
A Review on Discrete-event Simulation and System Dynamics Studies
for Healthcare Problems
Eylül Damla Gönül-Sezer and Zeynep Ocak
Industrial and Systems Engineering Department, Yeditepe University, Kayışdağı, İstanbul, Turkey
Keywords: System Dynamics, Discrete-event Simulation, Healthcare Systems, Modelling.
Abstract: Modeling is the major necessity to enhance the existing systems. Healthcare systems also need to model for
advancing delivered services without compromising any other objectives. Thus, simulation techniques are
frequently preferred in healthcare problems. As was to be expected, simulation has various applications
which yields result in different perspectives. This study discusses two popular simulation techniques;
discrete event simulation and system dynamics techniques in healthcare system applications. The
applications are examined under four main branches based on their scopes. As a result, this paper evaluates
which of these simulation techniques is more practical for different natured healthcare problems.
1 INTRODUCTION
In healthcare problems, main objective must be to
manage overall system by considering patients, care
givers and governmental regulations. In many
applications, proposed models generally create a
solution to currently known problem by altering a
constraint or a parameter. However, this solution
may generate a new problem or increase the impact
of the existing one. Analyzing the influences of
proposed solutions in real systems may be
expensive, time consuming and inefficient for
ongoing processes (Forsberg et al., 2011; Sterman,
2006). Thus, to overcome such problems, simulation
models are preferred.
Simulation modeling has been a frequently used
technique in healthcare for more than four decades
(Brailsford, 2008). In simulation modeling, applied
methods have large spectrum starting from
behavioral to mathematical models (Jeffrey and
Seaton, 1995; Fildes and Ranyard, 1997). Basically,
modelers create solutions for patient flow and
capacity planning.
Discrete event simulation (DES) is accepted as
one of the most popular modeling techniques (Clark,
1999). Thus, DES applications on healthcare have a
significant dominance compared to system dynamics
(SD) method (Brailsford and Hilton, 2001).
However, 70% of SD researches are done to solve
real life problems, only the half of DES studies show
the same performance (Jahangirian et al., 2010).
In this study, SD and DES modeling techniques
are compared for specifically healthcare system
problems. To be able to reach this goal, healthcare
problems are decomposed based on their scopes into
4 major areas:
• Short-term resource management (SRM)
• Process improvement (PI)
• Forecasting & long-term strategy planning (FLSP)
• Causality (C)
In the following sections, DES and SD
applications in healthcare will be discussed in detail
under these four areas.
2 APPLICATIONS IN
HEALTHCARE
Stochastic systems and queuing models could be
interpreted as DES models with a preliminary
condition. Under these circumstances, entities
should be represented by discrete states over time
(Ramwadhdoebe et al., 2009; Fialho et al., 2011). In
this technique, modeler needs a clear event list of the
system and input data must be collected. The data
must be statistically appropriate. These requirements
are generally seen as weaknesses of DES method.
The strength of DES is the ability to incorporate
system details, time dependent behavior, and system
constraints. DES allows decision makers to access
297
Gönül-Sezer E. and Ocak Z..
A Review on Discrete-event Simulation and System Dynamics Studies for Healthcare Problems.
DOI: 10.5220/0005556302970302
In Proceedings of the 5th International Conference on Simulation and Modeling Methodologies, Technologies and Applications (SIMULTECH-2015),
pages 297-302
ISBN: 978-989-758-120-5
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

information about system performance as well as
insight through the effects of changing conditions
over time (Jun et al., 1999; Griffin et al., 2012).
SD models are constructed by stock and flow
variables using the feedback theory. Usage of stock
and flow diagrams offers an advantage to understand
and to clarify the system behavior over time. The
representation of feedback system reflects the
interactions among variables in overall system
easily. Another advantage of SD is in data collection
procedure. In SD, both quantitative and qualitative
data could be used without any restriction which is
not applicable in DES applications.
2.1 Short-term Resource Management
(SRM)
Short-term planning in emergency rooms, clinics
and operating theatres are frequently studied in DES
due to discrete nature of these systems (Fone et al.,
2003). In addition to this, some researchers claim
that there is a significant difficulty to study complex
or combination of multistage systems in DES (Günal
and Pidd, 2010). This statement could be explained
by the nature of the method; changing the scope of
the model means new data is required but that also
creates new restrictions in data analysis stage of
DES. Thus, adding new data is challenging.
Capacity management problems and patient flow
issues in healthcare are more popular areas where
DES is used. Critical resource and capacity
problems in emergency rooms, catheterization
rooms, clinics, and intensive care units are solved
with this simulation technique (Ahmed and
Alkhamis, 2009; Kadri et al., 2014; Rado et al.,
2014). In addition to single-stage problems, some
DES models are constituted for larger resource
allocation problems. Šteins et al. (2010) develops a
model for his thesis which aims to solve matter of
resource utilization for a combination of operating
room, intensive care and radiology examination
units. Meanwhile overall hospital resource allocation
problems are also solved by DES approach, but they
are generally hybrid models, and such studies are
shown rarely in literature (Cochran and Bharti,
2006).
Geranmayeh and Iyer (2008) analyze the
capacity planning for critical resources such as
critical services and procedures, required equipment
in an emergency department by using SD. They try
to develop an economic justification for investment
on laboratory and diagnostic facilities, and
physicians. Wu et al. (2013) try to portrait
differentiating pediatric workforce as a reaction to
altering demand on this specific sector in Taiwan.
The study proposes projections for short-term
demand and supply changes. As shown in given
examples, SD models are used for resource
management problems. However, nature of method
encourages the modelers to make further analysis on
long-term resource and capacity management
problems.
2.2 Process Improvement (PI)
In healthcare systems, the major concern of process
improvement problems is patient flow issues and
schedules. DES applications on patient flow
problems show that the main objective of modelers
is eliminating queues in specific departments. Some
of these papers only focus on enhancing operating
rooms schedules and reducing delay times for
examination and other operations (Marjamaa et al.,
2009; Denton et al., 2010). Additionally, alternatives
for interacting departments are also investigated
(Kuhl, 2012). Such models become too complex,
when a hospital or an institution is taken into
consideration as whole. DES applications are more
suitable for compact process improvement problems.
In process improvement analysis, diminishing
waiting times of patients in any unit of hospitals is
one of the most popular purposes in healthcare.
Minimizing the delays means eliminating
bottlenecks in patient flow processes.
A feedback system is utilized for an accident and
emergency department constituting a dynamic model
for variation of schedule (delay or lead time) in
accident and emergency departments in United
Kingdom (Lane et al., 2000). To diminish waiting
time of patients, they propose to increase the level of
some critical resources and reduce bed capacity. In
another study, as a preliminary model, waiting list
model in cardiac surgery is developed using SD
technique (Hilton, 2001). The main objective of this
study was to understand dynamics of waiting list by
using influence diagrams and interactions among
resources, schedules, etc. Also in another study, the
emergency and urgent care system is modeled by
system dynamics based on patient flow pathways,
and process improvement strategies are examined
for five different scenarios (Lattimer et al., 2004).
2.3 Forecasting and Long-term
Strategy Planning (FLSP)
Discrete event simulation technique is utilized for
long-term strategy planning in healthcare as hybrid
studies only. While DES solves the problems in
SIMULTECH2015-5thInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
298

policy implementations, SD models are appropriate
for policy design interventions (Zulkepli et al.,
2012). Therefore, SD is employed in forecasting
stage and to model the operation (based on the
forecasts) DES is applied in such studies.
To predict demand on long-term care in
Hampshire, a combined model has been developed
(Brailsford et al., 2010). In the first part, SD is used
to estimate population and dynamic demographic
changes in the land for upcoming 20 years. Then, a
DES model is constructed for resource and labor
utilization problems based on handled scenarios
from SD part of the study. In another study, the UK
healthcare system is analyzed for different
governance designs. The impacts and consequences
of designs on organizations are modeled as a hybrid
DES and SD model (Chahal et al., 2008). This
means that, in forecasting, DES is not capable.
Therefore, to provide estimation for future, modelers
need SD in simulation modeling. After creating
forecasts using SD model, DES is applicable to
animate the scenario. The impacts of tactical level
results created in SD model are analyzed in
operational level using DES technique.
Under this section, SD modelers basically
examine the role and interaction of risk factors and
develop forecasts based on their behavior.
Townshend and Turner (2002) studied a sexually
transmitted infection caused by bacteria of the genus
Chlamydia. The model reflects the future effects of
bacteria on behavior of infertility in the UK. In this
study, they provide forecasts for number of the
people who will be infected and forecast for people
treated. Same year, another model developed for one
of the critical communicable diseases; AIDS. This
model predicts the prevalence and volume of this
particular epidemic in Austria (Rauner, 2002). In
another study, a model was proposed for chronic
disease prevention and get projections for this
disease for 50 simulated years by using population
health and healthcare delivery system causal loop
diagrams (Homer et al., 2004). Chen (2003) handled
the non-acute care, home-based health services for
elders, and builds a dynamic model on patient
actions as a supplementary study to plan longitudinal
budget and capacity strategies in Norway. Barber
and his colleague (2010) also chose SD modeling
approach to estimate the medical specialist demand
in Spain, for year 2025. Another study tried to
estimate a next five-year -population for ambulatory
health demands in the US which can be used by
strategic planners (Diaz et al., 2012). Merrill et al.
(2013) stated the policies to execute electronic
health information exchange reports for a regional
health information department. Then, some policies
are advised to overcome the gap between resulted
demand and supply. Again, Ansah et al. (2014)
made projections for future demand analysis in
healthcare. The study shows rising demand on long-
term care for elder people and emphasize on
strategic thinking on resources such as personnel,
equipment, etc.
2.4 Causality (C)
In DES, identifying the relationship among variables
is challenging because it has state variables which
indicates events, queues, resources and time (Dong
et al., 2012). To overcome this problem, again
hybrid models are preferred in literature (Mittal,
2013; Guizzardi et al., 2012). DES models could
interpret the relation between sequential events
individually. By using this characteristic of DES, a
model is built for breast cancer and its screening
procedures (Brailsford, 2012). Including the
patients’ behavioral characteristics and other
psychological data in the model as attributes of
entities is the most attractive side of the study.
Brailsford (2014) suggests hybrid models to add
more behavioral causes in simulation models. Also
another hybrid model utilized to investigate
interventions for colon cancer screening. SD
determines how factors affect the screening rate.
Afterwards, six different interventions are examined
for screening levels on DES (Hosking et al., 2013).
Lubyansky (2005) created an SD model to
analyze the surgery system response in the US in
case of peak periods. These periods are explained
with sudden increases in demand on healthcare
services. Main goal was to model effects on surge
capacity based on demands of patients, supplied
resources (staff, equipment, material, operation
place, etc.), and healthcare policies in the US.
Faezipour and Ferreira (2011) studied the factors
affecting the patient satisfaction in healthcare and
develop an SD model to illustrate the relationship
among these factors. By this way, they developed a
plan for a more sustainable healthcare system.
Causal hypothesis employed in SD are also utilized
for Switzerland Health Reform. The service quality
and costs are analyzed by thinking population aging,
inflation, insurance and poverty (Hirsch et al., 2012).
Another model was developed to understand the
dynamics of long-term care laws, culture and
facilities in Taiwan are illustrated by seeking patient
satisfaction, service quality, administrative skills,
medical care personnel and resources Hsiao and
Huang, 2012). The factors related with global
AReviewonDiscrete-eventSimulationandSystemDynamicsStudiesforHealthcareProblems
299
attention to healthcare systems are analyzed with
another SD model that concerns about the behavioral
impacts of financing, national priority and
differences in health policy approaches (Hafner and
Shiffman, 2013). Another study is constituted for
interpreting the dynamics of child mortality in
Uganda (Rwashana et al., 2014). The factors related
with neonatal mortality are examined using causal
loops. The discrepancy in resources and lack of
awareness on health issues are determined to be as
the most critical factors in this study.
3 COMPARISON
The comparisons between DES and SD are
developed by using two different perspectives. As a
general comparison, the basic steps of modeling are
used. At the second one, the listed scopes of
healthcare problems in introduction are evaluated by
considering the first comparison method.
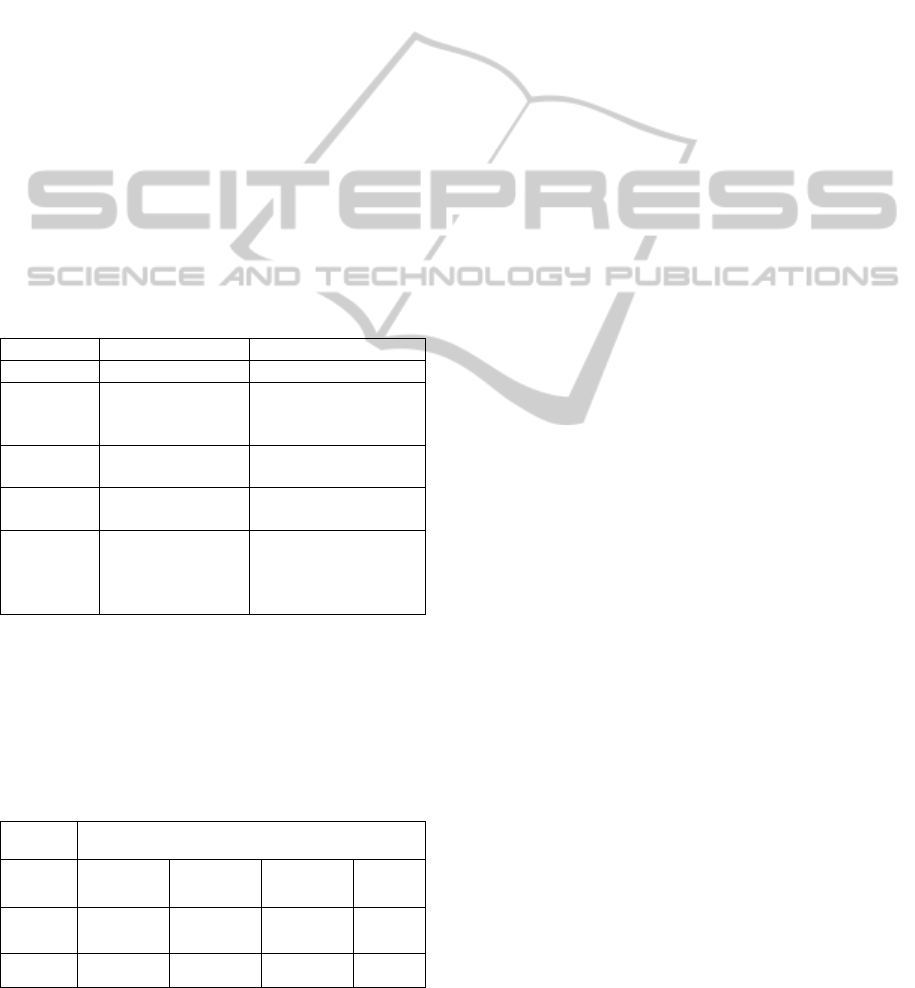
Table 1: Comparison of DES and SD based on simulation
steps.
DES SD
Scope
Operational Strategic
Design
the model
Strict event lists
based on queuing
model
Influence diagrams
based on variables in
model
Gather
the data
Statistically
approved data
No restriction on
data
Validate
the model
t-test Structural and
behavioral checks
Improve
the
system
Statistically
approved
alternative
models
Strategy
development based
on policy analysis
Reconsidering the healthcare problems based on the
five modeling steps for four major healthcare
problem areas on DES and SD applications in
literature, a ranking can be conducted as seen in
Table 2.
Table 2: Applicability of simulation types to healthcare
problems.
Healthcare Applications
(SRM) (PI) (FLSP) (C)
DES
Strong Strong Moderate Weak
SD
Weak Moderate Strong Strong
4 CONCLUSION AND FUTURE
WORK
Tailoring multilevel healthcare problems by DES is
generally problematic. Therefore, DES is preferred
for short-term decisions and analysis on specific
processes. As a result, short-term problems in patient
flow and resource allocation problems are modeled
using this technique. If the modeler needs to
understand causes of a phenomena or wants to get
long-term consequences of his decisions, SD could
be a better choice. Thus, forecasting, causal relations
and long-term consequences of actions could be
represented better with this technique. Considering
the strong aspects of both methods, hybrid studies
that combine these two methods are currently in
demand.
This study provides many suggestions for future
research . The study can be applied to generate
multiple comparisons for different agent-based
simulation techniques. Also, this study can be
extended with numerical and/or statistical evidences
and results.
Future research should examine the interrelated
problems of how to process the available
information on these simulation techniques and how
to use these measures to best control the system.
REFERENCES
Ahmed, M. A., Alkhamis, T. M. 2009.Simulation
optimization for an emergency department healthcare
unit in Kuwait. European Journal of Operational
Research 198(3), 936–942.
Ansah, J. P., Eberlein, R. L., Love, S. R., Bautista, M. A.,
Thompson, J. P., Malhotra, R., Matchar, D. B.
2014.Implications of long-term care capacity response
policies for an aging population: A simulation
analysis. Health Policy,116(1), 105-113.
Barber, P., López-Valcárcel, B. G. 2010.Forecasting the
need for medical specialists in Spain: application of a
system dynamics model. Human resources for health,
8(1), 24.
Brailsford, S. C. 2008. System dynamics: What’s in it for
healthcare simulation modellers. In Simulation
Conference, 2008. Winter (pp. 1478-1483). IEEE.
Brailsford, S. C. 2014. Modeling human behavior: an (ID)
entity crisis?. In Proceedings of the Winter Simulation
Conference (pp. 1539-1548). IEEE.
Brailsford, S. C., Desai, S. M., Viana, J. Towards the holy
grail: combining system dynamics and discrete-event
simulation in healthcare. 2010. In Simulation
Conference (WSC), Proceedings of the 2010
Winter(pp. 2293-2303). IEEE.
Brailsford, S. C., Harper, P. R., Sykes, J.
SIMULTECH2015-5thInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
300

2012.Incorporating human behaviour in simulation
models of screening for breast cancer. European
Journal of Operational Research, 219(3), 491-507.
Brailsford, S.C., Hilton, N. A. 2001. A comparison of
discrete event simulation and system dynamics for
modeling healthcare systems. In: Riley J (ed).
Proceedings from ORAHS 2000. Glasgow: Scotland,
pp 18–39.
Chahal, K., Eldabi, T. 2008.Applicability of hybrid
simulation to different modes of governance in UK
healthcare. In Simulation Conference, 2008. Winter
pp. 1469-1477. IEEE.
Chen, Y. 2003. A system dynamicsbased study on
elderly non-acute service in Norway. In Proceedings
of the 21st International Conference of the System
Dynamics Society, System Dynamics Society, New
York.
Clark, D. N. 1999.Strategic Level MS/OR Tool Usage in
the United Kingdom and New Zealand: A
Comparative Survey. Asia-Pacific Journal of
Operational Research 16 (1): 35-51.
Cochran, K. J., Bharti, A. 2006.A Multi-stage Stochastic
Methodology for Whole Hospital Bed Planning Under
Peak Loading. International Journal of Industrial and
Systems Engineering (1 (1/2)), 8-35.
Denton, B.T., Miller, A.J., Balasubramanian, H.J.,
Huschka, T.R. 2010. Optimal Allocation of Surgery
Blocks to Operating Rooms Under Uncertainty.
Operations Research, 58(4), 802—816.
Diaz, R., Behr, J. G., Tulpule, M. 2012.A system
dynamics model for simulating ambulatory health care
demands. Simulation in Healthcare, 7(4), 243-250.
Dong, Y., Chbat, N. W., Gupta, A., Hadzikadic, M., Gajic,
O. 2012.Systems modeling and simulation
applications for critical care medicine. Annals of
intensive care, 2(1), 1-10.
Faezipour, M., Ferreira, S. 2011. Applying systems
thinking to assess sustainability in healthcare system
of systems. International Journal of System of Systems
Engineering, 2(4), 290-308.
Fialho, A. S., Oliveira, M. D., Sá, A. B. 2011.Using
discrete event simulation to compare the performance
of family health unit and primary health care centre
organizational models in Portugal. BMC health
services research,11(1), 274.
Fildes R., Ranyard, J.C. 1997.Success and Survival of
Operational Research Groups – A Review. Journal of
the Operational Research Society 48 (4): 336-360.
Fone, D., Hollinghurst, S., Temple, M., Round, A., Lester,
N., Weightman, A., et al. 2003. Systematic review of
the use and value of computer simulation modelling in
population health and health care delivery. J Public
Health, 25(4):325-335.
Forsberg, H. H., Aronsson, H., Keller, C., Lindblad, S.
2011. Managing health care decisions and
improvement through simulation modeling. Quality
Management in Healthcare, 20(1), 15-29.
Geranmayeh, S., Iyer, A. S. 2008. Capacity Analysis of
Critical Hospital Resources Using System Dynamics
Approach. Unpublished Manuscript.
Griffin, J., Xia, S., Peng, S., Keskinocak, P.
2012.Improving patient flow in an obstetric unit.
Health care management science, 15(1), 1-14.
Guizzardi, G., Wagner, G. 2012.Tutorial: Conceptual
simulation modeling with Onto-UML. In Simulation
Conference (WSC), Proceedings of the 2012 Winter
(pp. 1-15). IEEE.
Günal, M. M., Pidd, M. 2010.Discrete event simulation for
performance modelling in health care: a review of the
literature. Journal of Simulation, 4(1), 42-51.
Hafner, T., Shiffman, J. 2013.The emergence of global
attention to health systems strengthening. Health
policy and planning, 28(1), 41-50.
Hilton, N. A. 2001.Exploration into the behavior of
cardiac waiting lists (Doctoral dissertation, University
of Southampton).
Hirsch, G., Homer, J., Milstein, B., Scherrer, L., Ingersoll,
C., Landy, L., Fisher, E. 2012.ReThink Health
Dynamics: Understanding and influencing local health
system change. In 30th International Conference of
the System Dynamics Society, St. Gallen, Switzerland.
Homer, J., Jones, A., Seville, D., Essien, J., Milstein, B.,
Murphy, D. 2004.The CDC's diabetes systems
modeling project: Developing a new tool for chronic
disease prevention and control. In 22nd International
Conference of the System Dynamics Society, pp. 25-
29.
Hosking, M., Roberts, S., Uzsoy, R., Joseph, T. M.
2013.Investigating interventions for increasing
colorectal cancer screening: Insights from a simulation
model. Socio-Economic Planning Sciences, 47(2),
142-155.
Hsiao, C. T., Huang, H. H. 2012.A causal model for the
development of long-term facilities: a case in Taiwan.
Quality & Quantity, 46(2), 471-481.
Jahangirian, M., Eldabi, T., Naseer, A., Stergioulas, L. K.,
Young, T. 2010.Simulation in manufacturing and
business: A review. European Journal of Operational
Research, 203(1), 1-13.
Jeffrey, P., Seaton, R. 1995.The Use of Operational
Research Tools: A Survey of Operational Research
Practitioners in the UK. Journal of the Operational
Research Society 46 (7): 797-808.
Jun J.B., Jacobson S.H., Swisher J.R. 1999.Application of
discrete-event simulation in health care clinics: A
survey. J Oper Res Soc, 50:109-123.
Kadri F., Chaabane S., Tahon C. 2014. Simulation-based
decision support system to pre-vent and predict strain
situations in emergency department systems.
Simulation Modelling Practice and Theory, 42, 32–52.
Kuhl, M. E. 2012.A simulation study of patient flow for
day of surgery admission. In Simulation Conference
(WSC) Proceedings of the 2012 Winter (pp. 1-7).
IEEE.
Lane, D. C., Monefeldt, C., Rosenhead, J. V.
2000.Looking in the wrong place for healthcare
improvements: A system dynamics study of an
accident and emergency department. Journal of the
operational Research Society, 518-531.
Lattimer, V., Brailsford, S., Turnbull, J., Tarnaras, P.,
AReviewonDiscrete-eventSimulationandSystemDynamicsStudiesforHealthcareProblems
301

Smith, H., George, S., Maslin-Prothero, S.
2004.Reviewing emergency care systems I: insights
from system dynamics modelling. Emergency
Medicine Journal, 21(6), 685-691.
Lubyansky A. A system dynamics model of health care
surge capacity. Proceedings of the 23rd International
Conference of the System Dynamics Society, Boston,
MA (2005).
Marjamaa, R., Torkki, P., Hirvensalo, E., and O. Kirvelä.
2009. What is the Best Workflow for an Operating
Room? A Simulation Study of Five Scenarios, Health
Care Management Science, 12(2), 142 -146.
Merrill, J. A., Deegan, M., Wilson, R. V., Kaushal, R.,
Fredericks, K. 2013.A system dy-namics evaluation
model: implementation of health information
exchange for public health reporting. Journal of the
American Medical Informatics Association.
Mittal, S. 2013.Emergence in stigmergic and complex
adaptive systems: A formal discrete event systems
perspective. Cognitive Systems Research, 21, 22-39.
Rado, O., Lupia, B., Leung, J.M.Y., Kuo, Y.-H., Graham,
C.A. 2014.Using Simulation to Analyze Patient Flows
in a Hospital Emergency Department in Hong Kong.
Springer Proceedings in Mathematics and Statistics
61, 289-301.
Ramwadhdoebe, S., Buskens, E., Sakkers, RJB., Stah,l JE.
2009.A tutorial on discrete event simulation for health
policy design and decision making: Optimizing
pediatric ultrasound screening for hip dysplasia as an
illustration. Health Policy, 93:143-150.
Rauner, M. S. 2002.Using simulation for AIDS policy
modeling: benefits for HIV/AIDS prevention policy
makers in Vienna, Austria. Health Care Management
Science, 5(2), 121-134.
Rwashana, A. S., Nakubulwa, S., Nakakeeto-Kijjambu,
M., Adam, T. 2014.Advancing the application of
systems thinking in health: understanding the
dynamics of neonatal mortality in Uganda. Health
Research Policy and Systems, 12(1), 36.
Steins, K., Persson, F., Holmer, M. 2010. Increasing
utilization in a hospital operating de-partment using
simulation modeling. Simulation, 86(8-9), 463-480.
Sterman, J. D. 2006.Learning from evidence in a complex
world. American journal of public health, 96(3), 505-
514.
Townshend, J. R. P., Turner, H. S. 2000. Analysing the
effectiveness of Chlamydia screening. Journal of the
Operational Research Society, 812-824.
Wu, M. H., Yu, J. Y., Huang, C. H. 2013.Theoretical
System Dynamics Modeling for Taiwan Pediatric
Workforce in an Era of National Health Insurance and
Low Birth Rates. Pediatrics & Neonatology, 54(6),
389-396.
Zulkepli, J., Eldabi, T., Mustafee, N. 2012.Hybrid
simulation for modelling large systems: an example of
integrated care model. In Simulation Conference
(WSC), Proceedings of the 2012 Winter (pp. 1-12).
IEEE.
SIMULTECH2015-5thInternationalConferenceonSimulationandModelingMethodologies,Technologiesand
Applications
302
