-
puter Vision and Pattern Recognition Workshop, 2003.
CVPRW ’03. Conference on, volume 4, pages 38–38.
Hongeng, S. and Nevatia, R. (2001). Multi-agent event
recognition. In Computer Vision, 2001. ICCV 2001.
Proceedings. Eighth IEEE International Conference
on, volume 2, pages 84–91 vol.2.
James, H. and Pacheco-Fowler, V. (2008). Cricothyrotomy.
N Engl J Med.
King, D., Ogilvie, M., Michailidou, M., Velmahos, G.,
Alam, H., deMoya, M., and Fikry, K. (2012). Fifty-
four emergent cricothyroidotomies: are surgeons re-
luctant teachers? Scand J Surg, 101(1):13–5.
Oliver, N., Horvitz, E., and Garg, A. (2002). Layered rep-
resentations for human activity recognition. In Mul-
timodal Interfaces, 2002. Proceedings. Fourth IEEE
International Conference on, pages 3–8.
Patrick, J.D. Safari, L. and Cheng.Y. (2013). Knowledge
discovery and knowledge reuse in clinical information
systems. Proc. The 10th IASTED International Con-
ference on Biomedical Engineering (BioMed 2013).
Safari, L. and Patrick, J. (2013). A temporal model for
clinical data analytics language. In Engineering in
Medicine and Biology Society (EMBC), 2013 35th
Annual International Conference of the IEEE, pages
3218–3221.
Vaswani, N., Roy-Chowdhury, A., and Chellappa, R.
(2005). ”shape activity”: a continuous-state hmm for
moving/deforming shapes with application to abnor-
mal activity detection. Image Processing, IEEE Trans-
actions on, 14(10):1603–1616.
Wang, H., Mann, N., Mears, G., Jacobson, K., and Yealy,
D. (2011). Out-of-hospital airway management in the
united states. Resuscitation, 82(4):378–385.
Warner, K., Sharar, S., Copass, M., and Bulger, E. (2009).
Prehospital management of the difficult airway: a
prospective cohort study. J Emerg Med, 36(3):257–
65.
White, L., Bly, R., D’Auria, D., Aghdasi, N., Bartell, P.,
Cheng, L., and Hannaford, B. (2013). Cricothyro-
tomy simulator with computational skill assessment
for procedural skill training in the developing world.
In AAO-HNSF Annual Meeting and OTO Expo.
White, L., Bly, R., D’Auria, D., Aghdasi, N., Bartell, P.,
Cheng, L., and Hannaford, B. (2014). Cricothyrotomy
simulator with computational skill assessment for pro-
cedural skill training in the developing world. Journal
of Otolaryngology - Head and Neck Surgery.
White, L., Bly, R., D’Auria, D., Bly, R., Aghdasi, N.,
Bartell, P., Jones, C., and Hannaford, B. (2012a).
Cricothyrotomy simulator training for the developing
word. In 2012 IEEE Global Humanitarian Technol-
ogy.
White, L., Bly, R., D’Auria, D., Bly, R., Aghdasi, N.,
Bartell, P., Jones, C., and Hannaford, B. (2012b).
Global simulation training in healthcare.
Zhou, L. and Hripcsak, G. (2007). Methodological review:
Temporal reasoning with medical data-a review with
emphasis on medical natural language processing. J.
of Biomedical Informatics, 40(2):183–202.
DiscoveringExpectedActivitiesinMedicalContextScientificDatabases
453
