
Standardization and Innovation for Smart e-Health Monitoring Devices
Albena Mihovska, Sofoklis A. Kyriazakos, Mihail Mihaylov and Ramjee Prasad
Center for TeleInfrastruktur (CTIF), Department of Electronic Systems, Aalborg University, FBV 7-C1, Aalborg, Denmark
Keywords: e-Health, ITU-T, Standardization, Requirements and Capabilities.
Abstract: The challenges faced by standardization in relation to the potential of wireless communication technologies
to deliver lower cost, higher efficiency, enhanced quality of experience and diversified smart e-Health
services, are multi-fold and determined by the complexity of the myriad of emerging user and usage
scenarios. In addition, there is the challenge of protection of privacy and the maintenance of trust. This
paper aims to show the evidence of the correlation between standardization and innovation in the area of e-
health technology. It describes a capability framework proposed for the delivery of e-Health services in
support of independent living. The proposed framework incorporates innovative research and standardized
solutions. The paper addresses the correlation between standardization and innovation, in particular for the
area of e-Health. It analyzes the potential of research to advance and harmonize the standardization efforts
towards sustainable e-Health solutions, and outlines some critical points for the future standardization work
in the related area.
1 INTRODUCTION
e-Health environments are extremely complex and
challenging to manage, as they are required to cope
with an assortment of patient conditions under
various circumstances with a number of resource
constraints. There is a large number of initiatives
(e.g., the EU European Innovation Partnership pilot
action on Active and Healthy Ageing –EIP AHA
and the EU Joint Programming on Ambient Assisted
Living), products and services that aim to provide a
robust strategy to face the challenge of designing
sustainable e-Health system solutions. The
Telecommunication Standardization Sector of the
International Telecommunication Union (ITU-T)
(ITU-T, n.d.) has recently recommended Y.2065
“Service and capability requirements for e-health
monitoring services” – a standards recommendation
document that classifies e-health monitoring services
(EHM) as EHM Healthcare, EHM Rehabilitation
and EHM Treatment services, and describes service
requirements according to the different roles
involved in the provisioning of these services (i.e.
EHM customer, EHM device provider, network
provider, platform provider and EHM application
provider) (Y.2065, (03/2014)). The EHM capability
requirements are defined with respect to the different
layers of the ITU-T GSI Internet of Things (IoT)
reference model specified in the ITU-T Y.2060
“Overview of the Internet of Things” (Y.2060,
(06/2012)) . According to ITU-T Y.2060, the IoT is
a global infrastructure for the information society,
enabling advanced services by interconnecting
(physical and virtual) things based on existing and
evolving interoperable information and
communication technologies. Within the ITU-T
concepts, a device in the context of IoT is a piece of
equipment with the mandatory capabilities of
communication and some optional capabilities of
sensing, actuation, data capture, data storage and
data processing. The devices collect various kinds of
information and provide it to the information and
communication networks for further processing.
This is also the most straightforward observation of
the correlation between standards and research
innovation.
While both devices and technologies carry equal
weight in the provision of IoT services in general,
and e-Health services, in particular, the devices used
in research projects are usually already standardized,
available on the market solutions. However, the
interconnection of devices into intelligently
communicating networks, which can be then an
inherent part of the infrastructure, requires novel
research. This in turn has the potential of enhancing
existing standards with new recommendations and
283
Mihovska A., A. Kyriazakos S., Mihaylov M. and Prasad R..
Standardization and Innovation for Smart e-Health Monitoring Devices.
DOI: 10.5220/0005318502830290
In Proceedings of the International Conference on Biomedical Electronics and Devices (SmartMedDev-2015), pages 283-290
ISBN: 978-989-758-071-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

architecture models (R. Prasad, 2013).
The European-funded under Framework Program
Seven (FP7) within Information Communication
Technology (ICT) project eWALL (eWall, 2013)
proposed an affordable, easy-to-implement smart,
“caring home” cognitive environment, that “senses”
intuitively the wishes and “learns” the needs of the
person that lives in this house, providing unobtrusive
daily support, notifying informal an formal
caregivers when necessary and serving as a bridge to
supportive services offered by the outside world. It
is a dynamic home environment that unobtrusively
monitors and interacts with its inhabitants while they
perform their activities of daily living (ADL), able to
recognize abnormal events as well as slowly
emerging shifts in behavior, and able to inform
associated users (caregivers, healthcare
professionals, family) appropriately to provide a
feeling of safety and comfort for all involved parties.
The key aspects of the project eWALL are
innovative research, evaluation and implementation
towards a short-and long-term exploitation impact.
This paper is further organized as follows. Section
II describes the eWALL user groups and scenarios
and derives the key requirements from a research
viewpoint to design a highly usable, efficient and
implementable e-Health service framework. The
main eWALL services to be provided are defined in
Section III. Section IV defines the required IoT
framework for the provision of the eWALL services.
Section V compares the derived services, devices
and capabilities to the ones defined within the ITU-T
recommendations and identifies commonalities and
gaps. Section VI concludes the paper.
2 EWALL USER GROUPS AND
SCENARIOS
2.1 Page Setup Main Requirements for
a Sustainable e-Health System
A successful e-Health system should be able to
maximize the potential societal impact of its use, and
thus, should be able to support a broad range of
target users. The general user groups will involve a
myriad of primary end users that can be categorized
according to their human health state, and a number
of secondary end users and third parties (e.g.,
technology providers). Smart home systems enable
constant monitoring and interpretation of health-
related parameters (e.g. ADL’s, medicine intake,
physiological parameters) in the primary user’s
everyday life, which give the informal caregivers
(i.e., a group of secondary users) the information
necessary to feel comfortable about the person they
care for, and need to rely less on professional
expertise, leading to reduction in visits to doctors.
For various chronic conditions, in which the use of
professional healthcare services is mandatory,
everyday monitoring and interpretation of the
patient’s relevant data can provide professional
caregivers (another secondary user group) with the
information vital to enable the focus of their efforts
on those patients who need it most. The key
requirements for enabling a sustainable e-Health
system, are the personalization and adaptation to
specific needs and preferences, the efficient data and
context sharing between the different required
services and artefacts, including the handling of
multiuser identification, auto configuration and
calibration systems. These requirements demand
high personalized usability and unobtrusive sensing.
eWALL incorporates a myriad of wireless and
wired communication and data processing
technologies and networked devices that interoperate
in the frames of the eWALL platform to provide e-
Health services.
Information is collected by means of sensing
devices and forwarded further by residential
gateways. To improve the interoperability between
sensors and residential gateways device type specific
standards developed by the Continua Health
Alliance can be used. Current solutions lack
interoperability and therefore impede the
establishment of a remote patient monitoring
solution market. The ISO/IEEE Standards 11073
standardizes the transfer of medical information and
can be used to achieve the above described aim (M.
Benner, June 2011). This is also a styandard used in
eWALL, which can then be enhanced further by the
research performed. Usage of Continua Certified™
products allows for enabling data interoperability,
which processing can be challenged by the wide
range of sensors from different vendors and
standards.
The Smart Open Services for European Patients
(epSOS) (epSOS, 2008-2014) is very useful to
enable cross-border interoperability and secure
access between electronic health record systems.
Secure transfer of personal medical data is key to
avoiding critical medical errors, and therefore, is a
key requirement for enabling a sustainable e-health
solution. The role of standards should also extend to
cover the critical aspects of privacy and trust. The
integration of the eWALL functionalities with
epSOS is achieved in such a way that the developed
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
284

modules can enhance the existing epSOS platform in
return. The proposed integration is vital to
strengthen the exploitation impact on a large scale of
the eWALL solution.
The patient must give her/his consent before any
of her/his data is made available. The health
professional’s permission to access the patient’s
medical data must be verified according to the
national security policy of the specific country the
patient originates from, and, if available, through a
patient privacy policy. This puts a strong emphasis
on the need to involve besides standardization
experts, also regulatory ones that would be able to
define suitable policies for a more unified
framework approach that, however, maintains the
specific to a country regulations.
2.2 First Section eWALL User Groups
In eWALL, for facilitating research and evaluation,
the human health is seen in one of two possible
states: (1) healthy (i.e., elderly users with age related
impairments-ARI), and (2) sub-healthy (i.e., users
diagnosed with Chronic Obstructive Pulmonary
Disease-COPD or suffering from mild cognitive
impairments, such as short term memory, language,
execution of complex or parallel tasks). Both groups
are considered as primary users. Both primary user
groups would need to interact to a certain extent
with two different types of secondary user groups,
namely:
1) Professional Caregivers: including nurses,
home care support professionals, medical doctors
(general practitioners, lung physicians);
2) Informal Caregivers: this user category
contains the primary user’s family, neighbors,
friends and anyone else not from the professional
healthcare field that provides any type of support,
including social support, housekeeping, or more
disease specific support.
In order to define a set of functional requirements
that align with the targeted end-user groups, typical
human-centered design approaches for e-Health
technology, such as ISO 9241-210 (British
Standardization Organization, 2010) or user-
centered design (Usability Professionals
Association, 2013) were applied to enable that the
prospective primary end user is the focal point
during the design of the capability framework. The
four following products are developed in order to
inform the design: user profiles, personas, scenarios,
and use cases. It should be mentioned, that eWALL
is suitable for application to primary users in four
possible human health states as defined by (Y.2065,
(03/2014)) but for this purpose the set of eWALL
services must be redefined accordingly.
2.3 Usage Scenarios
The eWALL usage scenarios are defined from the
point of view of the primary and the secondary users
with the purpose to create a common view on the
services needed. The eWall system is described as a
series of functionalities, for each persona. Each one
of these functionalities could correspond to a module
of the eWall system. Modules should be loosely
coupled and as less codependent as possible.
Communication between modules is done via
middleware and data and knowledge repositories. A
module output will be transformed into knowledge
that will form the user profile. The user profile
describes in depth the profile of the person for which
the eWall home installation is being used, from a
therapeutic perspective. Based on the scenarios a
number of application categories were defined as
shown in Table I.
Each of the application categories in Table I
contains several possible applications, which have to
be prioritized and defined in further detail. Many
applications may interact with other applications in
various ways.
Table 1: Application Categories for eWALL.
# Application Category
1 physical exercise
2 daily activity monitoring
3 daily functioning monitoring
4 nutritional coach
5 safety
6 medication support
7 social integration
8 healthcare support
9 calendar
10 cognitive stimulation
11 domotics
12 outdoor guidance
13 health monitoring
3 eWALL SERVICES
eWALL has the purpose to support ADL for the
described primary end user groups for an improved
quality of life and overall cost-efficiency. ADL can
be divided into basic ADLs and instrumental ADLs.
StandardizationandInnovationforSmarte-HealthMonitoringDevices
285
1) Basic ADLs.
The basic activities of daily living consist of
various self-care tasks: bathing, dressing and
undressing, eating, transferring from bed to chair,
and back; voluntarily control of toilet use; walking
(not bedridden).
2) Instrumental ADLs.
Instrumental activities of daily living are not
necessary for fundamental functioning, but enable
the individual to live independently within a
community, e.g., light housework, preparing meals;
taking medications; shopping for groceries or
clothes; using the telephone; managing money.
The eWALL services are grouped into the
following categories: a) risk management and home
safety; b) eHealth and c) lifestyle management.
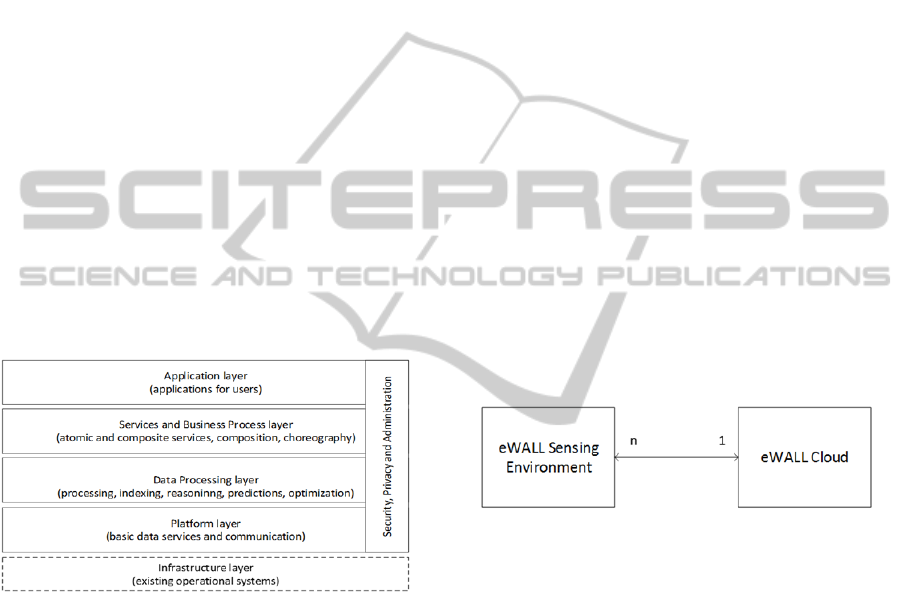
The eWALL services are delivered by the
eWALL cloud, and are classified as horizontal and
vertical services, given in Fig 1. The horizontal
services consist of service bricks that enable the
definition of a process, the personalization and
adaptation of a vertical service. The vertical services
are those developed for the eWALL system, either
by the medical service providers, or by the
developers.
Figure 1: eWALL capabilities implemented in a layer
structure.
The layered structure in Fig. 1 follows the
recommendations for the basic IoT capabilities as
defined in (Y.2060, 2012). eWALL has a set of
logical tiers (e.g., user services, business services,
data) to define how the system will interface with
the environment. A tier is a logical partitioning of a
system where each tier has a unique responsibility.
The difference between tier and a layer is that the
tier may represent a physical distribution of the
components and the functionality on separate
servers, computers, networks or remote locations.
Thus, tiers may imply physical separations. The
eWALL multi-tier architecture is described in more
detail in (eWall, 2013), (A. Mihovska, Oct.2014).
In-house metadata are not enough to support the
lifestyle of the eWALL primary users. Therefore, the
eWALL services are defined also by the data filtered
from various social networks and linked data
repositories in order to understand possible user
activities and rank them for high degree of
personalization.
The activities and situations the user is found in,
are used to extract habits, allowing eWALL to
anticipate the user’s actions.
Personalized services and applications about risk
management, e-health, e-care and lifestyle
management are offered via web support based on
the understanding of eWALL on the current and
expected situation, as well as the available activity
opportunities. Such services include personalized
recommendations, unobtrusive reminders and
alarms.
4 CAPABILITIES FRAMEWORK
AND REQUIREMENTS
The eWALL system is composed of two main
subsystems: the eWALL Sensing Environment and
the eWALL Cloud. The interaction between the two
is shown in Fig. 2.
Figure 2: eWALL main subsystems.
The eWALL Sensing Environment is envisioned
as a logical environment, deployed over a physical
space, which is mainly responsible for the explicit
and implicit interaction with the primary user.
“Implicit interaction” refers to the collection of
various data about the user and the user environment
from medical and environmental sensors and the
control of the environment through actuators.
“Explicit interaction” refers to the direct interaction
of the user when using audio/video devices and user
interaction sensors.
Two types of the eWALL Sensing Environment
are envisioned, namely:
1) Stationary or a Home Sensing Environment (HSE)
It is related to the physical surrounding of the user
when at home. Home sensing devices monitor the
status of vital environmental parameters in the
home, such as humidity, temperature, luminosity,
motion etc.
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
286

The Audio/Visual (A/V) Sensing provides full-
body 3D motion capture, face and voice recognition
capabilities build over C/C++ processing algorithms.
The A/V based emotion recognition system is a
considerably challenging field to generate an
intelligent system that is able to identify and
understand human emotions for various vital
purposes, e.g. security, society, entertainment, health
care, human-computer interaction, industrial and
personal robotics, surveillance and transportation.
The visual sensing is enabled by the infrared (IR)
depth-sensing technology and monochrome
complementary metal oxide semiconductor (CMOS)
camera of the Microsoft XBOX Kinect sensor. The
sensor outputs video at a frame rate of 30 Hz, while
the RGB video stream uses 8 bit VGA (Video
Graphics Array) resolution (640 x 480 pixels) and 8-
bit for each channel, whereas the depth stream is 640
× 480resolution and with 11-bit depth.
The speaker diarisatrion component is designed
to monitor and log the number of people verbally
interacting in the living room of the caring home.
The component uses one or several audio streams to
estimate the number of different speakers in the
room.
2) Mobile Sensing Environment (MSE)
It is centralized around the user mobile devices
when the user is outside of the home environment.
User vitals tracking concerns the person physical
activity as a function of time. The integral of the
modulus of body acceleration (IMA) values are a
reliable indication of activity, but can also be used to
classify different events or activities, like falls,
walking, running, housework, etc. Other wearable
sensors measure body information as they are
carried by the user and transfer their signals to the
gateway wirelessly. Such devices could be
smartphones, smartphones, pulse and SPO2 sensors,
the smart stethoscope, body temperature and so on.
The interoperability of all sensing devices is of
major importance for the integration and acceptance
of the proposed system. Most devices are from
different manufacturers and the goal of
standardization is to enable large-scale deployment
of telecare and telehealth services at reduced costs.
In order to fulfil the requirements for
standardization, the telehealth devices should meet
criteria for data exchange, data representation,
terminology for communication between them and
the device gateway (e.g. cell phones, personal
computers, health appliances).
In the process of device prototyping, eWall uses
Arduino and Libelium based sensing environment
testbeds, The Aruino uses Atmel ATmega 328P
microcontroller that works at 16 MHz clock and the
maximum size of the uploaded program - 32 kB.
Arduino Wireless Shield allows your Arduino board
to communicate wirelessly using ZigBee where in
eWall the XBee XB24-Z7WIT-004 module from
Digi (Digi, n.d.). Series 2 allows for a set up of
complex mesh networks based on the XBee ZB
ZigBee mesh firmware. The Libelium sensor nodes
and sensor gateway are equipped with XBee 868
PRO S5 radio modules (Digi, n.d.) which use one
single communication channel at a frequency of
869.4 – 869.65MHz (0.25 MHz bandwidth).
The data coming from the sensors is received by
the device gateway, processed with C/C++
algorithms and stored in CouchDB database hosted
on the “HomePC”. This format is in resource
description framework (RDF) triplets and the
description of the metadata is in JavaScript Object
Notation (JSON) format.
3) eWall Cloud
The eWALL Cloud is the central processing and
data storage subsystem. The eWALL applications
are based on “service bricks” that are available in a
“pool of services” in the eWALL cloud.
The eWALL cloud is connected to the home of
each primary user. The “service bricks” in the
eWALL cloud are in fact the various services
exposed by the devices. The “service bricks” are in
between the applications and the metadata stored in
the cloud Data Management Block, and act as
providers of specific aggregated data, after making
some reasoningon of the metadata. The applications
get such aggregated data from the “service bricks”
via JSON/REST over HTTP communication proto-
col.
The semantically-rich metadata obtained from
the sensing and monitoring devices and the data
from the cloud middleware services are fused to
extract higher-level context of the eWALL services.
The perceived in-house situation is fused with the
cloud metadata, allowing for the understanding of
the user’s reaction to recommendations and their
adaptation to the personal taste of the user. Such an
approach results in semantically rich and high level
context information that serves as input for the
eWALL intelligent decision support (IDSS) system.
Fig. 3 shows example of high level models in the
IDSS. eWALL implements the IEEE Suggested
Upper Merged Ontology (SUMO) concepts and
defines a set of specific sub-ontologies based on the it.
StandardizationandInnovationforSmarte-HealthMonitoringDevices
287
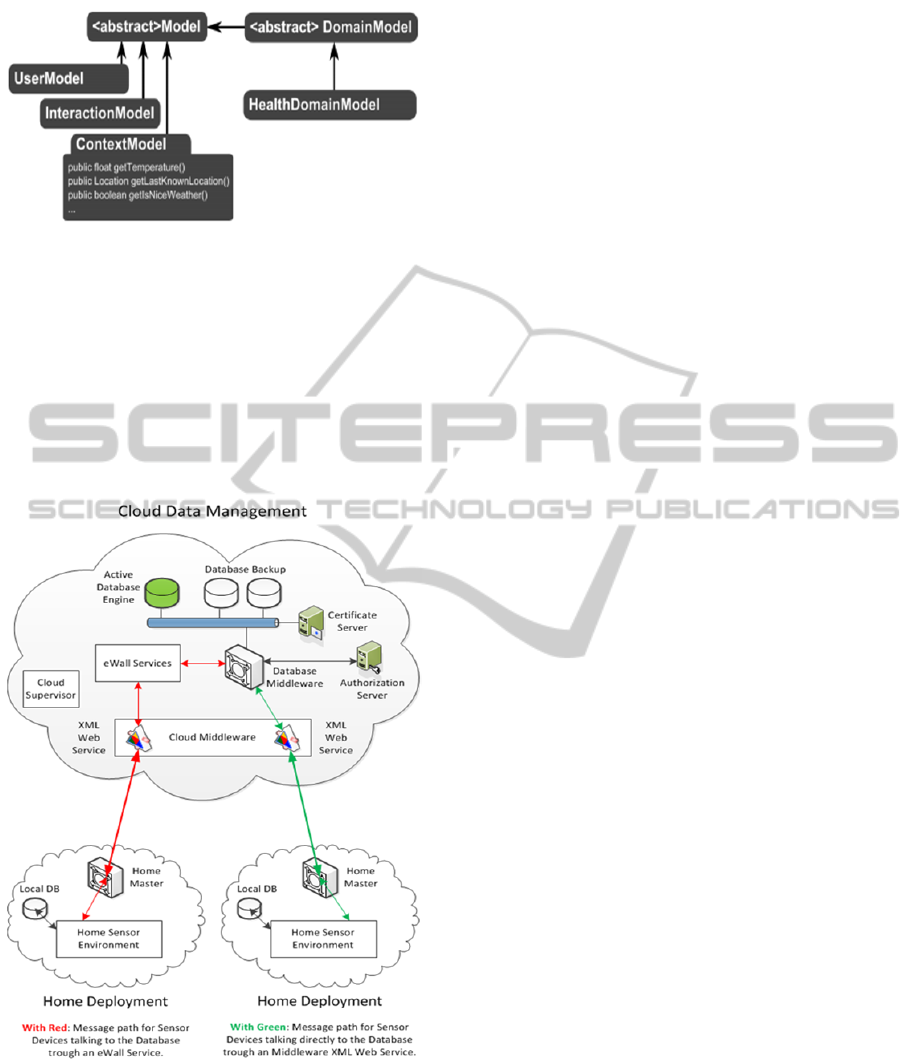
Figure 3: High level overview of the models used in the
IDSS Core.
Sensors/devices from the home environment
exchange information with the cloud storage via the
eWall service. In the cloud, there is a peer
application that has its own processing logic, adding
value to the communication beyond simple data
access. As an example, these could be applications
that need to take decisions based on data mining and
command sensors based on user behavioral patterns.
Figure 4: Data management approach for eWALL
supported.
Another highly innovative aspect is the
integration of radio frequency wireless technologies
with visible light communications (VLC) (e.g.,
related to IEEE 802.15.7 standardization) for the
provision of to support very dense low and high data
rate smart service connectivity (A. Kumar, 2014).
VLC will be investigated in the scope of the eWALL
scenarios and services. These are aspects that require
an integrated research and standardization effort in
order to impact the overall e-Health services and
products commercialization.
5 ANALYSIS OF e-HEALTH
RESEARCH WITH RESPECT
TO USE OF STANDARDS
RECOMMENDATIONS
In order to deliver a novel system for personalized
and context-aware services that can support the
active ageing, there is a clear need for a balanced co-
existence of innovative research and development
from a medical and technological perspective, on
one hand as well as compliance with existing
standards, to address advanced networking
paradigms, such as cloud connectivity, innovative-,
simple- and efficient-communication protocols,
patient mode surveillance and the development of
advanced application and services. Table II shows
the main requirements by which a sustainable e-
Health system solution should be evaluated and, by
which, also standardized solutions should be
aligned.
eWALL contributes greatly to the further
refinement of standards recommendations by
incorporating along with the research activities,
strong evaluation strategies, involving real-user
trials. Information obtained from such trials, will be
mapped to standards requirements for further
improvement on usability and user friendliness,
which can strengthen the position of standardization
as a transfer channel for further innovations.
eWALL involves all relevant end-user groups in
the research and development process by the
evaluation with real-field trials and thus is able to
provide a rich set of intelligent services, deployed in
realistic conditions that should be compliant with the
minimum set of privacy and ethical requirements.
Privacy-by-design is a key aspect to be incorporated
into standardization activities, and has the potential
to further impact already established e-Health
service recommendations such as defined in
(Y.2065, (03/2014)). Examples of such services are
the personal health monitoring, home safety, mobile
services, care and rehabilitation management
services.
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
288

Table 2: Critical Characteristics for the Evaluation of
e-Health Solutions and Standards.
Critical
characteristics
Description Type of evaluation
Interopera-
bility
Ability of the difference devices
and services to cooperate
seamlessly and provide a
seamless user experience.
System validation
and verification.
Extensive testing
for facilitating the
interoperation of the
devices and services.
Easy
personalization
Ability of the end user to adjust
the system and its building
blocks to needs without any
special ICT knowledge. Implicit
and intelligent adaptation to the
user profile and context.
Questionnaires;
observations;
interviews; process
analysis
Mobility
Ability of the user to be mobile
while receiving
e-Health services regardless of
location.
Observations;
interviews,
questionnaires,
technical validation.
Cost-
efficiency/
energy
management
Direct: consultation hour,
transfer of personnel.
Indirect: lost working hours per
clients Capital cost: equipment
(purchase, reforms). Support in
reducing the energy
consumption of the house.
System validation
and verification
based on
measurable units
for energy
consumption and
techno-economic
analysis. Statistical
Analysis
Low
Maintenance
Ability of the system to work
for hours without the need of
performing maintenance
actions. Self-healing
mechanisms.
Observations,
technical validation
and statistical
analysis.
Safety/
security
Level of acceptability of the
health risk (e.g., due to
complications or adverse effect)
associated with using a
technology. A function of the
caregiver’s judgment (in
deciding whether to use the
supporting technology for a
particular case).
Preserving confidentiality, data
integrity, strong authentication
and authorization mechanisms.
Technical
validation. Risk
assessment.
Observations;
interviews,
questionnaires
High reliability Fault tolerance
System validation
and verification.
Monitoring &
Measuring
Accessibility
Accessibility to the e-Health
services from everywhere. User
friendly interfaces, also
addressing patients with chronic
physical and cognitive
impairments.
System validation
and verification.
Questionnaires;
observations;
interviews
Satisfaction
Client: perception of physical
improvement, perceived
homecare, satisfaction level,
self-care at home. Perception
for self-care; perception of
social inclusion, avoidance of
new or re-occurring incidents.
Questionnaires;
observations;
interviews.
Technical
properties
Technical aspects, required
infrastructure, hardware,
software, conformance to
standards.
Tests, reviews,
guidelines,evaluatio
n reports.
Realistic
Definition of real-world
condition for the e-Health
system. Involvement of real
users
Involvement of
relevant end users
In addition to the identified state of the art of
legal science and data protection policy together
with the security and privacy problems in the
context of eWALL, the project also will define a
“Privacy-by-Design” methodology that would
encompass technical, economic and social aspects of
critical relevance to e-Health systems. Currently,
these activities are closely performed with the
European Telecommunication Standardization
Institute (ETSI)
The approach should relieve caregivers and other
users of any additional bureaucratic legal procedures
that the technology deployment may imply.
Standardization can help research by defining
target methodologies and requirements that in turn
can help scientists and technology producers, both,
to develop privacy protecting technical concepts.
6 CONCLUSION
This paper addressed the use of standardized e-
Health solutions in innovative research projects.
Although, that there is a broad agreement that
innovation is a key to economic prosperity, yet for
many researchers, companies and organizations, the
coupling of standardization and innovation is a
rather novel idea.
e-Health as an area of huge economic
significance and impact, needs standardization to
cope with the complexity of the usage and user
scenarios to be supported by the e-Health
technological solutions. This paper described and
analyzed the use of both standardized and innovative
research solutions for the design of highly
personalized e-Health services in support of
independent living and compensating for prevailing
age- or disease-related physical and cognitive
impairments. It was shown that sustainable e-Health
solutions must adopt standardized solutions in an
integrated approach with research and development
activities.
Innovative technical concepts for e-Health
systems must account for certain privacy and trust
goals. Standardization must account for certain basic
privacy and trust requirements, and work should be
performed jointly with regulatory experts. The
challenge is in how to harmonize a variety of e-
Health related policies adopted by various countries
and regions.
The core e-Health platform functionalities and the
embedded intelligence within strongly depend on the
actual sensing devices used. Industry accepted
definitions generally distinguish between a smart
StandardizationandInnovationforSmarte-HealthMonitoringDevices
289

and an intelligent sensor. Such definitions and their
application into innovative solutions are highly
dependent on the outcome of the standardization
effort.
ACKNOWLEDGEMENTS
This paper is partially based on the joint research
work of the EU-funded under FP7 project eWALL.
If any, should be placed before the references
section without numbering.
REFERENCES
A. Kumar, A. M. S. K. R. P., 2014. Visible Light Commu-
nications (VLC) for Ambient Assisted Living.[Online]
Available at: http://link.springer.com/article/11277/
WIRE-Article 1901.[Accessed Oct/2014]
A. Mihovska, S. K. R. P., Oct.2014. eWall for Active Long
Living: Assistive ICT Services for Chronically Ill and
Elderly Citizens. San Diego, California, USA., IEEE
SMC.
Digi, n.d. [Online] Available at: ttp://www.digi.com
[Accessed Oct 2014].
epSOS, 2008-2014. epSOS Project. [Online] Available at:
http://www.epsos.eu/[Accessed Oct 2014].
ETSI, n.d. European Telecommunication Standardization
Institute-ETSI. [Online] Available at: http://etsi.org.
[Accessed 2014 Oct].
eWall, 2013. EU FP7 ICT Project eWALL, “eWall for
Active Long Living,”. [Online]
Available at: http://ewallproject.eu/[Accessed Nov
2014].
ITU-T, n.d. International Telecommunication Union.
[Online] Available at: http://www.itu.int/pub/T-REC.
[Accessed Oct 2014].
M. Benner, L. S., June 2011. Using Continua Health
Alliance Standard: Implementation and Experiences of
IEEE 11073. Luleå, Sweden., IEEE.
R. Prasad, A. M., 2013. “Challenges to 5G Standar-
dization,”.[Online] Available at: https://itunews.itu.
int/En/4619-Challenges-to-5G-standardization.note.as
px.[Accessed Oct 2014].
Y.2060, (06/2012). Series Y: Global Information
Infrastructure, Internet Protocol Aspects, and Next
generation Networks-Frameworks and functional
architecture models; Overview of the Internet of
things. [Online] Available at: http://www.itu.int/rec/T-
REC-Y.2060-201206-I/en.
[Accessed Nov 2014].
Y.2065, (03/2014). Series Y: Global Information
Infrastructure, Internet Protocol Aspects, and Next
generation Networks-Frameworks and functional
architecture models; Service and capability
requirements for e-health monitoring services.
[Online] Available at: http://www.itu.int/rec/T-REC-
Y.2065-201403-I/en[Accessed Oct 2014].
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
290
