
Coexistence of Wireless Systems for Remote Monitoring of Vital
Functions in the Unlicensed ISM Band
Aleksandra Rashkovska, Roman Trobec and Mihael Mohorčič
Department of Communication Systems, Jožef Stefan Institute, Jamova cesta 39, Ljubljana, Slovenia
Keywords: Wireless Body Sensor, Hospital, Telemedicine, Remote Monitoring, Coexistence.
Abstract: A recent trend in medical practice is the use of wearable wireless body sensors (WBS) to improve mobility
of patients and medical personnel during surgery and other procedures, accelerate patients’ recovery, and
facilitate remote monitoring of patients suffering from chronic diseases. Currently, Wireless Body Area
Networks (WBANs) are being introduced in already crowded unlicensed frequency bands, such as the ISM
band. This essentially leads to high interference with other electronic devices, low signal-to-noise ratio and
links with high bit-error rate. This paper discusses the requirements, benefits and issues related to a WBS in
a medical WBAN system for remote health monitoring, operating in the shared ISM frequency band. We
investigate the applicability of the concepts of cognitive communications in such environment to enhance
the coexistence, robustness, scalability, and utility of medical WBAN systems in heterogeneous wireless
networks environment.
1 INTRODUCTION
The health of hospitalized patients is regularly
assessed by periodic measurements of vital
functions’ indicators, such as respiratory rate, heart
rate, blood pressure and body temperature. With
close monitoring and dynamic change detection of
these patient’s parameters, necessary medical
assistance can be provided. If the patient’s condition
deteriorates and continuous monitoring is needed,
the patient is transferred to the intensive care unit.
However, the intensive care units have a limited
number of beds. In addition to the issue of
intermittent monitoring of vital functions in non-
intensive wards, there are other weaknesses in the
current health care system.
The interpretation of the patient’s condition and
the subsequent measures most often depend on the
medical personnel, who could be, in certain
conditions, overwhelmed with work or busy with
other patients. The measured indicators can also be
inaccurate, sometimes being biased by the
inexperience of the medical personnel or patient’s
stress, and therefore unreliable. The subsequent
interpretation of the documented measurements can
be difficult because they may be based on
insufficient or unreliable data.
The introduction of contemporary information
and communication technologies (ICT), as a support
to medical procedures and activities, is one of the
possibilities to increase the efficiency of the health
care system and to decrease its costs. This basic
premise is included in all strategic plans of the EU
and the rest of the world (European Union, 2004;
Dzenowagis & Kernen, 2005; World Health
Organization, 2006). Numerous studies have
confirmed the benefits of the development of
Telemedicine/Telecare systems (Chaboyer, et al.,
2008; Ekeland, et al., 2010). In this respect, wireless
communication technologies are increasingly used in
various medical applications, significantly
enhancing patients’ mobility after surgical
procedures and interventions, which can potentially
lead to earlier patients’ discharge from hospitals.
Additionally, wireless communications allow remote
monitoring of chronic patients and the elderly at
home. More specifically, the trends in recent years
are towards wireless body area networks (WBANs)
applied for patient monitoring (Coronel, et al.,
2004).
Although WBANs offer many benefits for
monitoring and telecare, their introduction in
hospital environments creates additional interference
problems that need to be carefully assessed and
mitigated. Namely, most of the WBANs include
medical sensors operating in the unlicensed
628
Rashkovska A., Trobec R. and Mohor
ˇ
ci
ˇ
c M..
Coexistence of Wireless Systems for Remote Monitoring of Vital Functions in the Unlicensed ISM Band.
DOI: 10.5220/0005284306280633
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 628-633
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

frequency band at 2.4 GHz (referred to as ISM band
- industrial, scientific and medical radio band).
Moreover, the ISM band is regularly used for
transmissions in the operating rooms where surgical
procedures are routinely assisted by electronic
devices that potentially can interfere with the
wireless sensors or vice versa. Also, there are a
number of other medical devices that transmit
critical information wirelessly, as well as ubiquitous
consumer devices with Bluetooth and Wi-Fi access.
In this paper, we consider applying transceivers
in wireless medical equipment that are capable of
dynamically adjusting parameters like frequency,
bandwidth/data-rate, and transmitter power level,
based on awareness of the environment in which
they operate, and thus avoid or minimize mutual
interference. More precisely, we propose the use of
the concepts of cognitive communications - a
challenging area with many approaches, various
development trends, and future directions still being
in the research focus (Fortuna & Mohorčič, 2009;
Steenkiste, et al., 2009). In this paper, we do not
focus on the operational aspects of cognitive
communications, but rather on their applicability to
improve the coexistence of wireless systems for
remote monitoring of vital functions with other
systems operating in the same frequency band.
The rest of the paper is organized as follows. In
Section 2, we discuss the requirements for a body
sensor to be considered in a WBAN for telemedicine
purposes. This section also includes the description
of a custom developed multifunctional wireless body
sensor. Section 3 describes the architecture of the
proposed telemedicine system, discusses the issues
in such operating environments and outlines the
applicability of cognitive communications
approaches to improve the coexistence in the ISM
band. Finally, Section 4 briefly summarizes the
paper.
2 MEDICAL WIRELESS BODY
SENSORS
The main requirements for a wireless body sensor
(WBS) in a medical environment include comfort,
lightweight, low cost, low power signal, operation
under various environmental conditions and
interference avoidance (Ikehara, et al., 2007).
Having a comfortable WBS that the user voluntarily
wears is one of the main criteria that a WBS should
fulfil. Light-weighted WBS furthermore improves
user comfort and allows for multiple sensors to be
comfortably worn at the same time. Low cost WBS
would make the WBAN system suitable for mass
manufactured health sensor networks.
Two aspects should be considered regarding the
transmit power of the WBS signal. First, since the
sensor is placed on the human skin for medical use,
the radiation caused by the large wireless
transmission power may have negative impact on the
human health. Second, in order to extend the life of
the sensor’s battery, the power consumption for the
transmitting signal should be minimized. Both
aspects set limitations on the power of the signal in a
WBAN system (Drude, 2007). Moreover, it is
necessary and important for the WBAN system to be
capable of detecting and receiving a very low power
signal from large background noise. In such
scenarios, alternative power sources making use of
energy harvesting can be considered, for example, a
Peltier device to convert body heat into electricity or
a piezoelectric device to convert body motion into
electricity (Baard, 2001). Moreover, studies have
shown that higher bit-rates actually help preserve
power (Rohde & Toftegaard, 2011).
The physical environment of WBAN also
provides great challenges that include body effects
and surrounding environment. The movement and
position of the human body can have a significant
impact on the propagation of the signal. One of the
most known phenomena of body effect is the body
shadowing effect (Cotton & Scanlon, 2007).
Another important impact comes from the
surrounding environment. The wireless signal
transmitted by the sensor will be reflected by the
floor, walls and surrounding object, which may lead
to the multi-path effect that can impose interference
on the original signal. Interference avoidance from
nearby users with a similar sensor system or other
electronic devices is accomplished by using low
power devices (also reducing energy consumption)
and by operating them in a frequency range where
they are unlikely to interfere.
Other characteristics required from a medical
WBAN include also: (i) On-board memory and basic
signal processing to extract relevant data, (ii) Data
compression to reduce the amount of data to be
transmitted and stored if re-transmission is required;
the last also implies time stamping of the data, (iii)
WBAN should easily interface with standard
computer and other medical equipment, (iv) There
must be a compromise between the communication
and the processing tasks, and furthermore with the
WBAN lifetime and the energy supplied by the
batteries.
CoexistenceofWirelessSystemsforRemoteMonitoringofVitalFunctionsintheUnlicensedISMBand
629
2.1 Multifunctional Wireless Body
Sensor
In this section, we discuss the initial, current and
future design of our custom developed
multifunctional wireless body sensor (MWBS)
guided by the requirements for WBAN.
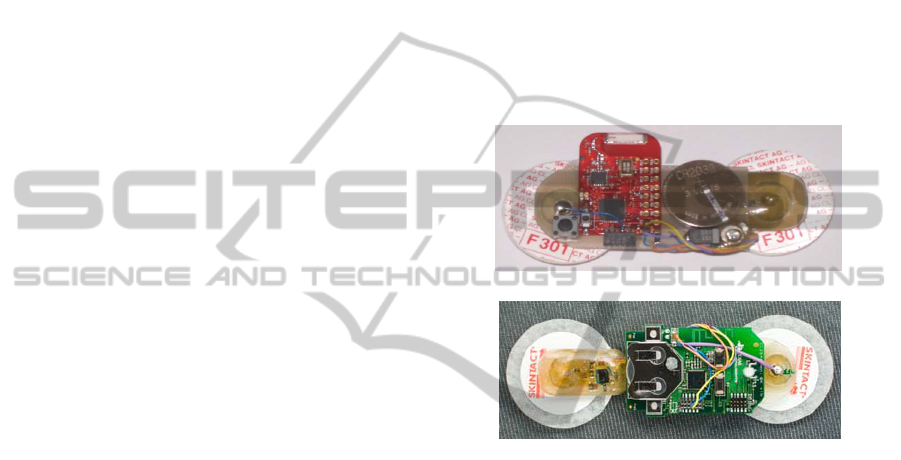
2.1.1 Initial Design
As an initial design, we prototyped a differential
wireless bio-electrode (WBE) for measuring ECG
and EEG (Trobec, et al., 2010). An example of the
prototype electrode is shown in Fig. 1a. The WBE
consists of two self-adhesive electrodes (which need
to be positioned at a distance of 5 cm when
performing measurements), a signal amplifier, a
microcontroller and a low-power 2.4 GHz radio
(Texas Instruments CC2500). It enables minimal use
of wires on the body and consequently maximal
wearing comfort. A coin battery powers the WBE.
When placed on the body surface near the heart, the
WBE measures the potential difference between the
electrodes and records a raw ECG signal. Triggered
by an internal clock, the WBE performs sampling of
the analogue signal and conversion of each sample
to a 10 bit digital signal. Seven consecutive samples
are collected into a buffer, labelled with a source
timestamp and then transmitted via SimpliciTI
wireless transmission protocol
(http://www.ti.com/simpliciti).
Other relevant data can be extracted from the raw
ECG signal using additional signal processing. First,
the WBE provides an alternative that resolves the
standard 12-lead ECG devices imperfections. The
measurements from three WBEs can form a lead
system that can potentially be used for
reconstruction of the 12-lead ECG (Tomašić, et al.,
2013; Trobec & Tomašić, 2011). Next, the ECG-
Derived Respiration (EDR) techniques are based on
the observation that the positions of the ECG
electrodes on the chest surface move relative to the
heart. We have confirmed that EDR is a viable
option for monitoring of the respiration frequency
and for rough classification of the breathing types
(Trobec, et al., 2012).
2.1.2 Current Design
The initial design has been upgraded to support the
newest version of Bluetooth technology – low
energy Bluetooth 4.0 (BLE) for transmission of
measured data from the MWBS. It enables direct
communication between the MWBS and
smartphones and devices with incorporated low
energy Bluetooth. An example of the current
prototype electrode is shown in Fig. 1b.
The Bluetooth low energy protocol is low-cost
wireless solution designed to meet special
requirements for long-term operation in devices with
limited energy capacity (e.g. coin-cell battery). Its
ultra-low peak, average and idle mode power
consumption and enhanced working range enable
the MWBS to operate on a single coin-cell battery
for several days while transmitting live stream of
raw ECG data (Bregar & Avbelj, 2013). The
maximal bit-rate of the data payload is 1 Mb/s,
which is sufficient also for high-resolution short-
term measurements.
(a)
(b)
Figure 1: (a) A prototype of the WBE with two self-
adhesive disposable electrodes, a lithium coin battery and
a ceramic chip antenna. (b) A prototype of the MWBS
with two self-adhesive disposable electrodes, a lithium
coin battery, a microprocessor, a BLE radio, and a printed
circuit board antenna.
2.1.3 Future Design
In future, with respect to data collection, more
sensors will be incorporated into the final version of
the MWBS, including sensors for measuring beat
rate, vascular pressure, oxygen saturation, skin
resistance, temperature, etc. Furthermore,
microphones, accelerometers and video sensors
could offer additional contextual data that could
contribute to a better estimate of the status of the
monitored patient. We envisage the use of advanced
signal processing techniques before transmission and
cognitive communications techniques to mitigate the
interference in the increasingly crowded ISM band.
HEALTHINF2015-InternationalConferenceonHealthInformatics
630
3 REMOTE HEALTH
MONITORING SYSTEM
ARCHITECTURE
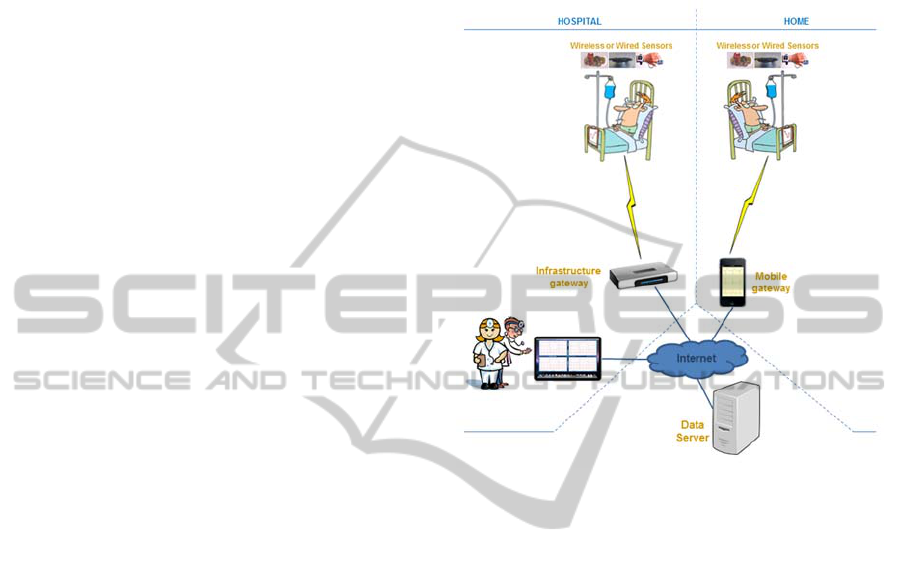
The scheme of the proposed wireless system for
remote monitoring of vital functions is shown in Fig.
2. The system establishes a virtual state of a semi-
intensive care unit, which significantly improves the
quality of hospital care. Patients are fitted with body
sensors for vital functions. The primary concern of
the system is reliable transfer of the collected data
from the sensors to a computer server that maintains
a database and is responsible for processing,
presentation, alerting and taking necessary actions.
Once the data resides on the server, the users of the
systems (patients/physicians/doctors) can access the
collected data in the database via a terminal of their
choice. The transfer of data from the sensors to the
data server is achieved through appropriate gateways
equipped with Internet connection. Before reaching
such a gateway, the data can be transferred through a
multi hop connection between intermediate devices.
We account as gateway not only a wireless static
gateway in the traditional sense, but also personal
terminals, such as smartphones and tablet PCs with
the ability for wireless transmission. Therefore, we
can distinguish two modes of operation. In the first
mode, more suitable for a home environment, the
personal terminal will act as a primary mobile
gateway (Pesko, et al., 2014). The data from the
sensors is transmitted for representation and/or
storing on the personal terminal. This can be
achieved with direct communication between the
sensor node and the mobile gateway (for example,
using a BLE link). The measurements are stored in
the personal terminal for preliminary monitoring and
processing with automated procedures based on the
comparison with threshold values, predetermined
rules and automatic learning. Furthermore, the
measured data is also sent to the remote data server.
In the second mode, more suitable for a hospital
environment, the data from sensors to the server is
transferred using fixed wireless infrastructure
gateways located in patients’ rooms and hospital
hallways. By using infrastructure gateways, the
coarse indoor location of the patient can be also
determined, which is not always the case when using
personal terminals. In this scenario, the personal
terminals should be considered as a secondary
device, serving more for preliminary representation
and processing of the data. Increasing the number of
redundant low cost wireless nodes can create a more
robust communications network. An ad-hoc network
with an appropriate multi-hop routing protocol and
redundant wireless nodes can provide redundant
communication pathways to the nearest wireless
gateway node (Biagioni & Chen, 2004; Jingling, et
al., 2010).
Figure 2: Conceptual scheme of the wireless system for
remote monitoring of vital functions.
3.1 Coexistence Issues in a Remote
Health Monitoring Wireless System
In the following, we discuss the applicability of the
concept of cognitive communication to the wireless
system for remote health monitoring.
3.1.1 Spectrum Sensing and Dynamic
Spectrum Access
Because of the requirements for low power
consumption in WBAN, a prerequisite for successful
operating frequency adaptation in WBAN is energy
efficient spectrum sensing. Spectrum sensing is a
highly demanding signal processing task, since the
radio signals in WBAN are weak and with possible
large background noise. Several research activities
have been carried out in order to evaluate different
approaches for energy-efficient spectrum sensing
under various assumptions (Biagioni & Bridges,
2002; Rohde & Toftegaard, 2011). Energy
harvesting has been also proposed as a solution to
complement the power supply requirements in the
context of cognitive sensor nodes (Barroca, et al.,
2012).
CoexistenceofWirelessSystemsforRemoteMonitoringofVitalFunctionsintheUnlicensedISMBand
631

Since hospitals represent a complex dynamic
ISM band radio environment, it is generally not
suitable to rely on WBAN devices capable of
accurate sensing and independent decision making.
A more viable solution is thus to equip the hospital
rooms and wards with spectrum sensing nodes,
similar as there are Wi-Fi access points, and use the
collected information to build an indoor radio
environment map (REM) (Atanasovski, et al., 2011).
REM can be built and maintained centrally or in a
distributed manner, and provides knowledge about
radio signal coverage and interference levels to a
dynamic spectrum management (DSM) system.
Furthermore, such centrally managed system can
assist in indoor localization of patients, personnel
and even equipment/instruments if equipped with
detectable radio devices.
3.1.2 Power and Mobility Management
In the described scenarios, problems can occur when
the patient moves with all the sensors attached,
which can cause for the sensors to lose their primary
point of connection to the gateway. Moreover, while
moving, the radio-operating environment can change
dynamically as there may be other transmitters
causing interference or ambient noise that can cause
data loss. Therefore, in a mobility scenario, since
nodes frequently change position, also some transmit
power level adjustments should be considered. For
example, when nodes are close to each other, their
transmission power can be lowered. Hence,
mobility-aware dynamic spectrum management
solutions must be incorporated. This means that in a
cognitive WBAN for medical applications in
unlicensed bands, depending on the protocol, either
the transmitting nodes need to have the capability to
perform cognitive functions or the network should
incorporate a smart scheduler.
In the search for solutions, it makes perfect sense
to base the implementations of cognitive
communications on one or more existing standards.
Moreover, using existing standards will also provide
compatibility with legacy devices already in
operation. Typical wireless technologies suitable for
use in WBAN are Bluetooth (based on IEEE
802.15.1), ZigBee (based on IEEE 802.15.4) and
802.11/WiFi (Golmie, et al., 2005). Bluetooth is
particularly suitable since its 4.0 version, as BLE-
supported devices can transmit low power in the
2.4 GHz worldwide ISM band.
Besides optimising to the required range, the
transmit power can also be optimised according to
the priority of the information from a given sensor
node. Sensor nodes can be grouped into nodes with
critical traffic and non-critical traffic. Transmission
for critical nodes would be prioritized over
transmissions for non-critical nodes by using higher
transmission power for critical traffic and lower
transmission power for non-critical traffic.
3.1.3 Optimal Assignment of Wireless
Interfaces
On the end-to-end network level, the transport
services should provide service delivery in
accordance with specific performance criteria and
cost parameters. In a heterogeneous wireless access
system, typical for the ISM band operating
environment, sensor units as well as mobile and
fixed infrastructure gateways may support multiple
wireless interfaces and have the ability to optimally
switch between them (Fortuna, et al., 2008). In
doing so, they may take into account operating
parameters (interference level, energy consumption,
etc.), transmission parameters (delay, bandwidth,
data priority level, etc.), application requirements
(presentation on intermediate devices, need for
advanced processing, etc.), and others.
4 CONCLUSIONS
In this paper, we addressed the coexistence of
medical WBANs for remote health monitoring with
other wireless networks operating in the shared ISM
frequency band. The trend of this type of networks is
towards implementation in already crowded
unlicensed frequency bands, characterised by
interference that may severely affect the
performance and reliability of very low power
devices such as WBSs. In order to reduce the
interference from other wireless systems and
enhance the performance, we discussed the
applicability of the concepts of cognitive
communications to medical WBAN systems,
pointing out dynamic access to temporarily available
spectrum, adjusting transmit power to operating
conditions and data priority, and setting up most
appropriate end-to-end transmission path.
REFERENCES
Atanasovski, V. et al., 2011. Constructing Radio
Environment Maps with Heterogeneous Spectrum
Sensor. IEEE Symposium on New Frontiers in
Dynamic Spectrum Access Networks (DySPAN 2011),
HEALTHINF2015-InternationalConferenceonHealthInformatics
632

3-6 May, pp. 660-661.
Baard, E., 2001. People Power: Capturing The Body’s
Energy For Work On and Off Earth. (Online)
Available at: http://extropians.weidai.com/extropians.
4Q01/3513.html (Accessed September 2014).
Barroca, N. et al., 2012. Electromagnetic Energy
Harvesting for Wireless Body Area Networks with
Cognitive Radio Capabilities. Proceedings of URSI.
Biagioni, E. & Bridges, K., 2002. The Application of
Remote Sensor Technology to Assist the Recovery of
Rare and Endangered Species. Special issue on
Distributed Sensor Networks for the International
Journal of High Performance Computing
Applications, Volume 16, pp. 315-324.
Biagioni, E. & Chen, S., 2004. A Reliability Layer for Ad-
Hoc Wireless Sensor Network Routing. Proceedings
of the 37th Annual Hawaii International Conference
on System Sciences.
Bregar, K. & Avbelj, V., 2013. Multi-Functional Wireless
Body Sensor - Analysis of Autonomy. Proceedings of
MEET & GVS on the 36th International Convention
MIPRO 2013, pp. 346-349.
Chaboyer, W. et al., 2008. Predictors of Adverse Events in
Patients After Discharge From the Intensive Care Unit.
Am. J. Crit. Care, Volume 17, pp. 255-263.
Coronel, P. et al., 2004. Wireless body area and sensor
networks. Wireless World Research Forum, Briefings.
Cotton, S. L. & Scanlon, W. G., 2007. Characterization
and modeling of the indoor radio channel at 868 MHz
for a mobile bodyworn wireless personal area network.
IEEE Antennas and Wireless Propagation Letters,
Volume 6, pp. 51-55.
Drude, S., 2007. Requirements and Application Scenarios
for Body Area Networks. Mobile and Wireless
Communications Summit, 16th IST.
Dzenowagis, J. & Kernen, G., 2005. Connecting for
health: global vision, local insight: Report for the
World Summit on the Information Society, Geneva:
World Health Organization.
Ekeland, A., Bowes, A. & Flottorp, S., 2010.
Effectiveness of telemedicine: A systematic review of
reviews. Int. J. Med. Inform, Volume 79, pp. 736-771.
European Union, 2004. eHealth Ministerial Declaration,
22 May 2003. In: E-Health: Current Situation and
Examples of Implemented and Beneficial E-Health
Applications. Brussels: IOS Press, pp. 35-38.
Fortuna, C. & Mohorčič, M., 2009. Trends in the
development of communication networks: Cognitive
networks. Computer Networks, Volume 53, pp. 1354-
1376.
Fortuna, C., Mohorčič, M. & Filipič, B., 2008.
Multiobjective Optimization of Service Delivery Over
a Heterogeneous Wireless Access System.
Proceedings of the IEEE International Symposium on
Wireless Communication Systems, ISWCS 2008, pp.
133-137.
Golmie, N., Cypher, D. & Rebala, O., 2005. Performance
analysis of low rate wireless technologies for medical
applications. Computer Communications, Volume 28,
pp. 1266-1275.
Ikehara, C. S., Biagioni, E. & Crosby, M. E., 2007. Ad-
Hoc Wireless Body Area Network for Augmented
Cognition Sensors. In: D. Schmorrow & L. Reeves,
eds. Augmented Cognition. Berlin, Heidelberg:
Springer-Verlag, p. 38–46.
Jingling, F., Wei, L. & Yang, L., 2010. Performance
Enhancement of Wireless Body Area Network System
Combined with Cognitive Radio. Proceedings of the
International Conference on Communications and
Mobile Computing, CMC 2010, pp. 313-317.
Pesko, M. et al., 2014. Smartphone with augmented
gateway functionality as opportunistic WSN gateway
device. Wireless Personal Communications, Volume
78, pp. 1811-1826.
Rohde, J. & Toftegaard, T. S., 2011. Adapting Cognitive
Radio Technology for Low-Power Wireless Personal
Area Network Devices. Wireless Pers. Commun.,
Volume 58, pp. 111-123.
Steenkiste, P., Sicker, D., Minden, G. & Raychaudhuri,
D., 2009. Future Directions in Cognitive Radio
Network Research. NSF Workshop Report.
Tomašić, I., Frljak, S. & Trobec, R., 2013. Estimating the
universal positions of wireless body electrodes for
measuring cardiac electrical activity. IEEE Trans. Inf
.Technol. Biomed., Volume 60, pp. 3368-3374.
Trobec, R., Depolli, M. & Avbelj, V., 2010. Wireless
network of bipolar body electrodes. Proceedings of the
7th International Conference on Wireless On-demand
Network Systems and Services, WONS 2010, p. 145–
149.
Trobec, R., Rashkovska, A. & Avbelj, V., 2012. Two
proximal skin electrodes – a body sensor for
respiration rate. Sensors, Volume 12, pp. 13813-
13828.
Trobec, R. & Tomašić, I., 2011. Synthesis of the 12-lead
electrocardiogram from differential leads. IEEE Trans.
Inf .Technol. Biomed., Volume 15, pp. 615-621.
World Health Organization, 2006. eHealth tools and
services: Needs of the Member States. Report of the
Global Observatory for eHealth.
CoexistenceofWirelessSystemsforRemoteMonitoringofVitalFunctionsintheUnlicensedISMBand
633
