
Computer Games for Older Adults beyond Entertainment
and Training: Possible Tools for Early Warnings
Concept and Proof of Concept
Béla Pataki
1
, Péter Hanák
2
and Gábor Csukly
3
1
Department of Measurement and Information Systems, Budapest University of Technology and Economics,
Műegyetem rakpart 3., Budapest, H-1111, Hungary
2
Healthcare Technologies Knowledge Centre, Budapest University of Technology and Economics,
Műegyetem rakpart 3., Budapest, H-1111, Hungary
3
Department of Psychiatry and Psychotherapy, Semmelweis University, Balassa utca 6., Budapest, H-1038, Hungary
Keywords: Computer Games, Serious Games, Silver Games, Cognitive Disorders, Mild Cognitive Impairment (MCI).
Abstract: Old age cognitive deficit is a relatively new mass-phenomenon due to the fast growth of older populations,
and the fact that dementia is chronic, progressive, long lasting and, so far, incurable. However, in the early
phase of cognitive decline symptoms do not manifest clearly, and may remain unexplored for a longer peri-
od of time. Clinical tests, using either paper-based or computerized methods, are made quite infrequently,
providing too sparse snapshots of the cognitive performance. In this paper, computer games are proposed
for home monitoring of possible significant changes in mental state. This approach is advantageous as it is a
regular but voluntary method. This way, more frequent assessments are possible than with the traditional
clinical test scenario. Problem descriptions, possible solutions and methods, presented in this paper, have
been elaborated in the AAL project Maintaining and Measuring Mental Wellness (M3W). The ultimate goal
of the project is to develop a computer game toolset and a methodology for monitoring the mental state of
older adults remotely (at home). As it is a complex task, only basic considerations and concepts, a few chal-
lenges, problems and potential solutions, the proposed architecture, and the proofs of the concept are pre-
sented in the paper.
1 INTRODUCTION
The world's population is aging: “those aged 65
years or over will account for 28.7 % of the EU-28’s
population by 2080, compared with 18.2 % in 2013.
As a result of the population movement between age
groups, the EU-28’s old-age dependency ratio is
projected to almost double from 27.5 % in 2013 to
51.0 % by 2080 (Eurostat, 2014).
Older adults have to cope with physical and men-
tal impairments. Old age cognitive deficit is a rela-
tively new mass-phenomenon due to the fast growth
of older populations, and the fact that dementia is
chronic, progressive, long lasting and, so far, incur-
able. According to Alzheimer's Research UK, “the
annual economic cost of dementia is nearly the same
as the combined economic costs of cancer and heart
disease” (Alzheimer’s, 2014). In December 2013,
the G8 dementia summit called for strengthening
and joining efforts to “identify a cure or a disease-
modifying therapy for dementia by 2025”, and
acknowledged prevention, timely diagnosis and
early intervention of dementia as innovation priori-
ties (Gov.UK, 2013).
Various paper- and object-based psychological
tests have been in use since the beginning of the 20
th
century, aiming at recognizing cognitive disorders.
Recently, their computerized variants as well as
neuroimaging methods have been available for diag-
nostic purposes in clinics. As these are expensive
and need the contribution of specialists, they are not
suitable for mass screening.
In this paper, we propose to use computer games
for the home monitoring of eventual significant
changes in mental state. This approach is advanta-
geous as it is a regular but voluntary method. This
way, more frequent assessments are possible than
with the traditional clinical test scenario.
Section 2 and 3 characterize briefly variants of
cognitive impairments and their recognition possibil-
ities. Section 4 presents the conceptual model of the
285
Pataki B., Hanák P. and Csukly G..
Computer Games for Older Adults beyond Entertainment and Training: Possible Tools for Early Warnings - Concept and Proof of Concept.
DOI: 10.5220/0005530402850294
In Proceedings of the 1st International Conference on Information and Communication Technologies for Ageing Well and e-Health (AGEWELL-2015),
pages 285-294
ISBN: 978-989-758-102-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

proposed system for the assessment of mental
changes. Section 5 describes the system developed
in the Maintaining and Measuring Mental Wellness
(M3W) project: first, it summarizes the so-called
early pilot, then sketches the M3W ICT architecture,
presents the game categories, and finally introduces
the logging and scoring procedures. Section 6 dis-
cusses evaluation challenges and proposes several
approaches. Section 7 presents proofs of the detec-
tion method. Finally, Section 8 summarizes our
findings, and shows directions for further work.
2 COGNITIVE IMPAIRMENTS
The early sign of having a higher risk for a patholog-
ical decrease in cognition is called Mild Cognitive
Impairment, abbreviated as MCI (Werner, 2008); in
this state, conversion to dementia is much higher
(>10-15%) than with healthy older people. The im-
portance of recognizing the population at risk is
underlined by scientific data showing that treatment
initiated in the early phase can prolong this phase,
and improve the ability for independence (Budd,
2011). However, in the early phase of cognitive
decline symptoms do not manifest clearly, and may
remain unexplored for a longer period of time. Fur-
ther, it is not easy to identify the stage at which the
process becomes abnormal, and the affected person
requires serious attention, perhaps medical interven-
tion, as MCI is a set of symptoms rather than a spe-
cific medical condition or disease. A person with
MCI has subtle problems with one or more of the
following (Alzheimer’s, 2015):
• day-to-day memory,
• planning,
• language,
• attention,
• visuospatial skills (the ability to interpret objects
and shapes).
With early detection of MCI people at risk can
get advice, support and therapy in time. Early diag-
nosis also allows people to plan ahead while they are
still able to do so. As said above, cognitive decline
can be significantly slowed down in an early stage.
However, early detection is rare because cognitive
tests are usually performed only when there are
clear signs of cognitive deficit. The natural denying
effect by the older adult, their family members and
friends may lead to significant additional delays.
Traditional, validated, paper-based clinical tests
constitute the gold standard but they have several
drawbacks. Such tests require specialist centres and
highly trained professionals. Therefore, there is a
growing interest in the development of computerized
cognitive assessment batteries (Cantab, 2015),
(MindStreams, 2015), (Dwolatzky, 2011). However,
clinical tests, using either paper-based or computer-
ized methods, are made quite infrequently, provid-
ing too sparse snapshots of the cognitive perfor-
mance.
3 GAMIFYING MCI DETECTION
Regular home – remote – monitoring of changes in
mental state offers a powerful alternative, even if it
allows only relatively noisy and less targeted meas-
urements. It has the advantage of frequent assess-
ments, and thus it offers the possibility of evaluating
temporal trends. Current computerized and clinically
validated tests are not suitable for this purpose as
they have been developed for professional use; in
consequence, they are expensive, not entertaining,
and require the presence of medical staff. Therefore,
new measurement methodologies should be devel-
oped and validated, specifically for this strategy.
As more and more older adults use computers,
and many of them play computer games regularly,
this activity can be exploited for measuring their
performance in those games. According to some
experimental studies, this performance is related to
their cognitive state. In consequence, there is a
growing interest in the development of special com-
puter games for cognitive monitoring and training
purposes, addressing specific cognitive domains,
such as verbal fluency (Jimison, 2008), executive
functions (López-Martínez, 2011), or perceptual and
motor functions (Ogomori, 2011).
A major challenge in using computer games in-
stead of cognitive tests is that entertainment capabil-
ity and measurement power pose contradictory re-
quirements. There are three approaches in game
development for older adults, namely
• adapting well-known, popular games (e.g.,
chess, Tangram or Tic-tac-toe (Menza-Kubo,
2013), Find the Pairs, Freecell (M3W, 2015);
• transforming special clinical tests, e.g., Corsi
block-tapping, paired associates learning, Wis-
consin card sorting (M3W, 2015), into games;
• developing new games specially designed for
this purpose (López-Martínez, 2011).
Regular monitoring may be (1) controlled or (2)
voluntary. Controlled monitoring works only with a
highly motivated minority; since most older adults
are mentally healthy in the early monitoring period
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
286
(i.e., before detecting a decline), they deny to partic-
ipate in controlled monitoring as it seems to under-
mine their preferred independence.
Our basic idea is the following: with regular but
voluntary use of computer games developed or
modified specifically for older adults, we may be
able to measure the mental changes and tendencies
over time in an entertaining way.
The problems, possible solutions and methods,
presented in this paper, are based on a recent re-
search project, Maintaining and Measuring Mental
Wellness (M3W, 2015), (Sirály, 2013), (Hanák,
2013). The ultimate goal of the project is to develop
a toolset and a methodology for monitoring the men-
tal state of older adults remotely (e.g., at home),
which is a very complex task. Therefore, only the
basic considerations and concepts, a few challenges,
problems and solutions, the proposed architecture,
and the proofs of the concept are presented in this
paper. Many other important problems, such as
player motivation and game selection, are not dis-
cussed here in detail.
One of the biggest challenges is to find the right
balance between entertainment capability and
measurement power. In order to cope with this chal-
lenge, the game set has been evolving since our
early pilot experiments, performed in 2012/2013.
Unfortunately, the changing of the games and the
collected data poses another significant challenge as
basically non-comparable data have to be compared
somehow in the long run. To this end, we propose a
kind of sensor-fusion approach that will be described
later, in Section 6.
4 CONCEPTUAL MODEL
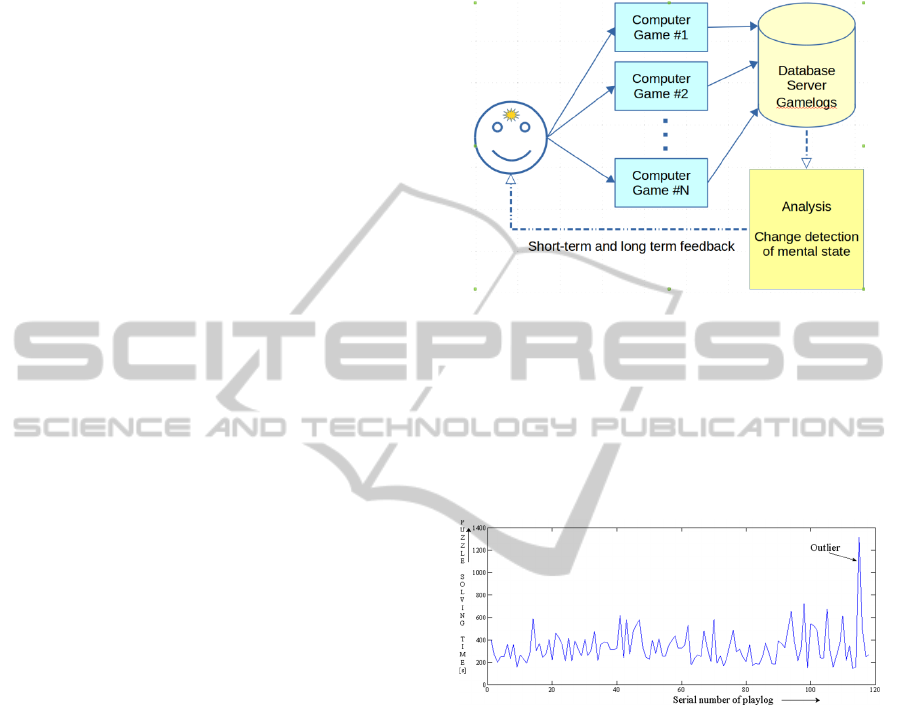
The basic conceptual model of the proposed system
is shown in Figure 1. The final goal is to provide
appropriate long-term feedback (warning) to the user
or to a caregiver, family member, medical expert,
etc., when a significant change in mental state has
occurred. Short-term feedback is needed as motiva-
tion to continue participation in the monitoring.
Several games have been considered. Most of the
chosen ones are logical puzzles, or games that need
the intensive use of the short-term memory (its dete-
rioration is one of the best indicators of MCI), but
other important cognitive abilities and processes
(attention, executive function, comprehension, lan-
guage skills, planning, decision making, etc.) are
targeted as well (see details in Section 5).
Two types of basic parameters are measured cur-
rently: the solving time of the puzzle and the amount
of the good and bad steps taken during the solution.
Figure 1: Basic conceptual model of the cognitive state
evaluation system.
In Figure 2, a typical series of performance is
shown for a player playing the same game nearly
120 times. The time span of that series was 14
months. The performance is fluctuating around a
mean value, and there is an outlier far from the usual
values.
Figure 2: Typical performance series of a player measured
with a given computer game.
Beyond the general problems of such systems
(e.g., data privacy concerns), this approach has its
special challenges:
1) How to measure cognitive performance using
computer games?
2) How to cope with the typically heavy noise of
the uncontrolled (home) measurement envi-
ronment?
3) How to motivate people to take part in the long
run?
4) How to compare performance shown in differ-
ent games, which is basically a special sensor-
fusion problem?
After describing the ICT architecture and com-
ponents in the next section, we shall propose various
ComputerGamesforOlderAdultsbeyondEntertainmentandTraining:PossibleToolsforEarlyWarnings-Conceptand
ProofofConcept
287
approaches and procedures as possible answers to
these challenges.
5 ICT ARCHITECTURE AND
COMPONENTS
5.1 Early Pilot
In a one-year pilot study in 2012/2013, more than 50
volunteers registered to take part and help evaluate
the framework and the games developed at that time.
Due to the voluntary nature of the project only about
20 of them played regularly for nearly one year at
home and in an elderly home. (Of course, the paral-
lel development of the program package was a
drawback for the players.) The average age of these
regular players was 70.3, and the standard deviation
was 10.9 years.
Because of the relatively short test period, its rel-
evance was limited in regard to mental aging; none-
theless, we found some findings as clearly important
for the long run as well. Parallel to the home moni-
toring pilot study, clinical examinations on patients
with mental problems (MCI, Alzheimer’s disease,
etc.) were also performed (Sirály, 2013); (Sirály,
2015).
The software package for the early pilot was
written in Java, and had to be downloaded and in-
stalled; it was a challenge for many older adults.
Recent advancements of internet and browser tech-
nologies have made it possible to develop the soft-
ware in HTML5, JavaScript and PHP in the second
phase, go online, and become available on various
platforms, including touchscreen devices.
5.2 Global Architecture
The current implementation is composed of the
M3W frame and the set of games – the Game Ser-
vice. The M3W frame ensures a unified layout and
provides various services to the games, incl. com-
pleting and passing the gamelogs to the Data Ser-
vice. The Game Service can be displayed in a big-
enough iframe in any webpage. Authentication and
authorization – i.e. provision of a User Register – is
the responsibility of the webserver hosting the Game
Service.
For older adults, especially for those with limited
computer skills and, to some extent, affected by
cognitive impairment, ease of use (incl. easy regis-
tration and login) is especially important. For them,
modern Single-Sign-On (SSO) solutions can be very
helpful. Therefore, despite the immature status of
and frequent changes in SSO applications, we have
implemented such services based on an open source
solution, simpleSAMLphp (SSP) that is used world-
wide in higher education. With SSP, on the one
hand, a so-called identity provider (IdP) can inte-
grate authentication services of a number of external
authentication sources, incl. social login services
offered by social network providers, such as Google,
Facebook and LinkedIn. On the other hand, a web-
service can be amended by a so-called service pro-
vider (SP) with SSP such that this webservice can
utilize the authentication mechanisms of one or more
IdPs.
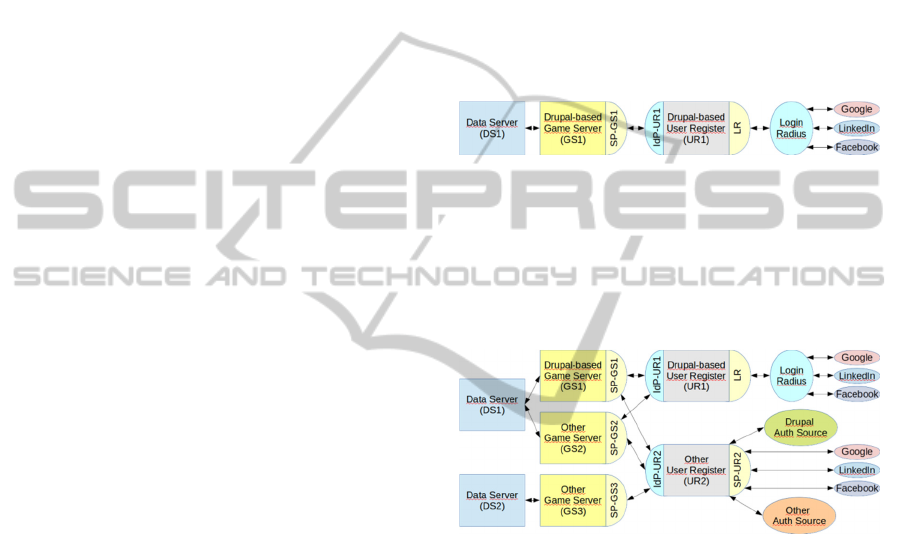
Figure 3: Simple distributed architecture.
In the simplest case, User Register (UR), Game
Service (GS) and Data Service (DS) can run on the
same server (e.g., a Drupal 7 instance may be used
for this purpose). A simple distributed architecture is
depicted in Figure 3.
Figure 4: Complex distributed architecture.
Sometimes more sophisticated architectures are
needed. For example, with a high number of users
the load on a single GS may be too high, and a sec-
ond GS has to be added. In another situation, privacy
concerns or regulations might require that the UR
remain under the authority of an institution, or with-
in a country, so the UR must be duplicated or even
multiplied. Further, the collected data might be con-
sidered as sensitive despite that they contain no
personal data only an integer player identifier. In
such situations, it must be ensured that the DS be
duplicated or multiplied. SSP ensures the necessary
scalability and connectivity also in such cases. Fig-
ure 4 illustrates a situation where a complex M3W
system is realized by two DS, three GS, three UR
and six SSP instances, and other external services.
Note that both GS and UR services can be real-
ized without Drupal.
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
288

5.3 Cognitive Abilities and Game
Categories
Cognitive abilities are mental skills needed to carry
out tasks. They are mechanisms of how we learn,
remember, plan, execute, solve problems, pay atten-
tion, etc. Major categories of cognitive abilities are
perception, attention, memory, motor skills, lan-
guage skills, visual and spatial processing, and
executive functions.
Cognitive tests – traditional or computerized –
are designed to measure one of these abilities in
order to maximize their assessment capability; they
are not designed for frequent use. However, in case
of cognitive games, their measurement potential
must be accompanied by entertaining power as they
must motivate the user to play regularly for a long
time.
Figure 5: Snapshot of the M3W playground.
The M3W set of games tries to satisfy both ma-
jor requirements. Each game belongs to at least one
of five categories: attention, planning, language
skill, memory and execution (see Figure 5). Most
games try to focus on one cognitive category; e.g.,
Birds, Boxes, Differences or Lost Lego deals with
attention, Find the Pairs with memory, Gopher with
(motor) execution. Games belonging to category
planning are usually more complex, i.e. more de-
manding; examples for such games are FreeCell,
Sudoku, Blocks, Planargame, or Labyrinth (because
of its complexity the latter was added more for en-
tertainment than assessment).
Additionally, a few known tests are also made
available in the category cognitive tests. They may
be used as sort of reference: the results gained with
these tests may be compared with the results gained
with the games.
5.4 Game Logging
As mentioned in Section 4, the solving time and the
amount of good and bad steps have recently been
used for statistical analysis. However, parameters
describing the game settings, the gaming platform
and the course of playing the game are also recorded
in the game logs; these data can and will be used
later to compute suitable indicators.
Settings are game-specific such as difficulty level,
word length and language, turning or moving speed,
appearance time, board size, etc. Platform parame-
ters include monitor resolution, browser version,
operating system, the use of mouse, touchpad or
touchscreen, etc. The course of playing the game is
described by all significant mouse clicks or touches
with timestamps.
Game logs are json-objects, saved into files.
Each game log consists of five components and
several subcomponents:
1. Game descriptor
numeric identifier, name category, version
2. Player identifier
numeric identifier
3. Parameters:
date, options, seed, platform, log version
4. Events
game-specific series of time-stamped event-
items
5. Statistics
score, play time, game-specific aggregated val-
ues
5.5 Score Calculation
Scoring follows the same principle and procedure
for every game. The highest reachable score depends
on difficulty settings. On the lowest and highest
difficulty levels the maximal score is 600 and 1000,
respectively. High score limits on intermediate diffi-
culty levels (i.e., between the lowest and highest
levels) are distributed linearly. Difficulty levels are
defined in the game settings.
In every game, various faults may occur that
may lead to score deductions. Fault calculation may
take playtime, bad move, wrong mouse click, erro-
neous selection, etc. into account. The extent or
seriousness of a fault is called fault value. For each
fault, there is a threshold, a limit and a weight. A
fault value exceeding the threshold results in score
deduction. A fault value reaching the limit causes
maximal weighted deduction.
ComputerGamesforOlderAdultsbeyondEntertainmentandTraining:PossibleToolsforEarlyWarnings-Conceptand
ProofofConcept
289
The common score calculator has four argu-
ments: currentValues, goodValues, acceptableVal-
ues and weights.
Fault values are passed to the score calculator as
currentValues, threshold values as goodValues,
limits as acceptableValues, and weights as weights.
With weight=1.0, a fault value reaching the limit
sets the deduction to produce a score element of 333.
Smaller weights produce smaller deductions, larger
weights larger deductions.
The score calculator aggregates the deductions
caused by various faults. During calculation, when
the final score reaches 400, further deductions are
reduced to one-third of their original values. When
the final score reaches 200, score calculation stops.
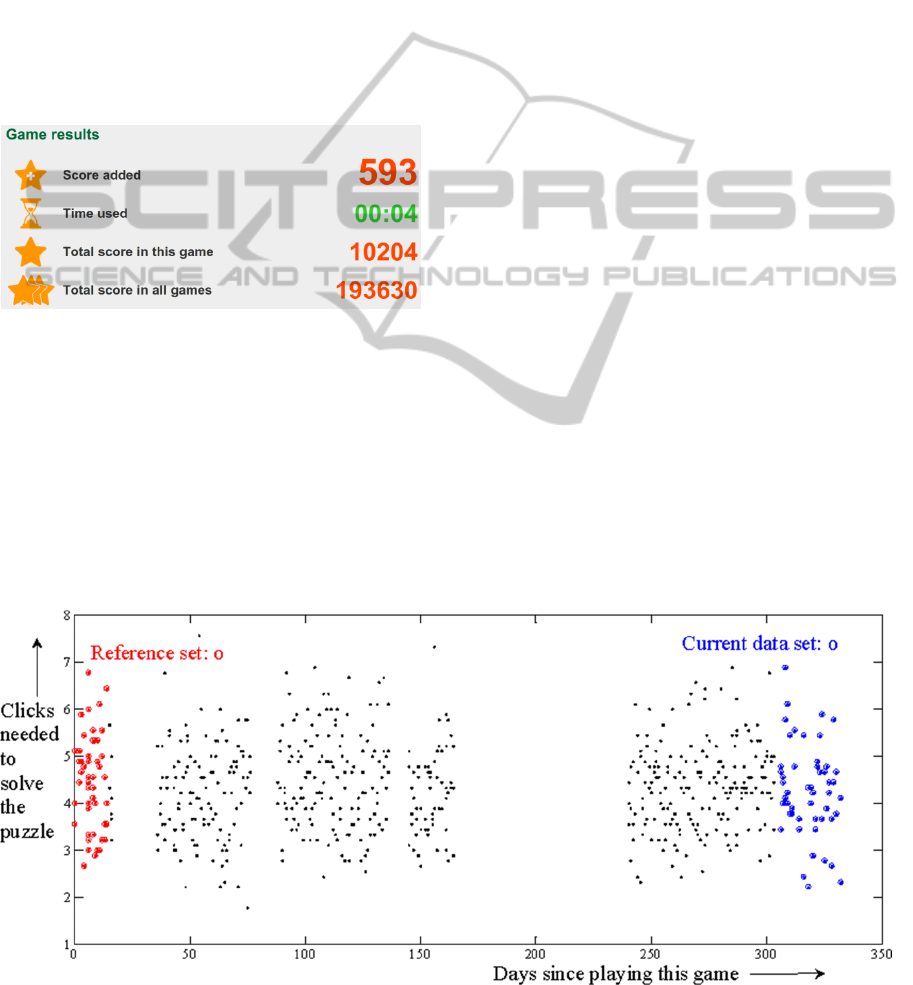
Figure 6: Snapshot of a game result.
Primary score calculation is performed by the
games themselves. The primary score is the basis for
the immediate feedback to the user (see Figure 6).
Secondary score calculation is performed when
stored game logs are reprocessed and uploaded into
the database. The secondary score is used as an
indicator of cognitive performance. (More sophisti-
cated indicators might also be computed.) Since all
original game logs are stored, score calculation may
be refined later in order to improve our assessment
methods, and thus the recognition of changes in
mental wellness.
6 SUGGESTIONS TO MEET THE
CHALLENGES
To assess the cognitive state, it is assumed that per-
formance measured in playing computer games
correlates with cognitive wellness. As it will be
shown in Section 7, there is indirect evidence that
this assumption is valid.
The measurement of the mental state on an abso-
lute scale is very difficult as it depends on education,
physical health, etc. For our purpose, fortunately, it
is enough to detect only the change in a person’s
cognitive performance, and it is an easier task.
For measuring change, a reference is needed.
There are two possibilities: the performance of a
person can be compared to the performance of other
persons in a reference group; or it can be compared
to a previously measured reference of the same per-
son.
Because the person-to-person comparison is af-
fected by several parameters that are unknown with
this voluntary, uncontrolled method (education,
physical abilities, family conditions, profession,
environment, etc.) the comparison to the same per-
son’s previous performance was chosen (c.f. Figure
7).
To cope with the heavy noise present, data are
cleaned before analysis: outliers are detected and
omitted. Outliers are usually caused by inter-
rupts(due to social or physiological reasons). There
is another noise term caused by random differences
Figure 7: Performance measure of a player during nearly one year.
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
290
between consecutive puzzles, by minor environmen-
tal disturbances, by tiredness, etc. It is reasonably
assumed that the short-term fluctuations are zero-
mean, stable independent random variables. To
decrease the assessment error caused by this noise
term, performance measured only in a single game
will not be evaluated; in its stead, performance
measured on a reference set will be compared to
performance on the current set (c.f. Figure 7).
While our goal is to detect the decline of perfor-
mance, in some periods improvements can occur as
well. The assumption is that the decline is preceded
by a longer period where the situation is stable or
deteriorating very slowly. Therefore, the reference is
chosen as the group of consecutive games in which
the person had shown stable performance (see Fig-
ure 7 and Figure 10).
The puzzle difficulty and the short-term change
of cognitive performance are both zero mean ran-
dom variables. The very slow, long-term change of
the cognitive state is modelled differently. There-
fore, if a change is detected in one of the integral
characteristics (mean, median, standard deviation),
or generally in the distribution of the composite
random variable (mental state plus game noise), then
it is caused by the slowly changing component mod-
elling the mental state.
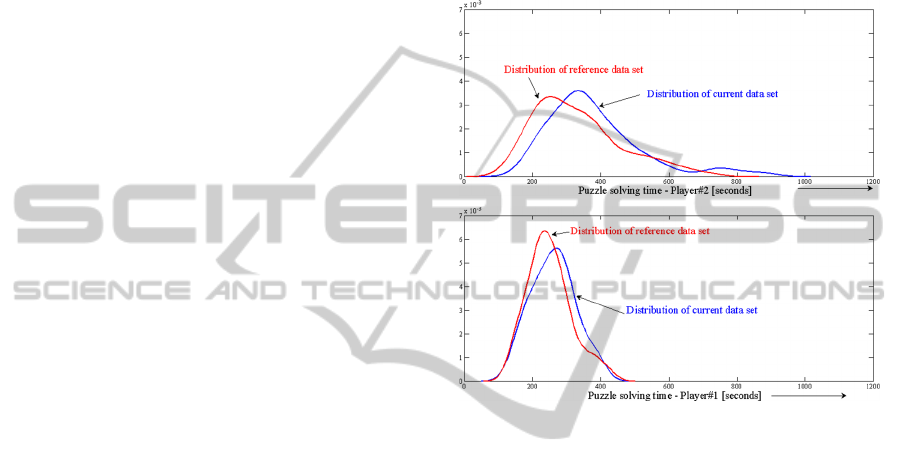
In Figure 8, the distributions of the same perfor-
mance measure (puzzle solving time) in the same
game are shown for two players. In each diagram
two performance distributions of the given player
are drawn (red line: distribution of reference data,
blue line: distribution of current data). Of course, the
performance distributions of the same players in two
time periods will not be exactly the same, but statis-
tically the identical distribution assumption cannot
be rejected. However, for different players, not only
the parameters of the distributions differ from player
to player but the shapes are different as well.
It was investigated whether the parameter distri-
butions are Gaussian ones or not. The Lilliefors test
rejected the normality hypothesis in most of the
cases. Therefore, nonparametric tests are suggested
to check if the distribution has not changed the hy-
pothesis.
6.1 Nonparametric Tests
There are several applicable nonparametric tests, for
example the Mann-Whitney U test, the Kolmogorov-
Smirnov two-sample test, the Wilcoxon signed-rank
test, etc. Any of these methods can be used to com-
pare the distribution of the reference subset with the
distribution of the currently examined subset of the
time series, and normality is not necessary. If we
detect a difference between the distributions of the
two sub-samples, and the current part of the series
has a smaller average (of ranks, of scores, etc.), then
the player shows performance degradation. Up to
now, the Kolmogorov-Smirnov two-sample test and
the chi-square test were extensively used. It will be
investigated later which is the optimal statistical
hypothesis test for this kind of problems.
Figure 8: Performance measure distributions of two play-
ers.
The following findings were obtained:
• The results gained with the Kolmogorov-
Smirnov two-sample test and the chi-square test
have confirmed that both the stability and the
change in the parameters are reliably estimated
with these statistical hypothesis tests.
• In case of a new game a learning phase occurs
when results are improving. The reference is
meaningful only when the performance is stabi-
lized (c.f. Figure 11).
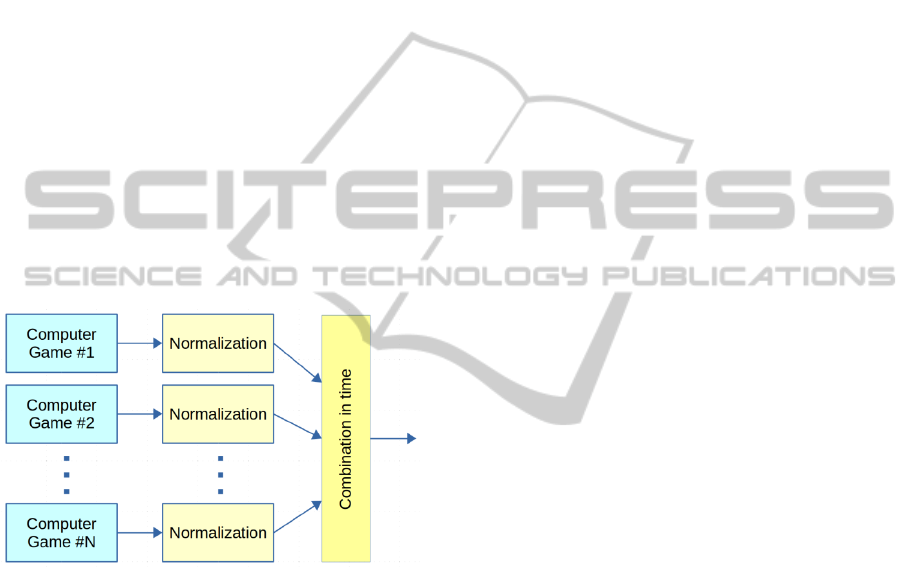
6.2 Sensor Fusion with Games as
Sensors
Motivation of older adults to play frequently and
regularly the computer games is one of the most
important challenges to solve. Early detection is the
purpose; but the main problem is that nobody knows
when the abnormal change will happen; maybe only
after many years, or in some persons’ life never.
Therefore, the motivation must be kept alive proba-
bly for years. It is a very complex problem in itself;
so only some aspects are discussed here. A basic
ComputerGamesforOlderAdultsbeyondEntertainmentandTraining:PossibleToolsforEarlyWarnings-Conceptand
ProofofConcept
291
assumption is that although there is an intrinsic mo-
tivation that everybody wants to sustain mental
abilities and an independent life of good quality,
generally it is not enough as a motivation in the
long-run. There must be other, extrinsic motivations,
too, e.g., entertaining ways of measurement, and
short-term, immediate feedback (c.f. Figure 1), en-
couraging the user to play further (e.g., scores, sym-
bolic rewards, encouraging messages).
Unfortunately, most people do not enjoy playing
the same game for years. Therefore, in different time
periods different games will be played by the same
person. In order to preserve the level of motivation
of the players, various games are offered (c.f. Figure
1 and 5). – In addition, as mentioned earlier, repro-
grammed or improved games and more sophisticated
logging may replace older ones as assessment meth-
ods are improving while time passes by, or technol-
ogy changes occur. – The performance indicators
measured with different games should somehow be
compared to each other. This implies a sensor fu-
sion and estimation problem; this was discussed in
our previous paper (Breuer, 2015).
Figure 9: The sensor fusion architecture.
In Figure 9, the sensor fusion scenario is illus-
trated. Architecturally, the scenario is a usual sensor
fusion arrangement where computer games are the
sensors. The most important difference is that in a
usual sensor fusion arrangement the sampling is
regular, typically periodic, and the sensors are sam-
pling parallel in the same time instant. In the com-
puter game fusion scenario only one game (sensor)
is used in a time instant, and the sampling intervals
are irregular. Therefore, the currently suggested
method is to normalize all the performance results to
the same zero-mean series, and combine the results
in time to form one combined time-series. In the
future the possibility of applying other fusion meth-
ods will be investigated.
In Figure 7, another effect is clearly present:
there are gaps in the playing activity due to health
problems or social reasons. Analysis of the data gaps
has shown that a few week long interrupts do not
change the performance significantly.
7 PROOF OF THE CONCEPT
Due to the long time needed to detect a critical cog-
nitive change, no direct proof could be collected
during the project till now. Nonetheless, by analyz-
ing the game logs (more than 50 voluntary persons
produced about 150 thousand game logs by playing
the games during the second pilot) some important
facts can be shown.
To provide some calibration, one of the comput-
erized cognitive tests (Paired Associates Learning,
PAL) was implemented in the M3W project, and
players were asked to perform it. Studies have
shown that MCI patients performed poorly on this
test (Égerházi, 2007). Analyzing the performance of
the voluntary players, it turned out that their perfor-
mance shown in the computer games correlates to
their performance measured by the PAL test (Sirály
2013), (Sirály, 2015).
In the PAL test, cards turn up in random posi-
tions after each other for 3 seconds, with abstract
shapes shown on one or more cards. Other cards
remain blank depending on the difficulty level.
When all shapes have been shown, the previously
shown shapes appear one by one in the centre of the
play area, and the player has to choose the card
where that shape has appeared earlier. The test con-
sists of five different levels in eight stages in total,
while the number of the shapes increases from 1 to 8
on the different stages. The player has 10 trials to
complete a given stage, otherwise the test ends. The
arrangement of the cards is asymmetric in the test,
and it changes from stage to stage.
In Figure 10, PAL test performance versus aver-
age puzzle solving time of four players is shown. The
PAL test was characterized by the trials needed to
reach the highest level performed by the given play-
er. Although there were much more participants who
performed PAL tests, these 4 players were selected
for demonstration as they all played more than 90
Freecell games. The outliers were omitted, and the
averages of the playtimes were taken.
In a current study (Sirály, 2015) brain magnetic
resonance (MR) examination was performed on 34
healthy older adults. Beyond the MR examination,
paper based and computerized neuropsychological
tests (i.e., PAL test) and computer games were ap-
plied. There was a correlation between the number
of attempts and the time required to complete the
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
292
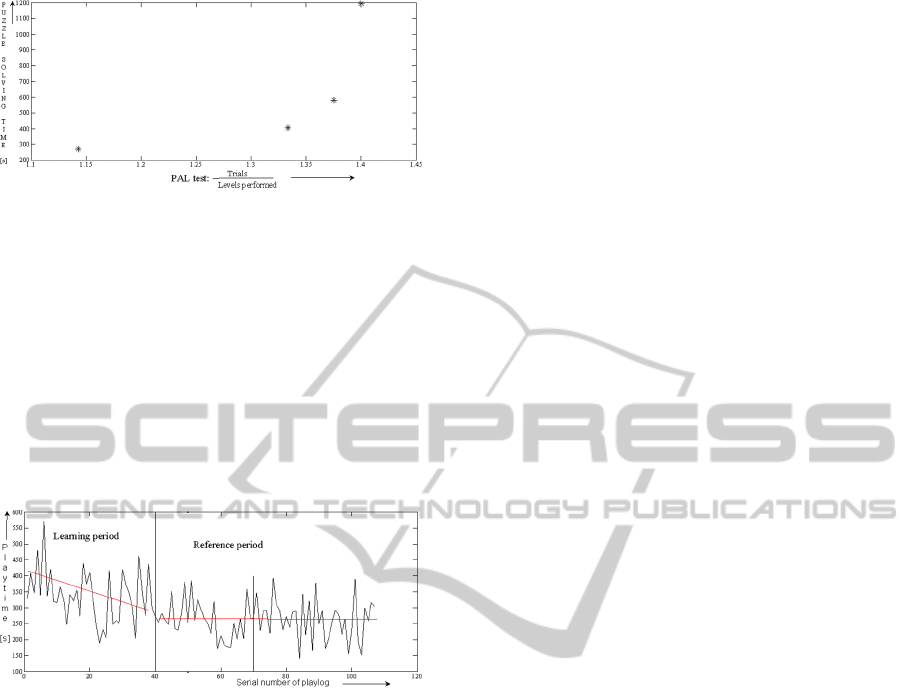
Figure 10: Performance reached at PAL tests and playing
one of the games.
Find the Pairs (also called Memory) game and the
volume of the entorhinal cortex, the temporal pole,
and the hippocampus. There was also a correlation
between the results of the PAL test and the Find the
Pairs game.
Although no healthy
→
MCI transition occurred
during the research period, the other change: signifi-
cant improvement was detected several times. In
Figure 11, performance of a player learning a new
game is shown.
Figure 11: Performance of a player learning a new game.
Applying the Kolmogorov-Smirnov two-sample
test, the same distributions null hypothesis is
• rejected for the learning period while compared
to the reference period (p= 0.0005),
• accepted for the first and second halves of the
reference period (p=0.28).
8 CONCLUSIONS AND FUTURE
WORK
Home monitoring of possible significant changes in
mental state using computer games has been pro-
posed. This approach is advantageous because it is a
regular but voluntary method. Some of the problems
have been analyzed, and solutions have been sug-
gested. The system assumes voluntary participation;
therefore, various games have been developed to
sustain motivation in the long run. In the game bat-
tery there are both well-known, popular games and
modified clinical tests; it is continuously evolving.
For change detection in cognitive performance
the comparison of actual data against historical data
gained from the very same person is proposed, i.e. a
reference set of performance results are to be com-
pared to the current set of results using statistical
hypothesis tests. The null hypothesis is that the two
sets are of the same distribution. Until the null-
hypothesis cannot be rejected, the stability of the
mental state can be assumed.
In the future,
• further pilots have to be launched to validate the
method by more clinical tests,
• the most appropriate games for both entertain-
ment and measurement purposes should be fur-
ther investigated,
• the feasibility of multiplayer games is to be ana-
lyzed,
• collected but currently not analysed data should
be involved into the examinations,
• the potential in the evaluation of the failed
games should be investigated.
ACKNOWLEDGEMENTS
This research was performed in the Maintaining and
Measuring Mental Wellness (M3W) project, sup-
ported by the AAL Joint Programme (ref. no. AAL-
2009-2-109) and the Hungarian KTIA (grant no.
AAL_08-1-2011-0005).
The authors gratefully acknowledge the contribu-
tions of their project partners in Greece, Luxem-
bourg, Switzerland and Hungary. We would like to
express our special thanks to
1. E. Sirály, Semmelweis University, for her con-
tribution to the clinical examinations with real
patients using the PAL test and a selection of
the M3W games;
2. N. Kiss and Á. Póczik, Budapest University of
Technology and Economics, for the improve-
ment and unification of the logging and scoring
procedures;
3. L. Ketskeméty, Budapest University of Tech-
nology and Economics, for exploring and elab-
orating various statistical evaluation algo-
rithms.
REFERENCES
Alzheimer's Society, UK, Dementia statistics, 2014,
http://www.alzheimersresearchuk.org/dementia-
statistics/ [retrieved: April, 2015]
ComputerGamesforOlderAdultsbeyondEntertainmentandTraining:PossibleToolsforEarlyWarnings-Conceptand
ProofofConcept
293

Alzheimer’s Society, Mild Cognitive Impairment, 2015.
http://www.alzheimers.org.uk/site/scripts/documents_i
nfo.php?documentID=120 [retrieved: April, 2015]
Breuer, P., Csukly, G., Hanák, P., Ketskeméty, L., Pataki,
B., 2015. Home Monitoring of Mental State with
Computer Games. In ACHI2015 8th International
Conference on Advances in Computer-Human Interac-
tions.
Budd, D. et al., 2011. Impact of early intervention and
disease modification in patients with predementia Alz-
heimer’s disease: a Markov model simulation. Clini-
coecon Outcomes Res, (2011) 3:189-195.
Cantab test battery, 2015. Cambridge Cognition,
http://www.cambridgecognition.com/ [retrieved: April,
2015]
Dwolatzky, T., 2011. The Mindstreams computerized
assessment battery for cognitive impairment and de-
mentia, PETRA’11 May 2011, pp. 501-504, ISBN:
978-1-4503-0772-7.
Égerházi, A., Berecz, R., Bartók, E., Degrell, I., 2007.
Automated Neuropsychological Test Battery (CAN-
TAB) in mild cognitive impairment and in Alzheimer's
disease. In Progress in Neuro-Psychopharmacology &
Biological Psychiatry 31 (2007) 746–751.
Eurostat, Population structure and ageing. 2014,
http://ec.europa.eu/eurostat/statistics-explained/index.
php/Population_structure_and_ageing
[retrieved: April, 2015]
Gov.UK, G8 dementia summit agreements, 2013,
https://www.gov.uk/government/publications/g8-
dementia-summit-agreements [retrieved: March, 2015]
Hanák, P., et al. 2013. Maintaining and Measuring Mental
Wellness, Proc. of the XXVI. Neumann Kollokvium,
Nov. 2013, pp. 107-110 (in Hungarian).
Jimison, H., Pavel, M. Le, T., 2008. Home-Based Cogni-
tive Monitoring Using Embedded Measures of Verbal
Fluency in a Computer Word Game, 30th Annual In-
ternational IEEE EMBS Conference, Aug. 2008, pp.
3312-3315. doi: 10.1109/IEMBS.2008.4649913.
López-Martínez, A., et al, 2011. Game of gifts purchase:
Computer-based training of executive functions for the
elderly, IEEE 1st International Conf. on Serious
Games and Applications for Health (SeGAH), Nov.
2011, pp. 1-8, Print ISBN:978-1-4673-0433-7 DOI:
10.1109/SeGAH.2011.6165448.
M3W Maintaining and Measuring Mental Wellness, 2015.
AAL Joint Programme project (ref. no. AAL-2009-2-
109) https://m3w-project.eu/ [retrieved: April, 2015]
Menza-Kubo, V., Morán, A., L., 2013. UCSA: a design
framework for usable cognitive system for the wor-
ried-well, Personal Ubiquitous Comput. Vol. 17, Issue
6, Aug. 2013, pp. 1135-1145. ISSN: 1617-4909. DOI:
10.1007/s00779-012-0554-x.
MindStreams, 2015. http://www.mind-streams.com/ [re-
trieved: April, 2015]
Ogomori, K., Nagamachi, M., Ishihara, K., Ishihara, S.,
Kohchi, M., 2011. Requirements for a Cognitive
Training Game for Elderly or Disabled People, Int.
Conf. on Biometrics and Kansai Engineering, Sept.
2011, pp 150–154, E-ISBN 978-0-7695-4512-7, Print-
ISBN 978-1-4577-1356-9,
DOI: 10.1109/ICBAKE.2011.30.
Sirály, E., et al., 2013. Differentiation between mild cogni-
tive impairment and healthy elderly population using
neuropsychological tests, Neuropsychopharmacol
Hung. (3), Sept. 2013, pp. 139-46.
Sirály, E., et al., 2015. Monitoring the Early Signs of
Cognitive Decline in Elderly by Computer Games: An
MRI Study, PLoS ONE. 2015; 10(2):e0117918.
doi:10.1371/journal.pone.0117918.
Werner, P., Korczyn, A. D., 2008. Mild cognitive impair-
ment: Conceptual, assessment, ethical, and social is-
sues. Clinical Interventions in Aging, 3(3), 413–420.
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
294
