
Incremental Learning Versus Batch Learning for Classification
of User’s Behaviour in Medical Imaging
Carlos Viana-Ferreira, Sérgio Matos and Carlos Costa
Instituto de Engenharia Electrónica e Telemática de Aveiro, Universidade de Aveiro, Campus Universitário de Santiago,
Aveiro, Portugal
Keywords: Batch Learning, DICOM, Incremental Learning, PACS, Pattern Recognition.
Abstract: Communication latency still hinders the adoption of Cloud computing paradigms in medical imaging
environments where it could serve as a reliable technology to support repository outsourcing solutions or
inter-institutional workflows, for instance. One way to overcome this is by implementing cache repositories
and prefetching mechanisms. Nevertheless, such solutions are usually based on static rules that may
inefficiently manage the cache storage capacity. For that reason, this paper compares a pattern recognition
system using incremental learning versus batch learning, in order to assess which one could be more
appropriately used in a medical imaging cache mechanism.
1 INTRODUCTION
Medical imaging is an important tool in medical
practice, giving physicians valuable information for
better diagnosis and treatment (Sylva, 2010, Rengier
et al., 2010). Many medical imaging processes are
supported by Picture Archiving and Communication
Systems (PACS) (Huang, 2011), an umbrella term
that embraces a set of technologies for acquisition,
visualization, storage and distribution of medical
imaging data (Valente et al., 2012). In order to do
so, these systems rely on large IT infrastructures,
comprising application servers, archives acquisition
equipment (i.e. modality equipment) and network
equipment, communicating through the Digital
Imaging and Communications in Medicine
(DICOM) standard (ACR-NEMA, 2011b).
Traditional PACS solutions are hosted in the
healthcare institution and all equipment is connected
in the physical layer by a Local Area Network
(LAN). Nevertheless, with the proliferation of high-
speed Internet connections, the PACS concept has
broadened its horizons, embracing:
Infrastructure outsourcing (Philbin et al.,
2011, Chen and Sion, 2011), i.e. the moving of
IT infrastructure from indoors to outdoors,
reducing maintenance costs.
Institutional collaboration (Marques Godinho
et al., 2014, Sutton, 2011, Silva et al., 2013b),
facilitating the remote access to examinations
and reports (Costa et al., 2009) in response to
the dispersion of patient’s data that arises from
their mobility between different institutions
(Viana-Ferreira and Costa, 2014a).
In both cases, communication latency is a critical
issue, because it is typically higher than in intra-
institutional processes (Viana-Ferreira and Costa,
2014a).
This is emphasized by the nature of the data,
since medical imaging examinations may reach
volumes of hundreds of megabytes for some
modalities (Yakami et al., 2011). To minimize this
problem, there are two possible solutions: (1) cache,
i.e. a small but fast repository hosted near the final
consumer that stores a portion of the main repository
data; and (2) prefetching, which consists in
requesting images before users request them.
However, the effectiveness of these solutions is
highly dependent on their capability of predicting
which data will be needed next. Most current
solutions are based on static rules over specific
parameters (Huang, 2011, Bui et al., 2001),
considering the specific workflow of each
institution. This tailoring constitutes a drawback of
these solutions, as they may not be suitable for more
dynamic scenarios, leading to a degradation of
service quality or even denial of service in particular
sets of conditions.
For these reasons, a pattern recognition solution
431
Viana-Ferreira C., Matos S. and Costa C..
Incremental Learning Versus Batch Learning for Classification of User’s Behaviour in Medical Imaging.
DOI: 10.5220/0005219704310438
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 431-438
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
that could automatically adapt itself to user’s
behaviours and institutional workflows, while also
giving special attention to situations that may
become critical for the overall performance of the
system, would be desirable. In this setting, this paper
presents a comparison between incremental learning
and batch training for such pattern recognition
approach.
2 MEDICAL IMAGING
LABORATORIES
Most medical imaging services, from acquisition and
storage, to transmission and visualization of medical
imaging data are manage by Picture Archiving and
Communication Systems (PACS) (Huang, 2011).
Most systems of this kind are intrinsically complex,
as they are responsible for handling all medical
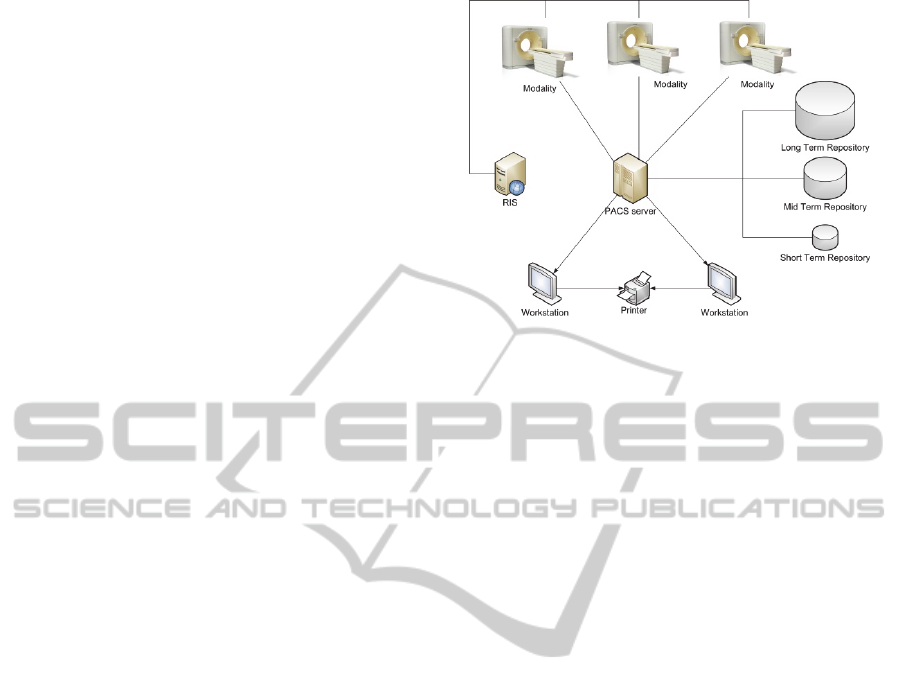
imaging data of a healthcare institution. Figure 1
shows an example of a PACS instance, composed by
several modalities (i.e. image acquisition devices),
the repository, a PACS server, workstations, printers
and a Radiology Information System (RIS), all
linked by a Local Area Network (LAN).
2.1 Digital Imaging
and Communications in Medicine
(DICOM)
Currently in version 3, the DICOM standard (ACR-
NEMA, 2011b) is composed of twenty parts,
defining a wide set of processes related to medical
imaging, such as: network communication layers,
service commands, encoding and data structures and
visualization processes (Pianykh, 2011). The wide
range of processes and its versatility made DICOM a
well-accepted standard, being currently followed by
virtually all medical imaging equipment. For this
work, the most important aspect of the standard is
related to the DICOM services (ACR-NEMA,
2011a), including:
C-Store service is used to push DICOM objects
into the repository.
C-Get is for requesting objects by their
identifiers from an archive.
C-Move service is for copying an object from
one repository into another.
C-Find is used to query an archive about objects
that match a query.
Figure 1: Typical PACS instance architecture (Viana-
Ferreira and Costa, 2014a).
2.2 Federation of Healthcare
Institutions
With the spread of fast Internet connections, the
PACS concept has reached different settings. One
example of this is the PACS described in (Silva et
al., 2013a).
This PACS serves two healthcare institutions at
the same time: Institution A and Institution B. While
both institutions have image acquisition devices,
only Institution A has a repository that stores all
produced images. This strategy allowed the
institutions to reduce costs with IT infrastructure,
while promoting medical cooperation. However, the
main drawback of this architecture is related to the
quality of the service provided to Institution B.
While Institution A accesses data via a fast LAN,
Institution B must rely on an Internet connection,
which is significantly slower than the LAN of
Institution A, to access the repository. This means
that any object exchange between the institutions
will be limited by the upstream bandwidth, which in
this case is 12 megabits per second. Although this is
already able to provide a satisfactory quality of
service, it cannot compete with the quality of service
provided by traditional indoor solutions (Philbin et
al., 2011), hindering the adoption of these federated
approaches.
One way to reduce this problem is to endow
Institution B with a cache and a prefetching
mechanism that populated the cache with
examinations that will be needed in a close future.
3 CACHE AND PREFETCHING
Cache is a small and fast repository that is used to
HEALTHINF2015-InternationalConferenceonHealthInformatics
432
hide the impact of communication latency, by
temporarily storing objects that more likely will be
needed soon. The population of this mechanism can
be carried out in two ways: (1) in a passive mode, in
which the cache is populated with the last used
objects; (2) in a more active way, recurring to
prefetching, i.e. predicting the objects that will be
needed and requesting them before the users do.
Either way, caches have a limited capacity, which
leads to the need of discarding some stored objects
when they are full. For this reason, one characteristic
of cache repositories is their replacement policy,
which discards the objects that are less probable of
being needed (Smith, 1982). There are numerous
cache replacement policies, the most traditional ones
being: Least Recently Used (LRU) (Ali et al., 2011),
by size (Williams et al.), First In First Out, by
predicting when they will be needed and discarding
the last ones (Jaleel et al., 2010), Least Frequently
Used (LFU) (Podlipnig and Boszormenyi, 2003), by
a decision function (Cao and Irani, 1997) and
randomized (Psounis and Prabhakar, 2001).
Healthcare institutions may store such huge
amounts of medical imaging data that it becomes
financially unfeasible to make all data accessible at
the best quality of service. For that reason, as
depicted in Figure 1, they store all data in long-term
repositories and only data that is more likely to be
needed is replicated in faster repositories, i.e. mid-
term and short-term repositories (Huang, 2011).
In this environment, prefetching is traditionally
carried out through static rules over predefined
parameters (Huang, 2011). Nevertheless, such
solutions are usually especially designed for each
situation or are too generic, causing the prefetching
of too many objects and overloading the network
with useless traffic. As an example, in (Bui et al.,
2001), a prefetching mechanism with static rules
based on multiple information sources is describes.
The tests carried out by the authors indicated a recall
of 100%, but only 50% of precision. This means
that, although all needed data was prefetched, only
half of the prefetch data were relevant.
The authors believe that machine learning and
pattern recognition can lead to more effective cache
and prefetching mechanisms. Nevertheless, it is a
relatively unexplored field, with only residual
references found in the literature. An example is the
work described in (Liu Sheng et al., 2000), in which
neural networks and decision trees were tested to
predict which patient’s images would be needed.
However, we did not find any solution that took into
account distinct usage patterns.
4 PATTERN RECOGNITION
Pattern recognition has been an active research field
for the last decades (Pal and Pal, 2001) and it
consists on the development of algorithms for
automatic decision-making processes (Maji and Pal,
2011), using data to infer patterns (Yegnanarayana,
2009, Duda et al., 2012). This has been applied in a
wide range of scenarios, such as: rivers bio-
assessment (Feio et al., 2013), computer-aided
diagnosis (Ramírez et al., 2013), content based
image retrieval (Valente et al., 2013), stock market
index prediction (Guresen et al., 2011) and computer
vision (Chen et al., 2010).
Pattern recognition embraces a set of tasks, such
as: pattern association, pattern classification, pattern
mapping, pattern grouping, and feature mapping,
among others (Yegnanarayana, 2009). In this article,
we are focused in the pattern classification problem
that consists on the use of a set of patterns and their
labels and finding the distinctions between patterns
of distinct labels (Duda et al., 2012).
4.1 Artificial Neural Networks
One of the most well-known machine learning
methods for pattern classification is the artificial
neural networks (ANN) (Yegnanarayana, 2009).
Due to its versatility, its ability to detect nonlinear
relationships between variables and because of being
able to update with new samples, the algorithm used
in this work is based on ANN.
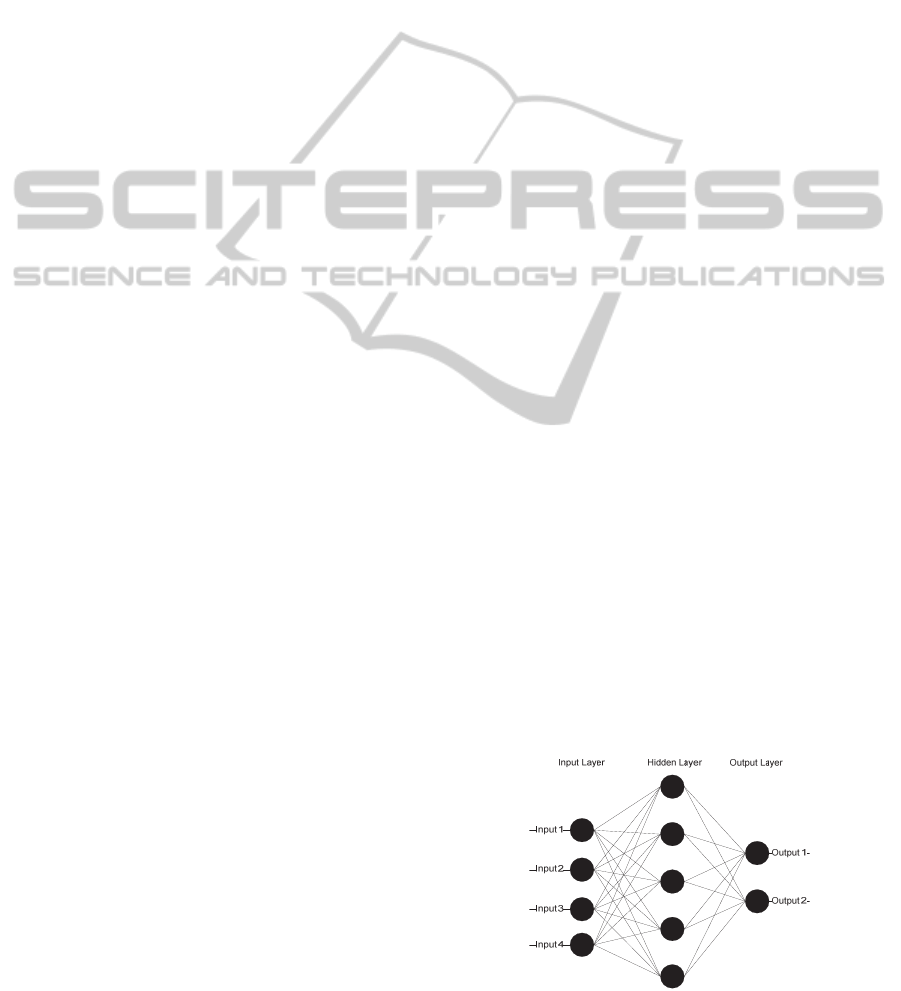
Basically, it consists on a group of processing
units (or neurons) that are linked in a determined
way. One of the possible topologies is the multilayer
perceptron (MLP), where the processing units are
organized in layers, and usually each one of them
receives the output of all processing units of the
previous layer. For example, Figure 2 shows a
representation of a MLP that receives 4 inputs and
returns 2 outputs, having one hidden layer with 5
neurons.
Figure 2: Representation of a multilayer perceptron.
IncrementalLearningVersusBatchLearningforClassificationofUser'sBehaviourinMedicalImaging
433

4.2 Models, Classes and Features
For this work, the authors applied a previously
developed algorithm that predicts which class of
objects will be needed, considering the C-Finds sent
to the PACS server. This algorithm considers four
distinct usage pattern classes:
Pattern revising (class 1): user is revising
multiple studies of a single patient, for instance
in a patient’s appointment or when a clinician is
evaluating the history of a patient.
Modality revising (class 2): user is revising
studies of a specific modality in a time window.
Inconsequent query (class 3): this pattern class
is for some queries which do not result in C-
Move requests. One example of this is when a
user erroneously introduces the search
parameter. Another example is produced by
some DICOM viewers that repeatedly send C-
Find requests to refresh the interface.
“Other usage” (class 4): this usage pattern is
for all usage patterns that do not relate directly
to the healthcare provision service itself in
healthcare institutions, for instance, a data
auditing.
The algorithm taken as the basis of this work
uses five MLPs for each workstation in the PACS:
Four MLPs, one for each class, with 26 input
perceptrons, 250 perceptrons in the hidden layer
and 1 output perceptron. As features, these
MLPs uses three kinds of features: (1) time
features that describe the pattern according to its
temporal location; (2) history features that
describe the pattern according to the user
history until the moment of the C-Find of this
pattern; and (3) the type of query.
One MLP with 4 input perceptrons, 20
perceptrons in the hidden layer and 4 output
perceptrons. Since the other four MLPs are
trained independently, this MLP is used to take
into account the outputs of the others and reach
a conclusion about the actual class.
5 EXPERIMENTAL PROCEDURE
In this work, we compared the use of incremental
learning to the use of a previously trained model (i.e.
batch learning) when classifying the usage pattern
when a C-Find request is detected. The objective of
this pattern recognition step is to help infer which set
of objects will more likely be requested afterwards,
which in turn would allow developing and
improving cache replacement and prefetching
mechanisms.
5.1 Oracle
The oracle is a module that provides the
classification of previous usage patterns, based on
information about C-Move requests produced after
the C-Find requests. This is a key component of the
system, since it gives the actual classification of the
patterns, to be used in training and updating the
models that will then be applied online.
The labelling of the patterns is carried out in the
following way:
If there is only one C-Move between two C-
Finds, it uses also the previous and the next
patterns.
If no studies were requested between two C-
Finds, this patter is classified as “Inconsequent
query” (class 3).
If (almost) all requested studies are from the
same patient, then the pattern is assigned as
“Patient revising” (class 1).
If it does not pass the previous test and (almost)
all requested studies are of the same modality,
then the pattern is assigned as “Modality
revising” (class 2).
In case a pattern seems ambiguous, i.e. if
considering only the first C-Move requests the
pattern would be assigned as one class, but if
considering only the last C-Move requests the
pattern would be assigned as other class, then
the oracle will only consider the first C-Move
requests.
If the pattern failed all previous evaluations then
the pattern is assigned as class 3.
5.2 Real-world Dataset
The real-world datasets is divided in two parts: a
XML file and an index. The XML file contains
anonymized information about 5186 DICOM
messages that were sent to and from the PACS
server in a period of roughly 3 months, while the
index has data about the studies stored in the clinics’
database. In both parts of the dataset, data was
anonymized using hash functions to guarantee
patient’s privacy, while enabling the reproduction of
the queries and their respective results.
After processing the messages with the oracle,
we concluded that the real-world dataset consists of
17% patterns of class 1; 4% patterns of class 2; 29%
patterns of class 3; and 50% patterns of class 4.
HEALTHINF2015-InternationalConferenceonHealthInformatics
434

5.3 Synthesized Dataset
Ideally, we would use only real-world data for the
tests, nevertheless, due to bureaucratic and ethical
issues real-world datasets are not easy to obtain.
Moreover, even when they are obtained, the range of
distinct situations is usually limited.
In order to complement the results obtained with
the real-world dataset, we have used a synthesizer of
DICOM traffic based on behaviour profiles (Viana-
Ferreira and Costa, 2014b). With this tool we have
simulated the behaviour of three workstations in a
one-year period:
Workstation A has a regular behaviour along
the experiment.
Workstation B is most exclusively used to
review studies of a given modality in the first
six months, but in the following six months is
used also for patient appointments.
Workstation C behaves without a notion of
timetable, being used indistinctly along time.
This represents a workstation in a volatile
scenario.
Table 1
shows the distribution in percentage of
the samples among the 4 classes in the three
simulated workstations. It also includes the
distribution of the whole dataset with the three
workstations combined.
Table 1: Distribution of the samples among the distinct
classes (1 – Patient revising, 2 – Modality revising, 3 –
Inconsequent query and 4 – Other usages) in the 3
synthetized workstations (A, B and C).and in the whole
synthesized dataset (Combined).
Class
Workstation A Workstation B Workstation C Combined
1 20.7 % 12.3 % 63.5 % 37.5 %
2 4.5 % 72.7 % 24.3 % 42.3 %
3 7.2 % 3.8 % 4.1 % 4.3 %
4 67.6 % 11.2 % 8.1 % 15.9 %
5.4 Experimental Tests and Discussion
The experimental tests were done with the two
datasets: real-world and synthesized ones. Each one
was tested under 4 distinct scenarios:
Train 25: batch learning with the 25% oldest
samples of the dataset, while the other 75% of
the dataset is used to test them.
Train 50: the 50% oldest samples were used to
train the models, while the others were used to
test them.
Train 75: 75% oldest sample were used to train
the models while the others 25% were used to
test the models.
Incremental Learning: only the first week was
used to train the models. From then on, the
samples of each week were used, firstly, to test
the models and, secondly, to update the model.
Each test condition was executed ten times and
the results averaged to mitigate the noise caused by
random initialization of MLPs. In order to compare
the performance of each learning method we chose
two measures: (1) the accuracy which is a ratio
between the number of times the prediction was
right and the total number of samples; and (2) the F-
Measure of each class which is calculated as shown
in equation 1.
2
2
̅
(1)
In equation 1, F-Measure(C) is the F-Measure of
class C, TC is the number of times the method
predicted the class C correctly, FC is the number of
times the method wrongly predicted the sample
belonged to class C, and
̅
is the number of times
the method wrongly labeled the sample as not
belonging to class C.
6 RESULTS
In this section, the results of the experiments are
presented, divided in real-world and synthesized
datasets.
6.1 Real-world Dataset
Figure 3 is a graph with the accuracy and the f-
measures for each class, in each testing condition
with the real-world dataset.
From the analysis of the graph, we can conclude
that the algorithm behaved worse for the least
representative class, i.e. class 2, in every condition.
Nevertheless, it must be highlighted that this is a
consequence of very few data about that usage
Figure 3: Graph with accuracy and F-measures for the real
dataset.
IncrementalLearningVersusBatchLearningforClassificationofUser'sBehaviourinMedicalImaging
435

pattern class, only 4% of class representation in the
dataset. Besides that, there are no evident differences
between the different testing conditions, i.e. Train
25, Train 50, Train 75 and Incremental learning.
This can be explained by the limited time window
represented by the dataset that did not include
situations like changes of medical staff in the
institution.
6.2 Synthesized Dataset
Figure 4 contains graphs of the f-measures for each
class and the overall accuracy. The first three
graphs, i.e. (a), (b) and (c), show the evaluation
measures for each workstation of the synthesized
dataset, while the last one, i.e. (d), shows the
evaluation measures for the whole synthesized
dataset.
From the analysis of the graphs, emphasis to the
f-measure for class 1 in workstation B, where all
training/testing scenarios had less than 15%, while
the incremental learning achieved more than 50%.
This can be explained by the nature of the
synthesized data for this workstation, with a change
in behavior during the experiment. The results
clearly show that the incremental learning was the
only training method capable of adapting the
classifiers for this situation. Moreover, we can
conclude that incremental learning was only worse
than the batch learning conditions in workstation C
which represents a very volatile scenario.
6.3 Overall Discussion
For what concerns accuracies, all testing conditions
demonstrated to achieve roughly the same accuracy.
Nevertheless, the Train 75 scenario was slightly
better for the synthesized dataset, while the
Incremental Learning was the best for the real-world
dataset.
Concerning f-measures, incremental learning has
proven to be more effective in classes with less
representation in the dataset, while only slightly
worse for classes with more representation in the
dataset.
Nevertheless, it must be highlighted that the
results of the incremental learning includes all
predictions of the model, starting from the second
week of data, when the models were in a very
immature state. This means that with only a slight
degradation of performance, we could launch the
solution with only one week of data, instead of 3
months, which is represented by the Train 25
condition in the synthesized dataset.
7 CONCLUSIONS
In this paper, we tested a pattern recognition system
that is based on machine learning for classification
Figure 4: Graphs with the accuracy and F-measures for each synthesized workstation and for the combined dataset: (a)
workstation A; (b) workstation B; (c) workstation C; (d) combined.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Accuracy F‐Measure
Class1
F‐Measure
Class2
F‐Measure
Class3
F‐Measure
Class4
Train25 Train50 Train75 IncrementalLearning
(a)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Accuracy F‐Measure
Class1
F‐Measure
Class2
F‐Measure
Class3
F‐Measure
Class4
Train25 Train50 Train75 IncrementalLearning
(b)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Accuracy F‐Measure
Class1
F‐Measure
Class2
F‐Measure
Class3
F‐Measure
Class4
Train25 Train50 Train75 IncrementalLearning
(c)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Accuracy F‐Measure
Class1
F‐Measure
Class2
F‐Measure
Class3
F‐Measure
Class4
Train25 Train50 Train75 IncrementalLearning
(d)
HEALTHINF2015-InternationalConferenceonHealthInformatics
436

of users’ behaviours.
The tested aimed to compare incremental
learning with batch learning conditions, to assess if
incremental learning is advantageous or not for this
scenario.
We have concluded that despite of a minor
degradation of the results in some cases, incremental
learning is advantageous for pattern recognition
since it has a smaller length of time for deployment.
Besides, even the slight degradation of performance
may be explained with the premature start of result
extraction from the incremental learning testing
condition.
Based on these results, as future work the authors
will use incremental learning for the pattern
recognition algorithm that aims at giving
information to prefetching and cache replacement
agents about which subset of images will be
probably needed in a close future.
ACKNOWLEDGEMENTS
This work has received support from the EU/EFPIA
Innovative Medicines Initiative Joint Undertaking
(EMIF grant n° 115372). Carlos Viana-Ferreira is
funded by the FCT grant SFRH/BD/68280/2010.
Sérgio Matos is funded under the FCT Investigator
programme.
REFERENCES
ACR-NEMA 2011a. Digital Imaging and
Communications in Medicine. Part 4: Service Class
Specifications. Rosslyn, VA, USA: NEMA.
ACR-NEMA 2011b. Digital Imaging and
Communications in Medicine (DICOM). Rosslyn,
VA: National Electrical Manufacturers Association.
Ali, W., Shamsuddin, S. M. & Ismail, A. S. 2011. A
survey of Web caching and prefetching. Int. J.
Advance. Soft Comput. Appl, 3, 18-44.
Bui, A. A., Mcnitt-Gray, M. F., Goldin, J. G., Cardenas,
A. F. & Aberle, D. R. 2001. Problem-oriented
prefetching for an integrated clinical imaging
workstation. Journal of the American Medical
Informatics Association, 8, 242-253.
Cao, P. & Irani, S. Cost-aware WWW proxy caching
algorithms. Proceedings of the 1997 USENIX
Symposium on Internet Technology and Systems,
1997.
Chen, C.-H., Pau, L.-F. & Wang, P. S.-P. 2010. Handbook
of pattern recognition and computer vision, World
Scientific.
Chen, Y. & Sion, R. 2011. To cloud or not to cloud?:
musings on costs and viability. Proceedings of the 2nd
ACM Symposium on Cloud Computing. Cascais,
Portugal: ACM.
Costa, C., Freitas, F., Pereira, M., Silva, A. & Oliveira, J.
L. 2009. Indexing and retrieving DICOM data in
disperse and unstructured archives. International
Journal of Computer Assisted Radiology and Surgery,
4, 71-77.
Duda, R. O., Hart, P. E. & Stork, D. G. 2012. Pattern
classification, John Wiley & Sons.
Feio, M. J., Viana-Ferreira, C. & Costa, C. 2013.
Combining Multiple MAChine Learning Algorithms
to Predict Taxa Under Reference Conditions For
Streams Bioassessment. River Research and
Applications, n/a-n/a.
Guresen, E., Kayakutlu, G. & Daim, T. U. 2011. Using
artificial neural network models in stock market index
prediction. Expert Systems with Applications, 38,
10389-10397.
Huang, H. 2011. PACS and imaging informatics: basic
principles and applications, Wiley-Blackwell.
Jaleel, A., Theobald, K. B., Simon C. Steely, J. & Emer, J.
2010. High performance cache replacement using re-
reference interval prediction (RRIP). Proceedings of
the 37th annual international symposium on Computer
architecture. Saint-Malo, France: ACM.
Liu Sheng, O. R., Wei, C.-P., Hu, P. J.-H. & Chang, N.
2000. Automated learning of patient image retrieval
knowledge: neural networks versus inductive decision
trees. Decision Support Systems, 30, 105-124.
Maji, P. & Pal, S. K. 2011. Rough-Fuzzy Pattern
Recognition: Applications in Bioinformatics and
Medical Imaging, John Wiley & Sons.
Marques Godinho, T., Viana-Ferreira, C., Bastiao Silva, L.
& Costa, C. 2014. A Routing Mechanism for Cloud
Outsourcing of Medical Imaging Repositories.
Biomedical and Health Informatics, IEEE Journal of,
PP, 1-1.
Pal, S. K. & Pal, A. 2001. Pattern recognition: from
classical to modern approaches, World Scientific.
Philbin, J., Prior, F. & Nagy, P. 2011. Will the Next
Generation of PACS Be Sitting on a Cloud? Journal of
Digital Imaging, 24, 179-183.
Pianykh, O. S. 2011. Digital imaging and communications
in medicine (DICOM), Springer.
Podlipnig, S. & Boszormenyi, L. 2003. A survey of Web
cache replacement strategies. ACM Comput. Surv., 35,
374-398.
Psounis, K. & Prabhakar, B. A randomized Web-cache
replacement scheme. INFOCOM 2001. Twentieth
Annual Joint Conference of the IEEE Computer and
Communications Societies. Proceedings. IEEE, 2001
2001. 1407-1415 vol.3.
Ramírez, J., Górriz, J. M., Salas-Gonzalez, D., Romero,
A., López, M., Álvarez, I. & Gómez-Río, M. 2013.
Computer-aided diagnosis of Alzheimer’s type
dementia combining support vector machines and
discriminant set of features. Information Sciences,
237, 59-72.
Rengier, F., Mehndiratta, A., Tengg-Kobligk, H.,
Zechmann, C. M., Unterhinninghofen, R., Kauczor, H.
IncrementalLearningVersusBatchLearningforClassificationofUser'sBehaviourinMedicalImaging
437

U. & Giesel, F. L. 2010. 3D printing based on imaging
data: review of medical applications. International
Journal of Computer Assisted Radiology and Surgery,
5, 335-341.
Silva, L. A. B., Costa, C. & Oliveira, J. L. 2013a. An agile
framework to support distributed medical imaging
scenarios. IEEE International Conference on
Healthcare Informatics 2013 (ICHI 2013).
Philadelphia, USA.
Silva, L. B., Costa, C. & Oliveira, J. 2013b. DICOM relay
over the cloud. International Journal of Computer
Assisted Radiology and Surgery, 8, 323-333.
Smith, A. J. 1982. Cache memories. ACM Computing
Surveys (CSUR), 14, 473-530.
Sutton, L. N. 2011. PACS and diagnostic imaging service
delivery—A UK perspective. European Journal of
Radiology, 78, 243-249.
Sylva, P. 2010. A Situation Analysis on PACS prospects
for a Developing Nation. Sri Lanka Journal of Bio-
Medical Informatics, 1, 112-117.
Valente, F., Costa, C. & Silva, A. 2013. Dicoogle, a Pacs
Featuring Profiled Content Based Image Retrieval.
PLoS ONE, 8, e61888.
Valente, F., Viana-Ferreira, C., Costa, C. & Oliveira, J. L.
2012. A RESTful Image Gateway for Multiple
Medical Image Repositories. Information Technology
in Biomedicine, IEEE Transactions on, 16, 356-364.
Viana-Ferreira, C. & Costa, C. 2014a. Challenges of
Using Cloud Computing in Medical Imaging. In:
Ramachandran, M. (ed.) Advances in cloud Computing
Research.
Viana-Ferreira, C. & Costa, C. 2014b. DICOM Traffic
Generator based on behavior profiles. In: IEEE (ed.)
IEEE-EMBS International Conferences on Biomedical
and Health Informatics. Valencia, Spain.
Williams, S., Abrams, M., Standridge, C. R., Abdulla, G.
& Fox, E. A. Removal Policies in Network Caches for
World-Wide Web Documents.
Yakami, M., Ishizu, K., Kubo, T., Okada, T. & Togashi,
K. 2011. Development and Evaluation of a Low-Cost
and High-Capacity DICOM Image Data Storage
System for Research. Journal of Digital Imaging, 24,
190-195.
Yegnanarayana, B. 2009. Artificial neural networks, PHI
Learning Pvt. Ltd.
HEALTHINF2015-InternationalConferenceonHealthInformatics
438
