
The Potential of the m-Health Platform to Safeguard Public Health
The Nigerian Example
Allen Nnanwuba Adum, Uche Patricia Ekwugha and Ngozi Marion Emmanuel
Department of Mass Communication, Nnamdi Azikiwe University, Awka, Anambra State, Nigeria
Keywords: Mobile Authentication Service, Public Health Informatics, Fake Drugs, m-Health.
Abstract: Nigeria has a problem with fake drugs. This issue got to an intolerable height in 1989 when over 150
children died as a result of ingesting paracetamol syrup containing diethylene glycol. The National Agency
for Food and Drug Administration and Control (NAFDAC) was formed in 1993, as an agency under the
Nigerian federal ministry of health, to check the tide of fake drugs and adulterated products. To achieve this
mission, NAFDAC, in 2010, launched the Mobile Authentication Service (MAS) – a mobile-phone m-
Health platform, which empowers medication drug users to instantaneously verify the authenticity or
otherwise of a medication drug before purchase. This study sought to ascertain the workability of MAS
among medication drug users; and factors negating this platform. The study was designed as a survey. Data
was collected from 400 medication drug users in Lagos state, Nigeria, through a structured survey. Results
show that 91 percent of the respondents were aware of MAS and 53 percent among these utilized it prior to
purchasing medication drugs, while 9 percent were neither aware of MAS nor utilize it. The notable barriers
to the use of MAS found in this study were lack of awareness and the unreliable nature of the MAS.
1 INTRODUCTION
Mobile telephony, popularly known as GSM, was
introduced in Nigeria in the year 2001. Prior to this
development, Nigerians relied on telephone
landlines provided by state-owned telecom service,
NITEL (Nigerian Telecommunications). Today,
with the advent of mobile telephony, 118,850,928
Nigerians have been connected to GSM lines. Out of
this number, 553,425 actively use their mobile
phones (WWW.ncc.gov.ng). This was not obtainable
in the era of landline phone services in Nigeria.
Mobile telephony has engendered many
possibilities. Nigerians have been empowered to
make and receive calls from any part of the country,
once there is network coverage by any of the
operational telecom services. Also, SMS could be
sent and received in a matter of minutes or even
seconds. Nigerians no longer need to go and stand in
queues at NITEL call centres or phone booths to
make calls; neither do they need to write letters
which might take days, weeks or even months to get
to their various destinations. The Internet can now
be accessed on the go by owners of mobile phones.
This situation brings to mind the reality of Marshall
McLuhan’s idea of a Global Village.
In recent times, the use of mobile telephony has
gone beyond the conventional calls and SMS.
Today, mobile phones are being used as m-Health
tools. Mobile Health, also known as mHealth or m-
Health implies the use of mobile communication
devices such as mobile phones for health services
(Cipresso et al, 2012). One good example of m-
Health is the Mobile Authentication Service (MAS)
introduced by Nigeria’s National Agency for Food
and Drug Administration and Control (NAFDAC) in
the year 2010. According to Osuolale (2011:3) “this
is a world-first, showing the pro-active [stance] of
Nigeria in the global fight to rid the world of fake
medication.”
Nigeria is the largest medication drugs market in
Africa. The issue of fake pharmaceuticals has been a
problem in. Nigeria. Nigeria imports 70 percent of
its drugs from India and China, two main sources of
fake and adulterated pharmaceutical products. Also,
The World Health Organization reports that, 70
percent of drugs in circulation in Nigeria are
counterfeit (WHO Report 2014). Again, Osibo
(1998) observes that there may be more fake drugs
than authentic drugs in circulation in Nigeria.
Akuyili (2005) notes that drug counterfeiting started
383
Adum A., Ekwugha U. and Emmanuel N..
The Potential of the m-Health Platform to Safeguard Public Health - The Nigerian Example.
DOI: 10.5220/0005215203830389
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 383-389
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
in Nigeria way back in the 60s; meaning, Nigerians
have been dying from fake drugs for decades. “
According to Davison (2011) and Bansal, Malla,
Gudala and, Tiwari (2013), a counterfeit medication
or a counterfeit drug is regarded as a medication or
pharmaceutical product which is produced and sold
with the intent to deceptively represent its origin,
authenticity or effectiveness.
In 1988, the World Health Assembly passed a
resolution requesting every member-nation to help
combat the menace of counterfeit drugs. Barely a
year after this resolution, the issue of deaths from
fake drugs in Nigeria became unbearable with the
deaths of 150 children as a result of ingesting
paracetamol syrup which contained diethylene
glycol.
The World Customs Organization estimates that
the fake drug market is a $200 Billion a year
industry; with a strong base in developing
economies. Also, the World Health Organization
estimates that 30 percent of drugs in developing
economies are faked and may be very harmful to
consumers.
In order to check fake and adulterated drugs in
Nigeria, the government established the NAFDAC
in 1993; and in 1994 it became a full agency under
the federal ministry of health.
In pursuit of its mandate, NAFDAC, on the 2nd
of February 2010, launched the first Mobile
Authentication Service (MAS) on anti- malaria drug,
Lonart-DS, marketed by Greenlife Pharmaceuticals,
Nigeria. MAS is a technology-based anti-drug
counterfeiting mobile telephony initiative, developed
by Sproxil Incorporated. Sproxil is a privately-
owned company founded in 2008 (and incorporated
in 2009) by Ghanaian-born Ashifi Gogo, a
Holekamp Family Ph.D. Innovation Fellow at
Dartmouth College. Sproxil provides a consumer
SMS and App. product verification service which
help consumers avoid purchasing counterfeit
products. Sproxil has operations in Ghana (serving
West Africa), Nigeria, Kenya (serving East Africa),
and India (Sproxil Solutions, 2014).
NAFDAC’s Mobile Authentication Service,
powered by Sproxil, allows prospective Nigerian
drug consumers to confirm the authenticity or
otherwise of a particular drug at the point of
purchase. The technical components of MAS include
a scratch panel pre-printed by Sproxil that can be
affixed on packs of medication or printed codes
embossed directly by manufacturers on medication
packs; mobile phone and GSM network service host
the Sproxil authentication portal. All the consumer
needs to do is to scratch the panel on the drug pack
and text a 12-digit number on it to 38353 without
paying any charges. A confirmatory message as to
the authenticity of the drug should come in a matter
of seconds.
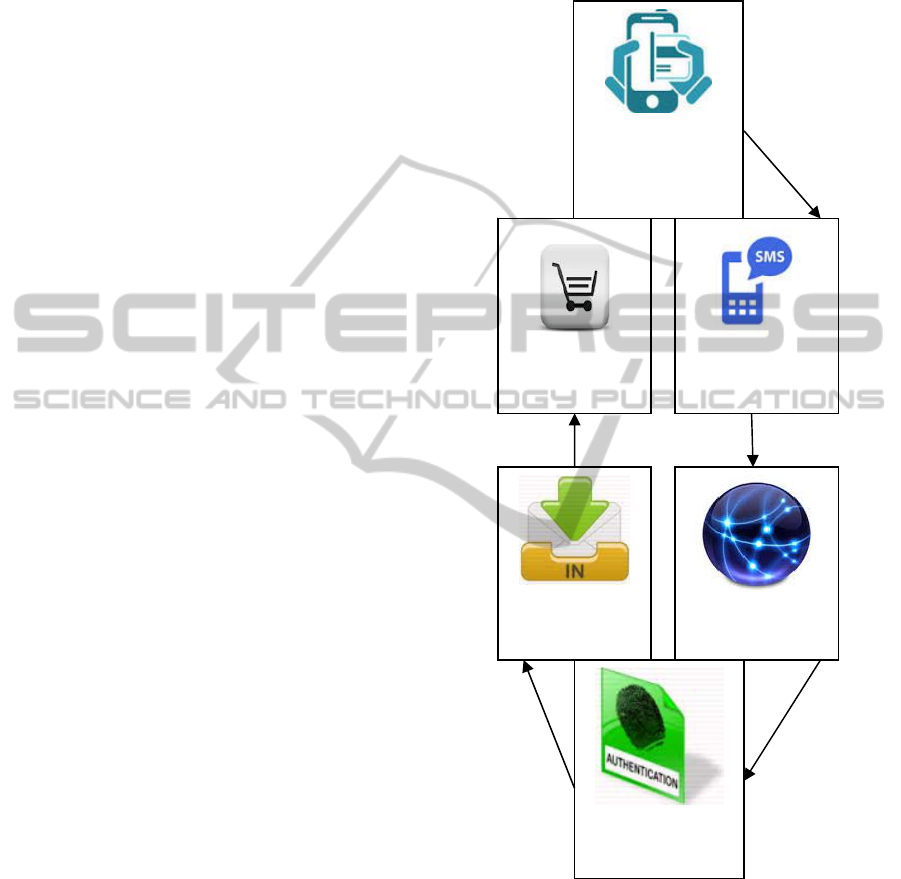
Figure 1: How MAS works.
But the question is: is this as seamless as it sounds?
The lead author of this paper got a Lonart anti-
malarial drug on the 21
st
of January 2014, and sent
the pin (182032090421) to 38353 by 07:22 pm. Up
until now he’s yet to get the confirmatory message
from 38353. How many Nigerians face this kind of
situation? Does it make them unwillingly to utilize
MAS or perceive the service as unworkable? How
many are indeed aware of the existence of MAS?
Scratch-off
panel on pack for
12 digit PIN
Text 38353 using
mobile phone
Purchase
Confirmatory
message
Network Service
hosting Sproxil
p
ortal
Authentication by
Sproxil portal
HEALTHINF2015-InternationalConferenceonHealthInformatics
384

These questions are pertinent because, negligible
utilization of m-Health tool such as MAS, as a result
of certain barriers would amount to a big waste of
public informatics which would have otherwise
enhanced public health.
2 AIMS OF STUDY
The main aim of the study was to investigate the
utilization of NAFDAC’s Mobile Authentication
Service (MAS) among Nigerian medication drug
users and barriers to utilizing this innovation. The
study sought answers to the following questions:
1. Who among Nigerian medication drug users are
aware of NAFDAC’s Mobile Authentication
Service?
2. How many of these medication drug users indeed
utilize NAFDAC’s Mobile Authentication
Service?
3. What are the barriers to the utilization of the
Mobile Authentication Service?
3 METHOD
This study was designed as a survey. Focus was on
Lagos State, Nigeria. Lagos is a cosmopolitan city.
This city is also a major seaport and with a
population (according to Nigeria’s 2006 population
census) of 17.5 million (a population that is larger
than the population of Rwanda, 11.46 million
according to CIA World Fact book), it is the most
populous city in Nigeria This strategic position of
Lagos makes it a good starting point for almost
every innovation in Nigeria. This had informed
situating this study in Lagos State, Nigeria.
A sample of 400 medication drug users was used
for the study. This sample was arrived at using Taro
Yamane’s formula for determining sample size n=
N/1+ N (e)
2
. By a simple random sample we
selected 10 Local Government Areas from the
available 21 LGAs, using table of random digits,
The Local Government Areas are: Ojo; Amuwo-
odofin; Badagry; Alimosho; Ifako-ijaiye; Ikeja;
Surulere; Mushin; Ikorodu and Apapa. A validated
questionnaire was used as research instrument. Four
hundred copies of the questionnaire were distributed
at the rate of 40 copies per local government area;
389 completed surveys were returned, representing a
response rate of 97 percent.
A series of questions were asked on awareness of
NAFDAC’s Mobile Authentication Service;
utilization of Mobile Authentication Service and
barriers to the utilization of Mobile Authentication
Service.
4 THEORETICAL BASIS
This study was anchored on The Health belief
Model (HBM). The HBM is a psychological model
first developed in the 1950s by social psychologists
Hochbaum, Rosenstock and Kegels. HBM is used to
explain and predict health behaviors. In the light of
this, the core assumptions of this study, in line with
the HBM framework, are that a medication drug user
will take a health-related action (i.e., use Mobile
Authentication Service) if they:
1. feel that a negative health condition (ailments as
a result of ingesting fake drugs) can be avoided,
2. have positive expectations that by taking
a
recommended action, he/she will avoid
a
negative health condition (i.e., using Mobile
Authentication Service will be effective in
helping them not to purchase fake drugs), and
3. believe that they can successfully take a
recommended health action (i.e., they can use
Mobile Authentication Service withou
t
difficulties) (Rosenstock, 1974).
5 RESULTS
The distribution in the sample was 37 percent male
and 63 percent female. One third of the medication
drug users are civil servants, one quarter
professionals, one sixth business people, one eighth
university students, one twentieth artisans and self-
employed persons, one fortieth farmers and one
sixtieth unemployed persons. The majority of these
medication drug users were within the 18-30 age
bracket. Data also show that 52 percent of the
respondents were single, 47 percent married. The
remaining one percent were either separated or
divorced.
In terms of educational qualification, about two
thirds of the respondents indicated that they have
had secondary education; about 17 percent had first
degrees or above while the remaining one fifth did
not indicate any chosen option for the question.
We can therefore say that our respondents are
young persons who fall mainly within the middle
and lower classes of the Nigerian society.
ThePotentialofthem-HealthPlatformtoSafeguardPublicHealth-TheNigerianExample
385
5.1 Purchase of Medication Drugs
over the Counter
Here we attempted to establish who among the
respondents engaged in over the counter drug
purchase. Survey question five in the questionnaire
was used for this purpose.
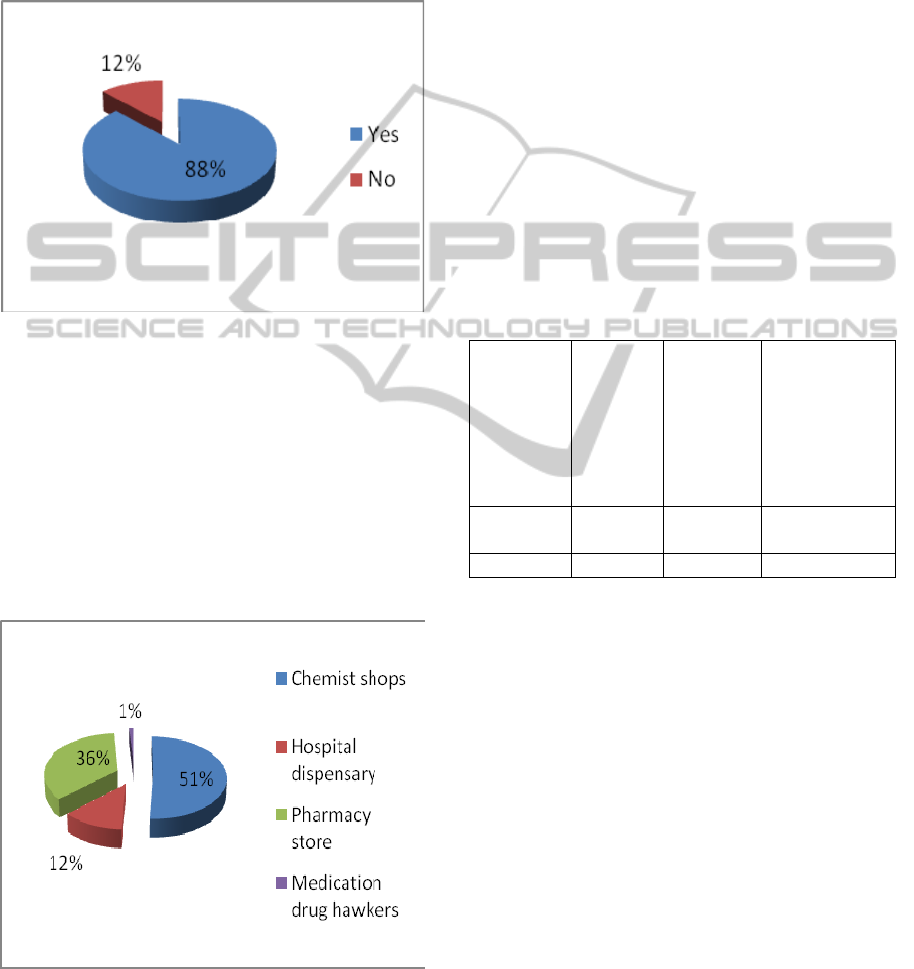
Figure 2: Respondents who purchased drugs over the
counter.
The study found that over two thirds of the
respondents purchased medication drugs over the
counter, while 12 percent were affirmative that they
did not purchase medication drugs over the counter.
It appears logical to say that our data suggest that a
majority among the respondents at one point in time
have purchased medication drugs over the counter.
5.2 Sources of Drug Supply
Figure 3: Respondents’ main source of drug supply.
Our data suggest that more of the respondents had
Chemist shops as their main source of drug supply;
‘Chemist’ as they are popularly known in Nigeria
are drug stores closer and more accessible to the
ordinary citizenry. Figure 3 shows that 51 percent of
the respondents purchased medication drugs from
Chemist shops; a little above two fourths got drugs
from pharmacy stores while 12 percent got drugs at
hospital dispensaries. One percent of the respondents
said they got drugs from hawkers. The ‘Chemist’ or
‘Patent medicine store’, by virtue of being run by
people who might not be regarded as well trained
medical personnel – even though most are
government-registered – could become fertile
grounds for the sale of fake drugs to unsuspecting
members of the Nigerian public. That large number
of people patronise the ‘Chemist’, as data in this
study show, points to the need to utilize the MAS at
the grassroots.
5.3 Ownership and Use of Mobile
Phones
Table 1: Ownership and use of mobile phones.
Own
mobile
phones
(N=389)
(%)
Own
mobile
phones
with text
message
features
(N=389)
(%)
Respondents
who wrote text
messages
(N=389)
(%)
Yes
No
97
3
100
0
93
7
Total 100 100
100
Our data show that 97 percent of the respondents
own mobile phones; virtually all these mobile
phones have features for text messaging. This is
against three percent that do not own mobile phones
and seven percent that own mobile phones but
cannot write text messages. Ninety-three percent of
the respondents claimed they could write text
messages.
Technology is something that appears to take
time before people get accustomed to it. Having the
right literacy means the ability to use ICT devices
like the text messaging feature on mobile phones.
Not having the necessary literacy apparently
accounts for the inability of seven percent among the
respondents to use mobile telephony text messaging
feature.
HEALTHINF2015-InternationalConferenceonHealthInformatics
386
5.4 Awareness of the Existence of
NAFDAC’s Mobile Authentication
Service
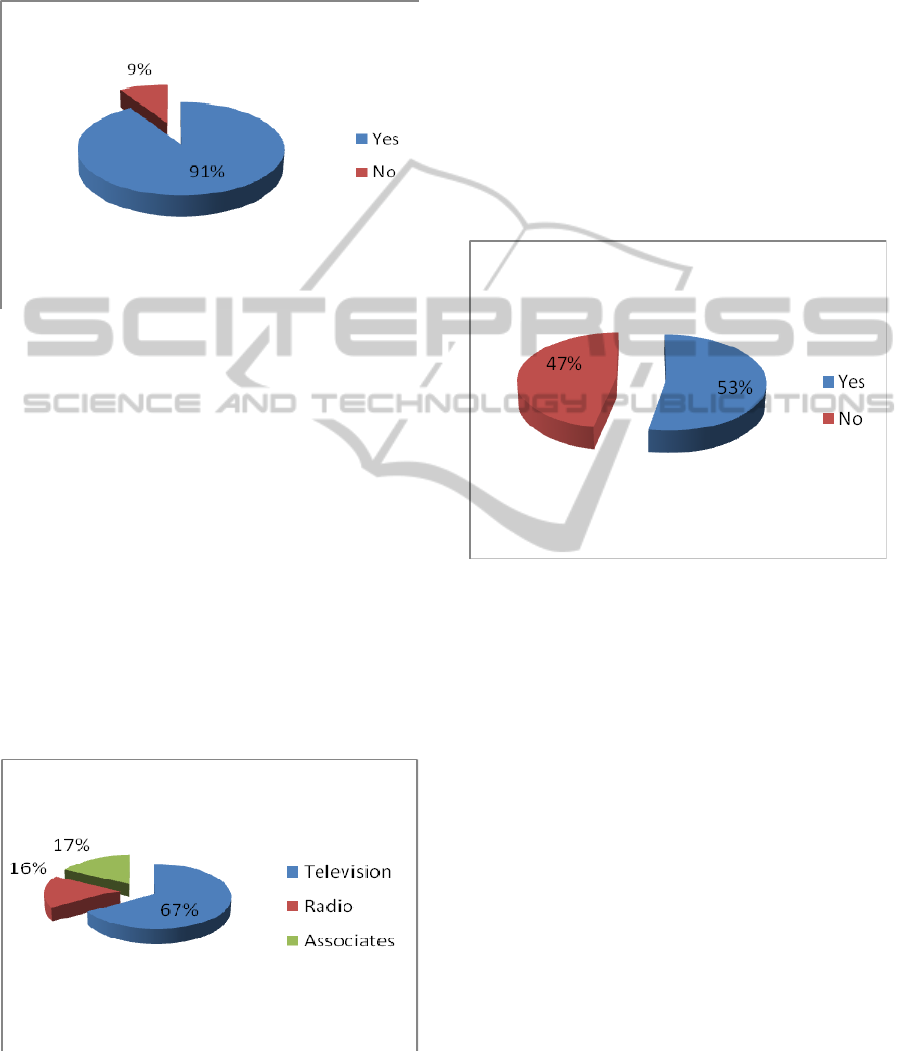
Figure 4: Respondents who have heard about NAFDAC’S
MAS.
The data in Figure 4 show that as at the time of this
study, majority of medication drug users studied in
the Lagos area were aware of the existence of
NAFDAC’s Mobile Authentication Service. Only 9
percent of the respondents affirmed not knowing
about the existence of MAS. This data would
suggest that NAFDAC’s public enlightenment
campaigns have been largely successful in
sensitizing the public on the need to safeguard their
health through the utilization of MAS; but more still
needs to be done by way of enlightenment to
consolidate the gains already made.
5.5 Sources of Information about
NAFDAC’s MAS
Figure 5: Respondents’ sources of information about
NAFDAC’s MAS.
On the question of sources of information on
NAFDAC’s MAS, the study found that 67 percent of
the respondents indicated that they got to know
about the NAFDAC’s MAS through enlightenment
campaigns on television (Figure 5); Seventeen
percent of the respondents said they got to know
about MAS through associates, while 16 percent of
the respondents said they got to know about MAS
via the Radio. None of the respondents chose the
Magazine, Newspapers, Billboards or Posters as the
medium through which they got to know about
MAS; therefore they were not reflected in our
presentation.
5.6 Utilization of NAFDAC’s MAS
.
Figure 6: Respondents who have used MAS to confirm the
authenticity of Medication drugs before purchase.
With regard to the respondents’ utilization of
NAFDAC’s MAS to authenticate medication drugs
before purchase, we found that a little above two
fourths of the respondents who said they were aware
of MAS also said they have used it to confirm the
authenticity of medication drugs before purchase;
while over two fifths among these respondents were
not affirmative as to having used MAS to
authenticate medication drugs before purchase.
5.7 Barriers to Utilizing NAFDAC’s
MAS
Data in Figure 7 show that close to 40 per cent of the
respondents who used NAFDAC’s MAS had some
difficulties; notably, delayed or non-arrival of
confirmatory SMS messages indicating whether a
drug about to be purchased is genuine or not; while
61 percent said they had no problems using the
mobile service. Network coverage is one issue that
negates the operations of the authentication portal in
ThePotentialofthem-HealthPlatformtoSafeguardPublicHealth-TheNigerianExample
387
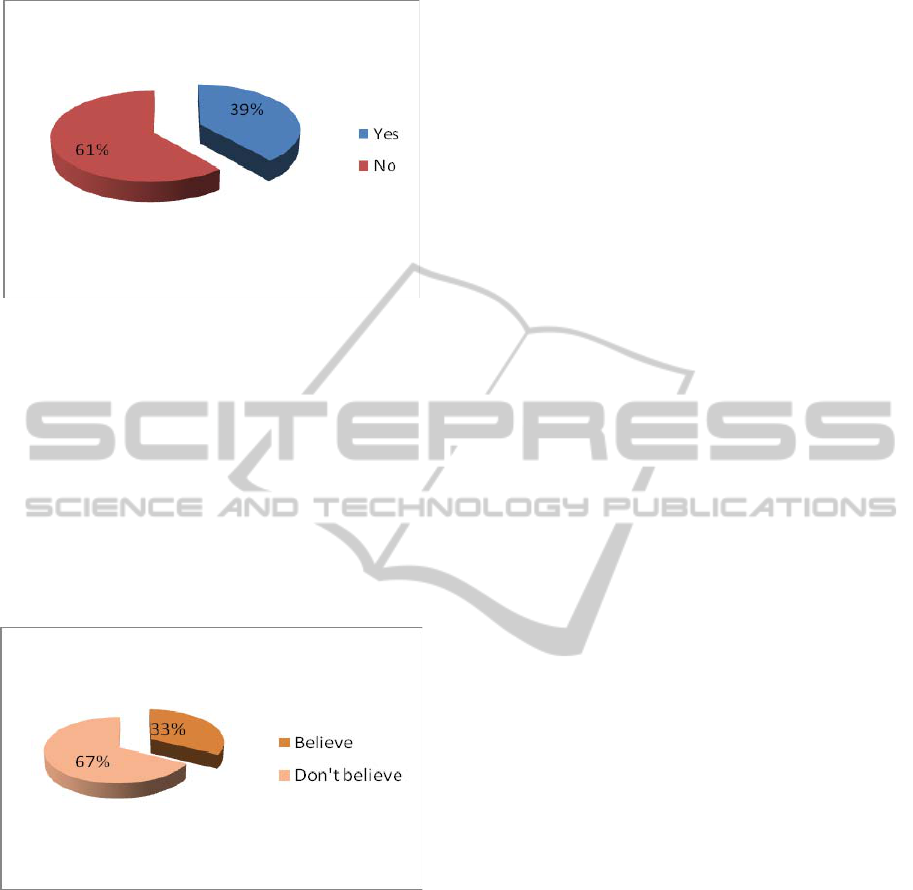
Figure 7: Respondents who have difficulties using MAS to
confirm the authenticity of Medication drugs before
purchase.
relaying confirmatory message to medication drug
users. Overall, the picture here is that MAS, going
by the number of people who could use it without
difficulties, as suggested by the findings of this
study, has the potential to be a workable m-Health
platform to safeguard the medication drug users
from purchasing and ingesting fake drugs.
5.8 Workability of NAFDAC’s MAS
Figure 8: Respondents’ perception of the workability of
NAFDAC’s MAS.
Part of this study examined how the respondents
perceived the workability of NAFDAC’s MAS. The
data in Figure 8 reveals that 33.percent of the
respondents believe that NAFDAC’s MAS is
workable in Nigeria, while 67 percent believe
otherwise. The fact that the service is balky might be
the basis for the position of those who do not believe
in the workability of this m-Health platform.
6 SUMMARY AND CONCLUSION
Our data show that our respondents are mainly
young persons who come from the middle and lower
classes of the Nigerian society.
The study found that more of the respondents are
aware of NAFDAC’s Mobile Authentication Service
and a greater percentage among them use the mobile
service before making purchase decisions. The data
suggest that nearly all medication drug users studied,
whose phones have text messaging features, can
actually compose text messages. Our data also
indicate that not all medication drug users who own
mobile phones, and were aware of MAS, utilized the
Mobile Authentication Service to verify the
genuineness or otherwise of pharmaceutical
products.
On the workability of the MAS m-Health
platform, a sizeable number of the respondents who
used the MAS, encountered difficulties ranging from
delayed confirmatory messages to non-arrival of
confirmatory messages. However, a significant
number of MAS users expressed high hopes of its
workability in Nigeria.
Overall, the findings of the study suggest that the
potential to safeguard public health through the
NAFDAC’s MAS m-Health platform is feasible and
with little effort at technical reappraisal and
improvement, the MAS innovation could be a
critical element that could assist Nigeria in the fight
against fake drugs which are harmful to medication
drug users.
7 RECOMMENDATIONS
Based on the findings of this study, it becomes
imperative to make recommendations that could
help NAFDAC, as well as relevant stakeholders who
may find the contents of this research helpful. These
recommendations are as follows:
NAFDAC should as a matter of necessity,
intensify efforts on massive integrated awareness
creation on its Mobile Authentication. Service.
This is because, the relative success or failure of
an initiative, irrespective of how noble, is
measured by the level of awareness and
acceptability by its targets. Statistics gotten in the
course of this study suggest high level of
awareness, but more needs to be done to further
consolidate this gain.
NAFDAC should also bear in mind that not
everyone who owns mobile phones that are text
HEALTHINF2015-InternationalConferenceonHealthInformatics
388

messaging-enabled, can write text messages.
This is another pitfall to the Mobile
Authentication Service, because even when
medication drugs users are willing to utilize
MAS, they may be deterred by the inability to
compose text messages. Special considerations
should be given to this category of persons in the
event of any future modification of MAS.
Issues of delayed or non arrival of confirmatory
messages from the Mobile Authentication
Service portal should be addressed. This appears
to be the greatest stumbling block to the
utilization of the service. First time users of
MAS who fail to get confirmatory text messages
from the portal, could be discouraged from using
it further, and may also discourage others with
their experiences. Positive testaments from the
users of MAS could go a long way in influencing
and convincing other medication drugs users,
who are yet to utilize MAS.
Seminars and workshops should be organised
periodically at different locations, to sensitize
and create adequate awareness about MAS.
Community and village heads as well as popular
celebrities should also be integrated in
campaigns pertaining to MAS. The goodwill and
positive images of these individuals could be
transferred to MAS, thus making it acceptable to
medication drugs users.
REFERENCES
Akunyili, D. (2005). “Counterfeit and Sub-standard Drugs,
Nigeria’s Experience: Implications, Challenges, Actions
and Recommendations”. A paper presented at a
meeting for key interest groups on health organised by
the World Bank in Washington D. C. 10th -11th
March 2005.
Bansal, D, Malla S, Gudala K, Tiwari P (March 2013).
“Anti-Counterfeit Technologies: A Pharmaceutical
Industry Perspective”, Sci Pharm 81 (1) 1-13.
CIA World Factbook
Cipresso, P.; Serino S., Villani D., Repetto C., Selitti L.,
Albani G., Mauro A., Gaggioli A., Riva G. (2012). "Is
your phone so smart to affect your states? An
exploratory study based on psychophysiological
measures". Neurocomputing 84: 23–30.
Davison, M. (2011). “Pharmaceutical Anti-Counterfeiting:
Combating the Real Danger from Fake Drugs’, Wiley.
p426.
National Population Census, 2006
Osibo, O.O. 1998. Faking and counterfeiting of drugs.
West African Journal of Pharmacy. 12(1):53 – 57.
Osuolale, J. A. (2011). “The Use of Mobile Phone to
check for the Authenticity of Pharmaceutical Products in
Nigeria a case study of Mobile Authentication Service
(MAS)”. Department of Archaeology and
Anthropology University of Ibadan, Nigeria.
Rosenstock, I. (1974). Historical Origins of the Health
Belief Model. Health Education Monographs. Vol. 2 No.
4.
Sproxil Solutions (2014). Sproxil and IBM partner to fight
counterfeit drugs. Retrieved 30th March 2014 from
http://www.en.wikipedia.org/wiki/sproxil
WHO Report 2014, retrieved from
http://www.who.int/medicines/services/counterfeit/impact/
ImpactF_S/en/index1.html.
www.ncc.gov.ng
ThePotentialofthem-HealthPlatformtoSafeguardPublicHealth-TheNigerianExample
389
