
Automatic Prevention of Medication Errors
Mobile System Based on Near Field Communication (NFC) Technology
Ana-María López
1
, Eduardo Pascual
1
, Ana-María Salinas
1
, Guillermo Azuara
1
and Rafael Gómez
2
1
Escuela Univeritaria Politécnica de Teruel, University of Zaragoza, Ciudad Escolar s/n, Teruel, Spain
2
San José Hospital, Servicio Aragonés de la Salud, Teruel, Spain
Keywords: Medication Error, Smartphone, Near Field Communication.
Abstract: In this paper a mobile system aimed to avoid medication error in home environments is described. It is
based on unambiguous identification of pillboxes or drugs packages with a Near Field Communication
(NFC) tag. This tag, whose information can be quickly read with a mobile phone equipped with an NFC
interface, can also store information about the patient and the prescribed dose. These data can be actualized
with the smartphone whenever the patient confirms a new medication-take just by approaching the
smartphone to the labelled box. The information is also locally saved in the phone and can be sent by SMS
to caregivers if necessary. The information into the NFC tag converts a simple mobile app into an
ubiquitous computing (ubicomp) context aware tool that avoids drug or patient confusion. To ensure that
even patients with low technological experience will be able and, more important, wish to use this system,
we have followed a user centered design methodology. The system adapts to different patients profiles, and
to different degrees of digital literacy.
1 INTRODUCTION
Patient’s safety is one of the quality goals of the
healthcare systems. Possible risks to this security are
medication errors that can occur both in hospitals
and in the usual patients’ place of residence. A
medication error is defined as “any preventable
event that may cause or lead to inappropriate
medication use or patient harm while the medication
is in the control of the health care professional,
patient, or consumer.” (NCCMERP, 1998)
Medication errors are the cause of up to the 5% of
hospital admissions (Pasto-Cardona, 2009)
In this work we have developed a software tool
to be used in an android device with a Near Field
Communication (NFC) interface. The application
allows the user to visualice on the device screen the
information about a medicine that he considers
necessary. The application also controls that the
drug taking occurs in a correct way. Every drug case
is labelled with a NFC tag. These labels have a
double function. They stored information about the
medicine that can be actualized every time the
patient takes a new dose. Besides, tags are the
control element that inform the device about the
exact drug that it is going to be taken and when it
was last ingested. In this way, the application
prevents drug confusion or repeating a take. The
systems is aimed at people that want to avoid this
kind of mistakes and will not be useful without the
patient’s collaboration.
In order to create an application that really
fulfills the needs of patients, we have followed a
user centered design methodology. The information
collected from users with different profiles has lead
to the definition of specific and functional
requirements and has guided the design process of
the user interface. Also, we pursue that persons not
familiarized with the use of smartphones could feel
encouraged to use this application due to a simple
and intuitive performance. NFC technology
facilitates this interaction since the application is
started and the information is available and updated,
just by approaching the phone to the labelled drug.
In the next section, the use of automatic
identification technologies and mobile applications
to control drug management are revised. In section
3, we describe and justify the design methodology.
The results obtained at every step of the process are
shown including the software requirements, the
structure of the system and the interface of the
application. We end this paper summarizing our
276
López A., Pascual E., Salinas A., Azuara G. and Gómez R..
Automatic Prevention of Medication Errors - Mobile System Based on Near Field Communication (NFC) Technology.
DOI: 10.5220/0005186702760283
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 276-283
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

main conclusions and advancing the next steps of
our research.
2 RELATED WORK
To avoid error medication, the right patient must
take the right dose of the right drug at the right
moment in the right way (Benjamin, 2003). It
implies the management of a great amount of data
about patients, drugs and illnesses. This information
must be always available and correctly cross-
checked. The clear identification of patients and
drugs is essential
For this reason, automatic identification systems
have been widely used as a tool to prevent
medication errors. In our case, elements based on
radiofrequency communication have been chosen.
2.1 RFID Systems to Control Drug
Treatment
The radiofrequency identification, RFID, belongs to
the group of the automatic identification and data
capture (AIDC) technologies, like code bars, smart
cards or techniques of biometric identification. It is
based on the use of a unique identification code for
every element. This code is known as Unique
Identifying Digit (UID) and it is stored in the
internal memory of a RFID tag. In order to
automatically identify one item, a RFID tag is
attached to it. The UID that stands for this tag and
for the object can be read and communicated to a
control system by means of an RFID reader that
interrogates the tag using a radio frequency
electromagnetic wave. The tag answers with its own
radiofrequency signal. No precise alignment
between the reader and the RFID tag is required.
The basic elements of an RFID system are the
RFID tag, the RFID reader and the RFID software
known as middleware (Glover, 2006). The RFID tag
acts as the identification element. It’s formed by an
electronic chip, an antenna and a storage memory.
This memory has always reserved, locked blocks
where the unique code UID is saved. The tag
memory can have a bank, the user memory zone,
where new data can be written, read and modified by
the reader. In this way, pertinent information about
the medication-taking process can be dynamically
saved inside the identification element. RFID
systems can access to information and save new data
with no connection to a data management system
though they generally work fully integrated to them.
NFC technology stands for a RFID subsystem
that works in the 13.56 MHz frequency band and
shows a short read-range (below 5 cm). NFC readers
are integrated in small mobile devices, as
smartphones. A short operation distance enhances
safety and security on the exchange of information.
The use of RFID tags in both, medicaments and
patients, has been successfully implemented in
several hospitals (Lai, 2007) (Lahtela, 2008)
(Darianian, 2008a) (Sun, 2008) (Oztekin, 2010)
(Chien, 2011) (Qin, 2011) (Alabdulhaftih, 2013).
Every patient is uniquely identified by a RFID
wristband. When a RFID reader connected to the
hospital database reads the UID, the entire patient’s
data are available to the caregivers. Labelling drugs
makes it possible to crosscheck data by reading
simultaneously the patient’s wristband and the
medicament tag. Errors can be immediately detected
prevented and recorded.
Similar systems have been developed aimed to
reduce errors in medical treatments at home
environments (Agarawala, 2004) (Bardram, 2004)
(Bravo, 2013) (Chen, 2007) (Darianian, 2008b).
Medicaments are integrated into the information
management system when they are RFID labelled,
since RFID/NFC readers allow direct
communication with databases (Internet of Things).
The storage capacity of the RFID/NFC tags allows
to different caregivers, with different devices,
recording the daily events. In this way, the
information is saved just at the moment it happens
and all those involved in the care of a patient get to
know what has occurred when they are absent. If
mobile devices are used, the system can go on
working even if the patient moves to a different
place. NFC control systems based on the use of
smartphones, have been implemented as a
communication channel between patients,
caregivers, pharmacists and doctors (Iglesias, 2009)
(Vergara, 2010) (Engel, 2013) (Swedberg, 2009).
The doctor creates a NFC tag with pertinent
patient’s data such as the medicaments to be
provided by the pharmacist, their dosage or the
patient’s known allergies. Every authorized user can
collect this information with its smartphone and can
also add more information. In the case of patients
with physical or mental disabilities the phone can be
used to automatic warn caregivers.
2.2 Android Apps for Medicine
Adherence Control
The new information and communication
technologies are being quickly integrated in our
everyday activities. They provide access to
AutomaticPreventionofMedicationErrors-MobileSystemBasedonNearFieldCommunication(NFC)Technology
277

information anywhere, guarantee communication at
any moment and improve people’s life quality.
Smartphones and the development of open operating
systems as Android have brought forth a great
number of mobile applications aimed at
entertainment, personal organization or access to
specific information. In this context, many apps have
emerged, focused on the health self-control in
general, and particularly to the medicine adherence
control.
We have analyzed the functionality of three of
the most used apps. Their performance is based on
the following tasks:
To introduce general information about the
medicament.
To configure specific information about
dosage. It is possible to work with different
users.
To set flexible alerts.
To generate reports from the information
stored in a database.
None of these apps use NFC tools, so problems
as mistaking a drug for a different one cannot be
avoided. Besides, the information about the process
is only stored in a local database hosted in the
smartphone. So, if this phone is not operative or
accessible, no one can check the last medication
takings. Also, all these applications are intended for
users that are fond of smartphones and like to
experiment with this kind of apps. A degree of
previous digital experience is needed to use them
properly and, above all, without increasing the time
and effort required to accomplish an everyday task.
3 USER CENTERED DESIGN
METHODOLOGY
3.1 Justification. Ubiquitous
Computing Systems
In the previous section, several experiences about
the use of RFID/NFC technology to control drugs
taking have been referenced. In all cases, doctors
and/or pharmacists are the ones to configure the
information saved in the identification tags.
Therefore these examples are integrated in a
healthcare organization and, in many cases are
reduced to successful pilot experiments, mainly,
when home environment is involved.
Our approached seeks that the patients (or their
caregivers) configure the information related to
every medicament and save it on the NFC tags. So,
only if they consider the system as indeed useful,
they will incorporate the tool as a support for their
daily care. We have followed a user centered design
methodology from the initial step of requirements
definition to the test of the prototype with real
patients. We complete the steps of a model process
(Resatsch, 2010) associated with ubiquitous
computing systems.
We develop a mobile computing system. This
kind of system is considered a subsystem of
ubiquitous computing systems. Physical objects (in
this case, the different drugs containers) are linked to
the virtual world by mean of the NFC/RFID tags
attached to them. RFID tags are considered natural
ubiquitous elements that have provided a new form
of interaction between men and machines. One of
the possible definitions for ubicomp system is a
network and communication infrastructure defined
by the presence of various, miniaturized, networked
and often invisible technology situated within the
range of everyday human actions encompassing
applications, supporting interactions and processes
with ease of use (Resatsch, 2010). In our mobile
system, the devices are smartphones that are not
invisible and imply a clear interaction human-
device. In some cases, these elements are fully
integrated in people’s everyday life and will not
imply a special effort related to the task of taking
medication. But depending on the degree of users’
digital literacy, we must ensure both, perceived
usefulness and ease of use. So, we have to integrate
our application in the scenarios in which users carry
out their daily task reducing the awareness of the
interaction with the ubicomp infrastructure.
The first step of the model process is to define an
initial idea. We have introduced this starting point in
the first section of this paper. We analyze the
information from different potential users to refine
this idea, define the software requirements, and
create a low fidelity prototype which is assessed by
selected users. Finally, a working prototype is
developed.
3.2 Motivation. Functional
and Non-functional Requirements
3.2.1 Selecting Information Sources
In order to foster the user acceptance, we must know
more about its intents, identities, needs and desires.
The first step of the model process is to collect
information to identify the functions that are really
needed and, more important, that will not be
rejected.
HEALTHINF2015-InternationalConferenceonHealthInformatics
278

Searching for a wide user acceptance, two
different profiles have been analyzed:
Polymedicated chronically ill patients;
Patients with a temporary disease that required
up to three medicaments simultaneously.
In both cases we have identified lead users that
will contribute to the whole design process. Besides,
in some steps we have collected information from a
larger group of users, especially in order to create
the proper interaction scenarios.
Two group interviews have been carried out to
caregivers of Parkinson patients. Besides, a low
fidelity prototype has been shown and discussed.
This group of users that stands for the first studied
profile is not familiarized with the use of
smartphones. So, we have selected as lead user a
younger patient, with a wide experience in the use of
this kind of devices, which suffers from multiple
sclerosis.
In the case of the second profile, the researchers
themselves perform as lead users. We form a
heterogeneous working group which includes
engineers, doctors and psychology students. The
level of familiarity with new technologies is quite
different. In order to limit the specific functionality a
web multiple choice questionnaire, based on
(Morisky, 1986), was sent to multiple users.
3.2.2 Collected Information
The interviews with the group of polymedicated
chronically ill patients aimed to describe the context
where the medication process takes place. The main
conclusions extracted, in the case of Parkinson
patients’ caregivers, are listed below:
Patients are not able to control their
medication intake. Caregivers are usually aged
people that are not familiarized with
smartphones, but they can be helped by
younger relatives.
Parkinson patients must take a great amount of
drugs. Therefore, labelling every medicament
is not efficient. They require support to set up
a pillbox.
Parkinson treatments are very specific. It can
be said that no two patients are alike.
The caregivers have developed a personal
system to control medication. They are not
interested at all in changing it unless the new
system shows clear advantages and does not
involve a great learning effort.
In the case of general users (sporadic, non-
multiple medication), researchers have shared their
own experience. Besides, a web multiple choice
questionnaire has been send to multiple users to
stablish which bad habits are more common. The
questions (with possible answers are Never, seldom,
often, always) are:
Do you forget to take your medication?
Are you careless with the intake time?
Do you leave the treatment unfinished if you
feel better?
Do you leave the treatment unfinished if you
feel worse?
Do you mistake a medicament for another?
Do you forget the instructions given by your
doctor?
The method use to spread the questionnaire,
electronic mail, reduces the information from aged
people that do not use this kind of communication
tool. However, this kind of patients can be mainly
included in the group of polymedicated chronically
ill patients. The poor habits more frequent are the
carelessness in the time of taking the medication
(more than 25% of participants often forget the exact
time) and the cessation of allocated medication when
the patient feels better (almost 5% do it always and
more than 30% often stop taking it).
3.2.3 Functional and Non-functional
Requirements
Two roles are defined in the ubicomp structure. The
first one is a local role which manages the
application and the labelled drugs. It is necessary to
have the specific software installed in the
smartphone and access to the NFC tags. The second
one is a remote role that just needs a smartphone
connected to the mobile phone network ready for
receiving SMS when the medication protocol is not
fulfilled. In what follows, we described the specific
software functionality, so when users are mentioned,
we referred to local role users. These users can be
patients, caregivers or doctors.
The main functional requirements are listed
below:
Users can configure medication-taking issues
(drug information and dosage) both in the
smartphone and in the memory of the NFC
tag;
Users can control medication intake just by
approaching the smartphone to the labelled
tag.
Users can program alarms related to their
medication events.
Users can configure when an emergency
contact person will receive a warning in case
a medication error takes place.
AutomaticPreventionofMedicationErrors-MobileSystemBasedonNearFieldCommunication(NFC)Technology
279
Users can access to the information
generated during the medication process.
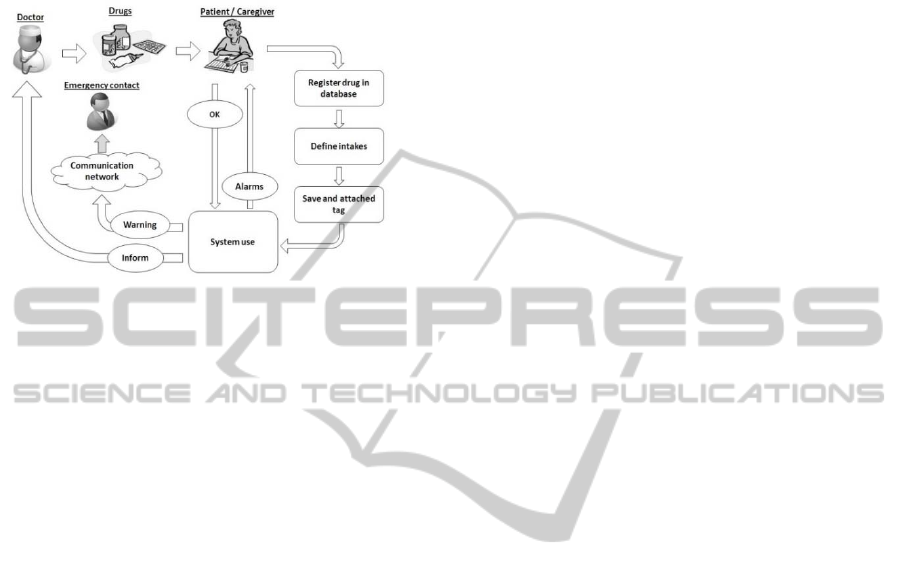
An overview of these tasks is shown in figure 1
that shows the system workflow.
Figure 1: System workflow.
Going into more detail, the configuration function
will adapt to two different scenarios:
Single-medicament intake
Pillbox set up.
The control function must be context sensitive:
Personal context: adapted to the specific
patient.
Action-related context: adapted to the
medicament read by the NFC interface.
Time-specific context: adapted to the drug
dose configured and the time where the action
is done.
Depending on these context parameters different
actions must be conducted. The software can just
mark an intake as done in both, phone and NFC tag
or must send a SMS to a remote user because the
intake of a pill is forgotten or the patient has taken
the wrong one.
Regarding to non-functional requisites, the
control function of the system is designed to interact
with users with different degrees of digital
alphabetization. In this way, for users not
familiarized with the use of smartphones, the
interaction with the system is based on reading the
NFC tag and simple voice commands. At the same
time, expert users can interact with the application as
they do with similar, well-known ones. The main
non-functional requisites are:
Work in mobile devices with Android
operative system and NFC interface.
Correct visualization on screens with different
sizes and densities.
Fast response. The NFC interaction is almost
instantaneous.
Configuration flexibility. The systems needs a
minimum set of data to work, but the user can
increase the saved information.
Possibility to access to the basic functionality
(medication-taking control) without using the
touch screen.
3.3 Low-fidelity Prototype
Two different low-fidelity prototypes have been
created. The first one was aimed to show the initial
idea during the first group interview hold at the
Parkinson association. Together with a tagged
medication box, researchers play a simple
dramatization to make it clear how to interact with
the tagged box in order to configure the information
stored in it, control medication taking and recover
information about past intakes. In this way, users
could see the technology in action and express their
feelings about it, the advantages they perceived and
their fears about using it.
After the information collection that led to the
requirement definition, a simple mock-up
prototyping was developed and evaluated by the lead
users. They will also perform their medicament
intakes with the initial working prototype that is
going to be described in the next section.
3.4 Initial Working Prototype
The overall architecture of the system is shown on
figure 2. The central device is an android
smartphone where the specific software is installed.
The application includes a local SQLite database
where all the configuration and control information
is stored. The app makes use of phone resources as
the camera and the NFC reader. The camera is used
to add a photograph of the medicament as
configuration information. The NFC reader is
indispensable to control the medication intake with
the tagged pill container. This device must also be
able to connect to a provider’s mobile network to
send a warning by SMS when the process goes
wrong.
There are two main modes of operation. One is
intended to people used to working with mobile
apps. The second one allows controlling the
medication intake just by approaching the phone to
the medicament and confirming the process using
simple voice commands.
The first mode of operation begins with patient
selection. Next, three possible actions are accessible:
configuration, intake-control and reports. The
configuration function allows to introduce the
HEALTHINF2015-InternationalConferenceonHealthInformatics
280
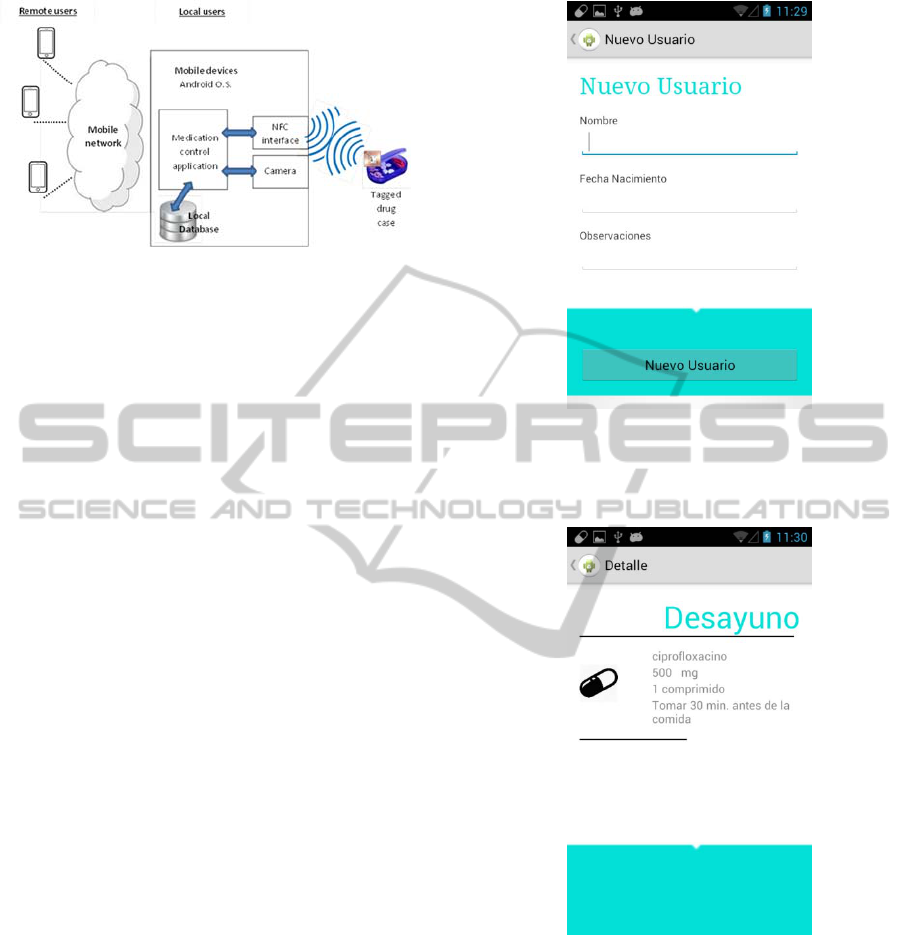
Figure 2: System architecture.
general information of a drug and to define intakes.
To adapt to the two both studied profiles, two kinds
of intakes can be configured:
Single medicament.
Pillbox.
To determine an intake one or more (in the case
of pillboxes) medicaments are chosen and the
dosage (amount and time) fixed. It is also possible to
define an alarm for the patients and to stablish the
criteria that will result in the dispatch of an SMS.
The configuration of an intake ends after the
relevant data are saved into NFC tag. This tag is
attached to the medicament box or to the pillbox. In
figures 3 and 4 the interface to introduce patient’s
data and the information summary of a configured
intake respectively are shown. So far, Spanish is the
only language covered.
In figure 5 the flowchart for the control function
is shown. The data saved inside the tag memory are
the name of the medicament (or the identification of
the pillbox case), the patient that must take it and the
date of the last three intakes. The information about
user, drug and time from both, NFC and local
database are cross checked to decide if the action is
correct and warn to the patients if an error is about to
happen.
Finally, user can access to a report screen that
collects and show information corresponding to a
date and medicament chosen by the user.
The second mode of interaction only allows to
access to the control function. When the patient
approaches the smartphone to the labelled
medicament, the application opens directly the
control screen for the patient whose data are
included in the NFC memory. A voice command, as
a welcome message, names the patient that can
check if the context defined by the data recovered
from the NFC tag (patient, medicament, last intake)
corresponds to the actual situation. All the warning
and confirmation interactions will be performed by
simple voice commands. It could be said that the
Figure 3: Patients’ data configuration screen. New user’s
(nuevo usuario) data must be provided: Name (nombre),
date of birth (Fecha Nacimiento) and comments
(Observaciones).
Figure 4: Intake information summary. We can see the
instructions for the breakfast (Desayuno) intake.
user is not aware that the device he is handling is a
smartphone, but it is just the bridge to a natural,
simple interaction with the system that eases the
process of medication. At this stage, an experienced
user must help with the configuration function.
AutomaticPreventionofMedicationErrors-MobileSystemBasedonNearFieldCommunication(NFC)Technology
281
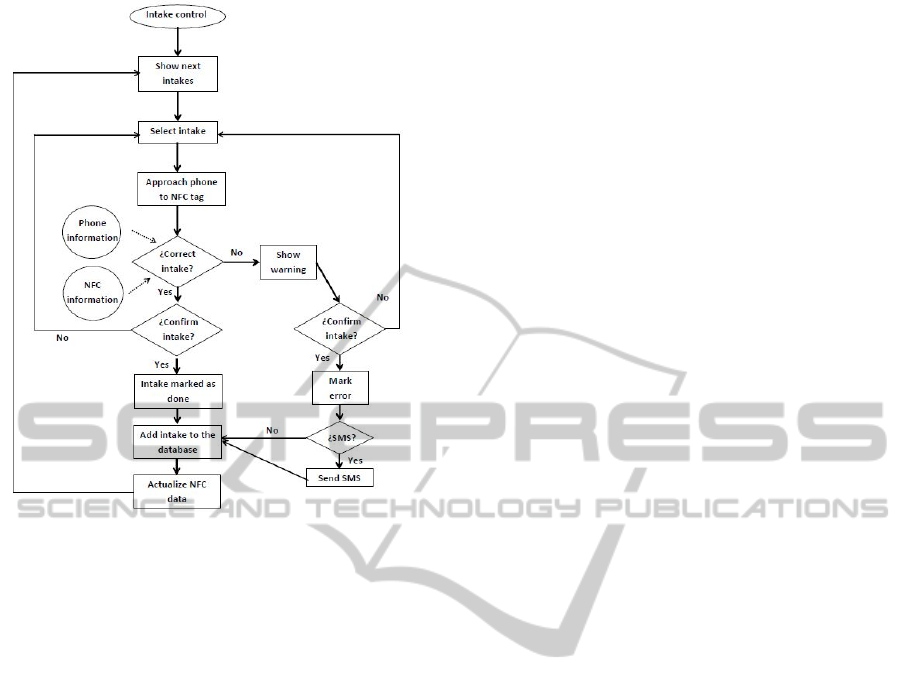
Figure 5: Flowchart of the control function.
4 CONCLUSIONS AND FUTURE
STEPS
The use of radiofrequency identification to prevent
incidents in the medication process has been widely
used in both, hospital and home environments. The
configuration of the RFID tags and devices was
generally done by doctors or pharmacists. All the
elements involved were integrated in the complex
hospital information systems and cannot be used by
patients and caregivers in an independent way. One
of our main aims is to allow patients themselves to
configure the system, as long as they are provided
with NFC tags. Smartphones applications for
adherence control are specially intended for the
personal or familiar care, but cannot control that a
drug is mistaken because there is no automatic data
cross-checking as our system in a novel way
implements. The NFC information prevents that a
drug can be confused with another or that a patient
takes a medicament not prescribed to him. In an
emergency, if the phone is operative, a complete 24-
hours report can be consulted. One of the main new
contribution of our systems is that, even if it is
impossible to collect the information saved in the
phone (for example, patient unconscious, phone
turned off and no one knowing the password) the
data stored in the NFC tag will confirm if a specific
intake was done or not. The data stored in the NFC
tag are written following the NFC Data Exchange
Format (NDEF) and can be read by the basic NFC
apps installed in every NFC device.
Our application is flexible and adapts to patients
that takes medication sporadically and to chronic
polymedicated patients as different kinds of intakes:
single medicament or pillbox are possible. Besides,
the control action has been designed in order to
reduce the cognitive load required to accomplish the
task. The use of NFC as well as a simple speech
recognition system eases the human machine
interaction. We hope that this interaction will be
natural enough to encouraged chronic patients to
integrate this tool in their everyday actions.
The main next step of our work is the system
evaluation by led users in order to get an improved
product that could be published in the android Play
Store. Our aim is to conduct a long term observation
of patients that use the app and patients who take
their medicines as usual. In this way, we can
measure the error reduction.
To reduce the digital knowledge required to
perform the configuration function, the information
about the drugs and their prescribed dose could be
automatically saved in the phone database from a
website controlled by doctors and/or pharmacists.
The device could save the selected data in the NFC
tag just by approaching to the medicament.
As recently the new iPhone 6 has NFC interface
(The Verge, 2014) the system could be also
developed in iOS platform.
ACKNOWLEDGEMENTS
This work was supported by Antonio Gargallo
University Foundation, Project 2014/B016 and by
Spanish Ministry of Economy and Competitiveness,
Project TIN2011-28169-C05-02.
We would also like to thank staff and members
of the Aragonese Parkinson Association (Delegation
of Teruel) for sharing their experiences with us.
REFERENCES
Agarawala, A. Greenberg, S. Ho, G., 2004. The context-
aware pill bottle and medication monitor. In: Sixth
International Conference on Ubiquitous Computing.
September 7-10 2004, Nottingham, England.
Germany: Springer.
Alabdulhaftih, M. Sampangi, R.V. Sampalli, S., 2013.
NFC-enabled smartphone application for drug
HEALTHINF2015-InternationalConferenceonHealthInformatics
282

interaction and drug allergy detection. In: 5th
International Workshop on Near Field
Communication (NFC). February 5, 2013, Zurich,
Switzerland. USA: IEEE, 1-6.
Bardram, J.E., 2004. Applications of ContextAware
Computing in Hospital Work – Examples and Design
Principles. In: ACM Symposium on Applied
Computing. March 14-17 2004, Nicosia, Cyprus.
USA: ACM Press.
Benjamin, D.M., 2003. Reducing medication errors and
increasing patient safety: case studies in clinical
pharmacology. Journal of Clinical Pharmacology 43
(7) 768–783.
Bravo, J. López de Ipiña, D. Hervás, R., 2013. RFID
breadcrumbs for enhanced care data management and
dissemination. Personal and Ubiquitous Computing
Journal 17 (6), 1095-1104.
Chen, YC. Hsieh, MF. Wang, CC. Lee, HR., 2007.
RFIDBased Intelligent Systems for Home
Healthcare. In: International Conference on Consumer
Electronics, ICCE 2007. January 10-14 2007, Las
Vegas, NV, USA. USA: IEEE.
Chien, HY. Yang, CC. Wu, TC. Lee, CF., 2011.
Two RFIDbased Solutions to Enhance Inpatient
Medication Safety. Journal of Medical Systems. 35
(3), 36975.
Darianian, M. Michael, M.P., 2008a. A Low Power
Pervasive RFID Identification System for Medication
Safety in Hospital or Home TeleCare. In: 3rd
International Symposium on Wireless Pervasive
Computing (ISWPC 2008), May 7-9 2008, Santorini,
Greece,. USA: IEEE, 143–146.
Darianian, M. Michael, M.P., 2008b. Smart Home Mobile
RFIDbased InternetOfThings Systems and
Services. In: International Conference on Advanced
Computer Theory and Engineering. December 22-28,
2008, Phuket, Thailand. USA: IEEE.
Engel, T. Koennings, M. von Heydebrand, N. Goswami,
S. Krcmar, H., 2013. A NFC-based Concept for
Medication Related Patient Services. In European
Conference on Smart Objects, Systems and
Technologies (SmartSysTech), 11-12 June, 2013,
Erlangen, Germany. USA: IEEE, 1-10.
Glover, B. Himanshu B., 2006. RFID Essentials (Theory
in Practice) O'Reilly Media, Inc. Sebastopol.
Iglesias, R. Parra, J. Cruces, C. Gómez De Segura, N., 2009.
Experiencing NFC-based Touch for Home Healthcare. In:
International Conference on Pervasive Technologies
Related to Assistive Environments - PETRA 2009 9-13
June, 2009, Corfu, Greece. USA: ACM Press, 1-4,
Lahtela, A., Hassinen, M. Jylhä, V., 2008. RFID and NFC
in Healthcare: Safety of Hospitals Medication Care.
In: Pervasive Computing Technologies for
Healthcare. January 30 – February 1, 2008,
Tampere, Finland. USA: IEEE.
Lai, CH. Chien, SW. Chang, LH. Chen, SH. Fang,
K., 2007. Enhancing Medication Safety and
Healthcare for Inpatients Using RFID. PICMET 2007,
August 5-9, 2007 Portland, Oregon USA. USA:
PICMET.
Morisky D.E., Green L.W., Levine D.M., 1986.
Concurrent and predictive validity of a self-reported
measure of medication adherence. Medical Care 24
(1). 67-74.
NCCMERP. National Coordinating Council for
Medication Error Reporting and Prevention, 1998.
NCCMERP Taxonomy of medication errors.
http://www.nccmerp.org/aboutmederrors.htm Last access
July 2014.
Oztekin, A. Pajouh, F.M. Delen, D. Swim, L.K., 2010. An
RFID network design methodology for asset tracking
in healthcare. Decision Support Systems 49, 100–109.
Pasto, L. Masuet, C. Bara, Castro, I. Clopés, A. Pàez, F.
Schönenberger, J.A. Gorgas, M.Q. Codina, C., 2009.
Estudio de incidencia de los errores de medicación en
los procesos de utilización del medicamento:
prescripción, transcripción, validación, preparación,
dispensación y administración en el ámbito
hospitalario. Farmacia Hospitalaria. 33 (5), 257268.
Qin, Z. Huang, G.Q. DAI, Q., 2011. No Room for Error:
RFIDenabled Smart PointofCare Medication
Process in Hospital Wards. In: 2011 IEEE
International Conference on RFIDTechnologies and
Applications. September 15-16, 2011Sitges, Spain.
USA: IEEE.
Resatsch, R. (2010) Ubiquitous Computing. Developing
and Evaluating Near Field Communication
Applications, Gabler Verlag. Heildeberg.
Sun, P.R. Wang, B.H. Wu, F., 2008. A New Method to
Guard Inpatient Medication Safety by the
Implementation of RFID. Journal of Medical Systems.
32 (4), 2732.
Swedberg, C., 2009.NFC Brings Visibility to British Home
Care.
http://www.rfidjournal.com/articles/view?5011. Last
access July 2014.
The Verge, 2014. iPhone 6 will reportedly feature NFC
and Apple's own mobile payments platform.
http://www.theverge.com/2014/8/28/6078359/iphone-
6-will-feature-nfc-and-apple-mobile-payments Last
access August 2014.
Vergara, M. Díaz-Hellín, P. Fontecha, J. Hervás, R.
Sánchez-Barba, C. Fuentes, C. Bravo, J., 2010.
Mobile Prescription: an NFC-based proposal for AAL.
In: Second International Workshop on Near Field
Communication. April 20, 2010, Monaco. USA: IEEE.
27 – 32.
AutomaticPreventionofMedicationErrors-MobileSystemBasedonNearFieldCommunication(NFC)Technology
283
