
Advanced Multi-parametric Monitoring and Analysis for
Diagnosis and Optimal Management of Epilepsy and
Related Brain Disorders: The ARMOR Project
Christos P. Antonopoulos
1
, Nikolaos S. Voros
1
, André Bideaux
2
,
Panagiota Anastasopoulou
2
, Stefan Hey
2
and Wilhelm Stork
2
1
Technological Educational Institute of Western Greece,
Computer and Informatics Engineering Department,
Embedded System Design and Applications Lab,
National Road Antiriou-Ioanninon, 30020, Antirio, Greece, 30020, Greece
{chantonopoulos, voros}@teimes.gr
2
Karlsruhe Institute of Technology,
Institute for Information Processing Technologies, Engesserstr. 5, 76131 Karlsruhe, Germany
{panagiota.anastasopoulou, andre.bideaux, stefan.hey,
wilhelm.stork}@kit.edu
Abstract. The ARMOR project addresses the needs of the epileptic patient and
healthcare professional, aiming at the design and development of a non-
intrusive Personal Health System (PHS) for the monitoring and analysis of epi-
lepsy-relevant multi-parametric data, (i.e. EEG, EOG, EMG, EKG, skin con-
ductance data) and the documentation of the epilepsy related symptoms.
ARMOR platform incorporates models derived from data analysis based on al-
ready existing state-of-the-art communication platform solutions emphasizing
on security issues and required adaptations to meet ARMOR specifications. In
this context, this chapter aims to provide an extensive description of the main
aspects and issues addressed in the project as well as the main characteristics of
the developed platform.
1 Introduction
In this chapter we are introducing the main concepts of ARMOR EU funded project.
The main goal of the specific project is to manage and analyze a large number of
already acquired and new multimodal and advanced technology data from brain and
body activities of patients with epileptic disorders and controls (Magnetoencephalog-
raphy (MEG), multichannel Electroencephalography (EEG), video, Electrocardio-
gram (ECG), Galvanic skin response (GSR), Electromyography (EMG), etc) aiming
to design a more holistic, personalized, medically efficient and economical monitor-
ing system.
The ARMOR project effectively tackles requirements posed by both patients and
professionals, regarding a low cost yet highly efficient and secure ambulatory epilep-
sy monitoring platform. The platform is able to acquire as well as analyze (either
34
Hey S., Anastasopoulou P., Bideaux A., Stork W., Voros N. and Antonopoulos C.
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The ARMOR Project.
DOI: 10.5220/0006144500340055
In European IST Projects - The Quest for Excellence Towards 2020 (EPS Vienna 2014), pages 34-55
ISBN: 978-989-758-101-4
Copyright
c
2014 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

online or offline) epilepsy-relevant multi-parametric data, (i.e. EEG, EOG, EMG,
EKG, skin conductance data).
Epilepsy is a common, devastating and still incurable disorder. Although in most
cases its symptoms can be ameliorated by life-long pharmaceutical treatment, still this
treatment needs continuous adjustment and change to retain its efficacy. Due to its
multifactorial causes and paroxysmal nature, epilepsy needs multi-parametric moni-
toring for purposes of accurate diagnosis, prediction, alerting and prevention, treat-
ment follow-up and presurgical evaluation. The incidence of epilepsy is age-related,
higher in children; epileptic seizures occur in 1-2% of the general population and in
4% of children. During the periods of childhood and adolescence non-epileptic par-
oxysmal events (NEPE) also occur more frequently than in adult life with similar
clinical features. It is important to note that 30% of people with epilepsies have also
NEPE. Furthermore, epileptic seizures differ with respect to motor, cognitive, affec-
tive and autonomic and EEG manifestations. Their recognition and full understanding
is the basis for the optimal management (including additional diagnostic tests and
genetics) and treatment. The total cost of epilepsy in EU is counted upwards of 15
billion euros per year, with the severe impact on the patient of the social stigma and
the feeling of unpredictably seized, being unaccountable [1-3].
Current diagnostic methodologies and the need for advancement in this area com-
prise yet another important factor making epilepsy a prominent disorder to tackle.
Such methodologies include video EEG that records the habitual suspected event or
ambulatory EEG without video (for long term home recordings). Therefore, there is a
need for more accurate diagnosis of integrated seizure phenotype in individual pa-
tients, which will allow better understanding of underlying mechanisms, prediction
(and alert) of time and type of seizure (and alert) and availability of medical assis-
tance and advice [4-9].
In order to tackle the aforementioned challenges, ARMOR project developed an
ambulatory monitoring system for diagnosis and management, limited scalp EEG
covering and custom-designed multi-polygraphy (textile based EMG, body activity
sensors, autonomic and other biological data such as blood pressure, temperature,
sugar blood levels and O
2
and CO
2
saturation continuous monitoring). Diagnosis of a
disease as multifactorial and unpredictable as epilepsy demands continuous observa-
tion and correlation analysis of as many parameters as possible of the patient’s brain,
body and the environment.
In the context of ARMOR project, the above major medical problem has been ad-
dressed by employing the current advanced ICT technology and further advancement
in data analysis included in a way, which will benefit both the patient and the econo-
my of the health care system. In that respect, exploiting state-of-art wireless sensor
networking technologies ARMOR is envisioned as an ambulatory monitoring system
for diagnosis and management with video, limited scalp EEG covering and custom-
designed multi-polygraphy (textile based EMG, body activity sensors, autonomic and
other biological data such as blood pressure, temperature, sugar blood levels and O2
and CO2 saturation continuous monitoring). Therefore, issues such as efficient and
robust communication performance, minimization of power consumption and integra-
tion of different diverse technologies comprise cornerstones of such endeavor. Fur-
thermore, in the context of a complete end-to-end Personal Health System (PHS)
ARMOR platform includes the development of information and Tele-alarm Server as
35
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
35
well as client software for the ARMOR information and tele-alarm services. At the
same time emphasis is paid on secure communication between client software, home
gateway and wearable sensors while providing a wide range of health reporting ser-
vices and applications (Mobile, web-based and in-the-cloud back-office). From the
very beginning to the end of the project the theoretical background has also been
elaborated and the effectiveness of the ARMOR sensors has been improved by tar-
geted research work that proceeded in parallel with the steps described above. This
research involved sophisticated analysis of existing data from expensive devices (that
are not routinely available in clinics, e.g. multichannel EEG and/or MEG) and analy-
sis of selected data obtained during ARMOR project, which represent prototypical
examples or critical cases for diagnosis and classification.
2 System Architecture
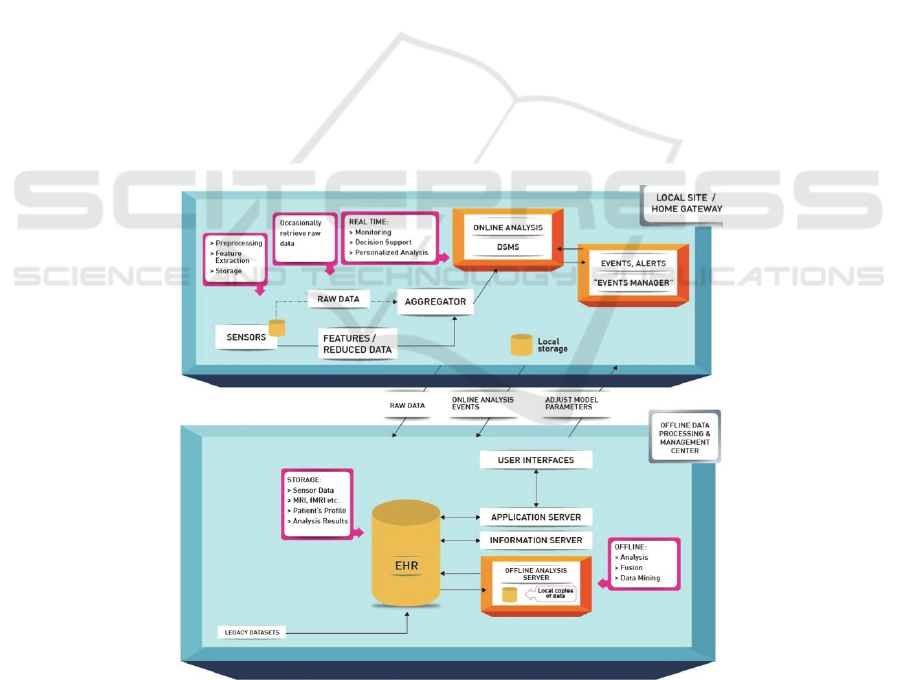
Aiming towards a holistic, medically efficient and economical monitoring system
ARMOR platform addresses all functional aspects required. Thus, following the
overall system architecture as depicted in Figure 1 a critical segment comprises of the
sensors enabling the data acquisition in the local site (e.g. the patient's home envi-
ronment). Based on the extensive experience of ARMOR consortium as well as on
the equipment provided by the involved partners, multi-parametric data acquisition is
offered through a wide range of possible sensors gathering a wide range of medical
data continuously and in real-time.
Fig. 1. ARMOR Platform Architecture.
36
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
36

The first level of data aggregation and processing is done at the home gateway
where the ARMOR MiddleWare (AMW) provides access towards the upper modules
and vice versa. The role of the AMW is crucial since it comprises of the gateway
point between the sensor hardware equipment and the functional modules of software
application. Specifically, on one hand, support is provided for all types of data and
sensors utilized in the context of ARMOR, and on the other hand a wide range of
services is provided in order to support the depicted functional modules. Furthermore,
it functions as the communication bus among all required modules.
The ARMOR information server, as part of a complete remote Electronic Health
Record (EHR) system, is also a critical component of ARMOR system since it hosts
the models derived from extended research effort for multi-parametric data analysis.
However, such functionality requires close collaboration with patient data stored in
secure databases, which comprise another important subsystem of the ARMOR plat-
form. Another functionally critical module depicted is the ARMOR Application
Server. It provides to specialized personnel, like patients, medical stuff and caregiv-
ers, access to ARMOR system through a wide range of user interfaces. Such interfac-
es include visualization of multi-parametric data processing results, EHR access and
personal tracking or nutrition habits and vital signs information.
Finally, ARMOR emphasizes on security issues of sensitive medical data through
a specialized security layer where all ARMOR sub-systems area actively involved.
The first layer tackling security issues are sensors ensuring secure data acquisition
and transferring towards the aggregation point/s. All storage sites also employ securi-
ty techniques ensuring data integrity and privacy. Data communication and data trans-
ferring are challenging issues that have to be addressed, especially when they are
performed over the air. Both sensor communication and backhaul communication
parts of systems like ARMOR are susceptible to a wide range of dangers and possible
attacks requiring special attention. Finally, as far as the offline data processing and
data management center are concerned, access rights, user authentication and authori-
zation have also been taken into account as part of ARMOR EHR system.
2.1 Mobile Sensors for Multiparametric Monitoring in Patients with Epileptic
Disorders
As ARMOR’s main target is patients with epileptic disorders, it is vital to have EEG
sensors present in the system, as it is an essential component in the evaluation of
epilepsy. It has been shown that ambulatory long-term EEG recordings with intensive
monitoring have led to better classifications of seizures and treatment results [10].
Because 30-60% of all patients are unaware of their seizures, multiparametric moni-
toring can lead to new results with optimal treatment. Without EEG recordings, false
diagnosis may be made, as various phenomena are similar to the resulting behavior of
a seizure.
Electrocardiogram (ECG) is used to record the electrical activity of the heart. It is
an effective means to help to rule out a seizure being caused by the way the heart is
working. It has been noted that in some seizures, especially those located in the tem-
poral lobe, experience a change in heart rate prior to or at the onset of the seizure
[11]. A study showed an increase in heart rate of at least 10 beats per minute in 73 %
37
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
37

of seizures (93 % of patients) and this occurred most often around seizure onset. In
23 % of seizures (49 % of patients) the rate increase preceded both the electrographic
and the clinical onset [12]. Such changes may clarify the timing of seizure onset and
can be useful for seizure diagnosis and for automatic seizure detection.
Therefore the goal is to develop a multiparametric monitoring system that assists
in diagnosis, prognosis and treatment of the disease. Such system should fulfill the
following criteria: it should be non-invasive, mobile, continuous and unobtrusive and
all possible security and privacy aspects should be taken into account. This section
describes the design of the sensors for mobile epilepsy monitoring.
2.1.1 Sensor Requirements for Multiparametric Monitoring of Patients with Epileptic
Disorders
2.1.1.1 Functional Requirements
The functional requirement of ARMOR system include:
Sampling Rate: The sampling rate for the physiological signals varies depending
on the physiological parameter that is assessed and based on the state of the art re-
search.
Resolution: The output of the sensors offers at least 12-bit resolution.
Data Format: The data format of the physiological sensor data that is used is
based on the unisens-format. This is a universal and generic format suitable for
recording and archiving sensor data from various recording systems and with var-
ious sampling frequencies.
Interfaces: The sensors communicate with the aggregator wirelessly by using the
Bluetooth interface in order to transmit the pre-processed data for the online
analysis or/and via USB in order to store the assessed raw data.
Online Analysis: The online analysis can be partially performed on the sensor
side, where the data are pre-processed and on the aggregator where a novel
Data
Stream Management System
(DSMS) effectively performs the further analysis that
needs extra computation power.
Security: The communication between the sensors platform and the aggregator
employs encryption algorithms such as AES.
2.1.1.2 Non-functional Requirements
The non functional requirement of ARMOR system include:
Weight, Dimensions, Housing: In order to develop a system appropriate for use in
everyday life, the sensor platform have to be as unobtrusive as possible. Of course
some technical limitations such as the battery consumption/ dimension might lead
to bigger housings. A trade-off between the comfort and the system lifetime has to
be made.
Usability: Usability is a very important aspect that is also taken into account, as
the end-users (Doctor, Patient, Healthcare Professional, Family Member or Care-
giver) might be persons with limited technical knowledge. Therefore, the software
38
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
38

for starting/stopping the sensors offers an adequate GUI and special attention to
user friendliness is paid.
Calibration & Service: Calibration and service must also be supported by the
producer/distributor of the specific unit.
Distribution to the End-users: The patient will be wired-up at the hospital before
he/she goes off to spend his/her day. The electrodes will be firmly fixed by the
caregivers, whereas the sensors mostly needed for monitoring during nocturnal
sleep will be easily placed / replaced by the patients before he/she goes to bed and
unplugged in the morning after awakening.
Time of Use: The sensors should be able to measure for at least 24 hours.
Price: The price of the final system will depend on the number of units that will
have to be used.
2.1.2 The ARMOR Sensor System for Mobile Epilepsy Monitoring
In order to achieve the main requirement, the multi-parametric monitoring, different
sensors are integrated in the system. This includes not only the most relevant bio-
signal for epilepsy monitoring, the EEG but also ECG, GSR and a push button that
have be proven to be important in mobile epilepsy monitoring [13-15]. For this sys-
tem the following sensors have been selected.
The EEG module (Trackit
TM, Lifelines Ltd, Over Wallop, UK) is a mobile ambu-
latory device that can measure up to 32 channels with a sampling rate of 256 Hz.
Each channel has an ADC resolution of 16 Bit and has a maximum differential AC
input 10 mV. Depending on the number of channels, the sampling rate and the battery
used the device can achieve up to 96 hours of recording.
The ECG module (ekgMove, movisens GmbH, Karlsruhe, Germany) is a single
channel ECG recorder with a 12-bit resolution and a sampling rate from 256 Hz to
1024 Hz. The module can either be used with electrodes integrated into a wearable
chest strap, which is light, small and comfortable or be used with conventional dis-
posable wet electrodes. The electrodes of the chest strap are dry, allowing the every-
day use. To assess the patient’s physical activity, the module has also an integrated
triaxial acceleration sensor (adxl345, Analog Devices Inc.) with a range of ±8 g and a
sampling frequency of 64 Hz and an air pressure sensor (BMP085, Bosch GmbH)
with a sampling frequency of 8 Hz and a resolution of 0.03 hPa.
Fig. 2. ECG-Sensor with activity monitoring module.
The GSR module (edaMove, movisens GmbH, Karlsruhe, Germany) measures the skin
conductance with a sampling rate of 32Hz. The measurement range of the GSR module is
39
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
39

2μS to 100μS and its resolution is 14 bit. With this one can measure both the electrodermal
activity level (EDL) and responses (EDR). Furthermore the module has the same sensor
set to measure physical activity integrated as the ECG module.
Fig. 3. GSR Sensor.
The push button module (bioPLUX, PluX, Arruda dos Vinhos, Portugal) is a device
that collects up to 8 signals from various sensors and transmits the signals via Bluetooth to
a computer, where they can be viewed in real time. The resolution of bioPLUX is 12 bits,
and its sampling frequency is up to 1 kHz. For this system only one channel with a push
button sensor is used.
To assess additional context parameters like sound, light or geographic position, a
smartphone can be used. Connection between Smartphone, Sensor and Aggregator is
also realized by Bluetooth interface.
2.2 Communication Infrastructure
From communication point of view, ARMOR project developed a secure and effi-
cient platform that is able to acquire data, aggregate them to a gateway on the home
environment, exploiting state-of-the-art Wireless Sensor Network technologies and
finally convey them to a data repository residing into a hospital or a caregiver facility.
Consequently, a complete communication infrastructure comprises a multifaceted
objective in order to achieve efficient and secure end-to-end data handling and trans-
ferring.
Respectively, the whole process can be segmented into three major parts: (a) the
sensors data acquisition functionality, (b) the wireless transmission of data from the
sensor to the aggregation point, and finally (c) EHR for controlling data management
and data extraction from home gateway to the hospital facility.
2.2.1 Secure Sensors' Data Acquisition
Focusing on the sensors side, one key requirement is related to security. This is be-
cause respective devices comprise a potentially weak and vulnerable point in the
whole chain of data flow. Specifically, typical WSN sensors employed in the
ARMOR platform are small, low cost, devices operating unattended (e.g. in a pa-
40
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
40

tient's home environment) for extended periods of time thus being relatively easily
acquired by unauthorized persons trying to access sensitive data. ARMOR sensors
dispose of a Bluetooth interface, a debugger interface, a power supply and a local
storage on a SD card. The debugger is used to read or flash the sensor and to debug
the program. With respect to these main characteristics various alternatives have been
studied and adopted to enhance security provision. To avoid the read of the data or
the program code from the microcontroller, the debugger interface is disabled. The
sensor platform disposes of a special interface to update the flash with a program
code: the so-called “bootloader”. This interface gives no access to the storage and can
only be used to transfer a program. In the case of using an encryption of the local
storage it is advisable that this interface is disabled as well. Additionally, attacks over
the power supply are normally made in laboratory to get a secret key that is not
changing and need to use measurement instruments direct on the sensor. In the case
of a platform using data encryption, the secret key is changing periodically with re-
spect to new measurements. The secret key is needed while saving the data on the
local storage and so the user of the sensor will notice this kind of attacks.
ARMOR sensors are based on the MSP 430 microcontroller unit from Texas In-
struments offering a performance optimized software implementation of the Ad-
vanced Encryption Standard (AES). This implementation is designed for the 16-bit
RISC architecture of the Texas Instruments MSP 430 controller family and it is pro-
vide as a C interface offering high level security AES crypto features [16].
Research on similar commercial products has shown that no encryption mecha-
nism on the local storage is used [17,18]. Based on the above risk analysis encryption
on the local storage is not required.
2.2.2 Wireless Sensor Network Data Transmission
In the context of a demanding medical application, such as epilepsy monitoring, a
wide range of different signals leading to diverse data traffic requirements are re-
quired to be transferred. For example, in ARMOR project the sampling frequency of
signals acquired could span from few Hz or tens of Hz (e.g. accelerometer and respi-
ration sensor) up to hundreds of Hz or around 1 KHz (e.g. EEG and ECG signals).
Taking into consideration that each sample is typically represented by a 16-bit num-
ber as well as that in many cases multiple sensors are required in each case (e.g. a
complete EEG monitoring may require tens of EEG electrodes) it can be easily de-
duced that a wide range of traffic rates must be supported.
However, selecting an appropriate technology is not straightforward due to the
specific requirements posed by typical WSN sensors and platforms. During the last
few years, state of the art WSN technologies exhibit impressive advances advocating
respective system as a prominent solution for demanding applications. On one hand,
advances in hardware design, integrated embedded systems and miniaturization have
proven that extremely small devices, yet sufficiently powerful, can be implemented.
Additionally, such devices offer the capabilities to acquire data from the physical
world, store and process them, but even more importantly to transmit them wirelessly
using embedded transceivers. On the other hand, software developments have intro-
duced a completely new communication paradigm attracting high interest both from
academia and industry offering flexibility, rapid network deployment, self-
41
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
41

organization, distributed operation, power aware functionalities etc. All these capabil-
ities offered have led to significant advancements in various networking areas espe-
cially focusing on physical, MAC and routing layers of the ISO/OSI networking
model [17, 18] characterizing respective technologies.
However, offering the aforementioned characteristics comes at the cost of extreme
limitations in critical aspects, which comprise Achilles’ hill especially regarding pro-
cessing power, storage capabilities, communication bandwidth and most importantly
energy availability. The implementation of a typical WSN node is based on compo-
nents with extremely limited resources such as low processing capabilities (usually
provided by 16-Bit based Micro Controller Units), limited available memory (in the
area of 10 Kbyte RAM) and scarce energy availability; most prominent WSN plat-
forms base their operation on few AA batteries or even batteries with significantly
less capacity like Shimmer [19] platform that uses 450 mAh batteries. At the same
time, nodes are expected to operate unattended for extended periods of time.
Furthermore, in order to live up to the expectations of sensitive applications such
as the medical ones, another equally critical aspect that short range wireless commu-
nication technologies have to address is the provision of adequate security. It is com-
monly accepted that in sensitive nowadays applications it is of paramount importance
to guarantee that data gathered, stored and transferred comply with strict ethical and
legislative regulations as well as data privacy, data integrity and authentication of
communication parties [20]. In order to provide these features, we must rely on the
efficient execution of robust and state of the art cipher algorithms. In the context of
the ARMOR platform, Bluetooth protocol was employed for ARMOR WSN infra-
structure, while IEEE 802.15.4 was also considered and evaluated.
Bluetooth is a wireless radio specification designed to replace cables as the medi-
um for data and voice signals between electronic devices. The specification is defined
by the Bluetooth Special Interest Group (SIG), which is made up of over 1000 elec-
tronics manufacturers. Primarily intended for mobile devices, Bluetooth’s design
places high priority on small size, low power consumption and low costs. Bluetooth
specification seeks to simplify communication between electronic devices by auto-
mating the connection process.
Bluetooth radios operate in the unlicensed 2.4 GHz Industrial, Scientific, and
Medical application (ISM) frequency range. This frequency is already widely used by
all kind of devices such as microwave ovens, baby monitors, cordless telephones, and
802.11b/g wireless networking devices. In order to avoid interference from these
devices, Bluetooth uses a technology called spread spectrum frequency hopping.
Spread spectrum frequency hopping changes the transmission frequency up to 1600
times per second across 79 different frequencies. As a result, interference on any of
those frequencies will only last a fraction of a second. This, coupled with the limited
range of Bluetooth radio transmitters, results in a robust signal that is highly tolerant
of other devices sharing the same frequency.
Contrary to IEEE 802.15.4 based solutions, where all relative platforms are char-
acterized by analogous capabilities, Bluetooth based solutions vary significantly de-
pending both on the version of the protocol supported and even more on the specific
implementation's characteristics. Therefore, concerning data rates solutions covering
a wide range from 300 Kbps up to 1.5 Mbps can be found [19], [21], [22].
42
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
42

Furthermore, contrary to IEEE 802.15.4, which effectively leaves security support
to the higher ISO/OSI layer, Bluetooth offers a complete security specification with
respective advantages and disadvantages. Bluetooth security is based on three critical
services: authentication, authorization, and encryption. The authentication service is
supported by ensuring that a device seeking a connection is indeed the one it claims
to be. Authorization is the process that determines whether or not a requesting device
is allowed access to specific information or services. Encryption helps to ensure con-
fidentiality by protecting private data from being viewed by unintended recipients.
Bluetooth v2 devices, upon which ARMOR platform is based, can be set in one of
three different security modes. In security mode 1, no security measures are utilized.
Any other Bluetooth device can access the data and services of a device in security
mode 1. Security mode 2 enacts security measures based on authorization. In this
mode, different trust levels can be defined for each of the services offered by the
device. Security mode 3 requires both authentication and encryption. The security
features of the Bluetooth specification provide for secure communication at the link
level that comprises a weak point. Moreover, there are some weaknesses that need to
be considered. These weaknesses arise from the specification’s heavy reliance on
device authentication for security services as well as the level of control that the user
has over Bluetooth devices and their configuration. The current Bluetooth specifica-
tion does not provide any means of user authentication. The lack of any means of user
authentication coupled with the reliance on device authentication leaves Bluetooth
particularly vulnerable to spoofing attacks and the misuse of authenticated devices
[23].
Based on projections indicating the rapid increase of short range wireless commu-
nication devices (e.g. in the context of a cyber physical system) the need for more
secure systems using stronger cipher algorithms, while not requiring excessive re-
sources, will also increase. Even more, provision should be made for cases where
new communication technologies will appear or when existing technologies (e.g.
Bluetooth) will need to coexist with new ones without compromising security level.
In such cases, an implementation not being limited by cipher algorithms of particular
communication protocol (e.g. E0 and E1 of Bluetooth) but rather following a more
widely adopted paradigm (e.g. AES) will be of significant added value.
In order to deal with the aforementioned challenges, in the context of ARMOR an
ultra-low power hardware encryption module has been developed. It provides high
security level regardless of the underlying communication technology employed and
is based AES encryption algorithm [49]. AES algorithm has been standardized by the
National Institute of Standards and Technology (NIST) as a highly secure block ci-
phering method. It has replaced the old DES algorithm, whose key sizes were becom-
ing too small. The developed encryption module implements AES algorithm in FPGA
technology and is highly optimized for ultra-low power dissipation rendering it an
ideal solution for WSN network applications. The encryption module has been care-
fully designed to require minimum logic resources as well as utilizing power aware
design techniques in architectural (8-bit datapath, use of sequential structures, re-
source reuse, optimized Galois Field Multiplier which is the structural datapath ele-
ment of the cryptographic engine, pipelining, path balancing, one hot FSM encoding)
as well as in FPGA implementation level (clock and data disabling). The use of these
techniques has resulted in a significant performance/silicon footprint ratio [24].
43
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
43

2.2.3 Personal/Electronic Health Record Technologies
In the context of a holistic approach like the one offered by ARMOR project, the
adoption of the proper EHR technology is of paramount importance. As part of
ARMOR system it entails all aspects of data handling, management and transferring
from the home environment of the user (i.e. the patient) to the service provider that
can be a hospital, a clinic, a doctor or any kind of care giving facility. ARMOR’s
Personal Health Records (PHR) intends to be a standard electronic management sys-
tem of medical information exchanged on between the patient and his/her physicians,
as well as amongst medical organizations that collaborate for providing integrated
medical care services. ARMOR PHR has been designed using the latest technology
that allows efficient and secure handling of patients’ sensitive medical data.
Significant effort has been devoted to security aspects since in today’s global and
mobile economy, it is common to hear stories of companies paying significant costs
and exposing themselves to lawsuits due to corporate assets and data being compro-
mised. At the same time, IT departments started to face new risks associated with the
growing need to support remote access to mobile users, partners and customers. Ad-
ministrators must constantly compromise the risks associated with providing remote
access with increasing demands for mobility. Remote users require access to compa-
ny’s resources any time from anywhere, using any computer whether it is provided by
a company, own laptop or an internet cafe PC, mobile or handheld PDA device. E-
Health systems, platforms and services are also examples of such requirements. They
employ standard networking technologies and hence they are vulnerable to same
types of attacks. Having to deal with extremely sensitive private and personal data,
they are also exposed at the risk of law suits and they need to employ much more
stringent security mechanisms, including data acquisition from distributed medical
instruments and protection of (often) distributed EHR repositories against intrusion
and data theft.
The end-to-end security is one of the possible approaches to counter fight these
risks. End-to-end security means that sensitive data are encrypted all the way from the
device side application back to the enterprise. Rather than relying on transport-level
security (such as Secure Sockets Layer, or SSL), end-to-end security puts the power
of strong encryption in the user's hands, all through a simple interface. The specific
requirements posed for the technology adopted in ARMOR included: authenticated
and authorized sensor information access, secure Web service interfaces to PHR and
secure Web services with HTTP.
Nowadays the area of EHR technologies has attracted high interest as indicated by
the wide range of standardization bodies involved [25]. The data structure algorithms
and the user iInterfaces proposed [26-28] as well as the number of different and di-
verse implementations [29-33]. The ARMOR platform has adopted the intLIFEPHR
solution provided by Intracom S. A. Telecom Solutions, which is member of the
ARMOR consortium. intLIFEPHR consists of the following subsystems:
Electronic Health Record Subsystem
Vital Signs Monitoring Subsystem
Personal Health Record Subsystem
intLIFE Management Subsystem
44
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
44

Through the above features intLIFEPHR perfectly suited the needs of the ARMOR
platform offering an efficient, robust and secure backhaul connection between the
home environment and caregivers' facility.
2.3 System Middleware
The ARMOR Middleware (AMW) represents the ICT component that provides the
necessary infrastructure to acquire & store locally and upload to remote server (the
PHR) sensor data. It provides infrastructure for real time computation of raw sensor
data (modalities) along with the necessary data aggregation and synchronization func-
tions. It also provides a notification module that communicates specific events (main-
ly alarms) to high-level applications
AMW consists mainly of three parts. The first part is the xAffect that collects all the
data from the sensors and fuses them to a synchronized data stream. The second part is the
graphical user interface. It is used to interact with the patient or healthcare professional
and also handles the data storage and uploads. The last part is the Data Stream Manage-
ment System (DSMS), which it uses the data stream to perform online analysis to detect
events of special interest.
2.3.1 xAffect
xAffect is a software framework developed by the Research Center for Information Tech-
nology, Karlsruhe, Germany. It has been developed in Java to fulfill real-time data pro-
cessing, easy integration of different data sources, easy integration of algorithms and data
logging of raw as well as derived data [34]. The data format, which is being used, is the
unisens-format. This is a universal and generic format suitable for recording and archiving
sensor data from various recording systems and with various sampling frequencies [35].
Although xAffect™ offers much functionality, in the context of ARMOR two
main parts of it have been tailored to ARMOR needs: data streaming and data re-
cording, which fulfill AMW’s integration requirements successfully. However the
capabilities for data fusion remain available as complement to the data stream man-
agement system, named ARMOR Insight.
Version 1.01.846 of xAffect™ allows to use it as library, which resulted in em-
bedding it as a component in AMW. The specific version has also been modified in
order to customize the interface with AMW that was necessary to achieve the perfor-
mance and the functionality required for the AMW. The changes that were introduced
can be summarized as follows:
Additional libraries for bioPlux and TrackIT. In order to use a broad spectrum of
sensors, non-existing libraries had to be written from scratch.
A decryption module that allows realizing ciphered data coming from ARMOR
sensors will come ciphered.
Data acquisition pause/resume to achieve the needs for the control of the sensor
data acquisition.
A custom notification module for communicating xAffect state to AMW DSMS.
Data recording functionalities have been extended to provide configurable file
45
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
45
splitting (in order to reduce high network consumption during heavy data up-
loads), alarm signal detection and a communication system with AMW PHR up
loader daemon.
Data streaming functionalities have been extended to provide hot-plug client con-
nections and custom xml output data formats (including gzip for network traffic
optimization).
2.3.2 Graphical User Interface
In the Graphical User Interface (GUI) the user enters his/her username and password
and the patient-id, which corresponds to a personalized profile from the Server. Af-
terwards the user can press the configure button to initialize the communication with
the sensors. Furthermore the profile contains information about the alarm settings.
This enables the system Middleware to set up the DSMS with the customized set of
alarms [36].
Fig. 4. ARMOR Graphical User Interface.
When the configuration process has finished successfully the user is able to start
the measurement by pressing the record button. During recording, the data are
streamed from the sensors through xAffect towards the DSMS and the local storage.
The GUI also allows the user to pause or resume the measurement. This allows the
subject to interrupt the data acquisition and move out of the Bluetooth range of the
Home Gateway.
2.3.3 Data Stream Management System (DSMS)
The DSMS function takes place on-line, where real time processing of modalities is
performed. The DSMS is based on Microsoft™ StreamInsight™ platform created for
the development and deployment of complex event processing (CEP) applications.
46
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
46

It’s a high-throughput stream processing architecture that uses .NET Framework-
based development platform.
The development done at the DSMS allows receiving xAffect™ sensor data in re-
al time and forewards them in a lossless way to the computation algorithms. In this
way, the framework is able to create queries and policies over data.
Lossless data streaming between xAffect™ and DSMS is achieved by employing
TCP channel. This makes sure the built-in architecture of StreamInsight™ can work
with the synchronized data coming from xAffect™.
The main objective of the DSMS is to deliver alarm and warning events prede-
fined in the profile. One of the most important events is the push button detection.
Other events are for example an alpha rhythm or seizure detection.
3 Epilepsy Monitoring and Data Analysis
The proposed system provides novel functionality for both real-time (online) and
offline analysis of data. New techniques have been developed for multi-parametric
sensor data mining (data fusion and correlation analysis, integration of information
from various data sources/modalities, similarity analysis of signals, clustering, classi-
fication and prediction). Novel real time (online) analysis methods for multi-
parametric stream data have also been developed aiming at detecting signals beyond
the limits, identify seizure premonitory signs, discover typical patterns of activity
followed by seizures and detect any typical patterns of activity/behaviour based on
models that will be created. Trade-offs for automated analysis are taking place at the
local site of each patient (instead of at the Health Center) aiming to reduce processing
time, storage requirements and communication cost, facilitating the reduction of raw
data to secondary and tertiary parameters (that have been correlated), have also been
taken into account. All analysis and emergency alert mechanisms are based on a per-
sonalized model according to the patient's health profile. New decision support tools
for advising the patient, triggering an alarm and detecting emergency situations have
also been developed.
In addition, new informatics tools have been developed for offline analysis of
multi-parametric data correlation with other stored data about the patient (EEG, PET,
SPECT, fMRI, genetic data) and the disease, offline data fusion for certain combina-
tions of modalities (e.g. MEG, MRI) taking place at the Health Center with the partic-
ipation of medical experts as well as new functionality that will provide feedback to
the online analysis model. ARMOR has also contributed with novel contributions in
the analysis of multidimensional time series, similarity analysis of signals, detection
of patterns and associations between external indicators and mental states, analysis of
associations among signals and symptoms, discovery of lag correlation among differ-
ent signals, detection of vital signs of a person changing in a significant manner,
identification of motifs (in spatio-temporal signals) and frequently repeated patterns
or outliers (corresponding to seizure signs), and automatic summarization of results
for each patient.
Moreover, new techniques have been investigated for the detailed offline tomo-
graphic analysis of multichannel EEG and MEG data recorded simultaneously with
47
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
47

measurements of heart activity (EKG), Galvanic skin Response (GSR) and other
measurements that can be easily incorporated in the online monitoring for normal and
epileptic patients in awake state and at different sleep stages obtaining the most direct
insight of what is happening in the brain. As far as sensor data acquisition and pre-
processing (cleaning, integration, transformation and reduction) are concerned, both
existing and novel techniques for data reduction and summarization (to deal with data
streaming) have been considered.
Finally, in the context of ARMOR, existing database technologies have been ex-
tended to support the organization of multi-parametric data including the support of
efficient storage and retrieval capabilities such as multidimensional indexing. The
ARMOR databases store logs of all events, recorded values from sensors and other
metrics that are monitored, personalized patient health profiles, medical information
including guidelines for diseases, symptoms, medication, potential side effects of
medication, etc.
3.1 Current Practices and Challenges for Epilpsy Monitoring
Unprovoked seizures and epilepsy are fairly common treatable neurological condi-
tions (incidence of unprovoked seizures 33 to 98 per 100,000 per year; incidence of
epilepsy 23 to 190 per 100,000 per year; prevalence of epilepsy 3 to 41 per 1000;
lifetime risk of epilepsy: 1 to 3%) [37]. There is considerable disagreement about the
recurrence risk following a first seizure. Estimates of the recurrence rates following
the first seizure over two and three years have varied between 23% [38] and 71%
[39]; the risk of recurrence has been estimated at 14% at one year, 29% at three years
and 34% at five years [40]. In a systematic review and meta-analysis including both
prospective and retrospective observational studies, the pooled estimate of the risk of
recurrence of a first unprovoked seizure at two years was 42% (95% CI 39 to 44)
[41]. The more seizures an individual have had, the higher the risk of subsequent
seizures; the risk of a recurrence following two seizures is approximately 73% and
after three seizures is 76%. There is evidence that early treatment can reduce the risk
of seizure recurrence, and its efficacy depends largely on the appropriate drug choice
in relation to the particular clinical syndrome. Therefore, early and accurate diagnosis
of epilepsy is crucial in patients’ management. However, there are two important
clinical problems to consider.
First, the initial symptom of epilepsy (the first seizure in life) usually manifests as
an episode of loss or impairment of consciousness, usually associated with change of
muscle tone. The diagnostic challenge here is to distinguish an epileptic seizure from
other medical conditions that present with similar clinical features but require com-
pletely different and specific for each clinical category treatment and management.
These clinical entities manifest as non-traumatic transient loss of consciousness, i.e. a
brief clinical episode, characterised by rapid loss of normal responsiveness, loss or
reduction of muscle tone or stiffness and amnesia for the event [42].
Second, the generic term “epilepsy” is unsatisfactory for clinical use. Intense clin-
ical and genetic research over the last few decades have identified a large number of
well defined epilepsy syndromes with different clinical, EEG, neuropsychological,
and neuroimaging profiles, natural history and prognosis, conditions that ultimately
48
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
48

require different management. Identification of the particular form or epilepsy syn-
drome is the cornerstone of meaningful, optimal management.
Therefore, there are two major steps in the orderly diagnostic process of the pa-
tient with possible new onset epilepsy: 1) is it epilepsy or another disorder of Transi-
ent Loss of Consciousness (TLC)? and 2) what type of epilepsy is it?
Syncope is the commonest cause of TLC, due to cerebral hypoperfusion. Neurally
mediated (vasovagal, neurocardiogenic or reflex) syncope can happen in up to 40%
of the general population and can be misdiagnosed as epilepsy, particularly when it
results to cerebral hypoxia and to a reflex anoxic seizure. Cardiogenic syncope is due
to structural heart disease or arrhythmia, and psychogenic syncope can mimic organic
types of syncope [43].
Detailed history regarding possible triggers and the circumstances of the event and
accounts of several episodes from patients and onlookers are essential for the diagno-
sis of syncope and its differentiation from epilepsy and other causes of TLC. Physical
(heart auscultation and BP measurements) and neurological examination may reveal
specific cardiac or autonomic disorders and prompt the relevant referrals. An EEG is
not a basic ancillary test, unless a diagnosis of epilepsy is likely; however, on rare but
well documented occasions, focal epileptic seizures (mainly right temporal) may
trigger cardiac asystole and anoxic seizures. Important laboratory tests include:
Electrocariogram (ECG) which determines the cause in less than 5% of cases [44].
Echocardiography, of undetermined but generally small diagnostic yield (detects
structural cardiac abnormalities) [45].
Exercise test, of less than 1% diagnostic yield. Prolonged monitoring for 48h
(Holter) or few weeks (continuous loop recorders) or months (invasive Medronic
device planted subcutaneously). A frequent problem is detection of arrhythmias
without symptoms.
Tilt table test (positive in 50% of patients with syncope) [46].
Other autonomic function test (of undetermined but generally small diagnostic
yield, time consuming and expensive).
Diagnosis of epilepsy may also require differentiation from other paroxysmal events
that may alter or appear to alter neurological function to produce motor signs or sen-
sory, autonomic or psychic symptoms that at least superficially resemble those occur-
ring during epileptic seizures. Such clinical events are typically known as non-
epileptic seizures (NES), and can be either of physiological (PhNES) or psychogenic
(PsNES) origin; distinction between these two types is important for proper treatment
and management and relies on recognition of organic symptoms and signs. More than
30% of the patients referred to epilepsy centers have NES only whereas a smaller
proportion has epileptic and NES in combination, particularly PsNES.
In order to deal with the aforementioned challenges, ARMOR allows progress be-
yond the above diagnostic and follow-up procedures by:
Combining all appropriate measurements of brain and body activity at the same
time.
Integrating these multi-parametric and multimodal data so as to allow better dif-
ferential diagnosis of epileptic from non-epileptic seizures as well as to define bet-
ter the type of epilepsy seizures represent.
49
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
49

Allowing a custom made selection of the most simple and economical sensors to
be employed in each patient, based on (a) advanced analysis of data with initial
extended use of many sensors and (b) experience gained from advanced analysis
of similar cases.
Allowing the final monitoring to be conducted at the patient's (child's) own physi-
cal environment and in a cheaper and more efficient way (for clinical purposes).
ARMOR also provides a valuable clinical tool to clinical epileptologists as it
solves several different current technical problems of long term monitoring and
communication of the many parameters needed to describe the complex nature of
paroxysmal seizures.
ARMOR through basic and clinical research has shed light to our ignorance on
several questions of epileptology which demand long term and accurate multi-
modal and multi-parametric monitoring including: (a) electroclinical correlations
of loss of consciousness in generalized seizures, (b) sleep/epilepsy relationships
and (c) stress and other triggers/premonitory signs of epileptic seizures.
The possible relationship of above to the localization of epileptic foci activations
in brain space - with implications to pathophysiology of epilepsy and its therapeu-
tics including presurgical evaluation.
3.2 Offline Data Analysis Algorithms
The offline data analysis in ARMOR has two main goals: to help accurate diagnoses
and to support the online monitoring of patients. Various methods have been devel-
oped. These newly developed and other, already available, methods have been used to
analyze data from patients with epileptic disorders and healthy individuals, including
whole night polygraphic recording. The tools for polysomnography have offered
valuable experience in dealing with issues related to data from long term monitoring
(8 hours). Beyond the known strong interdependencies between sleep and epilepsy
[47], additional justification for studying normal sleep microstructure features has
been given by recent findings linking epileptic ictogenesis to sleep and more specifi-
cally to sleep instability [48], sleep K-complexes and sleep spindles. The results of
these offline data analyses provided new insights into different aspects of epilepsy
and sleep, and were relied upon to offer recommendation of the polygraphic online
monitoring of patients.
Every online recording performed with the ARMOR online platform system is up-
loaded to the Patient Health Record (PHR) database. From there it is transferred to
the offline analysis database. In order for this service to be precise, there are several
steps that should be followed. The first one is to check if there is a new recording in
PHR. It should be noted that every recording is related to a specific patient, a specific
device performing the recording and the data of the recording. The synchronization
service checks in specified time intervals for a new recording in the PHR system. If a
set of new recordings is detected, then these recordings are requested from the PHR
database. The format of the data in each new recording is Unisens. Once the whole
recording has been downloaded and checked for errors (e.g. download errors, missing
files etc) the data are transformed in EDF format. Once this step is completed a sub-
50
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
50
routine will handle the EDF data to extract all the necessary info and store them in the
offline analysis database. Then the newly uploaded data can be accessed through pre-
specified queries.
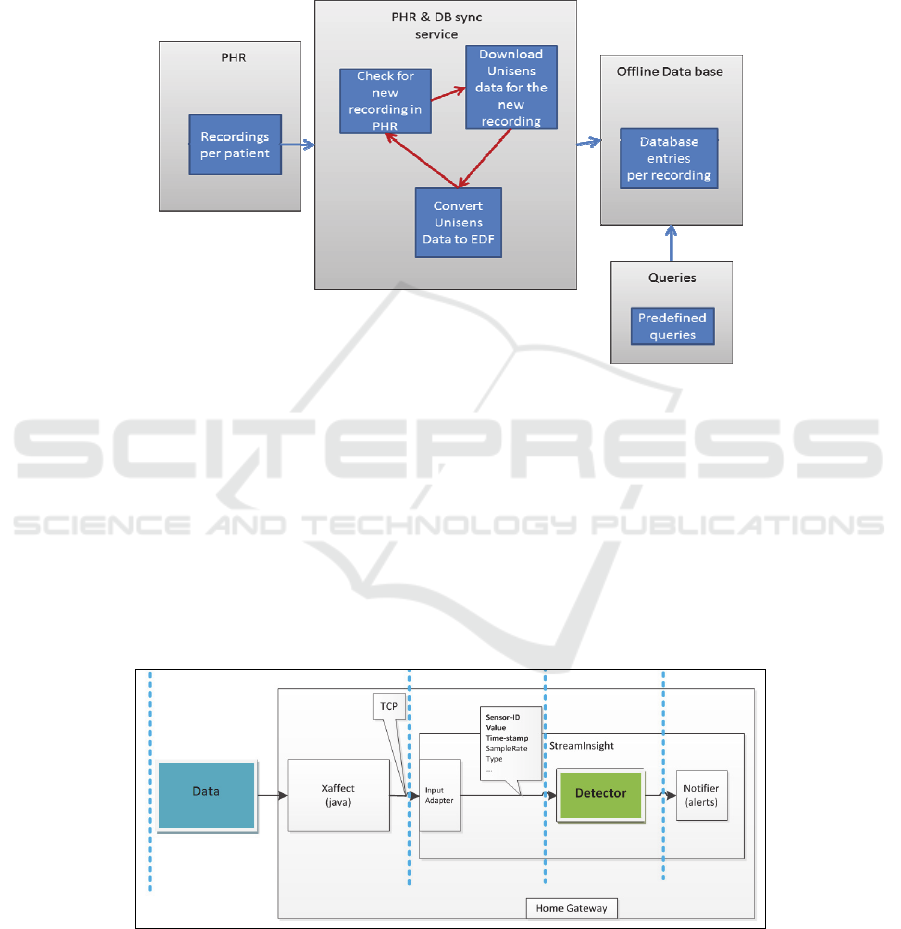
In the following figure the structure of the main components of the synchroniza-
tion of the two databases is presented.
Fig. 5. Main components of the database synchronization.
3.3 Online Data Analysis Algorithms
One way of performing an online analysis of sensor data is a multi-layer Data Mining
Model. These models are divided into four layers: data collection, data management,
event processing layer and data mining service layer. The ARMOR Online platform
is consisted of a similarly structured system. The data collection layer includes the
sensors and uses the xAffect tool for streaming the sensors’ data to a StreamInsight
application. The streamed data are being processed with a previously specified and
parameterised algorithm, before the detected events are extracted.
Fig. 6. Interface between different data management modules.
51
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
51

The core of each detection algorithm is implemented in Mathworks' Matlab envi-
ronment. Matlab offers many features that make the design of an algorithm more
efficient and effective as well as shortening the time needed for the development of
the algorithm. An online application on the other hand requires a Data Stream Man-
agement System (DSMS), which offers the ability to process online data in a time and
memory efficient way. The system used in our applications is StreamInsight from
Microsoft. To introduce our algorithms to the Microsoft's StreamInsight environment,
the .NET compiler and API of Mathworks have been used. In more detail, Mathworks
provides a compiler for .NET packages. The result of this procedure is a set of librar-
ies containing the algorithms and all the necessary components (functions, data such
as training models, etc) necessary for each algorithm. The compiled libraries can be
accessed by a StreamInsight application using the API that Mathworks provides. This
API is the Matlab Compiler Runtime, which provides all the necessary components in
order to use the algorithm in a stream application.
It should be noted that each algorithm has been designed to operate with segments
of the data, as it is necessary in an online application. In order to pre-process, the
streamed data, before having them processed from the detection algorithm, a set of
StreamInsight tools were used. Depending on the procedure followed by the detection
algorithm, the streamed data should be aggregated or transformed in matrices whose
rows and columns correspond to channels and samples of each segment, respectively.
The detection procedure is performed after this step. In the case of the seizure detec-
tor for each time window of the streamed data, a matrix should be formed. Each row
of this matrix contains the data values for one channel during the specific time win-
dow, whereas the columns of this matrix contain the values for all channels for a
specific time point. This transformation is possible due to StreamInsight's service of
User Defined Operator.
4 Conclusions
As detailed in the previous sections, ARMOR project has addressed various critical,
challenging and multifaceted objectives in order to effectively acquire, manage and
analyze large number of signals related to epilepsy monitoring and decision-making.
In order to offer such capabilities significant research, design and development efforts
have been devoted to different and diverse areas ranging from pure medical research
to engineering areas such as wireless sensor networking and data processing algo-
rithms.
In that respect, this chapter attempted to highlight the main issues tackled and pre-
sented the main achievements as well as the design aspects of ARMOR project. Ini-
tially, the main architectural goals of ARMOR platform were presented, focusing on
its main components. Then, the requirements and characteristics of the sensors used
was also presented, as well as the overall communication infrastructure employed for
robust, efficient and secure end-to-end transfer of user sensitive personal data. One of
the cornerstone components of ARMOR architecture, ARMOR middleware, was also
detailed. ARMOR middleware resides in the home gateway of ARMOR, plays multi-
ple roles in the monitoring process and provides diverse functionalities both related to
52
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
52

communication and data processing. The second part of the chapter focused on data
analysis processes and algorithms designed and developed in the context of the pro-
ject so as to gain significant insight to epilepsy monitoring and decision making.
Concluding, ARMOR project proposed a highly efficient system able to offer sig-
nificant assistance and advancements on epilepsy monitoring and decision-making
exploiting state-of-art technologies as well as extending them.
References
1. Christian M. Korff. Ingrid E. Scheffer, "Epilepsy classification: a cycle of evolution and
revolution", Curr Opin Neurol. 2013 Apr;26(2):163-7. doi: 10.1097/
WCO.0b013e32835ee58e.
2. ANNE T. BERG, J. HELEN CROSS, "Classification of epilepsies and seizures: historical
perspective and future directions", Handbook of Clinical Neurology, Vol. 107 (3rd series)
Epilepsy, Part I H. Stefan and W.H. Theodore, Editors, 2012 Elsevier B.V
3. Newton CR, Garcia HH, "Epilepsy in poor regions of the world", Lancet. 2012 Sep
29;380(9848):1193-201. doi: 10.1016/S0140-6736(12)61381-6.
4. Badea A, Kostopoulos GK, Ioannides AA. Surface visualization of electromagnetic brain
activity.J Neurosci Methods. 2003 Aug 15;127(2):137-47
5. Barnathan M, V. Megalooikonomou, C. Faloutsos, F. Mohamed, S. Faro, «High-order
Concept Discovery in Functional Brain Images», 7th IEEE International Symposium on
Biomedical Imaging: From Nano to Macro (ISBI), Rotterdam, The Netherlands, 2010, pp.
664-667.
6. Barnathan M, V. Megalooikonomou, C. Faloutsos, F.B. Mohamed, S. Faro, «TWave:
High-Order Analysis of Spatiotemporal Data», In Proceedings of the 14th Pacific-Asia
Conference on Knowledge Discovery and Data Mining (PAKDD), Hyderabad, India, June,
21-24, 2010, Advances in Knowledge Discovery and Data Mining, Lecture Notes in Com-
puter Science, 2010, Volume 6118/2010, pp. 246-253.
7. Iasemidis LD, Shiau DS, Pardalos PM, Chaovalitwongse W, Narayanan K, Prasad A,
Tsakalis K, Carney PR, and Sackellares JC. Long-Term prospective on-line real-time sei-
zure prediction. Clinical Neurophysiology 2005; 116(3):532-44.
8. Ioannides AA, Corsi-Cabrera M, Fenwick P, del Rio Portilla Y, Laskaris N, Khurshudyan
A, Theofilou D, Shibata T, Uchida S, Nakabayashi T and Kostopoulos GK.MEG tomogra-
phy of human cortex and brainstem activity in waking and REM sleep saccades. Cerebral
Cortex, 2004;14(1):56-72.
9. Velis D, Plouin P, Gotman J, da Silva FL; ILAE DMC Subcommittee on Neurophysiology.
Recommendations regarding the requirements and applications for long-term recordings in
epilepsy. Epilepsia 2007; 48(2), 379-84
10. Stefan H., Hopfengärtner R.: Epilepsy monitoring for therapy: Challenges and perspec-
tives. Clinical Neurophysiology 2009; 120:653-58.
11. Jones V.M., et al.: Biosignal and context monitoring: distributed multimedia applications of
body area networks in healthcare. 10th Workshop on Multimedia Signal Processing in
Cairns, 2008.
12. Zijlmans M., Flanagan D., Gotman J.: Heart rate changes and ECG abnormalities during
epileptic seizures: prevalence and definition of an objective clinical sign. Epilepsia 2002;
43: 847–54.
13. Massé F., Penders J., Serteyn A., Bussel M. van, Arends J.: Miniaturized Wireless ECG-
Monitor for Real-Time Detection of Epileptic Seizures. In: Wireless Health’10, San Diego,
USA (2010)
53
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
53

14. Nijsen, T. M., Arends, J. B., Griep, P. A., Cluitmans, P. J.: The potential value of three-
dimensional accelerometry for detection of motor seizures in severe epilepsy. In: Epilepsy
& Behavior 7, 1, 74–84 (2005)
15. Poh M.-Z., Loddenkemper T., Swenson N., Goyal S., Madsen J., Picard R.: Continuous
Monitoring of Electrodermal Activity During Epileptic Seizures Using a Wearable Sensor.
In: 32nd Annual International Conference of the IEEE EMBS Buenos Aires, Argentina
(2010)
16. Texas Instrumments MSP430 microcontroller crypto software features infor-
mations:http://jce.iaik.tugraz.at/sic/Products/Crypto_Software_for_Microcontrollers/Texas
_Instruments_MSP430_Microcontrollers
17. Somnomedics: http://somnomedics.eu/home.html
18. Medset telesmart: http://www.medset.com/index.php?id=45
19. Shimmer platform http://www.shimmer-research.com/
20. EU Directive: Data Protection Directive (Directive 95/46/EC), Directive on Privacy and
Electronic Communications (2002/58/EC), Directive 2011/24/EU of the European Parlia-
ment and of the Council of 9 March 2011 on the application of patients’ rights in cross-
border healthcare
21. MoviSens: http://www.movisens.com/en
22. Revoing2011: Revoking Networks "Advanced User Manual" Version 4.77 2/3/2011
23. SANS Institute InfoSec Reading Room , "Brush up on Bluetooth", 08/21/2003
24. George Krikis, Christos P. Antonopoulos, Nikolaos S. Voros, "Design and Implementation
of Efficient Reconfigurable Cipher Algorithms for Wireless Sensor Networks" 11th IEEE
International Conference on Industrial Informatics, Bohum, Germany, 29-31, July, 2013
25. Eichelberg M, et al. (2005), “A survey and analysis of Electronic Healthcare Re-cord
standards”, ACM Computing Surveys. 37(4):277–315
26. CEN/TC251–ISO/TC215 (2010), I. E. Electronic Healthcare Record (EHR) Communica-
tion. Parts 1: Reference Model, Part 2: Archetype Model, Part 3: Reference Archetypes and
Term lists, Part 4: Security and Part 5: Inter-face Specification. 2010
27. Rector, A. et al. (1993), A framework for modelling the electronic medical record. s.l. :
Methods Information Medical, 32: 109-119
28. Beale, T. (2002), “Archetypes constraint-based domain models for future-proof in-
formation systems”, OOPSLA-2002 Workshop on Behavioural Semantics
29. Microsoft HealthVault (http://www.healthvault.com)
30. World Medical Card (www.wmc-card.com)
31. INDIVO Health (indivohealth.org)
32. TOLVEN Patient/Clinician HR (www.tolven.org)
33. OpenMRS (http://www.open-emr.org)
34. Schaaff K., Mueller L., Kirst M., http://www.xaffect.org/
35. Kirst M., Ottenbacher J., www.unisens.org
36. A. Bideaux, P. Anastasopoulou, S. Hey, A. Cañadas, A. Fernandez: Mobile monitoring of
epileptic patients using a reconfigurable cyberphysical system that handles multi-
parametric data acquisition and analysis: MobiHealth 2014
37. Hauser WA, Hesdorffer DC. Epilepsy: frequency, causes and consequences. New York:
Demos Publications, 1990.
38. Pearce JL,Mackintosh HT. Prospective study of convulsion in childhood. The New Zealand
Medical Journal 1979;89:1–3.
39. Elwes RCD, Chesterman P, Reynolds EH. Prognosis after a first untreated tonic-clonic
seizure. Lancet 1985;2:752–3.
40. Hauser WA, Rich SS, Annegers JF, et al. Seizure recurrence after a first unprovoked sei-
zure: an extended follow-up. Neurology 1990; 40:1163–70.
41. Berg AT, Shinnar S. The risk of seizure recurrence following a first unprovoked seizure: a
quantitative review. Neurology 1991;41:965–72.
54
EPS Vienna 2014 2014 - European IST Projects - The Quest for Excellence Towards 2020
54

42. Crompton DE, Berkovic SF. The borderland of epilepsy: clinical and molecular features of
phenomena that mimic epileptic seizures. Lancet Neurol 2009; 8: 370-81.
43. Stephenson JBP. Fits and faints. London: MacKeith Press, 1990; Lempert T. Recognizing
syncope: pitfalls and surprises. J R Soc Med 1996; 89: 372-5.)
44. Hammill SC. Value and limitations of non-invasive assessment of syncope Cardiol Clin
1997; 15: 195-218
45. Kapoor WN. Evaluation and outcome of patients with syncope Medicine 1990; 69: 160-75
46. Kapoor WN, Smith MA, Miller NL. Upright tilt testing in evaluating syncope: a compre-
hensive literature review. Am J Med 1994; 97: 78-88
47. Kokkinos V, Koupparis A, Stavrinou M and Kostopoulos GKThe hypnospectrogram: An
EEG power spectrum based means to concurrently overview the macroscopic and micro-
scopic architecture of human sleep. Journal of Neuroscience Methods 2009; 185(1):29-38.
48. Halasz P, Kelemen A. Relationship of phasic sleep phenomena, spike-wave discharges, and
state-dependent responsiveness in sleep. Epilepsia. 2010 May;51(5):934-5.
49. Eric Conrad, “Advanced Encryption Standard”, WhitePaper
55
Advanced Multi-parametric Monitoring and Analysis for Diagnosis and Optimal Management of Epilepsy and Related Brain Disorders: The
ARMOR Project
55
