
Using Expressive and Talkative Virtual Characters in Social Anxiety
Disorder Treatment
Ana Paula Cláudio
1
, Maria Beatriz Carmo
1
, Augusta Gaspar
2,3
and Renato Teixeira
1
1
LabMAg, Faculdade de Ciências, Universidade de Lisboa, 1749-016 Lisboa, Portugal
2
CIS- Centro de Investigação e Intervenção Social, ISCTE Instituto Universitário de Lisboa, 1649-026 Lisboa, Portugal
3
Grupo de Psicologia, Faculdade de Ciências Humanas, Universidade Católica Portuguesa, 1649-023 Lisboa, Portugal
Keywords: Virtual Reality, Virtual Reality in Exposure Therapy (VRET), Social Anxiety, Fearing of Public Speaking,
User Study, Nonverbal Behaviour Research.
Abstract: Social Anxiety affects a significant number of people, limiting their personal and social life. We describe an
interactive Virtual Reality approach to the exposure therapy for social anxiety, resorting to virtual characters
that exhibit combinations of facial and body expressions controllable in real-time by the therapist. The
application described in this paper updates and significantly improves a former version: ameliorating the
graphical quality of the virtual characters and providing them with the ability of articulating a set of sentences.
The application executes in ordinary computers and it is easily used in counselling and research contexts.
Although we have only resorted to free or very low cost 3D models of virtual humans, we adopted strategies
to obtain an adequate final quality that we were able to validate with a significant number of observers.
Moreover, a set of therapists tested the application and gave positive feedback about its potential effectiveness
in Virtual Reality Exposure Therapy.
1 INTRODUCTION
Social phobia or Social Anxiety Disorder (SAD) is a
human condition characterized by intense anxiety
when the individual faces or anticipates public
performance (APA, 2000). This condition can be very
crippling in the personal, social and professional
domains, as those bearing it withdraw from social
contact; it also has a high comorbidity with
depression (Stein, 2000). People with SAD fear
negative social judgments and are hypervigilant for
signals in other’s behavior, thereby identifying faster
and more efficiently than other people facial clues to
threatening or negative content (Douilliez, 2012).
Therapy approaches to SAD include medication
relaxation methods, and psychotherapy, mainly
Cognitive-Behavioral Therapy (CBT). CBT produces
the most efficient and persistent improvements,
especially when it is applied as Exposure Therapy
(ET) (Beidel, 2007) which consists in exposing the
patient to the feared situation.
Virtual Reality (VR) has been used in ET since the
early 90’s, being called Virtual Reality applied to
Exposure Therapy (VRET).
Several studies have concluded that VRET
produces results that are similar to traditional
exposure therapy (Klinger, 2004; Herbelin, 2005).
VRET allows a precise control over the habituation
(and extinction) to the fear of the phobic object and
offers thus, several additional advantages over classic
ET (which is based on images and later contact with
in vivo situations).
Comparing with traditional ET, VRET presents
some important advantages: i) it allows scenario
configuration and interactions in order to fulfill each
patient’s needs and progress levels along the therapy;
ii) it provides better preparation of the patient before
facing a real life scenario, avoiding the risk of a
premature exposure to a real situation; iii) it reduces
the risk of taking steps backwards because of
overreactions, allowing a more stable and progressive
environment towards predictable and solid results; iv)
it assures patient privacy.
The downside of VRET is the cost of the
immersive virtual equipment (e.g., Head-Mounted
Displays, CAVE) and sometimes the secondary
effects reported by a few users (cybersickness)
(Laviola, 2000).
This paper describes a VR approach to the
treatment of SAD, specifically to the fear of public
speaking - before a jury in an evaluation context, in a
job interview or in some other similar scenario. The
348
Paula Cláudio A., Beatriz Carmo M., Gaspar A. and Teixeira R..
Using Expressive and Talkative Virtual Characters in Social Anxiety Disorder Treatment.
DOI: 10.5220/0005312203480355
In Proceedings of the 10th International Conference on Computer Graphics Theory and Applications (GRAPP-2015), pages 348-355
ISBN: 978-989-758-087-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

main idea is that in a session therapy, while the patient
faces a jury of one-to-three virtual characters that
show facial and body expressions, the therapist
controls these characters according to the level of
stress he/she wants to induce in the patient. This
control is accomplished through an interface (visible
only to the therapist) which, among other options,
triggers specific facial and body movements that can
be combined to convey neutral, positive or negative
emotional content, and simulate various degrees of
attention or lack of interest.
Before a therapy session, the therapist configures
the scenario by choosing the characters and their look
(hairstyle, clothes and glasses), their position at the
table and also the appearance of the room (classical
or modern furniture, different wall colors). The
simulation scenario must be projected on a canvas or
a wall, in such way that characters are displayed in
real size, enhancing the immersive effect.
Our application is also a useful tool to the
investigation of non-verbal behavior: the
communication effect related to facial or body actions
is not entirely known, and it is currently object of
intense academic debate (Gaspar 2014; Russell,
1997). The application allows the individual
visualization of a virtual human’s face (henceforth
VH) and supports many combinations of body and
facial behavioral units. It also makes possible a fine
tuning control over a single individual facial action,
whilst others are kept constant. Evaluating the impact
of these combinations in observers may clarify the
communicative role of single and composed actions,
giving clues about the treatment of social anxiety. It
may also assist various other research lines in the field
of non-verbal behavior.
The work described in this paper follows previous
work from the same team. A first version of the
application recreates an auditorium filled with virtual
characters with controllable behaviors but with few
facial expressions (Cláudio, 2013); a second version
considers a simulation of a jury composed by a set of
virtual characters with body and facial expressions
controllable by the therapist in real time (Cláudio,
2014). The development of each version has been
closely followed by a psychologist who has played a
crucial role in the identification of facial and body
expressions that potentially convey to the observer a
positive, a neutral or a negative feedback.
This paper addresses the implements included in
the present version, thus focusing the quality of the
virtual models; we report results from a validation
study concerning the VH’s facial expressions, and the
psychologist’s assumptions underpinning the creation
of the facial actions’ menu. Usability tests were
performed with experts (therapists) in order to study
the suitability of the application and its potential
effectiveness to VRET.
The document is organized as follows: next
section presents some of the most relevant work in the
area; section 3 describes our approach and the
implemented application; section 4 reports the VH’s
facial expression validation process and the
evaluation of the application by therapists; finally,
section 5 draws conclusions and lines for future work.
2 RELATED WORK
The first VR application to treat public fear before an
audience was presented in (North, 1998). This
application included a scenario with up to 100
characters. During a therapy session, the therapist was
able to vary the number of characters and their
attitudes, using pre-recorded video sequences. Patient
used an HMD, listening to the echo of his own voice.
Slater et al. created a virtual room with 8
characters with random autonomous behaviors, such
as swinging the head and eye blinking (Slater, 1999).
The initial study gathered 10 students, with different
levels of difficulty about public speaking, and was
extended later to include phobic and non-phobic
individuals (Pertaub, 2001; Pertaub, 2002; Slater,
2006).
James et al. proposed a double scenario: one
subway wagon populated by characters that express
neutral behaviors, which is considered a non-
demanding situation from a social interaction point of
view; and a more demanding situation that took place
in a bar with characters that look uninterested (James,
2003). The characters’ behavior included eye gazing
and pre-recorded sentences.
Klinger et al. conducted a study with 36
participants to evaluate changes in fear before public
speaking during 12 sessions (Klinger, 2004). To
recreate virtual characters, they used real people’s
photos in typical situations. Participants were divided
in 2 groups: one treated with CBT and the other with
VRET. A higher reduction in social anxiety was
reported in the VRET group.
Herbelin published a 200 patient validation test,
demonstrating that his platform fulfilled the
requirements of therapeutic exposure in social phobia
(Herbelin, 2005) and that clinic evaluation can be
improved with integrated monitoring tools, such as
eye-tracking.
All the referred approaches resorted to HMD
equipment; in a study described by Pertaub et al. half
of patients tried one of the virtual environments
UsingExpressiveandTalkativeVirtualCharactersinSocialAnxietyDisorderTreatment
349
through a HMD, while the rest of the group used a
desktop (Pertaub, 2002). Herbelin and Grillon, in
addition to an HMD and a computer screen also used
a big projection surface (Herbelin, 2005; Grillon,
2009).
Haworth et al. implemented virtual scenarios to be
visualized simultaneously by patient and therapist in
computer screens, possibly in different physical
locations and over the internet (Haworth, 2012).
Scenarios are oriented to patients suffering from
acrophobia (fear of heights) or arachnophobia (fear of
spiders). A Kinect is used to control patent body
movements (url-Kinect). The few results of this study
suggest that this type of low-cost solution is effective
in these phobias.
3 VIRTUAL SPECTATORS
Virtual Spectators is our VRET approach to the fear
of public speaking. The virtual scenario is, during a
therapy session, the stage to a simulation controlled
by the therapist and observed by the patient.
The application has two types of users: the
therapist as an active user, and the patient as a passive
user. The patient, while giving a speech in front of a
set of virtual humans, receives stimulus from these
characters; the therapist, who is observing patient’s
behavior and reaction to these stimulus, interacts with
the application in order to modify the simulation
accordingly, whether it is by varying the characters’
behavior, or by triggering multiple events in the
simulation scenario. The main initial scenario of the
application is configured by the therapist as well.
The equipment required to use the application is:
a computer, two sound columns, a projector and a
canvas or wall used as a projection surface. The
application generates two separate windows: the
simulation window, that must be projected, and the
interface window which is displayed in the therapist’s
computer. The sound columns must be close to the
projection to increase the degree of realism of the
simulation.
The equipment is inexpensive and it is easy to
install; the projected image should contain the models
of the VHs in real size, making it easy for the patient
to get an immersion feeling. Moreover, it is possible
to gather several people observing simultaneously the
simulation, which can be valuable in research or, for
instance, in the training of students. Additionally, all
the unpleasant secondary effects reported by some
users when using a RV equipment are eliminated.
The version here presented follows two others:
the first version simulates an audience with virtual
humans (Cláudio, 2013) and the second one a jury
composed by one to three virtual characters (Cláudio,
2014). This paper addresses the improvements
performed in this last version.
3.1 The Present Version
The main goal of this development stage in Virtual
Spectators was to provide characters with high
realism. Such goal had to be met without
compromising application’s performance, which had
to respond in real time to the therapist’s control.
Finding a balance between the characters’ final
appearance and the most critical aspects of the
application (number of polygons of the meshes, the
textures’ resolution and the complexity of the
illumination algorithms) was crucial to have the real
time response. Early on we realized that it was not
possible to improve the characters of the previous
versions. So we adopted completely distinct models.
After a series of tests, we found that the models
generated using free tools, such as MakeHuman (url-
MakeHumans) did not satisfied the aimed quality
level. Thus we shifted our approach to combining
different models (or parts of them) from the software
Poser (url-Poser) and from online repositories. In
such way, we produced two males and one female
characters appearing different ages, and named John,
Carl and Jessi (Figure 1, 2 and 3).
Figure 1: John model exhibiting two different facial
expressions.
Next, we proceeded to the animation of these
characters considering the characteristics and
functionalities of the software tools involved in the
implementation of the application: Blender (url-
Blender) and a free version of Unity3D (url-Unity).
In Unity, animations are obtained through rigging
animation, i.e., by animating a skeleton, a hierarchical
structure of interconnected bones.
The animation also comprises the process of
skinning: association of a bone to a certain set of
neighboring vertices. When a bone moves, it drags
GRAPP2015-InternationalConferenceonComputerGraphicsTheoryandApplications
350
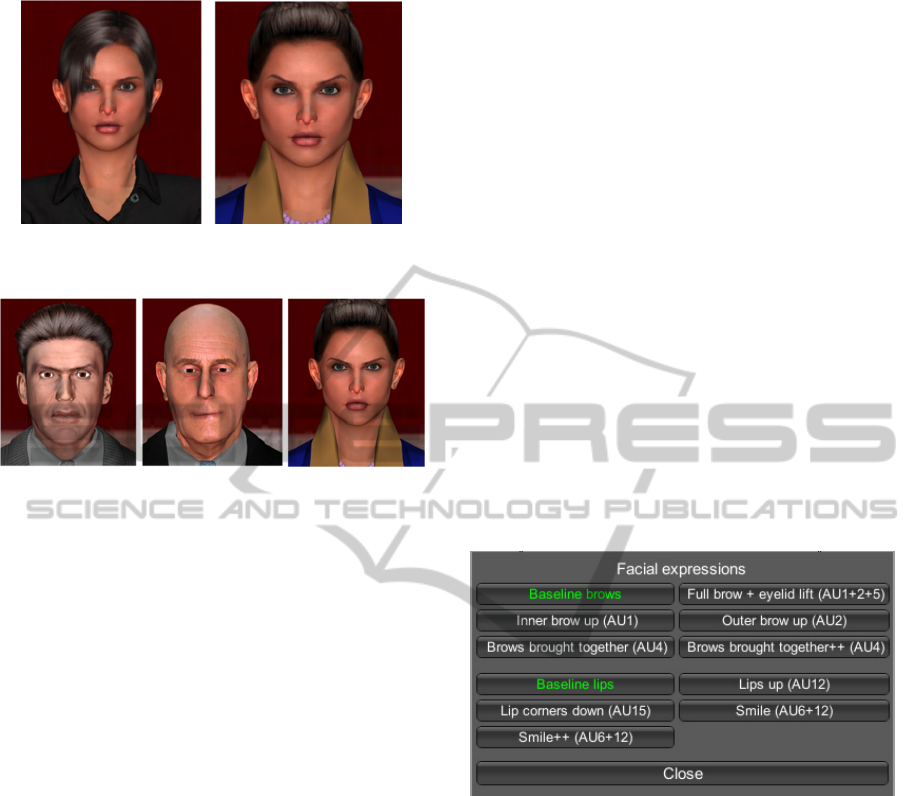
Figure 2: Jessi model exhibiting two different hair styles
and clothes.
Figure 3: Three virtual models exhibiting distinct facial
expressions (from left to right; John, Carl and Jessi).
the corresponding vertices with it; the vertices closest
to the bone suffer a bigger displacement than those
furthest away. In Blender, the association vertices-
bone and the weights that define the amplitude of the
translation are tuned resorting to a functionality called
weight painting.
In order to recycle as much as possible the
animations used in the previous version, we
proceeded to the integration of the skeleton of the old
characters into the new ones. However, the base
position of these skeletons does not match the
position of the mesh in the new characters, which
required a proper adjustment. Such adjustment led to
the modification of the base position of the skeleton
resulting in modifications in every animation that
relies on the bones used in the animation. Thus, each
animation had to be adjusted as well. Regarding
skinning, this process is created from scratch, both for
the face as for the body. Given that the three
characters are anatomically different, this exhaustive
process was repeated for every VH character.
3.2 Interface Functionalities
The current interface presents significant
improvements over the previous one in terms of
available functions, namely:
• Possibility of choosing between different
scenarios. The application is ready to new
scenarios that might be relevant to consider in the
future.
• A drag-and-drop mechanism that allows the user
to choose the characters: the user selects the
picture that represents the character and drags it to
the corresponding position in the table contained
in the virtual scenario; the photo of the character
turns grey as a sign that it is no longer available to
be chosen.
• Choosing glasses for a character previously
selected.
• Choosing a clothing style (formal or informal).
• Choosing a type of hairstyle between formal and
informal (except for Carl that is bald). Choosing
the hairstyle is independent from choosing clothes
allowing multiple combination of options.
• Character preview: therapist has the possibility to
visualize the selected and modified character with
the previous options. This preview allows a close-
up of its face.
3.3 Facial Expressions Interface
The interface that allows the user to control facial
expressions is illustrated in Figure 4.
Figure 4: The interface to manipulate facial expressions.
It contains buttons that correspond to Action
Units (AU) from Facial Action Coding System
(FACS) (Ekman, 2002); in two AUs (AU4, AU12)
there is an option to increase intensity. Our choice of
facial element to include and the universe of
expressions one can compose with them is based on
current validated knowledge on the content of human
facial behavior (for an updated review see (Gaspar,
2014)). Although there are applications, games and
films today with a wide range of expressive behavior,
the way expressive behavior is decoded by people and
what exactly do real people convey with their facial
and body behavior is still largely debated in emotion
Psychology (see (Russell, 1997)) so we opted for a
range of AUs and possible combinations, that has
been most consensually derived from behavioral
studies of spontaneous facial behavior (Gaspar, 2012;
Gaspar, 2014).
UsingExpressiveandTalkativeVirtualCharactersinSocialAnxietyDisorderTreatment
351

Furthermore, these facial compositions can also be
associated with several other body postures. Our
selection of postures is based on cross-cultural studies
of human non-verbal communication (Eibl-
Eibesfeldt, 1989).
Figure 5 shows the same model with different AU
combinations. The neutral face (upper left corner),
with no AU activated and a negative-emotion
expression, AU4 (upper right corner). In the lower
right, we see a combination of AU4 and AU15, both
related to negative affect. In the lower left corner we
see a combination of AU4 and AU6+12 (“smile”
button). The AU6+12 combination is the known as
“Duchenne smile”, and is consensually associated to
positive affect more than any other smile form.
Figure 5: Clockwise from top: a VH with a baseline face
(no AUs), displaying a frown (AU4), displaying a
combination of AU4 and AU15, displaying a combination
of AU4 and AU6+12 (the smile button).
3.4 Speaking Characters
Since our main goal is to attain realistic human-like
characters, it was considered a very important task to
include in the characters the ability of speaking.
Verbal communication plays an important role in
human interactions, reason why this requirement is
important. However, to provide a VH with the ability
to speak is a complex matter and difficult to
implement, requiring complex algorithms as well as
complex animation process. So, we conceived a
simple but effective solution.
The idea was to define a set of speeches that each
character could reproduce (with sound synchronized
with lip movements) and that were controllable and
triggered by the therapist during the simulation. On a
first trial, we implemented this solution for a single
character, John.
The main steps involved in this process are:
1. Record the intended set of speeches that will
figure in the application. It can easily be
accomplished using the microphone of a laptop.
2. Define and shape all mouth positions involved
in the process of animation of the characters
considering the sounds that need to be reproduced.
On a first instance we defined 5 shapes/states for
the Portuguese language: Base (baseline), A, E, O
and U. This means that every sound can be
obtained using only these 5 states.
3. Each shape corresponds to an animation.
Therefore, this includes a process of animating the
characters in order to be able to visually reproduce
these different states. The only bones affected
belong to the mouth area, namely, jaw and lips.
4. Decompose the sentence given as an input.
This is the sentence that the character should be
able to reproduce. Thus, any given sentence
should correspond to a sequence of animations
that the character has to process and verbalize. For
example, the sentence “Hello world” should be
translated to a language recognizable to the
character and it would correspond to the sequence
of animations (E,O,U,O,Base). This process
involves the following steps:
a) Decomposing the sentence into smaller
segments. The division of the sentence is
somewhat similar to division by syllabus.
However, each segment must contain a single
vowel. Given the example, it would be “He-
llo-w-o-rld” (in this approach, letter w is
considered as a vowel);
b) Evaluate each segment according to the
sounds each segment demands;
c) Add the corresponding animation to the buffer
of all animations that need to be played. For
example, a segment “He” will correspond to
state E, “llo” to O, and so on.
5. Reproduce sequentially all the animations. It
is defined a time interval between each animation
so that all animations can be synchronized with
the sound that starts playing as the therapist
triggers the event.
This approach provides a simple but realistic and
attractive solution. It is a good starting point towards
a more robust and complete approach. New states can
be considered in order to include a wider set of
sounds. As of now this solution only takes into
account Portuguese language so the proper
modifications are required for other languages.
GRAPP2015-InternationalConferenceonComputerGraphicsTheoryandApplications
352
4 EVALUATION AND
VA L I D AT I O N
This sections describes two evaluation tasks that have
been performed. A validation study was made to
confirm the assumptions of the psychologist in the
team during the creation of facial actions’ menu.
Additionally, we performed usability tests with a set
of experts (therapists) to study the suitability of the
application and its potential effectiveness in VRET.
4.1 Validation Phase
Beyond the theoretical framework that presided our
choice of expressive elements to include in the VHs,
derived from human behavior, it is necessary to
validate the content in the expressive behavior
displayed by the VH’s. This step precedes writing a
manual with guidelines for therapists who wish to
design a comprehensive intervention plan with the
different levels of positive/negative affect or
intimidation that the VH´s may convey. For such
purpose we have conducted a preliminary study of the
facial behavior content with a normative sample of 38
voluntary participants (31F; 7M), recruited in two
universities (ages 18- 25 yrs. old).
Participants were tested in groups of 10 and given
instructions on their appraisal tasks. These were
presented and controlled by an E-Prime 2.1
programmed experiment. Experiments took place in
a dim light room and consisted on participants
watching and rating each of 28 animated clips (3”
duration) with a close up view of a VH showing either
a neutral or an expressive face) projected on a canvas
2-3 meters in front of them. We tested expressions
comprised of the following AUs/AU combinations:
• Baseline eyebrows + Baseline lips
• Eyebrows brought together AU4
• Eyebrows brought together (more intense)++
(AU4)
• Full brow up and eyelid lift (AU1+2+5)
• Inner brow up (AU1)
• Outer brow up (AU2)
• Lips up (AU12)
• Smile (AU6+12)
• Intense smile ++ (AU6+12)
• Lip corners down (AU15)
• Eyebrows brought together++ (AU4) + Lips
up (AU12)
• Eyebrows brought together++ (AU4) + Lip
corners down (AU15)
• Inner brow up (AU1) + Lips up (AU12)
• Inner brow up (AU1) + Lip corners down
(AU15)
Clips were presented randomly to control for
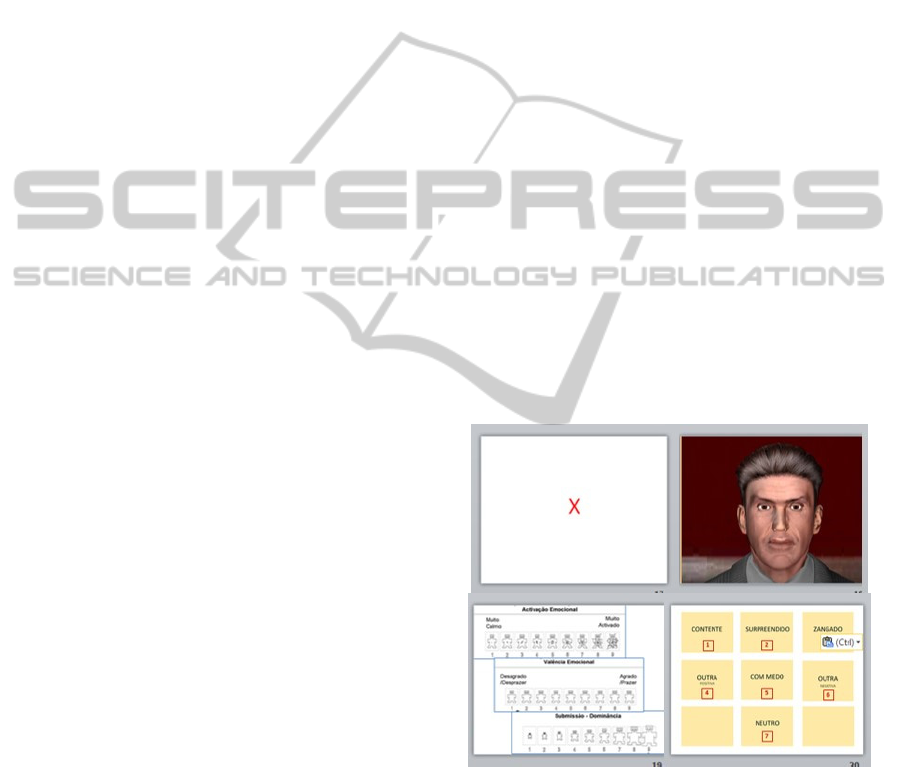
order effects. The first task consisted of rating the clip
on each of the Self-Assessment Manikin (SAM)
(Bradley, 1994) scales, a non-verbal pictorial
assessment technique that measures the arousal,
pleasure, and dominance associated with a person’s
affective reaction to an observed stimulus. The
second task consisted in choosing from a list of
emotion labels (happy, angry, surprised, fear, other
positive, other negative or neutral) the one that best
suited the face just watched (see Figure 6 with
screenshots used in the validation experiments).
Results were encouraging as they showed great
convergence in both content attribution and
emotional impact to many compositions, thus
validating our content assumptions when choosing
which expressive elements to include.
In regard to content, an independence Χ
2
test
performed on the cross tabulation of composition and
content, showed a highly significant association
between images and label (Χ
2
=2088.07; p<=.001;
N=978), with 12 out of 28 clips presenting
convergence above 75% (6 on the label angry, 4 on
happy, 1 on surprised and 1 o neutral). Convergence
was congruent with the expected content in all
convergent pictures.
Figure 6: Types of screens in the user experience.
As to emotional impact, images generally did not
elicit high Arousal (only 3 clips scored higher than
the Median). Valence was highly convergent, fitting
a narrow bell curve, with 100% of data below SD=1.9
and Mean=4.53, approaching the Median=5.
Regarding Dominance/control, 19 clips scored
higher than the Median, in an also centered
distribution where Mean=5.16 approaching the
UsingExpressiveandTalkativeVirtualCharactersinSocialAnxietyDisorderTreatment
353

Median=5 and 100% of data fell below SD=1.9; the
highest scores on feeling dominant occurred in
response to target faces that had been convergent on
positive content in the labelling task and resulted
from exposure to the female avatar, for exact same
compositions seen in male faces.
In conclusion, we were able to tabulate values for
relevant affective impact parameters - a crucial step
towards the setting up of a therapist’s manual with
validated content. It will be challenging to create
compositions that elicit higher levels of arousal and
Dominance/control. However, these may reveal
much different when the application is tested with a
clinical population, which is a future step in our
research.
4.2 Evaluation Phase
Another study was conducted with the goal of
evaluating the application on two main features:
usability and VH realism
We recruited 6 therapists (5F; 1M) ages 34- 59
years old. Within this group, only 2 elements had not
tried the previous version of the application. Tests
were conducted individually with each therapist, in a
dim light room (to improve visualization of images
and feeling of immersiveness). The apparatus for
tests was identical to that of typical application use: a
laptop computer connected to an LCD projector
displaying the image onto a projection canvas. Both
client and server were executed in localhost. Whilst
the therapist interface is shown in the laptop screen,
the client interface is projected onto the canvas
approaching real-life size. Two sound columns were
connected close to the projection canvas.
The evaluation was divided into 4 distinct phases:
character evaluation regarding realism (compared to
the previous version), usability of the implemented
functions, realism of the application as a whole, and
an open answer questionnaire section. Each part was
evaluated as the user performed each respective task.
As a result, in every section therapists considered
the new characters to be more realistic than those of
the previous version. The modifications made to the
configuration interface were welcomed as
improvements. Suggestions made to this interface
were:
• increase the number of available scenarios and
characters for higher versatility and the options
to edit each character;
• add new body animations (such as, looking at
the watch or touching the hair).
Each therapist was further asked to trigger a
specific speech in the “John” character and none had
difficulty performing this task. The favorite feature of
therapists in the new version is the VH’s ability to
speak.
Finally, every therapist mentioned that if
available, they would likely use the application in
their therapy sessions.
5 CONCLUSION AND FUTURE
WORK
One of the main questions related to the use of VRET
by the therapists is the cost of the immersive
equipment and some discomfort associated with its
use. Having this in mind, we sought to implement a
low cost solution that effectively assists in the
treatment of SAD resorting to VRET in the specific
situation of fear of public speaking, a common
problem.
The approach we propose involves ordinary
equipment: computer, sound system (two sound
columns are enough), projector and canvas (or a wall)
to project the simulations. The software for this
project (with no budget whatsoever) was developed
using freeware and free or very low cost 3D models.
The main disadvantage of this approach is the
difficulty in obtaining photo-realistic models.
Nonetheless, results from our content validation
experiments, facial expressions in our present models
are consistently interpreted by normative observers
and are decoded according to expectations derived
from emotion and expression science, which is
indirect evidence of realism. These gives us the
confidence to use the application to generate
animation clips to be used in the research domain of
non-verbal communication.
Tests performed with therapists further confirm
that the current models are more realistic than those
of the previous version. Speech articulation was seen
as a major improvement, and in general the idea of
using this tool in a clinical environment was
welcomed with enthusiasm.
The main follow up steps will be: i) to develop and
integrate in the application an artificial intelligence
module toward the simulation of emotions; ii)
afterwards, to validate the usefulness of the
application with a clinical population in a therapeutic
context.
ACKNOWLEDGMENTS
We acknowledge all the therapists and volunteers that
GRAPP2015-InternationalConferenceonComputerGraphicsTheoryandApplications
354

participated in our user study with no reward. We
thank our national funding agency for science,
technology and innovation (Fundação para a Ciência
e a Tecnologia- FCT) and the Research Unit LabMAg
for the financial support (through PEst-
OE/EEI/UI0434/2014) given to this work.
REFERENCES
APA- American Psychiatric Association, 2000. DSM-IV-
TR. American Psychiatric Publishing, Inc..
Beidel, D. C., Turner, S. M., 2007. Shy Children, Phobic
Adults: Nature and Treatment of Social Anxiety
Disorder. Washington, DC: APA, 2nd edition.
Bradley, M. M. and LANG, P. J., 1994. Measuring
Emotion: the Self-Assessment Manikin and the
Semantic Differential. J. Behav. Therap.. and Exp.
Psvchyatry, 25, 1, 49-59.
Cláudio, A.P., Carmo, M.B., Pinheiro, T., Esteves, F., 2013.
A Virtual Reality Solution to Handle Social Anxiety.
Int. J. of Creative Interfaces and Computer Graphics,
4(2):57-72.
Cláudio, A.P., Gaspar, A., Lopes, E., Carmo, M. B., 2014.
Virtual Characters with Affective Facial Behavior. In
Proc. GRAPP 2014, pp 348-355, SciTePress.
Douilliez, C. Yzerbyt, V., Gilboa-Schechtman, E.,
Philippot, P., 2012. Social anxiety biases the evaluation
of facial displays: Evidence from single face and multi-
facial stimuli. Cog and Emo, 26(6): 1107-1115.
Eibl-Eibesfeldt, I., 1989. Human Ethology. NY: Aldine de
Gruyter.
Ekman, P, Friesen, WV., Hager, J C., 2002. Facial action
coding system. Salt Lake City, UT: Research Nexus.
Gaspar, A., Esteves, F., 2012. Preschoolers faces in
spontaneous emotional contexts – how well do they
match adult facial expression prototypes? Int J Behav
Dev. 36(5), 348–357.
Gaspar, A., Esteves, F., Arriaga, P., 2014. On prototypical
facial expressions vs variation in facial behavior:
lessons learned on the “visibility” of emotions from
measuring facial actions in humans and apes. In M. Pina
and N. Gontier (Eds), The Evol. of Social Comm. in
poserPrimates: A Multidisciplinary Approach,
Interdisciplinary Evolution Research. New York:
Springer (pp.101-145).
Grillon, H., 2009. Simulating interactions with virtual
characters for the treatment of social phobia. Doctoral
dissertation, EPFL.
Haworth, M. B., Baljko, M., Faloutsos, P., 2012. PhoVR: a
virtual reality system to treat phobias. In Proceedings of
the 11th ACM SIGGRAPH International Conference
on Virtual-Reality Continuum and its Applications in
Industry, 171-174.
Herbelin, B., 2005. Virtual reality exposure therapy for
social phobia. Doctoral dissertation, EPFL.
James, L. K., et al., 2003. Social anxiety in virtual
environments: Results of a pilot study.
Cyberpsychology and behavior, 6(3), 237-243.
Klinger, E., et al., 2004. Virtual reality exposure in the
treatment of social phobia. Studies in health tech. and
informatics, 99, 91.
LaViola Jr, J. J., 2000. A discussion of cybersickness in
virtual environments. ACM SIGCHI Bulletin, 32(1),
47-56.
North, M. M., et al., 1998. Virtual reality therapy: an
effective treatment for the fear of public speaking. The
International Journal of Virtual Reality 3, 1-6.
Pertaub, D. P., Slater, M., Barker, C., 2001. An experiment
on fear of public speaking in virtual reality. Studies in
health tech. and informatics, 372-378.
Pertaub, D. P., Slater, M., Barker, C., 2002. An experiment
on public speaking anxiety in response to three different
types of virtual audience. Presence: Teleoperators and
Virtual Environments, 11(1), 68-78.
Russell, J. A., Fernandez-Dols, J. M., 1997. What does a
facial expression mean? In The psychology of facial
expression, pp. 3–30. New York, NY: Cambridge
University Press.
Slater, M., Pertaub, D. P., Steed, A., 1999. Public speaking
in virtual reality: Facing an audience of avatars. IEEE
CGandA, 19(2), 6-9.
Slater, M., et al., 2006. A virtual reprise of the Stanley
Milgram obedience experiments. PloS one, 1(1), e39.
Stein, M.B. and Kean, Y.M., 2000. Disability and Quality
of Life in Social Phobia: Epidemiologic Findings. Am
J Psychiatry 157: 1606–1613.
(last access to these sites on Dec 2014).
url-Blender http://www.blender.org/
url-Kinect http://www.microsoft.com/en-
us/kinectforwindows/
url-MakeHuman http://www.makehuman.org.
url-Poser http://my.smithmicro.com/poser-3d-animation-
software.html.
url-Unity http://Unity.com/
UsingExpressiveandTalkativeVirtualCharactersinSocialAnxietyDisorderTreatment
355
