
Towards Guidelines for the Design of Patient Feedback
in Stroke Rehabilitation Technology
Lilha Willems, Daniel Tetteroo and Panos Markopoulos
Eindhoven University of Technology, Den Dolech 2, 5612 AZ Eindhoven, The Netherlands
Keywords: Design Guidelines, Assistive Technology, Arm-Hand Rehabilitation, Stroke, Data Visualization.
Abstract: Feedback is known to play a key role for the effective rehabilitation of patients after stroke. Although
general guidelines exist for UI design for people with physical and cognitive disabilities, and feedback
systems have been evaluated with non-disabled persons, little is known about how best to design feedback
for interactive technologies supporting rehabilitation after stroke. This paper describes the iterative design
process of a feedback module for TagTrainer, a tangible interactive tabletop technology supporting arm-
hand training. Based on the evaluation of this technology with seven stroke patients, we propose five
guidelines for the design of patient feedback for stroke rehabilitation technology.
1 INTRODUCTION
Stroke prevalence is on the rise, due ageing of the
population (Hochstenbach-Waelen and Seelen,
2012; Krebs et al., 1998; Timmermans et al., 2009).
As a result, the health system is under severe
pressure due to an increasing ratio of stroke patients
to therapists. It has been suggested that patients
could receive better healthcare and have a higher
quality of life by using interactive technologies for
rehabilitation. According to (Timmermans, 2010)
the use of technology in the rehabilitation has four
main benefits:
It can create opportunities for patients to train
more often
It can provide a variety of exercises
It can enable the patient to practice in absence of
the therapist
It reduces workload of the paramedical staff
Additionaly, interactive technology is well suited
for motivating, involving, and immersing stroke
patients in their rehabilitation (Burke et al., 2009).
Interactive technology has been an area of research
for getting stroke patients more involved in their
rehabilitation, which they may otherwise find
tedious and not stimulating due to its intense and
repetitive nature (Lövquist and Dreifaldt, 2006).
One way interactive technologies can get stroke
patients more involved and motivated to perform
exercises is by incorporating the use of feedback
(Burke et al., 2009; Wulf et al., 2010). It has been
shown that in game design feedback plays a crucial
role in achieving more effective engagement (Burke
et al., 2009). Feedback makes users aware of their
progress towards goals and how their actions impact
their progress. It provides users with a means to
accomplish their goals and when this information is
provided effectively, it enables users to
independently learn and improve their performance.
In addition, (Winstein, 1991) has shown that
feedback enhances learning and self-efficacy when it
is positve and encouraging.
The use of effective feedback is therefore an
important means for improving stroke rehabilitation
and enabling patients to practice independently.
Research suggests that the (extrinsic) feedback
provided by technology carries special importance
for stroke patients due to their compromised intrinsic
feedback system as a result of the stroke
(Timmermans, 2010; Van Vliet and Wulf, 2006).
Extrinsic feedback, when provided properly, can
improve stroke patients’ learning and increase their
active involvement, motivation, confidence and self-
efficacy (Timmermans, 2010; Wulf et al., 2010).
Although the positive effects of feedback on the
stroke recovery process are somewhat understood,
the design of feedback systems targetted specifically
at stroke patients is an underexplored, but emergent
and important area of research. Therefore, we
present an investigation into how to provide
60
Willems L., Tetteroo D. and Markopoulos P..
Towards Guidelines for the Design of Patient Feedback in Stroke Rehabilitation Technology.
DOI: 10.5220/0005201900600068
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 60-68
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

effective feedback to stroke patients using different
options for feedback content and modality. We
addressed this question by performing an
exploratory case study with seven stroke patients
using the TagTrainer system (Tetteroo, 2013). In this
paper we present the design process of a feedback
module for TagTrainer. Finally, we present
guidelines for providing feedback with stroke
rehabilitation technology that have been derived
from the design and evaluation of this module.
2 RELATED WORK
2.1 Recovery after Stroke
There is ample research on the effects of feedback
on motor learning in non-disabled persons.
However, to which extent these findings apply to
stroke patients is largely unknown. For one, the
intrinsic feedback system of stroke patients is
impaired (Timmermans, 2010; Van Vliet and Wulf,
2006; Winstein, 1991), while this system plays an
important role in motor learning of non-disabled
persons. In addition, it has been suggested by
(Krakauer, 2006) that stroke may cause learning
deficits in the patients. This suggestion implies that
stroke patients require a different approach for
learning motor skills; a task that is simple for a
non-disabled person may be complex for a stroke
patient.
Movement recovery after stroke is usually
attributed to two mechanisms (Cirstea and Levin,
2007; Krakauer, 2006):
True recovery: this occurs when the same
muscles for a certain activity are once again used
as before the stroke.
Compensation: this occurs when alternative
muscles are used as a strategy, different than
before the stroke, to perform an activity.
According to (Krakauer, 2006) learning is
required for both mechanisms to occur and in order
to achieve this, rehabilitation should emphasize on
learning different techniques to reach a certain goal
and not just repetition of the same movements.
2.2 Feedback in Stroke Rehabilitation
In general there has been little research on the
effects of feedback in motor learning following
stroke. Depending on the impairments caused by the
stroke, different feedback is needed to accommodate
the patients’ capabilities and to facilitate motor
learning. The feedback should be adjusted to the
patient's stage of learning (Timmermans, 2010).
It is commonly accepted that three factors play
an important role in transmitting feedback to stroke
rehabilitation patients: focus of attention, feedback
content and feedback scheduling (Van Vliet and
Wulf, 2006).
(Cirstea and Levin, 2007) conducted a study with
the objective to determine if the manipulation of the
attentional focus may lead to arm motor recovery
during a repetitive pointing training intervention. In
their experiment participants were either provided
with Knowledge of Results (KR) that directs
attention to performance outcomes (external focus of
attention) after every 5th trial, or with Knowledge of
Performance (KP) that directs attention to arm
movement patterns (internal focus of attention),
concurrently and on a fading schedule. The results
showed that the motor improvements in stroke
patients whom received KP reflect true recovery, in
contrast with those who received the KR feedback.
This suggests that if the goal of rehabilitation is true
recovery, stroke patients may benefit more from KP
feedback. However, in their review study, (Van
Vliet and Wulf, 2006) found research that suggests
that feedback inducing external attentional focus
may be more effective to improve performance of
task execution after a stroke. In the same study, (Van
Vliet and Wulf, 2006) found that additional verbal
KR is redundant when KR information is inherent to
the task. When this is not the case, they found that
summary or average feedback benefits motor
learning of stroke patients.
For stroke rehabilitation, (Burke et al., 2009)
believe that feedback concerning failure should be
more conservative, and successful engagement
should be rewarded and encouraged. Furthermore
(Timmermans, 2010) argues that it is important to
give feedback concerning motor control as this
enhances learning, positively influences motivation,
self-efficacy, and compliance. Correct performance
feedback increases motivation while incorrect
performance feedback facilitates learning.
As for feedback scheduling, (Van Vliet and
Wulf, 2006) found that providing reduced feedback
to stroke patients may enhance learning. Apart from
this finding, little is known on how feedback
scheduling influences learning in stroke patients.
2.3 Designing for Impaired Persons
Older people form the majority of stroke patients. In
the U.S. nearly 75% of stroke patients are over the
age of 65. In fact after the age of 55 the chances of
TowardsGuidelinesfortheDesignofPatientFeedbackinStrokeRehabilitationTechnology
61

stroke doubles with every decade (Krakauer, 2006).
Given these statistics it is important to consider how
older people interact with technology, as they
generally experience a decline in sensory, cognitive,
and motor functions that can interfere when
interacting with technology (Ijsselsteijn et al., 2007;
Kurniawan and Zaphiris, 2005). In addition, even
though stroke is prominent in older people, it can
occur at any age and its consequences can also
induce cognitive- and motor impairments amongst
younger stroke patients.
The study of (Kurniawan and Zaphiris, 2005)
yielded several guidelines for designing websites for
older people. When applying those guidelines for
use in arm-hand rehabilitative technology the
following guidelines need to be considered:
Language should be simple, clear, and to the point.
Important information should be highlighted.
Irrelevant information causes too much distraction
for users with cognitive impairments.
Text design should be static, and presented in a
readable format with high contrast. With age the
color- and contrast sensitivity declines (Ijsselsteijn
et al., 2007).
Graphics should relevant and easy to understand.
Navigation cues should clear and provide current
location of the page.
These guidelines contribute to dealing with
limitations in vision and cognition, by which stroke
patients are often affected. Especially for cognition
it is important that the interface is simple and
intuitive, and to contain the proper affordances to
reduce the workload of information processing
(Ijsselsteijn et al., 2007).
In their study, (Ijsselsteijn et al., 2007) also
recommend providing the same, redundant
information using different modalities in order to
compensate for visual and auditory limitations. In
addition to these limitations, during stroke
rehabilitation redundancy is also necessary for
cognitive limitations. It is not uncommon for
therapists to repeat instructions to their patients
and/or actively guide patients’ attention towards
important information.
To determine how to provide effective feedback
to stroke patients, a feedback module system for
stroke rehabilitation technology was designed and
evaluated with stroke patients in a case study
involving the TagTrainer stroke rehabilitation
platform.
3 CASE STUDY: PATIENT
FEEDBACK FOR
TAGTRAINER
3.1 TagTrainer
TagTrainer (Tetteroo, 2013) is a technology for arm-
hand training in stroke rehabilitation. It allows
patients to manipulate physical objects (e.g. lift,
place, rotate) on one or more interactive tabletop
surfaces – called ‘TagTiles’ – that are connected to a
computer. TagTrainer allows therapists to use
objects of daily life for rehabilitation training, since
the TagTiles are able to detect the presence, position
and orientation of these objects as long as these are
tagged appropriately with RFID tags. TagTrainer
guides patients through an exercise by lighting up
areas on the TagTile boards where objects have to be
placed, moved or picked up from. Furthermore, the
system provides both written and spoken
instructions. Finally, TagTrainer collects
quantitative performance data (e.g. speed of
execution, number of repetitions) through the RFID
sensors in the TagTile boards, as well as qualitative
performance data (torso compensation, shoulder
compensation, accuracy of object placement on the
TagTile boards) through the RFID sensors in the
board and accelerometers attached to the patient’s
torso and shoulders.
Figure 1: A patient and therapist using TagTrainer in
arm-hand rehabilitation therapy.
An example TagTrainer exercise would ask a patient
to repeat a few times the following steps:
Pick up a cup with her left hand and place it on a
TagTile.
Pick up the cup from a TagTile and raise it to the
level of another TagTile, positioned at a 90-
degree angle to the first TagTile.
Touch the upper TagTile with the cup and put it
back on the lower TagTile.
HEALTHINF2015-InternationalConferenceonHealthInformatics
62

While rich performance data is collected by
TagTrainer, none of this information is currently
presented to patients. Therapists still have to
manually guide patients through exercises and
provide feedback about their performance (see
Figure 1). Given the importance of feedback for the
recovery process of stroke patients, we set out to
develop a patient feedback module for TagTrainer
based on existing literature and user research.
3.2 User Research
In order to get a better idea of how rehabilitation
sessions are set up, how patients are instructed and
supported by therapists, how therapists determine
appropriate feedback, and how feedback is currently
provided to patients, we conducted two unstructured
interviews with stroke rehabilitation therapists and
observed an arm-hand training session at a stroke
rehabilitation clinic (Adelante Centre of Expertise in
Rehabilitation and Audiology, Hoensbroek, NL).
3.2.1 Interviews with Therapists
Two unstructured interviews were performed with
stroke rehabilitation therapists at the before
mentioned rehabilitation clinic. The goal of the
interviews was to get insight into how therapists set
up training sessions for their patients, and how they
guide and work with them during these sessions.
At Adelante, the rehabilitation process is strictly
patient-centered. The therapist sits down with the
patient and asks the patient about the problems (s)he
encounters. Together with the patient, the therapist
will determine the goals the patient wants to achieve.
According to one therapist establishing goals helps
to keep the patient focused. When the patient’s goal
cannot be achieved straight away, the therapist will
divide it into smaller sub-goals that are easier to
achieve.
During training sessions, therapists usually
provide encouraging verbal feedback. Additionally,
they may make use of mirrors, physical guidance or
other materials if the situation requires it. Therapists
do not apply a systematic approach in giving
feedback because of the differences between
individual patients. Feedback that works for one
patient may not be suitable for another. Therefore,
feedback is tailored to the patient by employing a
trial-and-error approach. Finally the feedback given
differs amongst the therapists and is based on their
previous experiences (i.e. observed best practices).
One therapist indicated that during rehabilitation
it should be clear to patients why they must invest in
certain tasks, and that feedback should primarily
concern the quality (speed, fluency, and trajectory)
of movement. The other therapist stressed the
importance of keeping patients motivated with
feedback. Both therapists agreed that it is important
that patients experience success and are able to
achieve their goal. Therefore the therapists would
sometimes relax on giving ‘negative’ feedback and
give more encouraging feedback instead.
3.2.2 Observation of Arm-hand Training
Session
The first author embedded herself in the Adelante
stroke rehabilitation clinic to observe a one-hour
arm-hand training session. During the training
session, one therapist attended to five patients. Three
of them were practicing daily tasks independently
and did not receive feedback from the therapist.
The other two patients practiced different tasks
that were repetitive in nature. These patients
received more attention from the therapist, who
helped them in placing a harness around their
affected hand. Once the patients started performing
their exercises, the therapist predominantly gave
positive verbal feedback on their performance. Other
times, the therapist gave tips on how the patients
could execute the task more easily.
At the end of the training session, the therapist
requested the patients to rate their performance on a
scale from 1 to 10. In addition to that, patients
needed to make and write down a plan of which
exercises they planned to practice with their affected
arm over the coming weekend. The plan needed to
be very specific on time, location and duration of the
exercises. The overall goal was that they would use
their affected arm at least one hour a day during the
weekend.
3.2.3 Design Implications
From the user research, we distilled the following
implications for the feedback module design:
For patient involvement and motivation the goal
and purpose of the exercise performed should be
clear to the patient.
Provided feedback should be primarily positive
and tailored to the patient’s needs.
The design should allow for trial-and-error
approach for giving feedback.
3.3 Designing Patient Feedback
Although TagTrainer supports stroke patients in
TowardsGuidelinesfortheDesignofPatientFeedbackinStrokeRehabilitationTechnology
63

their training by providing them with instructions for
the execution of exercises, the current system does
not offer them feedback on their performance.
Therefore, we designed a patient feedback module
for TagTrainer that would provide stroke patients
with relevant feedback on their performance. Here
we present the final design, and then discuss relevant
experiences gathered during the design process and
from evaluations.
3.3.1 Method
The feedback module was designed in a user-
centered iterative process consisting of three
consecutive design-implement-evaluate cycles.
Initial design choices were based on suggestions
from previous research involving non-disabled
persons (e.g. (Shea and Wulf, 1999; Van Vliet and
Wulf, 2006)) and older people in general (e.g.
(Ijsselsteijn et al., 2007)), and the user research
reported on earlier in this paper.
During the evaluation sessions, patients
performed an exercise on the TagTrainer board. The
exercise required the participants to trace a diagonal
line 5 times with the affected arm using a small
(2x2x2 cm) wooden cube. While the exercise was
performed, the feedback module was presented on a
separate display in front of the user. The same
exercise was used throughout the design process.
After executing the exercise, the participants
were asked in an open interview questions
concerning their understanding of the displayed
information, which information felt to be missing or
redundant, and the perceived value of the
information presented.
3.3.2 Participants
The feedback software was evaluated with seven
stroke patients undergoing general arm-hand
rehabilitation at the Adelante Centre of Expertise in
Rehabilitation and Audiology, Hoensbroek, NL. The
age of the participants ranged between 50 and 83
years. The time since their stroke and the evaluation
ranged between weeks to a couple of months. All
participants were affected in their motor skills,
mostly affecting their upper extremities and gate,
and some participants were affected in their balance,
memory and visual capabilities.
3.3.3 Design
The feedback module designed aims to provide
relevant feedback throughout the patients' training
session. A session consists of a movement activity
that a patient needs to practice repeatedly for either a
fixed number of times, or for a given duration.
Sessions consist of individual trials: single units of
meaningful movement that the patient needs to
repeat during the session (e.g., the exercise
described above).
The feedback module was designed to guide
patients during the entire exercise session and thus
consists of four main screens. These screens are
shown 1) before the start of an exercise session, 2)
during the session, 3) after every block of 5 trials,
and 4) at the end of the session respectively (see
Figure 2).
The screen shown at the start of the session
(Figure 2-A) contains the exercise instructions and
its benefits. The instructions are presented as a series
of short sentences that are formulated in simple
language and displayed in a readable font. Benefits
are shown here because the therapists interviewed
during the initial design phase suggested that it will
motivate users to engage in the exercise.
While the patient is executing a block of 5 trials,
the feedback module shows the patient instructions
for the exercise and the patient’s progress in
completing the block (Figure 2-B). The reduced
feedback scheduling of 5 trials was chosen for
providing feedback during the session, because
(Cirstea and Levin, 2007) reported it to work well
for stroke patients.
After each block of 5 trials the feedback module
shows bar graphs with performance information
about those 5 trials (Figure 2-C). The bar graphs
denote the duration of every trial, and shoulder- and
torso-compensations performed during the trials.
The time measure was included because therapists
indicated that it will challenge and motivate patients
who are doing well in their rehabilitation. However,
for those who are not, the therapists fear it will
demotivate patients to perform the exercise.
Shoulder- and torso compensation measures were
included as they are major factors in arm-hand
rehabilitation. However, as is the case for the time
measure, these measures do not always apply to all
patients. The graph type denoting the performance
measures was decided upon together with the
therapists. The actual numbers of the performance
measures are not shown, as it is the pattern of the
results that gives the most important information,
according to the therapists interviewed in the initial
design phase. Textual KP-feedback is given for each
performance measure that either tells the user to
keep doing what he is doing, or how he can improve
HEALTHINF2015-InternationalConferenceonHealthInformatics
64
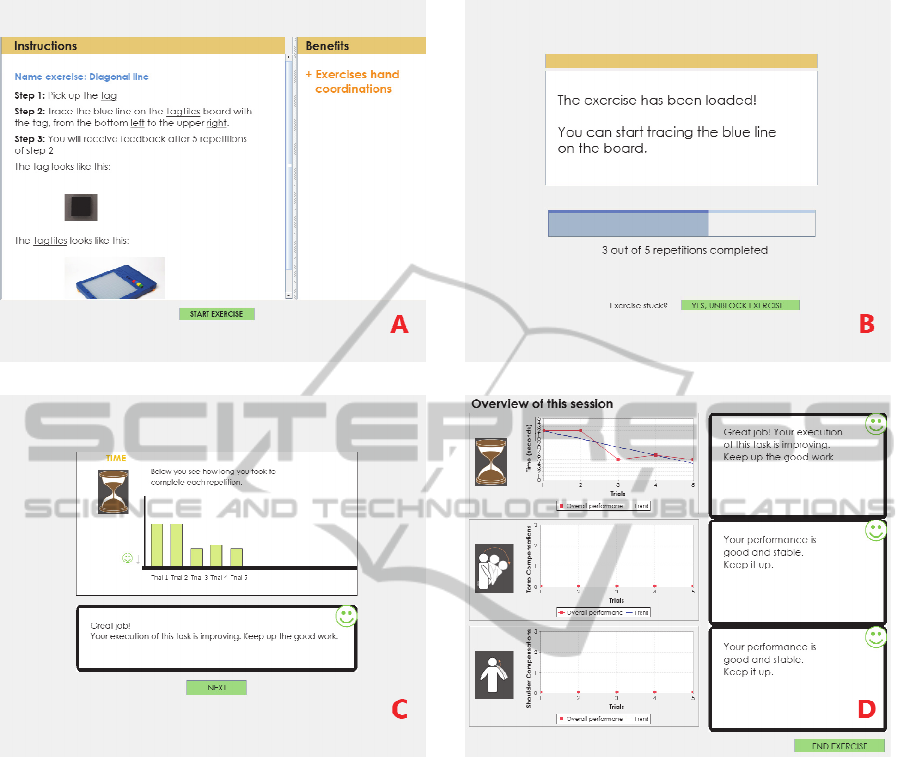
Figure 2: Screenshots from the feedback module: A) before the start of a session, B) during exercise execution, C) after
each block of 5 trials, D) at the end of the exercise.
his performance. In telling the user how to improve
his performance it only gives feedback concerning
the desired outcome and not how the user should
perform the movement to get to the desired outcome.
This induces an external locus of control and should
lead to enhanced learning (Shea and Wulf, 1999;
Van Vliet and Wulf, 2006; Wulf and Lewthwaite,
2010).
Finally, after a patient completes the entire
session, (s)he is presented with an overview of their
performance on execution time, shoulder- and
torso-compensation throughout the session, as well
as with appropriate KP-feedback (Figure 2-D).
3.3.4 Evaluation Results
Three factors play an important role in transmitting
feedback to stroke rehabilitation patients: feedback
content, feedback scheduling and focus of attention
(Van Vliet and Wulf, 2006). Given that the focus of
attention and scheduling of the feedback were not
varied in our study, we will not further report on
these. However, in addition to ‘traditional’ feedback
that is provided by therapists directly, we have used
several modalities for transmitting our feedback to
the participants and hence also report on results
concerning this factor.
3.3.4.1 Feedback Content
In the initial design of the screen shown before the
start of the exercise, performance results of earlier
sessions were included to show progress and hence
increase patient motivation. However this
information was found to be irrelevant and
distracting by the users as they were only concerned
with the task at hand: performing the exercise.
TowardsGuidelinesfortheDesignofPatientFeedbackinStrokeRehabilitationTechnology
65

Therefore, the information in this screen was limited
to the exercise instructions.
Instructions are shown again on the second
screen, in case the patient does not remember
exactly the nature of the task. The instructions on
this screen are presented in a condensed form, in an
attempt to reduce the amount of information the
patient needs to process while performing the
exercise. However, condensing the information
comes at the expense of less clarity of the
instructions and as a result one patient did not know
anymore how to perform the exercise.
After each block of five trials, the patients are
presented with graphs visualizing their performance
for those 5 trials. Initially the graphs were all shown
in one screen. However, during the evaluations one
participant indicated that he did not understand the
feedback information on this screen, even after
explanation. When the participant was prompted to
comment on the individual components on the
screen, including the bar chart, it turned out that the
participant did actually understand the information,
despite his initial claim of not being able to do so.
The problem was one of information density, and it
was decided to spread the information by giving
each graph its own screen that the users can leaf
through. This adjustment was included in the final
prototype and five participants indicated to perceive
less problems understanding the information on the
screen, compared to previous versions.
3.3.4.2 Feedback Modality
During the evaluations we observed that the system
at times failed in directing the users’ attention
properly. Two participants were reading the
instructions on the start screen and tried to execute
the exercise on the TagTrainer board before they
pressed the button to start the exercise. More
generally, most participants were confused about
when to look at the screen, and when to look at the
TagTile board. One participant mentioned that he
would prefer having the feedback on the TagTile
board instead of a separate computer screen. He
explained that during training he was focused on the
exercise task on the board and did not feel inclined
to constantly look back at the computer screen for
performance feedback.
For six participants it was not immediately clear
what was represented with the feedback shown as
bar graphs (see Figure 2-C). Participants found the
icons depicting the different types of feedback were
not self-explanatory enough. In addition, participants
reported that they felt the information shown should
be related to their personal context. It should
explain, for example, why certain feedback
information is important for them to know and what
it says about their performance. During the
evaluation five participants explicitly mentioned a
desire for information about their performance that
is relevant to their current situation.
Despite the participants not fully understanding
the graphs, the accompanying summary text (i.e.
KP-feedback) was clear. The participants stressed
the importance of the text containing information
about what is good or not good about their
performance. However, written information posed a
problem for four participants, as they were unable to
comprehend the written information due to poor
eyesight and cognitive limitations. However, once
the written information was vocalized, these
participants were able to grasp its meaning.
4 TOWARDS GUIDELINES FOR
PATIENT FEEDBACK
Based on experiences from the design process and
the results of the evaluations, we identified the
following set of design guidelines for feedback in
interactive stroke rehabilitation technology:
Provide Multimodal Information: Account for
sensory impairments that stroke patients might
have. E.g., vocalizing textual information for the
visually impaired (Ijsselsteijn et al., 2007). In
addition, providing multimodal information
enhances understanding and learning. E.g.,
during the evaluations vocalizing textual
information made it easier for stroke patients to
understand the information.
Provide Stepwise Guidance: Providing a
stepwise guidance through exercise instructions
alleviates the workload on the memory as it
provides information in more digestible bits.
Furthermore, providing a stepwise guidance
through the feedback will also improve a
patient’s understanding of the system.
Provide Context Related Information: The
feedback information presented should be
relevant to the patient's situation and
performance. If the information is not relevant,
the patient will lose motivation.
Prevent Information Overflow: It is easier for
stroke patients to process information when it is
provided to them in smaller bits. A means of
doing this is by only showing information that is
HEALTHINF2015-InternationalConferenceonHealthInformatics
66

relevant for the task at hand and by using short
sentences and simple language.
Allow for Customization: There is a great
variety in the disabilities that stroke patients may
have, and thus their individual needs for
feedback show an equal variation. Therefore, it is
crucial that feedback systems allow for
customization of feedback modality, scheduling
and content. So even though a stepwise
guidance, short sentences, and simple language
are recommended in general, there are patients
who want and can understand more complex and
related additional information about their
performance. By tailoring feedback to the needs
of individual patients, their motivation and
involvement in the exercise can be increased
(Timmermans et al., 2009).
5 DISCUSSION
In this paper we have presented the design and
evaluation of a patient feedback module for the
TagTrainer rehabilitation technology. Although our
evaluations have been performed with a limited
number of participants, we believe that the
experiences from our design process and the
findings from our evaluations provide useful
pointers to developers of interactive technologies for
stroke rehabilitation.
Although we believe that our guidelines contain
useful pointers for designers of interactive stroke
rehabilitation technology, we realize that the list of
guidelines is probably not complete. That is, these
designers should also take into account guidelines
that have been specified for other, related target
groups such as older people (e.g., (Ijsselsteijn et al.,
2007)).
The system that we have presented can be used
to further explore and research the effects of
feedback on stroke patients. The setup can also be
used in practice, as it allows therapists to employ
their trial-and-error approach in finding out what
works for their patient.
6 CONCLUSIONS
Providing feedback to stroke patients about their
performance in therapy is crucial to their recovery
process. However, due to cognitive damage
sustained by stroke, stroke patients’ information
processing is often impaired and their retention
limited. The contributions of this paper are the
design of a feedback module for TagTrainer, an
interactive stroke rehabilitation technology, and a set
of design guidelines for interactive stroke
rehabilitation technology that are based on
experiences we had, and evaluations we performed
during our design process.
These design guidelines address the specific
needs and account for the cognitive limitations that
stroke patients might have. We invite the community
to extend and validate these guidelines, in order to
improve the quality of technology supported stroke
rehabilitation, and eventually the quality of the lives
of people who are affected by stroke.
ACKNOWLEDGEMENTS
We acknowledge the support of the Innovation-
Oriented Research Programme ‘Integral Product
Creation and Realization (IOP IPCR)’ of the
Netherlands Ministry of Economic Affairs. In
addition, we would like to thank Adelante Centre of
Expertise in Rehabilitation and Audiology, and in
particular the therapists and patients who
participated in the design and evaluation of the
feedback module.
REFERENCES
Burke, J.W., McNeill, M.D.J., Charles, D.K., Morrow,
P.J., Crosbie, J.H., McDonough, S.M., 2009.
Optimising engagement for stroke rehabilitation using
serious games. Vis Comput 25, 1085–1099.
doi:10.1007/s00371-009-0387-4.
Cirstea, M.C., Levin, M.F., 2007. Improvement of arm
movement patterns and endpoint control depends on
type of feedback during practice in stroke survivors.
Neurorehabilitation and Neural Repair 21, 398–411.
Hochstenbach-Waelen, A., Seelen, H.A., 2012. Embracing
change: practical and theoretical considerations for
successful implementation of technology assisting
upper limb training in stroke. Journal of
neuroengineering and rehabilitation 9, 52.
doi:10.1186/1743-0003-9-52.
Ijsselsteijn, W., Nap, H.H., de Kort, Y., Poels, K., 2007.
Digital Game Design for Elderly Users, in:
Proceedings of the 2007 Conference on Future Play,
Future Play ’07. ACM, New York, NY, USA, pp. 17–
22. doi:10.1145/1328202.1328206.
Krakauer, J.W., 2006. Motor learning: its relevance to
stroke recovery and neurorehabilitation. Curr. Opin.
Neurol. 19, 84–90.
Krebs, H.I., Hogan, N., Aisen, M.L., Volpe, B.T., 1998.
Robot-aided neurorehabilitation. IEEE Trans Rehabil
TowardsGuidelinesfortheDesignofPatientFeedbackinStrokeRehabilitationTechnology
67

Eng 6, 75–87.
Kurniawan, S., Zaphiris, P., 2005. Research-derived Web
Design Guidelines for Older People, in: Proceedings
of the 7th International ACM SIGACCESS
Conference on Computers and Accessibility, Assets
’05. ACM, New York, NY, USA, pp. 129–135.
doi:10.1145/1090785.1090810.
Lövquist, E., Dreifaldt, U., 2006. The design of a haptic
exercise for post-stroke arm rehabilitation.
Shea, C.H., Wulf, G., 1999. Enhancing motor learning
through external-focus instructions and feedback.
Human Movement Science 18, 553–571.
doi:10.1016/S0167-9457(99)00031-7.
Tetteroo, D., 2013. TagTrainer: a meta-design approach to
interactive rehabilitation technology, in: End-User
Development - Fourth International Symposium,
Lecture Notes in Computer Science. Presented at the
IS-EUD 2013, Springer, Copenhagen, Denmark.
Timmermans, A., Seelen, H., Willmann, R., Kingma, H.,
2009. Technology-assisted training of arm-hand skills
in stroke: concepts on reacquisition of motor control
and therapist guidelines for rehabilitation technology
design. Journal of NeuroEngineering and
Rehabilitation 6, 1. doi:10.1186/1743-0003-6-1.
Timmermans, A.A.A., 2010. Technology-Supported
Training of Arm-Hand Skills in Stroke. Eindhoven
University of Technology, Eindhoven, the
Netherlands.
Van Vliet, P.M., Wulf, G., 2006. Extrinsic feedback for
motor learning after stroke: what is the evidence?
Disabil Rehabil 28, 831–840.
doi:10.1080/09638280500534937.
Winstein, C.J., 1991. Knowledge of results and motor
learning--implications for physical therapy. Phys Ther
71, 140–149.
Wulf, G., Lewthwaite, R., 2010. Effortless motor
learning? An external focus of attention enhances
movement effectiveness and efficiency., in: Effortless
Attention: A New Perspective in Attention and Action.
MIT Press, Cambridge, MA, USA, pp. 75–101.
Wulf, G., Shea, C., Lewthwaite, R., 2010. Motor skill
learning and performance: a review of influential
factors. Med Educ 44, 75–84. doi:10.1111/j.1365-
2923.2009.03421.x.
HEALTHINF2015-InternationalConferenceonHealthInformatics
68
