Kinematic Analysis of the Gait in Professional Ballet Dancers
The Effect of Rehabilitation Intervention on Movement of Lower Limbs and Pelvis
during the Gait in Professional Ballet Dancers
Lucie Teplá, Markéta Procházková, Zdeněk Svoboda, Miroslav Janura and Jana Vaculíková
Faculty of Physical Culture, Palacky University, Tr. Miru, Olomouc, Czech Republic
1 OBJECTIVES
Professional ballet dancers could be compared to
high-performance athletes (Leanderson et al., 1996).
Ballet position on the top of the foot (en´pointe)
requires extreme plantar flexion and foot pronation
(Lung, Chern, Hsieh & Yang, 2008). This is a
special situation that distinguishes dance from other
sports (Miller, 2006). This increases the risk for
overused injuries (Gilbert, Gross, & Klug, 1998).
These undesirable effects of ballet can be translated
to performance of common daily activities like
walking.
The aim of this study was to assess the effect of
rehabilitation intervention on kinematic parameters
during the gait in ballet dancers.
2 METHODS
Thirteen professional ballet dancers (5 males, 8
females; mean age 25.8±5.6 years; height 172.8±8.1
cm; weight 59.8±12.2 kg) participated in this study.
This experimental group participated in
rehabilitation intervention for six week.
Rehabilitation program consisted of neuromuscular
exercise techniques and manual therapy. We
evaluated performance of the gait in dancers before
and after this rehabilitation.
The experimental group was compared with the
group of twelve controls (3 males, 9 females; mean
age 24.3±2.75 years; height 173.3±6.01cm; weight
72.2±12.73 kg). The exclusion criteria for all
subjects were any serious musculoskeletal injuries or
surgery of the lower limbs.
Additionally, control
group had no ballet experience. Kinematic data were
obtained using the optoelectronic system Vicon MX
(Vicon Motion Systems, Oxford, London).
Reflective markers of kinematic model PlugInGait
were placed at the pelvis and the lower limbs. Each
participant performed five successful trials of gait at
self-selected walking speed.
Angle variables of lower limbs and pelvis were
evaluated in all three planes. The data was evaluated
in Statistica (Version 9.0, Stat-Soft, Inc., Tulsa, OK,
USA) using Wilcoxon test (p<0.05) for comparison
of differences between dancers before and after
rehabilitation and Mann-Whitney test (p<0.05) for
comparison of dancers and control group.
3 RESULTS
Selected kinematic variables in the observed groups
are shown in Figures 1–2 and Table 1. To compare
the experimental group before and after
rehabilitation, dancers demonstrated decreased hip
adduction (p < 0.05) after intervention. Dancers also
demonstrated significantly greater maximal ankle
dorsal flexion during the stance phase (p < 0.05) as
well as greater maximal hip abduction (p < 0.01)
before and after rehabilitation compared to the
control group. Dancers reached significant greater
internal knee rotation (p < 0.05) and smaller external
rotation (p < 0.05) after rehabilitation in comparison
with the control group. The other kinematic
variables were not statistically significant.
C D1 D2
0 102030405060708090100
–25
–20
–15
–10
–5
0
5
10
15
Gait cycle ( %)
A
n
k
l
e
a
n
g
l
e
(
d
e
g
r
e
e
s
)
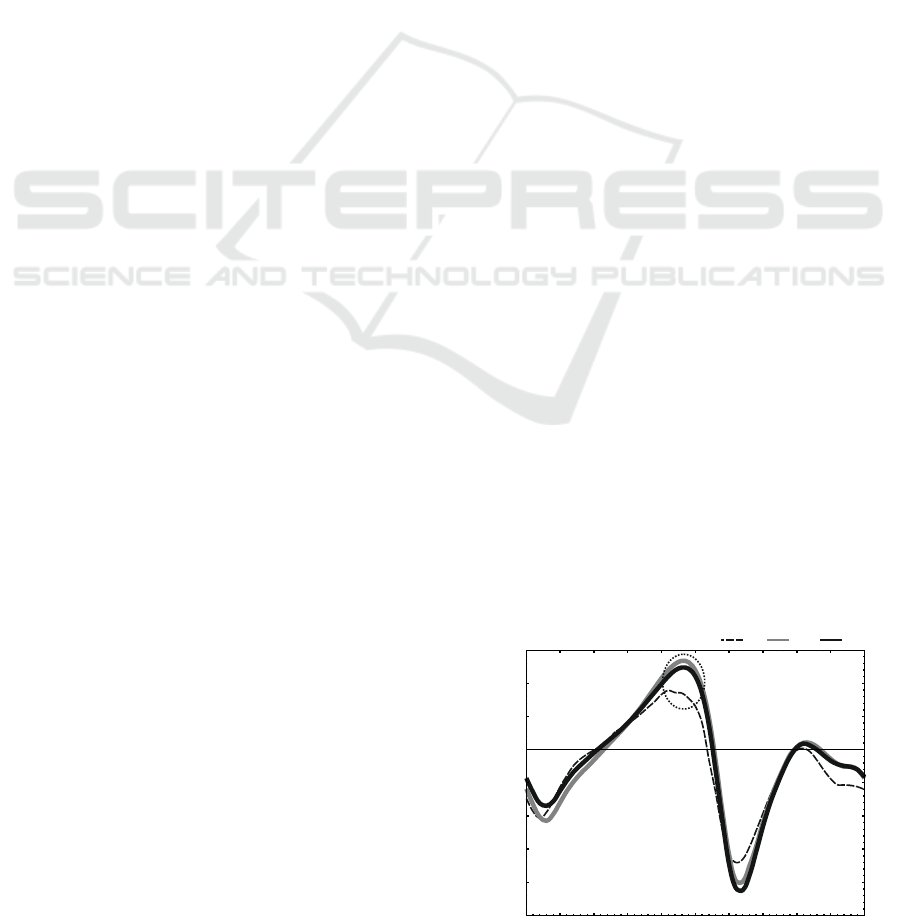
dorsal flexionplantar flexion
: p < 0 05D1 vs. C .
D2 vs. C: p < 0.05
Figure 1: Ankle movement in the sagittal plane during gait
(C – controls; D1 – dancers before rehabilitation; D2 –
dancers after rehabilitation).
Teplá L., Procházková M., Svoboda Z., Janura M. and Vaculíková J..
Kinematic Analysis of the Gait in Professional Ballet Dancers - The Effect of Rehabilitation Intervention on Movement of Lower Limbs and Pelvis during
the Gait in Professional Ballet Dancers.
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
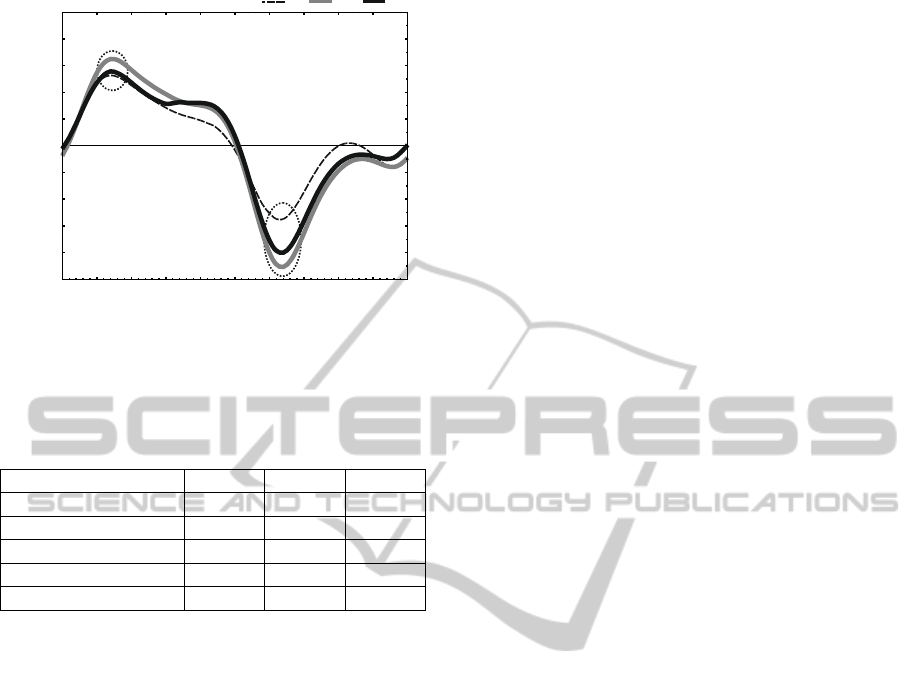
C D1 D2
Gait cycle (%)
Hi
p
a
n
g
le
(
d
e
g
rees)
adductionabduction
D: p < 0052 vs. C .
D1 vs 2: p < 0 05. D .
0 102030405060708090100
–10
–8
–6
–4
–2
0
2
4
6
8
Figure 2: Hip movement in the frontal plane during gait
(C – controls; D1 – dancers before rehabilitation; D2 –
dancers after rehabilitation).
Table 1: Maximal values (mean±SD) of selected
kinematic variables.
Variable C D1 D2
Ankle dorsal flexion*/& 7.8±7.5 14.2±3.3 13.5±3.1
Knee internal rotation * 23.0±8.7 14.9±8.3 23.9±21.3
Knee external rotation * 0.9±6.4 -7.1±6.8 -1.1±11.2
Hip abduction * / & -6.1±2.3 -9.3±2.0 -8.6±1.8
Hip adduction # 5.6±3.0 6.8±1.5 5.8±1.8
Legend:
C – controls; D1 – dancers before rehabilitation;
D2 – dancers after rehabilitation;
Statistically significant differences (p < 0.05):
* between controls and dancers before rehabilitation;
& between controls and dancers after rehabilitation;
# between dancers before and after rehabilitation.
4 DISCUSSION
The observed increased dorsal ankle flexion in
dancers can be explained by special ballet position
(e.g. grand plié, demi-plié), which require excessive
range of dorsal ankle flexion. If the foot is
frequently forced into extreme range of movements,
it loses ability to support the medial arch and act as a
shock absorption. Dancers subsequently overload
the medial part of the foot. This causes increased
pronation (Rusell, 2010). Insufficient range of
movement in hips together with hyperpronation is
compensated by increased external tibia rotation,
which was demostrated in dancers before
rehabilitation. This causes greater medial load of the
knee, which can predispose to injury (Cimelli and
Curran, 2012; Clippinger, 2007). In addition,
chronic ankle instability is often associated with hip
abductor weakness (Rusell, 2010). The increased
range of hip can be caused by inadequate
coordination between adductors and abductors.
The results show that six-week long
rehabilitation did not affect performance of walking
in professional dancers. However, the observed
parameters in dancers after rehabilitation can predict
improved alignment of these joints during gait,
which may reduce stress load being applied on the
lower limb´s structures. The results confirm that the
long-term rehabilitation should be a necessary part
of comprehensive care about dancers to improve
their ballet techniques and prevent injuries.
ACKNOWLEDGEMENTS
This work was supported by the Ministry of
Education, Youth and Sport of the Czech republic
(grant number MSM 6198959221) and Faculty of
Physical Culture (grant number FTK_2012:031).
REFERENCES
Leanderson, J., Eriksson, E., Nilsson, C., Wykman, A.,
1996. Proprioception in classical ballet dancers.
American Journal of Sports Medicine. 24(3), 370-4.
Clippinger, K.,
2007. Dance anatomy and kinesiology.
Human Kinetics, Champaign, 1
st
edition.
Russell, J. A., 2010. Acute ankle sprain in dancers.
Journal of Dance Medicine and Science. 14(3), 89–96.
Miller, C., 2006. Dance medicine: Current concepts.
Physical Medicine and Rehabilitation Clinics of North
America, 17(4), 803–811.
Lung, C.-W., Chern, J.-S., Hsieh, L.-F., Yang, S.-W.,
2008. The differences in gait pattern between dancers
and non-dancers. Journal of Mechanics. 24(4), 451–
457.
Gilbert, C. B., Gross, M. T., Klug, K. B., 1998.
Relationship between hip external rotation and turnout
angle for the five classical ballet positions. Journal of
Orthopaedic and Sports Physical Therapy. 27(5),
339–347.
Cimelli, S. N., Curran, S. A., 2012. Influence of turnout on
foot posture and its relationship to overuse
musculoskeletal injury in professional contemporary
dancers. Journal of the American Podiatric Medical
Association. 102(1), 25-33.
