
Using Domain Knowledge to Improve Intelligent Decision Support in
Intensive Medicine
A Study of Bacteriological Infections
Rui Veloso
1
, Filipe Portela
1
, Manuel Filipe Santos
1
, Álvaro Silva
2
, Fernando Rua
2
,
António Abelha
1
and José Machado
1
1
Algoritmi Centre, University of Minho, Guimarães, Portugal
2
Serviço Cuidados Intensivos, Centro Hospitalar do Porto, Hospital Santo António, Porto, Portugal
Keywords: Antibiotics, Therapies, Infections, Bacteria, Intensive Care Units, Heuristics, Artificial Intelligence,
INTCare, Decision Support.
Abstract: Nowadays antibiotic prescription is object of study in many countries. The rate of prescription varies from
country to country, without being found the reasons that justify those variations. In intensive care units the
number of new infections rising each day is caused by multiple factors like inpatient length of stay, low
defences of the body, chirurgical infections, among others. In order to complement the support of the
decision process about which should be the most efficient antibiotic it was developed a heuristic based in
domain knowledge extracted from biomedical experts. This algorithm is implemented by intelligent agents.
When an alert appear on the presence of a new infection, an agent collects the microbiological results for
cultures, it permits to identify the bacteria, then using the rules it searches for a role of antibiotics that can
be administered to the patient, based on past results. At the end the agent presents to physicians the top-five
sets and the success percentage of each antibiotic. This paper presents the approach proposed and a test with
a particular bacterium using real data provided by an Intensive Care Unit.
1 INTRODUCTION
Infections are the principal cause of mortality in
Intensive Care Units (ICU) both in Europe (Angus et
al., 2001) and USA (Vincent et al., 2006). According
to the medical community this type of problem is
most common in patient with more than five days of
stay.
Vincent et al. (2009) conducted a study about
infections in the ICU. In this study it was evaluated a
set of patient where 50% of the patients had an
infection. From the infected patients, in 70% of the
cases were prescribed therapeutics associated with
antibiotics and microbiological cultures being in
generally obtained positive results.
The antibiotic prescription varies pretty much
from country to country, being the reason unknown
(Lindbaek, 2006).
In many cases the patient body resists to the
administered antibiotic, being necessary to test and
prescribe another antibiotic. The main purpose of
this work is to explore a complementary approach in
order to support the decision process related to
infections. This work aims to answer to the question
“Is it possible to use an intelligent approach in
order to support the infection decision process?”
This paper introduces an algorithm based in the
heuristic concept to provide information about
alternative antibiotics that can have success in
control of a particularly infection.
The algorithm will be embedding in an
intelligent decision support system for intensive
medicine – INTCare system. The system is based
on agents responsible to collect and process the data
in real-time. The heuristic aims for scanning new
infections or patterns of infections. Whenever an
infection is found the system automatically runs the
algorithm returning to the clinical staff a list of
possible antibiotics that can be administered to the
patient.
The algorithm is responsible for finding the best
treatments for a specific infection. The system
searches all the treatments performed in the past and
based on the patient clinical data, admission
582
Veloso R., Portela F., Filipe Santos M., Silva Á., Rua F., Abelha A. and Machado J..
Using Domain Knowledge to Improve Intelligent Decision Support in Intensive Medicine - A Study of Bacteriological Infections .
DOI: 10.5220/0005286405820587
In Proceedings of the International Conference on Agents and Artificial Intelligence (ICAART-2015), pages 582-587
ISBN: 978-989-758-074-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

variables like age and sex, and shows some
alternative treatments that can achieve success in the
combat of the infection. This research also considers
factors like the cost, successful cases and expected
time to the antibiotic produce effect.
The system returns then a set of treatments
successfully applied in the past using input variables
similar to the patient data (case based approach).
To test this system they were used real data
provided by Intensive Care Unit of Centro
Hospitalar do Porto (CHP), Porto, Portugal. All of
this work is inserted in the INTCare research project.
This article is divided into five sections. The first
one consists in the introduction of the paper. The
main concepts and related work are described in
background that is the section number two of this
paper. On the third section it is described the data
analysis, the data transformations and it is presented
the heuristic algorithm and achieved results with the
application of the heuristic. Then in the section four
it is analysed and discussed the results and on the
last section they are presented some considerations
as well the future work.
2 BACKGROUND
2.1 Infection, Bacteria and Antibiotics
in Healthcare
Among bacteria, viruses, fungi and parasites, a very
small amount of these organisms are linked to the
development of infections, usually called pathogens.
An infectious disease is normally characterized by
symptoms like fever, pain and swelling and others
more specific to the organs that the infection is
affecting. The diagnosis of an infection is done
recurring to the isolation of a pathogen and grown of
them in artificial cultures. So these pathogens can be
identified and then it is administrated to the patient
the most convenient antibiotic (Ryan et al., 2004).
In Europe in each year about 4 million of
patients acquire an infection associated to healthcare
and approximately 37000 of them dies from the
contracted infection. The most common infections in
healthcare are: respiratory, urinary, surgical,
gastrointestinal and bloodstream (ECDC, 2012).
Bacteria are microorganisms; the smallest among
the living cells, without nucleus but all of them have
the nucleic acid and protein synthesis (Ray et al.,
2004).
The most common bacteria in healthcare are
Escherichia Coli, Pseudomonas aeruginosa,
Candida and Enterococcus species (ECDC, 2012).
The Pseudomonas aeruginosa is a common bacteria
from the Gram-negative class, it is a common
pathogen in inpatients with a length of stay superior
to one week. The infections provoked by this
pathogen are many and can be located on respiratory
track (pneumonia), heart (endocarditis), bloodstream
(bacteraemia) among others (Ray et al., 2004).
2.2 Heuristics
The term heuristic comes from the Greek and means
“to find out, discover”. Romanycia and Pelletier
(1985) created a survey of definitions and concluded
that a heuristic is a device that is used in problem
solving. It can be a strategy, knowledge, computer
program, data structure and have to guarantee the
supply of a solution. The heuristic developed in this
work is based on the medical domain knowledge
about antibiotics and infections in intensive
medicine.
2.3 INTCare
This study is being developed under the research
project INTCare. INTCare is an Intelligent Decision
Support System (IDSS) that is in constant
development and testing. It is deployed in the ICU
of the Centro Hospitalar do Porto (CHP). This IDSS
is based on intelligent agents (Santos et al., 2011)
and aims to predict clinical events as patient organ
failure (cardiovascular, respiratory, renal, hepatic,
neurological and hematologic systems), possible
readmissions, diseases, infections and patient
outcome (Portela et al., 2013). The system is able to
suggest procedures, treatments and therapies. This
system is based in four subsystems (data acquisition,
knowledge management, inference and interface)
that recur to intelligent agents in order to take
actions (Portela et al., 2013).
3 STUDY DESCRIPTION
3.1 Data Understanding
As above referred the administration of antibiotics is
an important issue because there is a great number of
particularities that should be analysed in the
treatment of infections. The system developed for
this study tries to eliminate some of those issues. In
order to analyse and identify treatment patterns it is
necessary to provide input variables for the system.
After some meetings with the medical staff of the
CHP it was defined a fixed variables package.
UsingDomainKnowledgetoImproveIntelligentDecisionSupportinIntensiveMedicine-AStudyofBacteriological
Infections
583
Independently the type of infection, it should be
always considered four type of variables. They are
age, sex, leucocytes and days of internment. The
remaining variables are related with the organic
system that the infection is affecting: cardiovascular,
respiratory, hepatic, renal, neurological and
hematologic. For the study it was considered
infections provoked by the Pseudomonas aeruginosa
a bacteria that typically affects the respiratory
system. To induce the models they were used four
variables related with this system: SPO2, PCO2 and
PaO2.
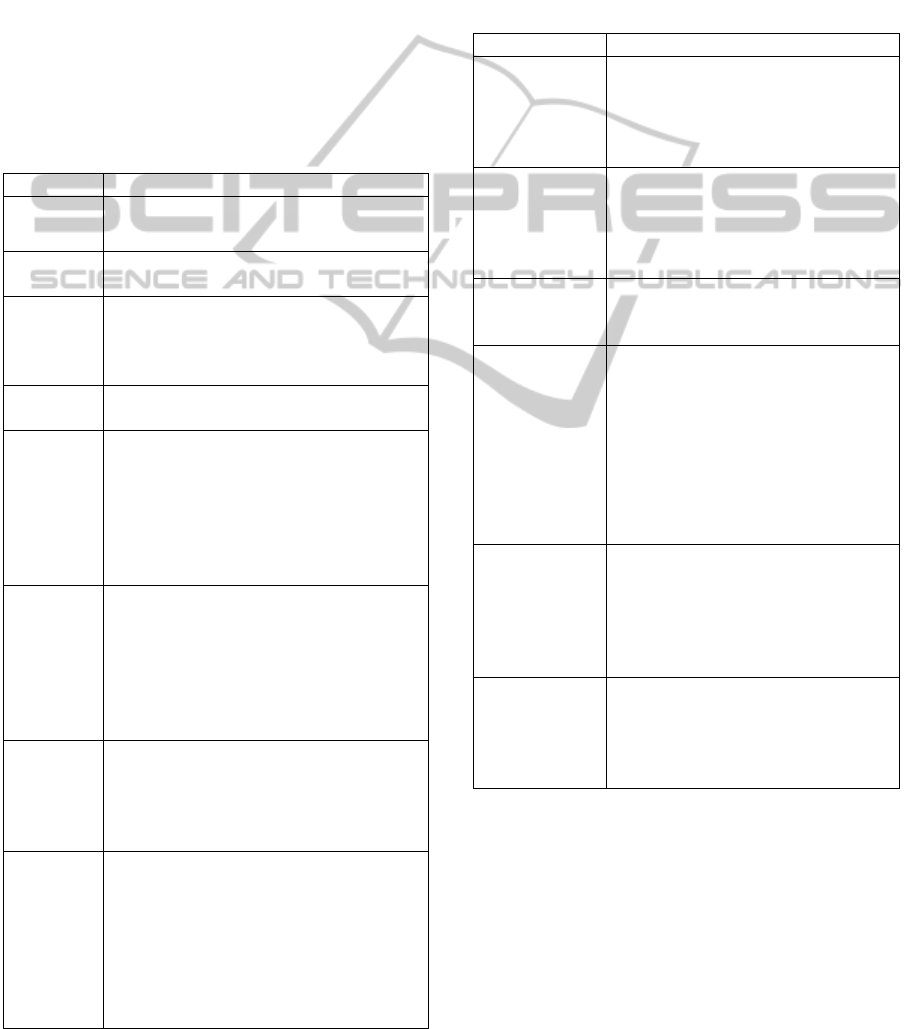
Table 1 shows the used variables for this study
on the first part of the heuristic algorithm and a brief
description of each one.
Table 1: Variables Used for Search.
Variable Description
age The patient age in years
sex
Information about the patient sex. Can be
male or female.
leuc
Leucocytes – quantity of leucocytes referred
in the laboratory analysis with the closest
date of the date in where the infection
appears.
doi
Length of stay – the number of days that the
patient is hospitalized in the ICU.
SPO2
Peripheral capillary oxygen saturation – is
an estimation of the oxygen saturation level.
Normal values are considered 95% to 100%.
Between 90% and 95% the oxygen
saturation is low but not necessarily
represents a health issue and below 90% is
considered that a patient is in hypoxemia.
PaCO2
Partial pressure of carbon dioxide –
Represents the partial pressure of CO2 in
arterial blood and expresses the
effectiveness of the alveolar ventilation.
Normal values are between 35 to 45 mm
Hg. If the value is higher than 45 mmHg the
patient is in hypercapnia.
PaO2
Oxygen partial pressure – refers to the
measurement of oxygen in the arterial
blood. The normal range is between 75-100
mm Hg. If the value is below that the
patient is not receiving enough oxygen.
PaO2/FIO2
Ratio of the oxygen partial pressure and
fraction of inspired oxygen – compares the
level of oxygen level in the blood with the
oxygen that is breathed. It’s very useful do
check if exists problems with how lungs
transfer the oxygen to the blood. If the ratio
is below to 250 mm Hg is one of the criteria
of evaluation for pneumonia.
The variables described in table 1 belong to the
search variables group. In order to perform the
heuristic algorithm it is necessary to have a set of
data containing results of past treatments. The
variables represented in this set, are the variables
mentioned in table 1 plus the variables: culture,
antibiotic, antibiotic result, days of treatment and
cost. Table 2 shows the variables present in the set
of data related with the past results.
Table 2: Variables related with past results.
Variable Description
tage, tsex,
tleuc, tdoi,
tSPO2,
tPaCO2,tPaO2,
tPaO2/FIO2
The variables represent the same
results as the ones from Table 1, but
it was added the prefix t for
treatment.
culture
Represents a positive case for some
bacteria. For example if the field as
the text “pseaer” it means the data
from that row represents a positive
case of pseaer bacteria.
antibiotic
This field represents the antibiotic
given to a patient in order to combat
bacteria.
antibiotic
result
The antibiotic result assumes two
results: positive and negative. If the
value is positive it means that the
antibiotic succeeds and the infection
is being stopped. If the value is
negative, it means the antibiotic did
not produce curative effects and it
was necessary to try with another
antibiotic.
Treatment
days
Is the number of days that the
antibiotic was administrated until
makes effect on the combat to the
infection. If the value is null it means
the antibiotic was not suited for the
bacteria.
cost
Represents the cost of the antibiotic
administration. This value is
obtained multiplying the unitary cost
of the dose by the number of days of
treatment.
In order to test the proposed algorithm it was used a
dataset of historic treatments. This dataset only
contains 275 rows referring to 42 inpatients
treatments using 5 different antibiotics. The dataset
size is small because at the moment there are some
laboratory results in a closed format which means
that we do not have access to the results of all the
bacteriological analysis. However to test this
approach the dataset is enough because it represents
a complete sample of an infection.
ICAART2015-InternationalConferenceonAgentsandArtificialIntelligence
584
3.2 Heuristic Approach
The heuristic searches for new infections and
patterns that can indicate an infection. When an
infection is detected it will wait for the results of
cultures analysis. When the culture results denote
the presence of a bacterium a search is performed for
looking for possible treatments.
Next, for a better understanding, an example will
be given using a real data for pseaer bacterium.
Despite of this representation, the heuristic
developed can be used in another type of infection /
bacteria, by only changing the input data and output
target.
An algorithm was developed for searching
possible treatments that best suit the case. The
historic treatments and domain knowledge are used
to find the list of best treatments possible.
The system needs a dataset. These data is
represented by the following groups:
Variables searched = {doi + leuc + age + sex +
SPO2 + PaCO2 + PaO2 + PaO2/FIO2}
Treatment history = {tdoi + tleuc + tage + tsex
+ tSPO2 + tPaCO2 + tPaO2 + tPaO2/FIO2 +
culture + antibiotic + antibiotic result}
An intelligent agent is constantly monitoring the
respiratory variables and when a set of results occur
the system emits a signal alerting for a possible
infection of the patient. Then the agent waits for the
microbiological cultures results to identify the
bacteria.
If the bacteria verified in the exam it is pseaer,
the agent invokes the function treatments -
responsible to found the possible treatments. This
function compares the biological variables from the
search with the variables from past treatments
(history).
The algorithm returns results where the search
and history variables are closer using priorities in the
calculation of the difference. In this part of the
algorithm it can be returned the treatment data,
considering other factors as the days of treatment
until the antibiotic makes effect and/or the cost of
the treatment.
The variables chosen to compare the results and
their priorities were defined meeting with medical
staff of CHP and they are:
1. SPO2;
2. doi;
3. leuc;
4. PaO2/FIO2 ratio;
5. PaO2;
6. PaCO2;
7. Age;
8. Sex;
This heuristic is represented by the following
algorithm:
Algorithm - Treatment Alternatives
Requires: search variables, history variables
1:
2:
Function Evaluate Infection
Get search variables
3: If SPO2 < 90 and (PaO2 < 75 or
PaCO2 > 75) and PaO2/FIO2 < 250
then
4: For
p
atient do
5: There is an infection? - Wait for
Cultures Results
6: I
f
Pseae
r
is positive Then
7: Function Treatments
8: Else
9: Wait for positive culture
results
10:
11:
12:
End i
f
End if
End Function
13:
14:
Function Treatments
Get search variables, history of
treatmen
t
15:
16:
17:
18:
If antibiotic result = success
Treatments = results ordered
by minimum difference between
variables
Else
N
o successful treatment
19: End i
f
20: Return Treatments
21: End function
For other bacteria the process of finding the best
treatment is the same. For these types of infections
the algorithm will change heuristic remains the
same. There will be only differences on the variables
used (but the two groups are the same) and on the
first if clause of the heuristic algorithm.
3.3 Results
As above referred, to test this heuristic it was used a
dataset with past treatments applied to inpatients.
Since this study pretend to test the viability of this
concept it was given an input so the system can
search for the results which best suits the input
variables. In future the agent will do this step in real-
time and using online-learning.
UsingDomainKnowledgetoImproveIntelligentDecisionSupportinIntensiveMedicine-AStudyofBacteriological
Infections
585
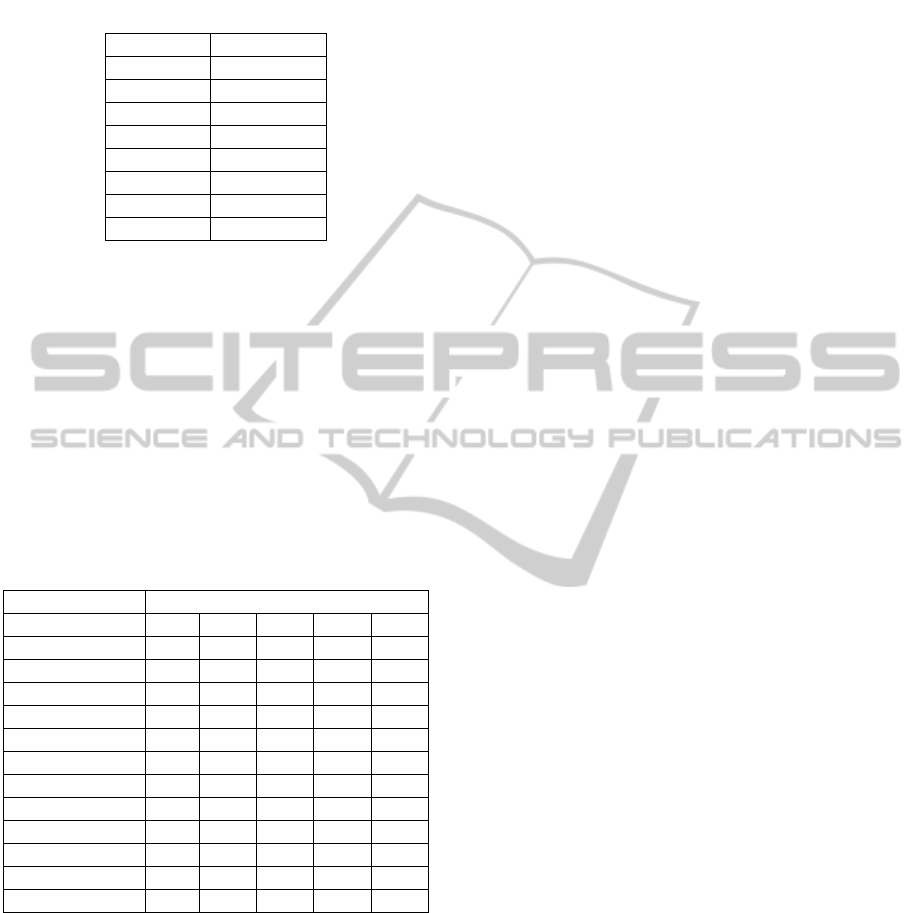
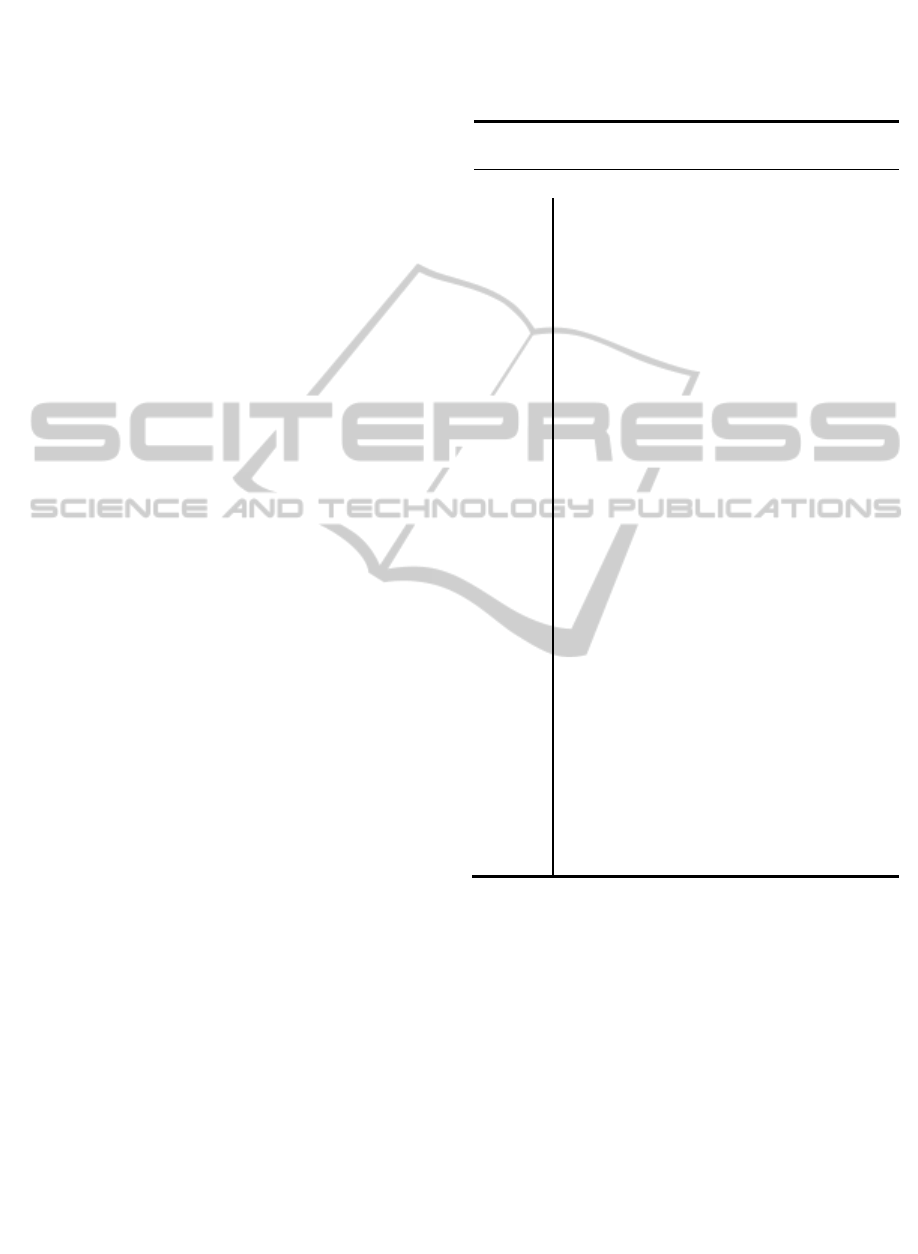
Table 3 represents the inputs given to the
algorithm – infected patient data.
Table 3: Inputs given to the algorithm.
Variable Description
doi 7
leuc 13
age 65
sex M
SPO2 90
PaCo2 41
PaO2 71
PaO2/FIO2 180
To exemplify the algorithm let’s consider a male
inpatient characterized by: Age = 65 years: Length
of stay=7 days; Leucocytes count = 13x10
9
/; SPO2 =
90%; PaCO2=41 mm Hg; PaO2=71 mm Hg; and a
PaO2/FIO2=180 mm Hg.
Given these inputs, the algorithm found 23
possible treatments. Table 4 indicates the result from
the search (top 5 results). This table presents the
historical variables values for each suggestion (R1-
R5), the antibiotic administered, the result achieved
(success or failure), the expected days for the
treatment and the treatment cost.
Table 4: Algorithm output.
Variable Results
R1 R2 R3 R4 R5
doi 8 12 7 4 12
leuc 14.5 14.2 13.2 15.2 16.1
age 70 60 80 65 60
sex M M M M F
SPO2 90 91 87 85 91
PaCo2 39.3 39.6 40.0 39.3 39.6
PaO2 71.5 73.3 70.8 57 55
PaO2/FIO2 181 194 196 198 198
Antibiotic Merop Colist Colist Fluco Pipera
Antibiotic Result Suc Suc Suc Suc Suc
Treatment Days 7 11 6 3 11
Cost 210 52 28 8 31
Along with these results the algorithm also gives
information about the support level of the
antibiotics. It is expressed in form of a percentage
and gives an overview of the antibiotics used in the
past and their success. For example, the output about
the antibiotics application for this infection is:
Meropenem (Merop) – Used successfully 5
times (26.3%); Used Unsuccessfully 14 times
(73.7%)
Colistin (Colist) – Used successfully 16 times
(52%); Used Unsuccessfully 14 times (48%)
Fluconazole (Fluco) – Used successfully 10
times (20%); Used Unsuccessfully 40 times
(80%)
Piperacillin (Pipera) – Used successfully 2
times (12.5%); Used Unsuccessfully 14 times
(87.5%)
4 DISCUSSION
Analysing the obtained results (table 4) it is possible
to observe that the algorithm suggest some treatment
options in this case the usage of colistin,
meropenem, fluconazole and piperacillin. So based
on this information the medical staff can decide on
which antibiotic should be prescribed using as base
the suggestions made by the algorithm.
The approach developed will be improved and
embedded into the INTCare System. The results will
be available anywhere and anytime by whom have
access privileges.
With this algorithm it is possible to observe a list
of treatments that can produce effects in the combat
of pseaer bacteria. By analysing this information the
clinical staff can have an idea about which is the
more adequate antibiotic.
The system proposes some scenarios about
treatments, eliminating at the start past treatments
which not produce any effect or that have very low
taxes of success.
The physicians are always responsible by the
final decision. The heuristic only is used to help
them to take the better decision in the patient best
interest.
5 CONCLUSIONS AND FUTURE
WORK
This study explored an approach using the heuristic
concept to develop a searching algorithm for
combating infections in order to help the doctors
taking better decisions and saving lives. The domain
knowledge combining literature and empirical
knowledge of the medical staff was crossed with
patient and antibiotic data in order to obtain the
rules. Additionally, this approach introduces the cost
factor in the decision criteria.
Preliminary results demonstrate de utility of the
approach and encourage further work in a wider
scope and the integration of the heuristic in INTCare
system in order to complement data mining
predictive models.
ICAART2015-InternationalConferenceonAgentsandArtificialIntelligence
586

The algorithm is represented by a set of rules that
can be easily stored in a knowledge base and
adapted to other infections.
Future work will include the development of an
intelligent agent to search and use:
other infections and bacteria;
other patient data to improve the heuristic.
ACKNOWLEDGEMENTS
This work has been supported by FCT – Fundação
para a Ciência e Tecnologia in the scope of the
project: Pest-OE/EEI/UI0319/2014 and PEst-
OE/EEI/UI0752/2014.
The authors would like to thank FCT
(Foundation of Science and Technology, Portugal)
for the financial support through the contract
PTDC/EEI-SII/1302/2012 (INTCare II).
REFERENCES
Angus, D.C., Linde-Zwirble, W.T., Lidicker, J., Clermont,
G., Carcillo, J., Pinsky, M.R., 2001. Epidemiology of
severe sepsis in the United States: analysis of
incidence, outcome, and associated costs of care. Crit.
Care Med. 29, 1303–1310.
ECDC, 2012. Surveillance of healthcare-associated
infections in Europe 2007. European Centre for
Disease Prevention and Control. Surveillance Report
from ECDC, Stockolm.
Lindbaek, M., 2006. Prescribing antibiotics to patients
with acute cough and otitis media. Br. J. Gen. Pract.
56, 164–165.
Portela, F., Pinto, F., Santos, M.F., 2012. Data mining
predictive models for pervasive intelligent decision
support in intensive care medicine.
Portela, F., Santos, M.F., Machado, J., Abelha, A., Silva,
Á., 2013. Pervasive and Intelligent Decision Support
in Critical Health Care Using Ensembles, in: Bursa,
M., Khuri, S., Renda, M.E. (Eds.), Information
Technology in Bio- and Medical Informatics, Lecture
Notes in Computer Science. Springer Berlin
Heidelberg, pp. 1–16.
Santos, M.F., Portela, F., Vilas-Boas, M., 2011.
INTCARE : multi-agent approach for real-time
intelligent decision support in intensive medicine.
SciTePress.
Ray, C. George, 1934- & Ryan, Kenneth J. (Kenneth
James), 1940- & Sherris, John C & ebrary, Inc 2004,
Sherris medical microbiology: an introduction to
infectious diseases, 4th ed, McGraw-Hill, New York.
Romanycia, M.H. J., Pelletier, F. J., 1985. What is a
Heuristic?. Computational Intelligence, 1, 47-58.
Vincent, J.-L., Rello, J., Marshall, J., Silva, E., Anzueto,
A., Martin, C.D., Moreno, R., Lipman, J., Gomersall,
C., Sakr, Y., Reinhart, K., EPIC II Group of
Investigators, 2009. International study of the
prevalence and outcomes of infection in intensive care
units. JAMA 302, 2323–2329.
doi:10.1001/jama.2009.1754.
Vincent, J.-L., Sakr, Y., Sprung, C.L., Ranieri, V.M.,
Reinhart, K., Gerlach, H., Moreno, R., Carlet, J., Le
Gall, J.-R., Payen, D., Sepsis Occurrence in Acutely Ill
Patients Investigators, 2006. Sepsis in European
intensive care units: results of the SOAP study. Crit.
Care Med. 34, 344–353.
UsingDomainKnowledgetoImproveIntelligentDecisionSupportinIntensiveMedicine-AStudyofBacteriological
Infections
587
