
Self-serve ICT-based Health Monitoring to Support Active Ageing
Mobyen Uddin Ahmed
1
, Jesica Rivero Espinosa
3
, Alenka Reissner
4
, Àlex Domingo
5
,
Hadi Banaee
1
, Amy Loutfi
1
and Xavier Rafael-Palou
2
1
Center for Applied Autonomous Sensor Systems, Örebro University, Fakultetsg. 1, 701 82 Örebro, Sweden
2
Barcelona Digital Technology Centre, C/RocBoronat, 11, MediaTIC Building 08018 Barcelona, Spain
3
Technosite, Fundosa Group R& D., Madrid, Spain
4
Zveza Društev Upokojencev Slovenije Ljubljana, Slovenia
5
Institut de l'Envelliment, Universitat Autònoma de Barcelona, Sant Antoni Maria Claret, 171 E 08041 Barcelona, Spain
Keywords: Healthcare Service, Health Monitoring, Blood Pressure, Blood Glucose, Pulse Rate, Activity Monitoring,
Recommendation, Alarm.
Abstract: Today, the healthcare monitoring is not limited to take place in primary care facilities simply due to
deployment of ICT. However, to support an ICT-based health monitoring, proper health parameters, sensor
devices, data communications, approaches, methods and their combination are still open challenges. This
paper presents a self-serve ICT-based health monitoring system to support active ageing by assisting seniors
to participate in regular monitoring of elderly’s health condition. Here, the main objective is to facilitate a
number of healthcare services to enable good health outcomes of healthy active living. Therefore, the
proposed approach is identified and constructed three different kinds of healthcare services: 1) real time
feedback generation service, 2) historical summary calculation service and 3) recommendation generation
service. These services are implemented considering a number of health parameters, such as, 1) blood
pressure, 2) blood glucose, 3) medication compliance, 4) weight monitoring, 5) physical activity, 6) pulse
monitoring etc. The services are evaluated in Spain and Slovenia through 2 prototypical systems, i.e.
year2prototype (Y2P) and year3prototype (Y3P) by 46 subjects (40 for Y2P and 6 for Y3P). The evaluation
results show the necessity and competence of the proposed healthcare services. In addition, the prototypical
system (i.e. Y3P) is found very much accepted and useful by most of the users.
1 INTRODUCTION
With the advent of relatively easy to acquire digital
health sensors and the communication infrastructure,
health monitoring at home is becoming increasingly
popular. Such solutions present benefits for
healthcare providers by enabling a more frequent
and continuous monitoring of patients. Of equal
importance are the benefits to the primary users, e.g.
residents who are able to be aware of their own
health parameters and their trends. An important
question to be considered in parallel to technological
development is how to interface the information
obtained from the system to the users who may have
little technical or medical expertise.
This paper presents an iterative and user centred
design approach to develop an ICT health
monitoring system for use at home. The system
integrates a number of off-the-shelf sensors into a
larger Ambient Assisted Living (AAL) framework.
Focus in this paper is put on the integration of the
various sensor components and the presentation of
information via services to the end users. Such
services include summaries of health parameters,
indication of trends and notifications of deviations.
To validate the proposed approach, user evaluations
have been performed in two countries with a
selected group of elderly users. The work performed
in this paper is part of a larger project called
SAAPHO, whose aim is to integrate health, social
and security services seamlessly in the same
architecture. This paper focuses only on the health
services, their design, and evaluation. The evaluation
results show the necessity and competence of the
proposed healthcare services. In addition, the
prototypical system (i.e. Y3P) is found very much
accepted and useful by most of the users.
374
Ahmed M., Rivero Espinosa J., Reissner A., Domingo À., Banaee H., Loutfi A. and Rafael-Palou X..
Self-serve ICT-based Health Monitoring to Support Active Ageing.
DOI: 10.5220/0005213403740382
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 374-382
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
2 RELATED WORK
SOPRANO (Soprano, 2014) project aims to develop
smart ICT-based assisted living services with easy to
use interfaces for older people. PERSONA (Persona,
2014) aimed at advancing the paradigm of Ambient
Intelligence (Aarts, 2004) for the development of
sustainable and affordable solutions for the
independent living of elderly. Many other research
projects address the need of older people
independent living through promotion of active
ageing (Czaja, 2005) and healthy habits. AMICA
(Crespo et al, 2010) tries to emulate the medical
consultation at home: auscultation and interview.
CCE (Hanák et al, 2012) is a dementia solution,
which comprises of connectivity between the
different physical components, sensors, medication
dispenser, server, and Net TV. The H@H system
(Health@Home, 2014) gathers the wearable sensors
data, which continuously monitor patients’ physio-
pathological cardiovascular and respiratory
parameters. The HELP (Claas et al, 2012) project
proposes solutions to improve the quality of life of
Parkinson’s disease patients based on: a body sensor
and actuator network and home devices to monitor
the health parameters (e.g. blood pressure) and body
activity (e.g. to detect gait, absence of movement).
Another project IS-ACTIVE (Ruxandra et al, 2011)
emphasizes the role of the home as care
environment, by providing real-time support to
patients. PAMAP is another healthcare system
(Hendeby et al, 2010), which comprises information
acquisition and management. Other mentionable
AAL projects, which are currently dealing with
healthcare systems, are: REMOTE, ELF@Home,
Dalia, and eCAALIX that aim to be assistant
systems for daily life of elderly (Catalogue of
Projects, 2014). The authors in (Pantelopoulos and
Bourbakis, 2010; Alemdar and Ersoy, 2010; Banaee
et al, 2013) present reviews in the research and
development of the wearable sensor systems in
health monitoring. According to these reviews, most
of the works are focusing on sensor devices and
communication protocols, i.e. low-cost, energy-
efficient ad hoc deployment of multi-modal sensors
and Bluetooth, Zigbee, Wi-Fi, GPRS and 3G
network communications. Similarly, authors in
(Jovanov et al, 2005; Nee et al, 2008; Varshney,
2007) present their research on homecare monitoring
where they have shown how to receive sensor
measurements and represent these measurements on
a computer or mobile device. Moreover, in (Pansiot
et al, 2007; Ahmed et al, 2013a; Ahmed et al, 2013b;
Ahmed et al, 2013c; Ahmed et al, 2012) the authors
presented remote health monitoring systems for
elderly using wireless sensor devices. SAAPHO
aims for an ICT based healthcare solution where the
proposed services are essentially designed based on
the feedback obtained from the elderly and intended
for daily use.
3 THE ICT-BASED HEALTH
MONITORING SYSTEM
The proposed approach has identified the healthcare
services mainly in three different kinds of facilities
for each parameter: 1) real time feedback generation
service, 2) historical summary calculation service
and 3) recommendation generation service. The goal
of the Real Time Feedback Generation Service is to
provide a feedback message based on sensor
readings in real time.
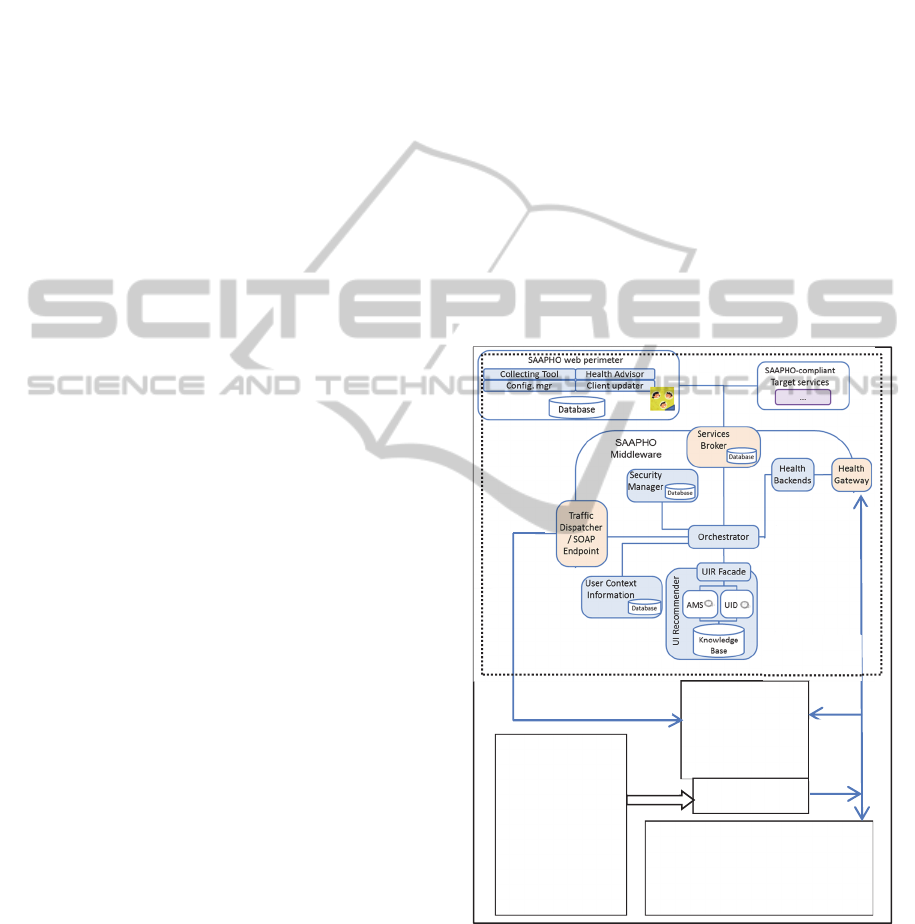
Figure 1: Architecture of the ICT-based health monitoring
system.
Here, a rule-based classification method is applied to
classify the measurements. For example, a blood
pressure measurement 142/92 mmHg could be
classified as “High blood pressure” and/or BMI 26.1
by measuring user’s weight
1
could be classified
User-Interface in
Android Tablet
Sensors are paired
through Bluetooth
AFEA
Health Intelligent Server (HIS)
Raw data measurements,
Classifications, Reminder status
Alarm status, Generate feedback on
measurement, Prioritization, etc
Health Sensor
Unit
Blood Pressure
Activity
Blood Glucose
Medication
Compliance
Pulse Monitoring
Weight Monitoring
Collector is in
Android device
Commun
ication
via
Bluetooth
https & SOAP communication
https &
SOAP
communi
cation
https & SOAP communication
AAL
architecture
Self-serveICT-basedHealthMonitoringtoSupportActiveAgeing
375

“Overweighed”. A set of rules used in the
classification method is mainly collected from the
literature study (MCMS, 2014; eCAP, 2014;
Culhane et al, 2005; Alberti et al, 1998;
Understanding blood pressure, 2014; Why exercise,
2014; Deurenberg et al, 1991), which is further
validated through healthcare practitioners. The
historical summary calculation service calculates
historical summary on a daily and weekly basis. The
goal of this service is to provide to the user a
possibility to see and compare the summary in a
graph for a specific range of dates. In order to
calculate the summary, the service will use raw data
measurements and the classification. This service
mainly considers the frequency of classes and the
number of total measurements. For example, in
order to monitor medication compliance it calculates
“total number of medication is taken”, “total number
of medications”, and “total number of medications
are skipped”.
The main objective of the Recommendation
Generation Service is to generate a recommendation
including reminder and alarm based on user’s
historical summary and raw data measurements.
Eight different kinds of recommendations are
implemented: 1) Devices_Not_Used is generated if
there is not any received measurement over one
week duration, 2) Medications_skipped is generated
if the number of medications skipped and the
number of medication that should be taken in a day
is equal, 3) Out_Of_Normal_Range is generated if
70% of the measurements classes are outside the
normal range considering a week, 4) Fluctuation is
generated if the measurements over a week show
fluctuation in more than 70% of the cases, 5)
Weight_Loss is generated if the current weight is
less than 3 kg comparing to the previous weight (3
months ago), 6)
Weight_Increased/Weight_Decreased is generated
considering one month measurements and a
calculated slope value, 7)
Activity_Increased/Activity_Decreased is generated
considering one week measurements and a
calculated slope value, 8) A monthly summary is
generated based on the raw measurements where
statistical features i.e. maximum, minimum, average
and standard deviation for each week are calculated.
The detail about the healthcare services can be found
in (Ahmed et al, 2014). The architecture of the
proposed ICT-based health monitoring system is
presented in Figure 1.
As it can be seen from Figure 1, the architecture
is divided into two parts, i.e. the AAL (Ambient
Assisted Living) and the rest. The AAL
architecture
(presented in chapter 3.1) is used as a core
framework of the proposed ICT-based health
monitoring system. Here, AAL architecture is
connected with the rest of the components of the
health system via the user interface and the Health
Gateway. The Health Sensor Unit contains of six
health’s related preventive parameters recommended
from the user requirements stage. Different
commercial Bluetooth sensor devices were acquired
to provide those parameters, for example, the blood
pressure and weight monitoring devices are
collected from a third party vendor OMRON
2
and
BeneCheck
3
and others are in-house products
provided by the partner IZM
4
which are under
development. These sensor devices are paired with
an android tablet device where it runs the User-
Interface and the Collector. The Collector receives
health measurements using Bluetooth Classic and
Low Energy (BLTE) communication from the
sensor devices upon user request through the User-
Interface. The Collector is based on native Java
source code, which is in general the main
programming language for Android devices.
Adaptive Front-End Application (AFEA) is the
main module in the user interface (UI) application,
which is in charge of handling the user interactions
and of presenting the information in a way indicated
by the AAL architecture. The interaction of the user
with the UI involves, in some cases, requests for
information to the TD (Traffic Dispatcher) for
obtaining all the information requested by the user
or needed by the device for presenting a correct
interface for the specific user. As soon as the
Collector receives the measurements it transfers
them to the Health Gateway through https protocol
and SOAP web service communication. The
measurements are sent as a zip file including
timestamps, battery and some other related
information. The User-Interface developed to be
delivered through Android tablets given their low
cost, portability, direct interaction and ease of use.
The Health Gateway mainly conveys the messages
among the Collector, Health Intelligent Server (HIS)
and Middleware. It classifies the measurements,
calculates priority, asks the HIS for the message ID
and finally forwards the data to the Middleware
through Health Backend (presented in chapter 3.1).
The HIS stores all the raw measurements and
generates message ID for the communication. It also
calculates daily and weekly historical summary and
stores them in a MySQL database. The user has a
direct access to HIS to see the historical summary
through the User-Interface. HIS also generates
recommendation in weekly basis based on historical
HEALTHINF2015-InternationalConferenceonHealthInformatics
376

summary and raw data measurements. The generated
recommendations are sent to the user through Health
Gateway, Health Backend and Middleware.
3.1 AAL (Ambient Assisted Living)
Architecture
The main objective of the AAL (Ambient Assisted
Living) architecture throughout the SAAPHO
project is to be accessible, adaptable, context-aware,
interoperable, ubiquitous, scalable, and to be able to
answer the requests of the User-Interface and of the
health connected to it in an efficient way. With the
collected ones that were published in (Doménech et
al, 2013), architecture was designed based on the
INREDIS architecture (INREDIS, 2014) and on the
reference architecture of universal (UNIVERSAAL,
2014).
Traffic Dispatcher (TD) takes the requests of the
user formalized by the AFEA about different types
of information and obtains the response from the
AAL architecture. These requests could be:
login/logout of the user, obtain adaptations, obtain
messages of the different services connected to
SAAPHO or obtain URLs of external services.
Among all of them, those relevant for the health
services are the following:
- Obtain messages related to health. These
messages are stored in the TD after they are
received from the AAL architecture (sent by
the User Interface Recommender or by the
Health Gateway) and until AFEA asks for them
and indicate to the TD that they have been
shown to the user.
- Obtain the URL of the Health Gateway. This is
useful to the AFEA to know where it has to
send the measures taken by the Collector in the
user’s device.
- Obtain URLs with information of healthy
habits. While the previous request of URLs is
done by the AFEA, the user does this request.
User Interface Recommender (UIR) indicates the
way in which the information should be presented to
the user through the User-Interface, sends messages
with generic recommendations, recommendations
related to the services connected to the AAL
architecture, or recommendations of new direct
accesses to social tools. This component has a
database that contains the information that could be
useful for the generation of recommendations of
information to be shown to the user and the
information about the appearance of the interface
(Character size, symbols used, font type, background
colour…) that the user selected in the Settings
section of the User-Interface. In relation to the
health services, the UIR stores the recommendations
send by the Health Gateway, and they are used for
generating recommendations for promoting active
and healthy ageing considering the historical list of
recommendations of the user. For example, the UIR
can send a congratulation message when the level of
a specific parameter is good during a period of time
or send general advices for having a healthy life.
Together with the generation of recommendations,
the UIR is also in charge of creating the textual
messages that are included in the health messages to
be presented to the user in a suitable way. For this,
the UIR studies the type of message, the gender, the
language and the name of the user, and creates the
text adapted to these characteristics. This text will be
included in all the messages received from the
Health Gateway. This component and the AFEA
component are the UI Model and the User
Interaction Management modules of universAAL
(Sala et al, 2013)
Services Broker (SB) hosts a registry of
descriptions of the services inside the AAL
architecture but also of other services that could be
useful for the users. Together with the storage of the
information of these services, the SB also allows to
link the user with them when he/she requests for a
type of information (for example, online health
newspaper), such as the SB makes a search of a
specific service that satisfies the topics indicated by
the user and that is more suitable for the profile of
the user. This makes the platform accessible from a
cognitive point of view, because the user, for
example, does not need to know the name of the
newspaper; he/she just says that he/she wants to read
sport news. To do this, the Services Broker has also
a database of users and their profiles and the
searches done by them. This database is constantly
updated with the new searches of the users and with
new entries of services in the catalogue. The
functionality of the Context Management and of the
Service Management in universAAL is included in
the SB (Sala et al, 2013).
The Orchestrator is the module in charge of
abstracting all the dependencies among all the other
modules of the architecture. This module redirects
the communication from one module to another,
decoupling each module from the rest, making the
modules independent from each other.
Security Manager (SM) controls the access of the
users and gateways to the system generating
SessionIDs. To do that, it has a cyphered database
with the information of the user, it generates
Self-serveICT-basedHealthMonitoringtoSupportActiveAgeing
377

SessionIDs, and controls that the SessionIDs used in
the AAL architecture are correct, cutting the sending
of information when a wrong behaviour, or an
incorrect SessionID, is detected. This involves four
main different functionalities:
- User registration in the system. When a new
user wants to use SAAPHO, his/her data will
be stored in the SM database. The SAAPHO
user identifier used by the architecture is the
UUID (Universally Unique Identifier), which
guarantees that the user is identified in a unique
way by any component in the platform but also
out of the AAL architecture.
- User login. Each time that the user wants to use
SAAPHO he/she will have to log into the User-
Interface. This process involves the sending of
the username and password to the SM and the
generation of the sessionID if the data was
right.
- Health Gateway registration. This process is
similar to the previous one, but in this case the
gateways are the components that send the
parameters to be validated by the SM for
obtaining the sessionID, and the parameter sent
is a registration token.
- Validation of sessionIDs and userIDs.
Health Backend (HB) is connected to the Health
Gateway, and it is in charge of prioritizing the
information sent by the gateway and transmitting it
to the user through the AAL architecture. The
prioritization of the messages sent by the gateway is
a function based on the priorities of the provided
measures and the priority of the users; and the load
balancing of the requests of the users to have a safe
and efficient communication. The main operations in
the HB are:
- Registration of the gateway in the AAL
architecture. If the gateway is in the SM, the
backend looks for a backend of the type of the
gateway that wants to be registered with space
to handle the load of a new gateway, and if
there isn't any, a new backend of that type is
created internally and in a transparent way for
the gateway, that always sends the information
to the same backend.
- Deregistration of the gateway. The backend
frees up the space associated to that gateway
and the sessionID of that gateway is closed.
- Forwarding of the real feedback and
recommendations coming from the Health
Gateway. When a new message is received in
the HB, it is sent to the Orchestrator to be sent
to the UIR for creating the textual message
through which the real feedback or the
recommendation is presented to the user in the
UI, and after that to the TD to be shown to the
user.
4 EVALUATION
In order to assess the usability, accessibility,
applicability, impact and user satisfaction, as well as
detecting areas for improvement, the health
monitoring system was evaluated using two different
prototypes resulting of the second and third year of
the SAAPHO project. The second year prototype
(Year2Prototype) provided a complete vision of
SAAPHO, including the User-Interface, but of
limited functionality. The final and third year
prototype (Year3Prototype) contained the full pack
of functionalities, services and devices of the
system.
4.1 Year2prototype (Y2P)
The prototype considered two health parameters (i.e.
blood pressure and activity monitoring) with a part
of healthcare services (i.e. real-time feedback
generation and historical summary calculation). The
aim of this evaluation is to test a prototype, which is
very similar in functionality and appearance to the
final one. The tasks related to health carried out by
each end user were:
Task 1: Logging into the SAAPHO Platform
with own Login data.
Task 2: Setting the preferred volume and text
size.
Task 3: Checking the historical summary
information of blood pressure.
Task 4: Measuring the blood pressure and
reading the results.
Task 5: Checking the physical activity results.
Figure 2: Average scores for easiness.
HEALTHINF2015-InternationalConferenceonHealthInformatics
378
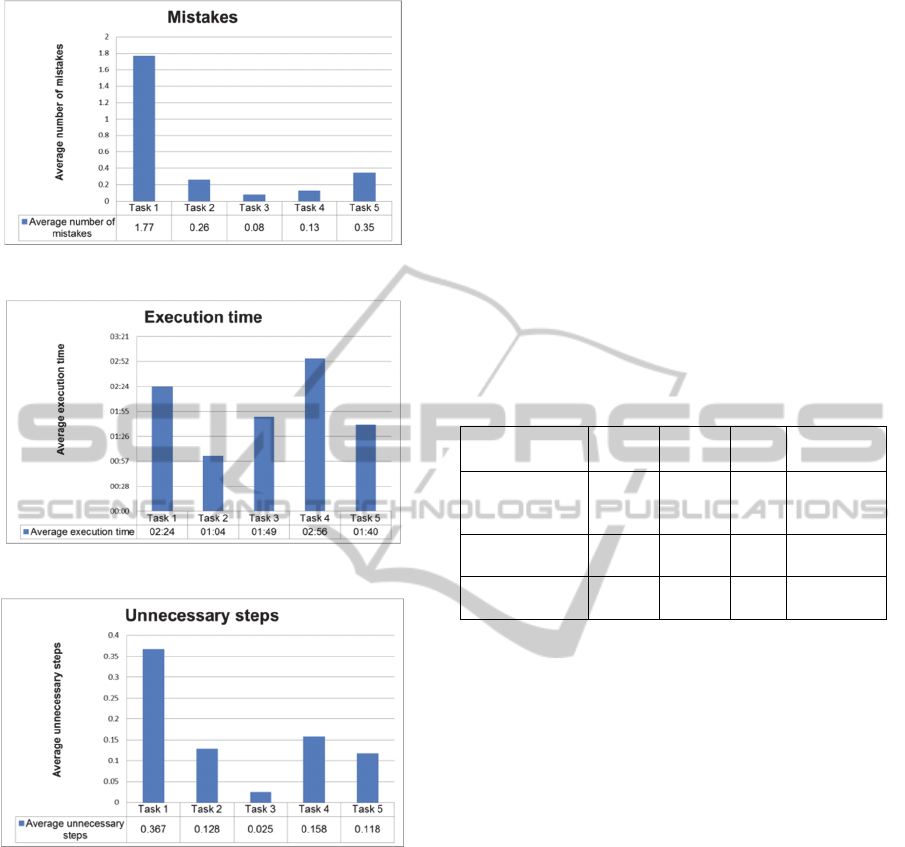
Figure 3: Average number of mistakes.
Figure 4: Average execution time.
Figure 5: Average unnecessary steps.
20 users in Slovenia, and 20 users in Spain
performed the tests. Each test took about one hour
and a half, and the tests were conducted one by one,
with a professional guiding the session, while a
video camera recorded all the user interaction with
the system. After the user carried out the complete
set of tasks, he had to respond to a questionnaire that
covered mostly the usability and applicability issues.
Afterwards, every video was reviewed and analysed,
so that every task for every user was documented as
far as execution time, use patterns, etc. Four
principles were considered for the main analysis: 1)
user-rated easiness 2) number of mistakes 3)
execution time and 4) unnecessary steps. The figures
below present the average values for different tasks.
As it can be seen from figures 2 to 5, the
SAAPHO platform was considered as being easy to
use as most of the scores were above 4 on a 1 to 5
scale (i.e. Figure
5
2). Task 1 (Login to SAAPHO)
was deemed the most difficult, this is probably
explained, because it was the first task, where users
had the first contact with the keyboard layout, but
still many users complained about difficulties with
most things related to text input. Similarly, Task 1
(Login to SAAPHO) had the highest number of
mistakes; again, users had difficulties dealing with
typing in text boxes (switching between fields was
one of the major difficulties). System stability and
performance also played a role in these cases. The
summary of the health related tasks considering all
four principles are presented in Table 1.
Table 1: Summary of the health related tasks.
Health Related
Tasks
No. of
Mistakes
User
Easiness
Time Unnecessary
Steps
Task 3: Check
Blood Pressure
history
0.078 4.35 01:49 0.025
Task 4: Measure
Blood Pressure
0.128 4.54 02:56 0.158
Task 5: Activity
monitor
0.353 4.94 01:40 0.118
Most users commented on the health aspects of the
SAAPHO platform as the one section they found the
most interesting, even if only two sensors were used
in Y2P testing (activity monitor and blood pressure
monitor). Also, usability of the two health tasks of
the system were deemed as very good, although the
layout of the blood pressure history charts made the
score a bit lower (hard to read and understand
because of too much data and therefore text was too
small on some charts).
4.2 Year3Prototype (Y3P)
The year3prototype considered most of the
healthcare parameters (i.e. blood pressure, blood
glucose, pulse monitoring and weight monitoring)
and services defined in section 3. The composition
of the trial formed by six participants from Spain
(n=3) and Slovenia (n=3). They were invited to use
the SAAPHO platform at their own home at least
during a month. The mean age of the 3 participants
in Spain was 69.3 (SD: 9.9); 66-72 years and the
mean age of the 3 participants in Slovenia was 65.7
(SD: 9.9); 60-74 years. Regarding the gender both in
Spain and Slovenia, 66.6% of the participants were
women (n=2) and 33.3% were men (n=1). 100% of
participants had experience using computers. 66.6%
Self-serveICT-basedHealthMonitoringtoSupportActiveAgeing
379
had experience in using tablet PC and all of them
had Internet at home.
Table 2: Summary of the health related questionnaire.
Healthcare
services
Questionnaire
Real-time
feedback
generation
Q1.How do you like the feedback messages
Q2. How useful is the SAAPHO measurement’s
classification
Q3. Any Comments on feedback messages
Historical
summary
Q4. How useful are the feedback charts
Q5. Any Comments on feedback Charts
Q6. How useful are the Daily-wise historical
summary charts
Q7. How useful are the Weekly-wise historical
summary charts
Q8. How useful are the raw data/historical
summary charts based on a selected date range
Q9. Any Comments on Historical Summary
Charts
Recommendat
ion
Q10. How do you like the recommendation
messages on “Devices_Not_Used”
Q11. How do you like the recommendation
messages on “Out_Of_Normal_Range”
Q12. How do you like the recommendation
messages on “Weight_Loss”
Q13. How do you like the recommendation
messages on “Weight_Increase/
Weight_Decreased”
Q14. How do you like the recommendation
messages on “Activity_Increase/
Activity_Decreased”
Q15. Any Comments on Textual
Recommendation messages
Each participant was equipped with a tablet running
the SAAPHO platform in the Y3P version. They had
to conduct several tasks in order to familiarize
themselves with the system and to know all
possibilities that SAAPHO offers. Researchers
contacted them frequently in order to check their
experience. First 3 days of monitoring, users had to
perform some specified tasks prepared by SAAPHO
in order to familiarize with the system.
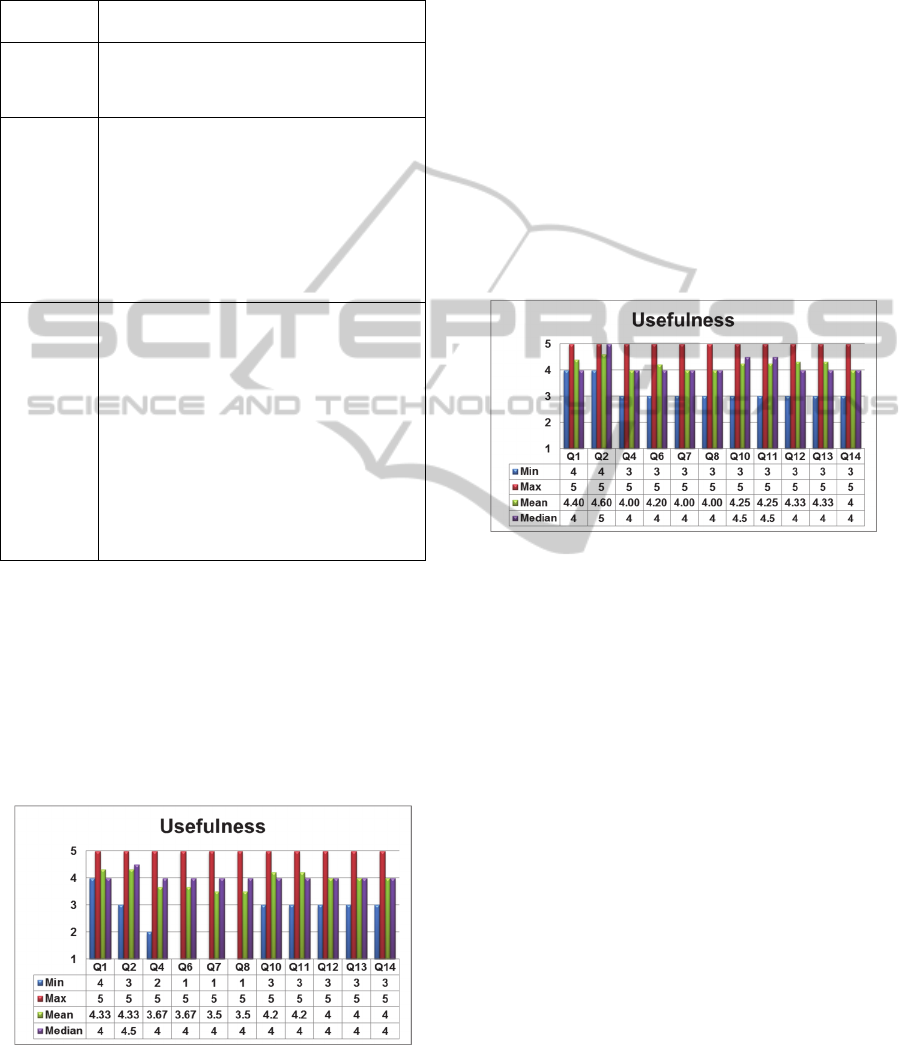
Figure 6: Statistical analysis on the score of usefulness.
After the 4
th
day the users were supposed to have
enough knowledge of the system to be able to work
autonomously and they experimented with the
system by themselves. After completing the 4 weeks
of testing, a set of questionaries’ was provided to the
users in order to evaluate the usefulness of the
proposed healthcare services. The questionnaires
were divided into three parts. User’s answers were
collected both in textual form and as evaluations (a 1
to 5 scale). The Table 2 presents a summary of the
health related questionnaire.
As it can be seen from the figure 6, most of the
questions have the answer 5 as maximum score and
for average and median are around 4. However, the
minimum scores are very low i.e. 1 or 2. The reason
behind this is that one of the participants had
problems with sensor devices and Bluetooth
connections and thus was not able to access the
functionality of the system properly.
Figure 7: Statistical analysis on the score of usefulness
after removing the outlier.
If the evaluation of this participant is considered as
outlier and removed from the analysis then the result
could be improved as presented in Figure 7. Here,
the figure shows that the minimum score is 3 or 4
and the median of the some questions is 4.5 or 5.
User’s comments on the healthcare services are
summarized and presented in Table 3.
As it can be seen from the evaluation result, the
healthcare services through the prototypical system
were acceptable by most of users both in Spain and
in Slovenia. Here, all participants would recommend
the proposed ICT-based health monitoring system to
another older person since they considered it very
easy and useful in relation to the offered services.
Nevertheless, one of them mentioned again the users
that could benefit the most from it: older people
living alone or with his/her partner or caregiver;
having health problems and/or mobility difficulties;
without cognitive problems; living in an old building
without lifts.
HEALTHINF2015-InternationalConferenceonHealthInformatics
380
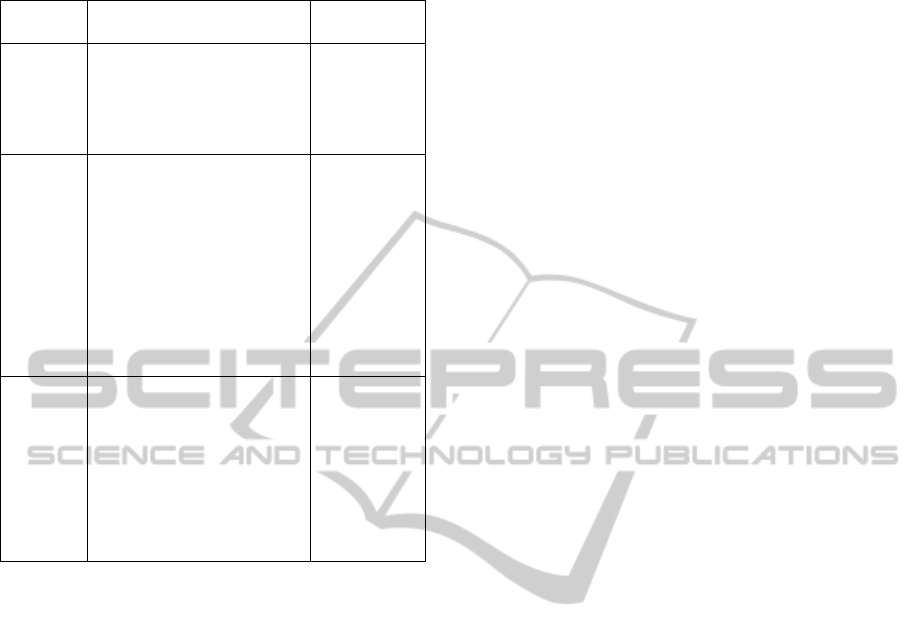
Table 3: Summary of the comments on healthcare
services.
Healthcare
services
Positive comments on the
services
Others
comments
Real-time
feedback
generation
The feedback messages are
excellent.
The feedback messages are useful
for quick information and a
general feeling.
Very practical and clear
I did not receive
notifications
about activity.
Historical
summary
The changes in blood pressure
and weight values are very
welcome for the health
evaluation.
The changes in blood pressure
and weight values are interesting.
Charts were very transparent.
Very practical and clear.
By choosing the date range it is
easier for me to determine the
time that interests me and the
health status at that time.
In relation to
Weight, I would
like to have
more
information
about the ideal
weight.
In relation to
BP, data are
difficult to
interpret.
Recommend
ation
Textual Recommendation
messages were excellent.
Recommendations were
understandable and correct.
To recommend contacting with
the doctor in case of not having
good health results is a good idea.
Information
received is not
clear.
I am not able to
judge as I very
rarely or almost
never received
the health
recommendation
messages.
4 CONCLUSIONS
This paper presents architecture of an ICT-based
health monitoring system, which allows for
information services connected to a number of
wireless health sensors. The article also describes
the integration of this system into a much wider and
extended AAL architecture (i.e. SAAPHO) that aims
to provide active aging to the elderly in their homes.
The paper has complemented the technological
aspects with user evaluation conducted in two
countries. The aim of this work has been to
investigate how users interact with monitoring
system at home, how well they are able to take the
measurements, and how well they are able to
negotiate through the various menus and options.
The aim of the paper has also been to evaluate
whether there was a perceived usefulness of the
system. Overall, the impression of the system has
been positive provided that there is relative ease in
operating the physical sensors. The level of detail of
the information has been deemed sufficient and the
textual recommendations were highly appreciated.
Both objective and subjective measures were used
for the evaluation. Future work will focus on
longitudinal evaluations deployed in larger user
groups. Also, cross-cultural differences between the
user groups will be studied when larger samples
sizes are used.
ACKNOWLEDGEMENTS
This work has been supported by the project named
SAAPHO (Secure Active Aging: Participation and Health
for the Old). The SAAPHO Project (aal-2010-3-035) is
funded by the Call AAL (Ambient Assisted Living) within
the Call 3, ICT-based solutions for advancement of older
persons’ independence and participation in the self-serve
society and by the following national agencies:
MINETUR (Spain); VDI/VDE Innovation + Technik
GmbH (Germany); Ministry of Higher Education, Science
and Technology (Slovenia); Vinnova (Sweden).
REFERENCES
Aarts, E., 2004, Ambient Intelligence: A Multimedia
Perspective. IEEE Multimedia, 11, 12-19.
Ahmed M. U.; Banaee H.; Loutfi A.; Rafael-Palou, X.,
2014. Intelligent Healthcare Services to Support
Health Monitoring of Elderly, Accepted in the
International Conference on IoT Technologies for
HealthCare, HealthyIoT, at Rome, Italy.
Ahmed, M.U.; Banaee, H.; Loutfi, A., 2013a. Health
monitoring for elderly: An application using case-
based reasoning and cluster analysis. ISRN Artif.
Intell., 2013, 380239.
Ahmed, M. U.; Loutfi, A., 2013b. Physical Activity
Identification using Supervised Machine Learning and
based on Pulse Rate, Advanced Computer Science &
Application, 4.
Ahmed, M. U.; Loutfi, A.; 2013c. Physical activity
classification for elderly based on pulse rate, in
Proceedings of the 10
th
International Conference on
Wearable Micro and Nano Technologies for
Personalized Health.
Ahmed, M. U.; Islam A. M.; A Loutfi.; 2012. A case-
based patient identification system using pulse
oximeter and a personalized health profile, in
Proceedings of the Health Sciences at 20
th
International Conference on Case-Based Reasoning,
Eds., Springer, Lyon, France, September 2012.
Alberti, K.G.M.M., Zimmet, P.Z., 1998. Definition,
diagnosis and classification of diabetes mellitus and its
complications. Part 1: diagnosis and classification of
diabetes mellitus. Report of a WHO Consultation.
Journal of Diabetic Medicine, 15, 539–553.
Alemdar, H., Ersoy, C., 2010. Wireless sensor networks
for healthcare: A survey. The International Journal of
Computer and Telecommunications Networking, 54,
2688-2710.
Banaee, H., Ahmed, M.U., Loutfi, A., 2013. Data Mining
Self-serveICT-basedHealthMonitoringtoSupportActiveAgeing
381

for Wearable Sensors in Health Monitoring Systems:
A Review of Recent Trends and Challenges. Sensors,
13, 17472-17500.
Catalogue of Projects 2013, Ambient Assisted Living Joint
Programme (AAL JP), Available online:
http://www.aal-europe.eu/wp-
content/uploads/2013/09/AALCatalogue2013_Final.p
df, (accessed on October 2014).
Claas, A., Albert, S., Jordi, R. S., Simon, H., Alejandro, R.
M., 2012. HELP: Optimizing Treatment of Parkinson's
Disease Patients. In proceeding of 3rd International
Conference on the Elderly and New Technologies.
Crespo, M., Sánchez, D., Crespo, F., Astorga, S., León, A.
2010. Collaborative Dialogue Agent for COPD Self-
management in AMICA: A First Insight. Advances in
Intelligent and Soft Computing, 70, 75-80.
Culhane, K. M., O'Connor, M., Lyons, D., Lyons, G. M.,
2005. Accelerometers in rehabilitation medicine for
older adults, Academic Journal of Age Ageing, 34,
556-60.
Czaja, S. J., 2005. The Impact of Aging on Access to
Technology. SIGACCESS Access. Comput, 83, 7-11.
Deurenberg P, Weststrate J.A., Seidell J.C., 1991. Body
mass index as a measure of body fatness: age- and sex-
specific prediction formulas, Br J Nutr; 65(2):105-14.
Doménech, S., Rivero, J., Coll-Planas, L., Sainz, F.J.,
Reissner, A., Miralles, F., 2013. Involving older
people in the design of an innovative technological
system promoting active aging: the SAAPHO project.
Journal of Accessibility and Design for All, 3, 13-27.
eCAP monitor for bottled medications, Information
Mediary Corporation (IMC), Available online:
http://informationmediary.com/ecap (accessed on
October 2014).
Hanák, P., Kiss, N., Kovácsházy, T., Pataki, B., Salamon,
M., Seres, Cs., Tóth, Cs., Varga, J., 2012. System
Architecture for Home Health and Patient Activity
Monitoring. 5
th
European Conference of the
International Federation for Medical and Biological
Engineering, pp 945-948.
Health@Home, Available online: http://www.aal-
europe.eu/projects/healthhome/ (accessed on October
2014).
Hendeby, G., Bleser, G., Lamprinos, I., Stricker, D., 2010.
Healthy Aging using Physical Activity Monitoring.
AALIANCE conference, Spain, 11-12, pp. 1-5.
INREDIS. Available online: http://www.inredis.es
(accessed on October 2014).
Jovanov, E., Milenkovic, A., Otto C., de Groen P.C.,
2005. A wireless body area network of intelligent
motion sensors for computer assisted physical
rehabilitation. J Neuroeng. Rehabil, 2, 1-10.
Medication Compliance Monitoring System (MCMS),
Cybernet Medical, Available online:
http://www.cybernetmedical.com/index.php/mcms
(accessed on October 2014).
Nee, O., Hein, A., Gorath, T., Hulsmann, N., Laleci, G.B.,
Yuksel, M., Olduz, M., Tasyurt, I., Orhan, U., Dogac,
A., Fruntelata, A., Ghiorghe, S., Ludwig, R., 2008.
SAPHIRE: intelligent healthcare monitoring based on
semantic interoperability platform: pilot applications,
Communications, IET 2008, 2, 192-201.
Pansiot, J., Stoyanov, D., McIlwraith, D., Lo, B. P., Yang,
G. Z., 2007. Ambient and wearable sensor fusion for
activity recognition in healthcare monitoring systems.
Proceedings of the 4
th
International Workshop on
Wearable and Implantable Body Sensor Networks
(IFBME’07), pp. 208–212.
Pantelopoulos, A., Bourbakis, N.G., 2010. A Survey on
Wearable Sensor-Based Systems for Health
Monitoring and Prognosis, Systems, IEEE
Transactions on Man, and Cybernetics, Part C:
Applications and Reviews, 40, 1-12.
Persona Project, Available online: http://www.aal-
persona.org/ (accessed on October 2014).
Ruxandra, B., Luminita, D., Alina, I., Horatiu, D., Ileana,
C., Mihai, B., 2011, IS-ACTIVE Project in Lab Trial
Phase. In Romanian Journal of Physical and
Rehabilitation Medicine, 21, 64-65.
Sala, P., Tazari, S., Farshchian, B., Furfari, F., 2013. The
universAAL Reference Architecture. universAAL
Deliverable D1.3 – E 2013.
Soprano Project, Available online: http://www.soprano-
ip.org/ (accessed on October 2014).
Understanding blood pressure readings. American Heart
Association. Available online:
http://www.heart.org/HEARTORG/Conditions/HighBl
oodPressure/AboutHighBloodPressure/Understanding-
Blood-Pressure-Readings_UCM_301764_Article.jsp,
(accessed on October 2014).
UNIVERSAAL. Available online:
http://universaal.org/index.php/es/about/about-project-
description (accessed on October 2014).
Varshney, U., 2007. Pervasive healthcare and wireless
health monitoring. Journal Mobile Networks and
Applications, 12, 113-127.
Why exercise with a Heart Rate Monitor, Available
online:
https://zsig.com/content/why_exercise_with_a_heart_r
ate_monitor_/, (accessed on October 2014).
1
http://wserver.flc.losrios.edu/~willson/fitns304/handouts/bodyCompositio
n.html
2
http://www.healthcare.omron.co.jp/bt/english/
3
http://www.glbiotech.com.tw/productdesc.php?pdtid=11
4
http://www.izm.fraunhofer.de/en.html
HEALTHINF2015-InternationalConferenceonHealthInformatics
382
