
A Mobile Guardian Angel Supporting Urban Mobility for People
with Dementia
An Errorless Learning based Approach
Laura Freina and Ilaria
Caponetto
CNR-ITD, via de Marini 6, 16149, Genova, Italy
Keywords: Mild Dementia, Cloud Computing, Geolocation Systems, Errorless Learning.
Abstract: Dementia is one of the main causes of dependency for old people in the world, and, according to several
studies, the number of people affected by such a problem is bound to grow significantly in future. This
represents a high social cost. Memory loss and disorientation to space and time are among the most
common problems in the early stages of dementia, causing worry in caregivers and consequently social
isolation for the people involved. A mobile system in support of the autonomous mobility around town
would offer a double advantage: allowing for more independence of the dementia affected people and
reassuring caregivers. In this paper, we discuss the possibility of adapting an existing mobile system,
developed for intellectually impaired young adults, to these specific target users. We identify in the errorless
learning approach a possible method to support the learning of a new, technologically based system
accessible to people with mild dementia, highlighting some potential issues that still need further
investigation, in particular learning transfer and spontaneous use.
1 INTRODUCTION
According to several studies, the number of people
in the world that have some sort of dementia is very
large and will probably increase in the next years.
Among the early symptom of dementia, the most
frequently reported ones are loss of memory and
disorientation to space and time. Therefore, people
who have dementia in its early stages start having
difficulty in finding their way, they wander with no
apparent destination, they feel lost and sometimes
actually lose their way.
Wandering and getting lost is one of the main
concerns of families and caregivers. They have a lot
of pressure and responsibilities, and often end up
limiting the person’s access to outdoors. Moreover,
people with dementia themselves are aware of the
issue and often feel insecure with the fact that they
may not know where they are and what time of the
day it is, therefore they limit themselves or accept
the imposed limitations. Locked doors cause social
exclusion and reduce the person’s interests and
activities, also causing the illness to get worse in a
shorter time.
Having a system in support of the personal
independence of people with mild dementia, by
allowing and aiding their free movements around
town would give them more freedom and the
possibility to lead a more active life for a longer
time. At the same time, such a system would offer
families and caregivers a tool to keep in touch with
their cared ones and always know where they are.
People with dementia would find a support to tell
them the time, guide them home, offer the
possibility to get in touch with a friendly voice and
ask for help when needed with a simple press of a
button.
In this paper, after introducing the most common
problems that characterize the early stages of
dementia, we discuss how a platform supporting
urban mobility could be adapted to maintain, as long
as possible, the mobility of these new target users.
Issues related to learning and being able to use the
new technology from people with mild dementia are
discussed, along with a feasible methodological
approach to address them.
2 SETTING THE SCENE
Dementia is not a specific disease, but rather an
overall term that describes a wide range of
307
Freina L. and Caponetto I..
A Mobile Guardian Angel Supporting Urban Mobility for People with Dementia - An Errorless Learning based Approach.
DOI: 10.5220/0005502503070312
In Proceedings of the 1st International Conference on Information and Communication Technologies for Ageing Well and e-Health (SocialICT-2015),
pages 307-312
ISBN: 978-989-758-102-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

symptoms associated with a decline in memory,
thinking and social abilities. In order to be classified
as dementia, the decline has to be severe enough to
reduce a person's ability to perform everyday
activities (Committee for Medicinal Products for
Human Use, 2008).
Although dementia mainly affects older people,
it is not a normal part of ageing, but rather the
consequence of some disease of the brain that
influences its functionalities. Alzheimer's disease
accounts for 60 to 70 percent of cases, vascular
dementia, which occurs after a stroke, is the second
most common dementia type, together they account
for about 90% of the cases.
Dementia is one of the major causes of disability
and dependency among older people worldwide:
according to the World Health Organization (WHO)
(World Health Organization, 2012), in 2012 35.6
million people had dementia. The total number of
people with dementia was projected to almost
double every 20 years, which means 65.7 million in
2030 and 115.4 million in 2050. About 150.000 new
cases per year have been estimated in Italy only (Di
Carlo et al., 2002).
Dementia has significant social and economic
implications in terms of direct medical and social
costs as well as the costs of informal care. The WHO
estimated that in 2010, the total global societal costs
of dementia was around 1.0% of the worldwide
gross domestic product or 0.6% if only direct costs
are considered.
Furthermore, dementia is devastating for the
families of affected people and for their caregivers.
Physical, emotional and economic pressures can
cause great stress to families and caregivers, and
support is required from the health, social, financial
and legal systems.
Within this frame, loss of memory and
orientation to space and time is a key issue in the
early stages of dementia. When the illness is still in
its mild or moderate stages, the person with
dementia would still be capable of moving around
town and leading an active life. Nevertheless, people
with dementia report difficulties in living with the
insecurity that you do not know where you are and
what time it of the day it is (Harris, 2006).
Unfortunately, the person’s freedom is often
drastically reduced, when not completely stopped,
by caregivers, who do not feel at ease when letting
their assisted ones free to move alone. People with
dementia are frequently denied the basic rights and
freedoms available to others, the limited or restricted
access to outdoors also causes them to be socially
isolated. These issues could be alleviated with the
use of technology (Topo, 2008), which can be
helpful in providing specific support and therefore
allowing more freedom for the person with dementia
to move around town in an autonomous manner.
Giving people with mild dementia a system that
can offer them a guide and help, which is always
present but not invasive, means giving them the
chance of being socially active for a longer time,
keeping up their interests and, therefore, slowing
down the progression of the illness. Furthermore, the
system would increase safety of the person and offer
support and reassurance to caregivers.
3 TOWARDS INNOVATIVE AIDS
In a previously developed project, “Smart Angel”, a
cloud based mobile system has been developed with
the aim of supporting urban mobility of people with
intellectual disabilities, in particular young adults
with the Down syndrome. Our position is that the
system, after being specifically adapted to the
different target population, could be effective also in
supporting and enhancing the orientation abilities of
people with mild dementia.
3.1 The Smart Angel Project
Smart Angel (Smart Angel, 2014), an Italian
regional project co-funded by the Liguria Region,
aims at favouring social inclusion of people with
intellectual disabilities by offering them accessible
tools supporting their daily activities and urban
mobility. The name “Smart Angel” wants to recall a
guardian angel, always at the person’s side,
providing help when needed in a non-invasive
manner.
Supporting the urban mobility of intellectually
impaired people is a key issue to promote and
enhance their full autonomy. Thus, one of the main
aims of the Smart Angel project was to enable them
to move around in the urban context and reach
relevant places (workplace, leisure, sports, home) by
themselves. This was done by relying on last-
generation existing technologies.
The project has been organized in a first training
phase in which the users’ orientation and mobility
skills are stimulated and trained by means of ad hoc
developed Serious Games, which make use of
innovative virtual reality devices (Freina, Busi,
Canessa, Caponetto, and Ott, 2014) (Freina and Ott,
2014). After this phase, the users start to move
around in their town and to get confident with places
and public transports. At the beginning, they are
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
308
closely supported and monitored by their educators.
As the user’s skills grow, the links with the
educators get looser until they are allowed to move
around in complete autonomy (at least along the
established paths) by relying only on the help of
mobile devices. Actually, this phase makes in-depth
use of both cloud and mobile technologies (Costa,
Freina, and Ott, 2015).
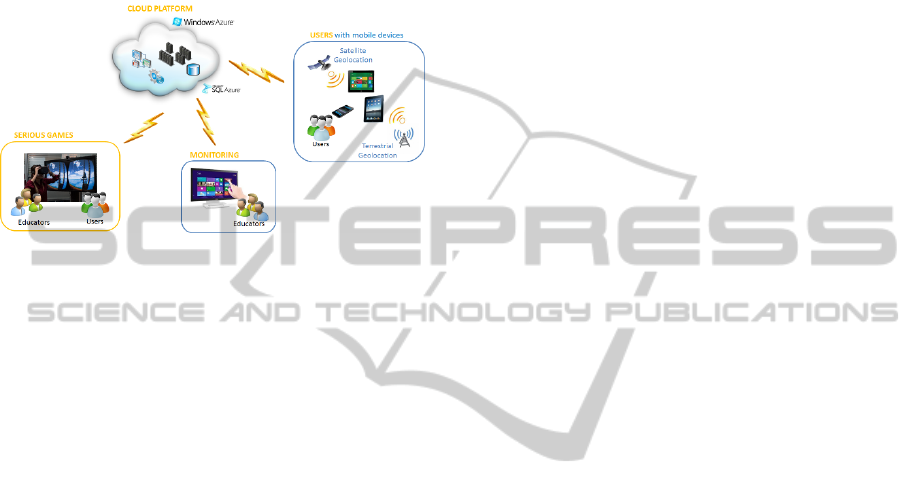
Figure 1: The Smart Angel System.
A central cloud based platform collects all the
users’ data and connects the other elements of the
system. Each user has his own smartphone, equipped
with specific apps, which allows him both to get
appropriate support during daily standard activities
and to move safely around town. A combination of
satellite and ground localization systems is involved
in tracing the users’ movement.
3.2 Adaptation of Smart Angel to the
New Target Population
The Smart Angel system has been developed for a
target population of intellectually impaired young
adults who have the abilities, either potential or real,
to move in town autonomously. Therefore, attention
has been focused on the development of basic
abilities and specific support to mobility. The typical
Smart Angel user is born in the digital era and is
acquainted with technology; they usually have their
own Smart Phone, which they used before entering
the project and learning a new app is considered a
fun activity.
People with dementia, on the other hand, are
usually aged and often have very little know-how
with respect to the new technologies. Furthermore,
they do not need to learn new abilities for moving
around, but rather to maintain already known skills
as long as possible. The basic functionalities needed
to support free mobility are the same, but the user
interfaces, as well as the initial intervention needed
to get the user acquainted with the new technologies
differ deeply.
It has been demonstrated that old people with
mild dementia symptoms can benefit from the use of
user-friendly technologies, even though they need
ongoing education and support (Hanson et al.,
2007).
4 AN INSIGHT INTO A POSSIBLE
METHODOLOGY
As reported in literature, the use of technologies,
both new and known ones, is possible for people
with dementia in its mild stages (Robinson, Brittain,
Lindsay, Jackson, and Olivier, 2009).
Robinson et al. report the development of a
technological system to support the independence of
people with dementia. Interestingly, the final users
have been closely involved in the definition of the
system to be tested, and the key issues to be
addressed were related to concerns about getting
lost, loss of confidence, which caused to the
reduction of daily activities and caregivers’ anxiety.
The use of some tracking technology and the
constant possibility to get in touch with one another
was considered as a good opportunity for caregivers
to give virtual support and give the person with
dementia more freedom.
Personalized solutions have been developed to
address some important drawbacks: the size of the
devices (the commercial ones were either too heavy
and awkward to carry or too small and difficult to
handle) and the fact that people with dementia may
have weak vision, making the use of the commercial
devices even more difficult. Today, these issues can
be easily solved thanks to the new technologies,
which, on the one hand offer tools that are small and
light, while, on the other hand, thanks to special
interfaces, can easily overcome the limitations due
to sight impairments.
Robinson et al. focus also on the reported
concern about social stigmatization: people
participating in the project wanted a system to
guarantee them a two-way communication and guide
them home that had to be flexible and discreet. This
issue is now automatically solved since the use of
smart mobile phones, equipped with navigation
systems and vocal interfaces has become widely
spread. Nobody would regard as strange speaking on
the phone, using a GPS navigation system or
interrogating a smart phone while walking around
town.
The reported experiments focused well on user
requirements, design and prototyping, but did not
AMobileGuardianAngelSupportingUrbanMobilityforPeoplewithDementia-AnErrorlessLearningbasedApproach
309

investigate on the solutions being actually used and
being effective. It would be of great interest to
explore which could be a possible methodology to
teach the target population the use of the new
technological tools in such a way that these tools
would actually be used effectively in real life. It
appears that the errorless learning approach could be
the answer to this issue.
4.1 Errorless Learning
The concept of errorless learning has been
introduced by Terrace (Terrace, 1963) who used it to
train pigeons in discriminating red and green lights.
In the errorless approach, the aim is that of
significantly reducing the error rate. People learn by
performing the same operation repeatedly, just like
the trial and error approach, but in this case, specific
attention is put on minimizing the number of errors.
Learning through trial and error requires the
learner to recognize when and where the error
occurred in order to resolve it. The explicit memory
is responsible for the recognition and correction of
the errors; this requires good skills of analysis,
which may be compromised in people with
dementia. If the error is not recognized as such, it
could be encoded into memory, which would result
in wrong responses later or conflicts between the
correct and the erroneous information. The errorless
approach, based on avoiding errors as much as
possible, minimizes this problem (Clare et al., 2000).
Different methods can be employed to minimize
errors during the learning phases, depending also on
the type of skill that has to be learned. For non-
procedural knowledge, spaced retrieval (in which the
information is rehearsed repeatedly with increasing
intervals between rehearsals) and vanishing cues (in
which the amount of cues given is enough to be
successful and is then reduced, keeping it always at
the minimum number required for success) are the
most used techniques. A stepwise approach is
suggested for the procedural knowledge.
4.2 Errorless Learning and Dementia
According to de Werd (de Werd, Boelen, Olde
Rikkert, and Kessels, 2013), people with dementia
still have the ability to acquire meaningful skills. In
particular, he reports the errorless approach to
learning as being more effective than other
approaches in teaching adults with dementia. He
presents various works based on the errorless
approach, reporting positive and long lasting effects
in learning the use of technological devices from
people with dementia: gains are generally
maintained at follow-up. In most cases novel tasks
were learned, in other cases familiar but forgotten
tasks or information were relearned.
People with dementia usually need a continuous
support in order to maintain their existing skills:
reinforcement may be frequently needed. Therefore,
caregivers would have to be involved in the learning
process. Even if attention has to be paid in order not
to overload them with responsibilities, they are
fundamental to train and maintain the newly learned
skills in the home environment.
In our case, we affirm that an errorless approach
could be used to teach people with mild dementia
how to use these new tools in order to have the best
possible support in their movements around town.
Such training has to be specifically studied keeping
in mind the distinctive problems of the target
population involved in the project, personalizing
each training path to individual needs in order to
stimulate and maintain, as much as possible, all the
skills and knowledge that are still available to the
user.
Furthermore, Nygård and Starkhammar (Nygård
and Starkhammar, 2007) report that sometimes
technology offers people with dementia a feeling of
safety that actually proves to be false. For example,
they may feel safe because they are carrying a
mobile phone and they are aware that they have the
possibility to ask for help if needed, but they have
actually never used the phone and may not be able to
do so. In our case, this phenomenon will also be
analysed. Even if the person may not be able to use
the tool in a real emergency, the increase in his
personal confidence resulting from the availability
of the system may lead to a better quality of life.
Moreover, caregivers would have the possibility to
trace the person at any moment, relieving their level
of anxiety.
4.3 Issues for Further Investigation
Even though the errorless learning approach,
enriched with specific training sessions tailored to
individual needs seems to be a feasible way to get
the most out of our system, some main issues are
still open and require further investigation. In
particular, we can foresee three critical issues:
physical management of the smart phone, transfer of
the learned skills to new situations and spontaneous
use of the tools when actually needed.
As far as the management of the smart phone is
concerned, the users need to learn some procedural
knowledge: sequences of actions to be performed at
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
310

certain times to guarantee its usability. In particular,
they have to remember to charge the smart phone
and to take it with them when leaving the house,
after checking that it is switched on. This issue can
be addressed by specific and fixed routines: in the
sequence of actions, the previous one triggers the
following step. For example, every time that the user
enters the house, he has to put the phone in charge in
a visible place near the entrance. When leaving the
house, he has to take the phone, check that it is on,
and carry it with him.
Learning transfer refers to the ability to use past
experiences to do a new task or the same task in a
new context (Barnett and Ceci, 2002). As reported
by Bier et al. (Bier et al., 2008), sometimes in
dementia learning is very effective, but transfer of
the learned skills to a new situation which may be
different from the one in which the skill has been
learned can be difficult. There are several techniques
aimed at minimizing this problem. For example,
learning can happen in locations that are as similar
as possible to the contexts where the skills will then
have to be applied, i.e. the users can practice the use
of their new devices while actually walking in the
real roads of their town. Furthermore, specific tasks
can be designed to stimulate transfer by asking the
person to use the new skills in different, but similar,
contexts. Studies reported by Bier et al. show that
transfer is possible in mild dementia when the target
situation is similar enough to the learning one.
The last critical issue that we have identified is
related to spontaneous use of the learned new skills
in everyday living, which has not yet been
extensively studied in literature. As reported by Bier
et al. (Bier et al., 2008), it may happen that a new
skill is learned, but then the person does not
spontaneously use it in everyday life, even when
prompted to do so. In our case, in order to use the
newly learned tools, the user has to be able to
recognize the situation (i.e. he is having problems
with his orientation to space or time), remember the
information (remember that he has a tool that can be
helpful and how to use it) and have an intention to
do it. It appears that stressing situations influence
negatively the users’ performance, therefore, an
action that may not cause any problem in a normal
situation, may be impossible when the context
becomes stressful. According to Nygård and
Starkhammar, using a technological tool in case of
an emergency outside the home is stressful, and
therefore unlikely to happen (Nygård and
Starkhammar, 2007).
5 CONCLUSIONS
Dementia appears to be one of the major causes of
dependency for old people in the whole world.
Among the most common symptoms of dementia,
there is memory loss and weak orientation to space
and time, which impact on the individual freedom to
move autonomously around town, causing social
isolation and limiting the person’s interests and
activities. We propose to use a cloud-based system,
which has been developed in support of the urban
mobility of people with intellectual disabilities and
that can be adapted to people affected by mild to
medium dementia. The system, which uses a set of
specific apps on a smart phone and a combination of
geolocation systems to keep track of the user’s
movements, offers him the possibility to receive
help when needed, to get in touch with a friendly
voice or to have suggestions to find the way back
home. At the same time, the system would be
socially discrete and non-invasive, guaranteeing the
person’s privacy and independence. Furthermore,
while increasing both independence and safety of the
person, the system would also support and reassure
families and caregivers.
Several issues have to be considered to make this
goal feasible. First of all, a specific adaptation of the
tool has to be done in order to respond to the
different needs of the users, making interfaces as
simple as possible and straightforward to use
(Bocconi, Dini, Ferlino, and Ott, 2006). Special
attention has then to be paid to the introduction of
the system into the users’ lives. The errorless
learning approach is probably the best way to teach
people with mild dementia how to take care and use
their new device. Individual learning paths need to
be studied with the direct and continuous support of
the caregivers and specific fixed routines are needed
in order to guarantee that the users remember to
charge their smart phones and carry them when
leaving the house.
Some issues still need further investigation. The
training phase has to be integrated with specific
actions to foster learning transfer, helping the people
with dementia to recognize those situations when the
tools could be helpful even when they differ from
the learning ones. Furthermore, spontaneous use of
the new system still has to be investigated,
especially with respect to stressing situations as may
be emergencies or, simply, realizing that we have
lost our way home.
A specific experiment is needed in order to find
an answer to these research questions, which would
give the community further insight on the learning
AMobileGuardianAngelSupportingUrbanMobilityforPeoplewithDementia-AnErrorlessLearningbasedApproach
311

possibilities still available to people with mild
dementia, as well as an assessment on the real
advantages of the use of a simple mobile based
system in support of their mobility.
ACKNOWLEDGEMENTS
The author would like to thank Michela Ott and
Ilaria Caponetto for their patience in reading and
making useful comments the present paper.
REFERENCES
Barnett, S. M., and Ceci, S. J. (2002). When and where do
we apply what we learn?: A taxonomy for far transfer.
Psychological Bulletin, 128(4), 612.
Bier, N., Provencher, V., Gagnon, L., Van der Linden, M.,
Adam, S., and Desrosiers, J. (2008). New learning in
dementia: transfer and spontaneous use of learning in
everyday life functioning. Two case studies.
Neuropsychological Rehabilitation, 18(January 2015),
204–235. doi:10.1080/09602010701406581.
Bocconi, S., Dini, S., Ferlino, L., and Ott, M. (2006,
September 20). Accessibility of Educational
Multimedia: in search of specific standards.
International Journal of Emerging Technologies in
Learning (iJET). Retrieved from http://online-
journals.org/index.php/i-jet/article/view/60.
Clare, L., Wilson, B. A., Carter, G., Breen, K., Gosses, A.,
and Hodges, J. R. (2000). Intervening with Everyday
Memory Problems in Dementia of Alzheimer Type:
An Errorless Learning Approach. Journal of Clinical
and Experimental Neuropsychology, 22(1), 132–146.
doi:10.1076/1380-3395(200002)22.
Committee for Medicinal Products for Human Use.
(2008). Guideline on medicinal products for the
treatment of Alzheimer’s Disease and other dementias
(No. CPMP/EWP/553/95 Rev. 1). London: European
Medicines Agency.
Costa, F., Freina, L., and Ott, M. (2015). A Cloud
Computing Based Instructional Scaffold to Help
People with the Down Syndrome Learn Their Way in
Town. In INTED (p. in press).
De Werd, M. M. E., Boelen, D., Olde Rikkert, M. G. M.,
and Kessels, R. P. C. (2013). Errorless learning of
everyday tasks in people with dementia. Clinical
Interventions in Aging, 8, 1177–1190.
doi:10.2147/CIA.S46809.
Di Carlo, A., Baldereschi, M., Amaducci, L., Lepore, V.,
Bracco, L., Maggi, S., … Inzitari, D. (2002). Incidence
of Dementia, Alzheimer’s Disease, and Vascular
Dementia in Italy. The ILSA Study. Journal of the
American Geriatrics Society, 50(1), 41–48.
doi:10.1046/j.1532-5415.2002.50006.x.
Freina, L., Busi, M., Canessa, A., Caponetto, I., and Ott,
M. (2014). Learning to Cope With Street Dangers: an
Interactive Environment for Intellectually Impaired. In
EDULEARN14.
Freina, L., and Ott, M. (2014). Discussing Implementation
Choices for Serious Games Supporting Spatial and
Orientation Skills. In ICERI 2014 (pp. 5182–5191).
Hanson, E., Magnusson, L., Arvidsson, H., Claesson, A.,
Keady, J., and Nolan, M. (2007). Working together
with persons with early stage dementia and their
family members to design a user-friendly technology-
based support service. Dementia, 6(3), 411–434.
doi:10.1177/1471301207081572.
Harris, P. B. (2006). The Experience of Living Alone
With Early Stage Alzheimer’s Disease: What Are the
Person's Concerns? Alzheimer’s Care Quarterly, 7(2),
84–94.
Nygård, L., and Starkhammar, S. (2007). The use of
everyday technology by people with dementia living
alone: mapping out the difficulties. Aging and Mental
Health, 11(February 2015), 144–155.
doi:10.1080/13607860600844168.
Robinson, L., Brittain, K., Lindsay, S., Jackson, D., and
Olivier, P. (2009). Keeping In Touch Everyday
(KITE) project: developing assistive technologies with
people with dementia and their carers to promote
independence. International Psychogeriatrics / IPA,
21(3), 494–502. doi:10.1017/S1041610209008448.
Smart Angel. (2014). Project Description. Retrieved from
www.smartangel.it.
Terrace, H. S. (1963). Discrimination learning with and
without “errors”. Journal of the Experimental Analysis
of Behavior, 6, 1–27. doi:10.1901/jeab.1963.6-1.
Topo, P. (2008). Technology Studies to Meet the Needs of
People With Dementia and Their Caregivers: A
Literature Review. Journal of Applied Gerontology,
28(1), 5–37. doi:10.1177/0733464808324019.
World Health Organization. (2012). Dementia. Retrieved
from
http://www.who.int/mediacentre/factsheets/fs362/en/
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
312
