Knowledge Management Problems in Paediatrics and Paediatrics
Neurology Departments
A Case Study based on the Grounded Theory
Helvi Nyerwanire
1
, Erja Mustonen-Ollila
1
, Antti Valpas
2
and Jukka Heikkonen
3
1
Innovation and Software, Lappeenranta University of Technology, Lappeenranta, Finland
2
Department of Obstetrics and Gynaecology, South Karelia Social and Health Care District, Lappeenranta, Finland
3
Department of Information Technology, University of Turku, Turku, Finland
Keywords: Knowledge Management, Healthcare, Empirical Research, Case Study, Grounded Theory.
Abstract: Knowledge management means how information communication technology systems and intellectual
human capital is applied to support knowledge creation, as well as in the capturing, organization, access,
and use of an organization’s intellectual capital. This paper investigates knowledge management problems
in paediatric and paediatric neurology departments. The Grounded Theory approach is applied in data
collection and analysis. The analysis revealed 8 thematic categories as follows: Patient, Physician, Patient
Data, Nurse, ICT Systems, Patient Treatment, Diagnosis, and Learning and Experience. The categories are
related to each other, and we found 13 higher levels of abstraction of statements. A conceptual framework
of knowledge management categories, their relationships to each other, and propositions to our categories
was developed by using the Grounded Theory approach. The relationships between the knowledge
management categories enhance confidence in the validity of the categories and their relationships, and
expand the emerging theory.
1 INTRODUCTION
In this study the healthcare environment, denoted as
department, is referred to as a place in which
medical, clinical and nursing knowledge is ingrained
in practitioners (Räisänen et al., 2009). Knowledge
management is defined as a process where
information communication technology (ICT)
systems are applied to support the activities in
organizing knowledge, expertise, skills and
communication (Alavi and Leidner, 2001). In spite
of the definition above, there are several problems
that hamper knowledge management, such as the use
of ICT systems (Viitanen et al., 2011; Martikainen et
al., 2012; Nykänen et al., 2012), access to patient
data (Reddy et al., 2009), communication barriers
(Hayes et al., 2011), resources and workload (Chadi,
2009), acute and emergency patient care situations
(Nevalainen et al., 2012), coordination inside and
outside the hospital (Burgess et al., 2012),
appointment scheduling (Martikainen et al., 2012),
treatment paths (Viitanen et al., 2011; Nykänen et
al., 2012), diagnosis (Heilmann, 2010), and
interpretation of patient data and information
interpretation (Viitanen et al., 2011; Martikainen et
al., 2012; Nykänen et al., 2012).
Thus, plenty of knowledge management
problems exist in healthcare, but studies are missing
from the paediatrics and paediatrics neurology area
how improved healthcare quality, lowered
healthcare costs, care providers’ ability to offer
healthcare, changes in the process of patient care
delivery and improved cost efficiency by offering
new ICT technologies by remote access with the
patient can bring improvements to healthcare
environment. Therefore we have applied past studies
and empirical evidence to carry out a qualitative in-
depth case study (Benbasat et al., 1987; Yin, 2003)
that identifies problems in knowledge management
in two hospital environments. We analyzed the
collected data with the Grounded Theory (GT)
approach by using Glaser and Strauss’s (1967) and
Pawluch and Neiterman’s (2010) research approach.
GT investigates phenomena in their natural context
and a data analysis is used to build up a theory from
empirical findings. Data collection continues until
‘theoretical saturation’ is reached (Glaser and
234
Nyerwanire, H., Mustonen-Ollila, E., Valpas, A. and Heikkonen, J..
Knowledge Management Problems in Paediatrics and Paediatrics Neurology Departments - A Case Study based on the Grounded Theory.
In Proceedings of the 7th International Joint Conference on Knowledge Discovery, Knowledge Engineering and Knowledge Management (IC3K 2015) - Volume 3: KMIS, pages 234-241
ISBN: 978-989-758-158-8
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Strauss, 1967). Our goal was to investigate
knowledge management problems in detail in a
paediatric department and paediatric neurology
department in a central hospital located in South
Karelia, Finland, and we found 401 knowledge
management observations supported by empirical
evidence. We categorized the observations with GT
analysis (Glaser and Strauss, 1967), and the analysis
revealed 8 thematic categories as follows: patient (2
observations), physician (83 observations), nurse (10
observations), patient data (61 observations), ICT
systems (147 observations), patient treatment (57
observations), diagnosis (16 observations), and
learning and experience (21 observations). The rest
of the paper is structured as follows. Section two
describes related research, section three presents the
research method, and section four outlines the data
analysis. Finally, section five contains conclusions
and discussion.
2 RELATED RESEARCH
Plenty of knowledge management problems have
been presented in the literature. They include for
example difficulties in making a diagnosis (Tucker,
2007) and difficulties in clinical investigations,
because investigations need a lot of time, experience
and knowledge (Curley et al. 1990). There is lack of
access to medical information journals (Norbert and
Lwoga, 2013), and lack of access to patient
information (Reddy et al., 2009). Reddy et al. (2009)
state that there is a communication barrier in ICT
systems in healthcare environments. In addition, the
oral information received from a patient is not clear
and the physicians can freeze in critical patient care
situations (Heilmann, 2010). Martikainen et al.
(2012) mention appointment scheduling and
consultation problems. According to Burgess et al.
(2012), there are coordination problems between
different caregivers. Mandl et al. (2001) state that
patient rights and parents’ permission complicate
physicians’ work. Martikainen et al. (2012) refer to
problems in ICT outcomes in patient work, as well
as physicians’ negative attitudes to ICT systems or
to patients (Viitanen et al., 2011). Chadi (2009)
mentions physicians' limited time and too many
patients. Nykänen et al. (2012) state that there is lack
of reliability of data or information. Dias et al.
(2003) argue that physicians' work is stressful, such
as late night working, many patients, or patient care
cases. Martikainen et al. (2012) claim that separate
subsystems need separate checking and each patient
must be treated differently, and physicians are not
too eager to search for follow-up data. There is
malfunction in lab tests, subsystems and procedures
(Viitanen et al., 2011). A lot of time is needed to
give information to the patient, and making a
rehabilitation plan needs a group of people from
different areas (Poskiparta et al., 2000). Brixey et al.
(2010) mention interruptions in daily work. Thus,
despite a growing interest in knowledge
management problems in healthcare, their
relationships have not been recognized in the
literature. Our study aims to respond to this lack of
studies and to provide useful information of
knowledge management in one specific paediatric
department and one paediatric neurology
department. Paediatrics carries out medical care of
children and paediatrics neurology carries out
medical care which specializes in treating nervous
system problems in children. The nervous systems
can be damaged permanently because the brain’s
development, and making the diagnosis and
treatment of neurological problems need a special
attention. The children’s diseases also need special
knowledge in order to be treated properly. Thus, this
study could bring benefits both to the patients and
care givers in this research context by discovering
what are the main knowledge management problems
and their relationships with each other. Based on
past studies, we have formulated the following
research questions:
RQ1: What are the main knowledge management
problems in paediatrics and paediatrics neurology?
RQ2: How are the knowledge management
problems in paediatrics and paediatrics neurology
related to each other?
3 RESEARCH METHOD
This study utilizes both qualitative and quantitative
research processes and theory building approaches.
It takes an in-depth case study, theory building and
Grounded Theory (GT) perspective involving
specific healthcare environments in which
knowledge management problems are studied
(Glaser and Strauss, 1967; Benbasat et al., 1987;
Eisenhard, 1989; Yin, 2003; Cresswell, 2007;
Pawluch and Neiterman, 2010). In these healthcare
environments, the cases were selected so that they
would either predict similar outcomes (i.e. literal
replication) or to produce contrasting results but for
predictable reasons (i.e. theoretical replication) (Yin,
2003). Theory triangulation was applied by
interpreting a single data set from multiple
perspectives to understand the research problems
Knowledge Management Problems in Paediatrics and Paediatrics Neurology Departments - A Case Study based on the Grounded Theory
235
(Denzin, 1978). The concepts and their relationships
were validated with the grounded theory approach
(Glaser and Strauss, 1967; Eisenhardt, 1989). During
the research, theoretical background knowledge was
gained, which increased the credibility of the study
(Miles and Huberman, 1994). According to
Eisenhardt (1989), the combination of case study
with the grounded theory approach has three major
strengths: it produces a novel theory, the emergent
theory is testable, and the resultant theory is
empirically valid. In the GT approach the theory
emerges from the data. According to Glaser and
Strauss (1967), there is no need to review any
literature of the studied area before entering the
field, and this is in line with our research.
Specifically, each interview transcript was analysed,
and major emergent themes and concepts were
identified in order to form similar categories (Myers
and Avison, 2002). In our case study, one paediatric
department and one paediatric neurology department
were the units of analysis in the Social and Health
Care District of South Karelia in Finland and its
central hospital (Eksote, 2013).
The definitions of knowledge management and
the objectives of the research formed the basis for
the interviews and data collection. In order to
address the research questions, we conducted nine
audio-recorded unstructured and semi-structured
interviews that investigated experiences in
knowledge management issues in the chosen
healthcare environment. The interview rounds were
carried out in March - May 2014 in the Paediatric
department, and in March - June 2014 in the
Paediatric Neurology department. The interviewees
were the chief physician in paediatrics neurology,
chief physician in paediatrics, one senior physician
in paediatrics, three junior physicians in paediatrics,
and three paediatric nurses. The interviewees had
been involved in many knowledge management
issues and processes in their own fields of expertise
during their working careers that extended over
periods of 6 to 14 years among the nurses and 3 to
43 years among the physicians, in different positions
either in South Karelia Social and Health Care
District or other healthcare environments in the
private or public sector in Finland.
3.1 Data Collection and Categorization
The interviews included frequent elaboration and
clarification of the meanings and terms, they were
audio-recorded, and the recordings were transcribed,
yielding over 206 pages of transcripts. After
transcribing the interviews, we used the Grounded
Theory based on our own intuition and knowledge in
fragmenting and reassembling our knowledge
management problems into thematic categories
(Glaser and Strauss, 1967; Pawluch and Neiterman,
2010) according to relevant terminology and past
studies that were the most refereed work in
categorizing concepts in the studied research area.
Since each thematic category was decomposed into
multiple items (traits) by using content analysis, the
items were matched with actual categories (in situ).
Thus, for each category a certain number of items
were identified that were likely to influence the
category at that point. Finally, the items were
validated with past studies. An example of each of
the thematic categories’ observation is presented in
Table 1. The problem with the thematic categories
was whether there would be enough proof found in
the data to derive the categories as valid and reliable,
and whether the categories discovered in the data
would be the correct ones.
4 ANALYSIS
After creating the chain of evidence in data
categorization, the total number of 401 different
empirical observations under 8 thematic categories
(see Table 1) were found by using Glaser and
Strauss’s (1967) and Pawluch and Neiterman’s
(2010) grounded theory analysis instructions, which
support the finding of categories grounded on data,
and also based on the researchers’ own intuition and
knowledge. Specifically, we have involved
fragmentation and reassembled our data into
thematic categories by trying to capture a broader
social system of ideas from the experience of the
social actors (Glaser and Strauss, 1967; Pawluch and
Neiterman, 2010), in this case the actors working in
the paediatrics and paediatrics neurology
departments. As shown in Table 1 above, eight
thematic categories were formed in the study:
Patient, Physician, Nurse, Patient Data, ICT
Systems, Patient Treatment, Diagnosis, and
Learning and Experience. The Patient category had
2 observations and 1 item; the Physician category 83
observations and 21 items; the Nurse category 10
observations and 7 items; the Patient Data category
61 observations and 14 items; the ICT Systems
category 147 observations and 17 items; the Patient
Treatment category 57 observations and 16 items;
and the Learning and Experience category had 21
observations and 6 items. The sum total of empirical
item observations (items) was 401, and the sum total
of different items was 88. Our conceptual
KMIS 2015 - 7th International Conference on Knowledge Management and Information Sharing
236

Table 1: An example of an observation concerning each thematic category, category definition, item number (item no),
item, and item definition.
Thematic
Category
Category Definition Item
No
Item Item Definition
Patient A patient receives care and
treatment by a physician or
nurse
1 Patient
anxiety
In patient care situations the patients can be
sometimes afraid and the patient’s worry about
him/herself affects the physician’s decision-
making (in diagnosis and treatments).
Physician A physician needs
knowledge of anatomy,
physiology, and medical
science, as well as
knowledge of how to apply
this knowledge in practice
1 Negative
attitudes
towards ICT
systems
There are negative attitudes because computer
programs are a hindrance to work and
subsystems are used via main systems, and
physicians are very anxious about using systems
this way.
Nurse A nurse is a trained nurse
specialized in patients'
(children) illnesses
1 Interruptions There are a lot of interruptions in daily work and
they make the nurse to forget what she/he was
doing, and also patients interrupt working in data
saving etc. issues.
Patient data Patient’s personal data,
medical history, treatments,
tests, examinations,
diagnoses, and consultation
requests
1 Information is
missing in the
systems,
paediatric
ward and
about patients
The systems miss task lists for staff, paper
information about patients is missing, check-up
lists are missing in the paediatrics ward,
instructions on how to handle double time data
saving and checking are missing, and acute
treatment guideline books must be available.
ICT
Systems
There are hundreds of ICT
systems in use at hospitals,
and the physicians and
other professionals use
them in their daily work
with patients.
1 Systems are
not in concord
The electronic prescription does not recognize
the treatment. The patient has a third system at
home, and in the university there is a fourth one
and none of these are totally in concord.
Patient
treatment
In the patient care process a
physician makes a
diagnostic decision and
determines the proper
treatment for the patient.
1 Treatment
based on
'Käypähoito'
does not work
In some clinical situations the treatment based
on 'Käypähoito' does not work and it is more
complicated to find the exact treatment strategies
from journal sources.
Diagnosis A process to examine the
patient s and define the
essence and circumstances
of a disease
1 No check-up
patient
information in
wards and
paediatrics
There are no check-up lists in wards and
paediatrics, check-up lists or staff used at the
wards do not exist in the systems.
Learning
and
experience
Acting to get new
knowledge or skills by
experience or reading, or
evaluating information or
data
1 New
information
or data need
studying,
evaluation
and critical
thinking
The biggest problem is that medicine is such a
huge concept, it has huge amount of information
that cannot all be remembered, and new
information needs to be studied or new results
must be waited for.
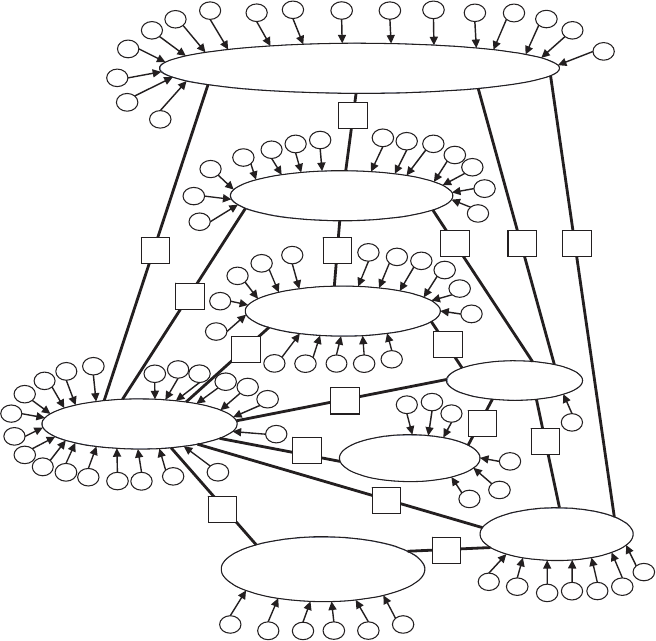
framework of the discovered categories (see Figure
1 below) is grounded on empirical evidence and
theories reflecting the findings in the field (Glaser
and Strauss, 1967; Pawluch and Neiterman, 2010).
In Figure 1, the categories are shown as ellipses, and
the bold lines marked with letters (A to O) describe
the relationships between the categories. The small
arrows with numbered circles pointing to the
categories are the multiple items (traits) to each
category composed by content analysis. After the
categories and relationships and items had been
found, we determined the properties of the
categories and propositions (hypotheses) on how the
categories were related on the basis of data (See
Table 2). Constant comparison between the data and
concepts in past studies in order to accumulate
Knowledge Management Problems in Paediatrics and Paediatrics Neurology Departments - A Case Study based on the Grounded Theory
237
evidence convergence on simple and well-defined
categories led us to 13 higher level of abstraction of
statements about the relationships between the
categories. This theorizing was in line with Pawluch
and Neiterman’s (2010) suggestions of creating a
grounded theory with Glaser and Strauss’s (1967)
approach.
5 CONCLUSIONS AND
DISCUSSION
The qualitative, empirical case study based on the
Grounded Theory approach (Glaser and Strauss,
1967) and nine in-depth interviews revealed that
many knowledge management problems can be
found in paediatric and paediatric neurology
department.
The study is in line with past studies concerning
problems in making diagnoses (Tucker, 2007), hard
clinical investigations (Curley et al., 1990), lack of
access to medical information journals (Norbert and
Lwoga, 2013), lack of access to patient information
and communication barriers in ICT systems (Reddy
et al., 2009), unclear oral information from a patient,
physicians freezing in emergency situations
(Heilmann, 2010), appointment scheduling and
consultation problems (Martikainen et al., 2012),
coordination problems between caregivers (Burgess
et al., 2012), patient rights and parents’ permissions
complicating physicians’ work (Mandl et al., 2001),
problems in ITC outcomes, physicians’ negative
attitudes to ICT systems and patients (Martikainen et
al., 2012; Viitanen et al., 2011), physicians limited
time with too many patients (Chadi, 2009), lack of
data reliability (Nykänen et al., 2012), physicians’
stress (Dias et al., 2003), systems needing double
checking, physicians’ not wanting to search for
follow-up data (Martikainen et al., (2012),
malfunctions in lab tests, subsystems and procedures
(Viitanen et al., 2011), long time needed to give
information to the patient and making a
rehabilitation plan needing a group of people from
different areas (Poskiparta et al., 2000), and
interruptions in daily work (Brixey et al., 2010).
Our results validated the conceptual framework,
Figure 1: Conceptual framework of categories.
Learning and
experience
ICT Systems
Nurse
Patient
Diagnosis
1
1
0
9
2
1
17
16
1
5
8
7
6
3
4
5
141
3
12
11
Patient Data
7
14
13
12
11
6
5
4
1
2
3
1
0
9
8
Patient Treatment
6
10
4
16
1
5
14
9
8
5
1
2
3
1
3
12
11
7
Physician
21
1
12
1
3
14
1
5
1
6
2
3
4
7
6
5
1
7
1
8
1
9
2
0
8
9
10
11
1
2 6
5
4
3
7
6
5
4
3
1
2
6
5
4
3
2
1
H
I
N
M L
O
J
G
D
C
A
B
E
K
F
P
KMIS 2015 - 7th International Conference on Knowledge Management and Information Sharing
238
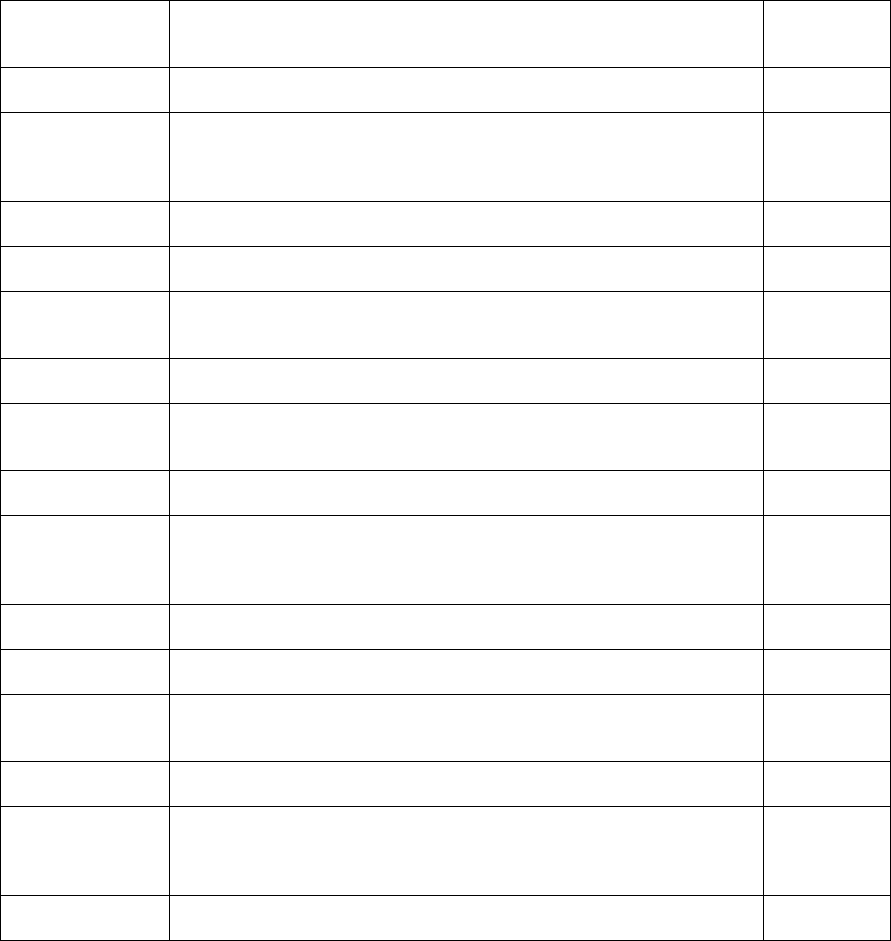
Table 2: Properties of categories and propositions (hypotheses) on how the categories are related on the basis of the data.
Category/Categories Properties of categories and propositions (hypotheses) on how the categories
are related (lines marked with the letters A to O in Figure 1) on the basis of the
data
Lines marked
with letters in
Figure 1
Physician, Learning
and Experience
The staff make harsh comments about the patients, parents, colleagues, even
themselves, and expertise is shared this way
A
Nurse, Learning and
Experience
Nurses look for evidence on how a medicine has helped elsewhere, and nurses
contact outside hospitals in Finland and find out how a certain disease is
treated or medicine is used, and then the department makes its own guidelines
on how to use it.
B
Nurse, Physician The nurses must decide who is the best physician to decide about new
medication
C
Physician,
Diagnosis
A diagnosis has to be done even if the patients denies to give samples of blood
or urine, and it is difficult to treat children if they refuse the tests
D
Diagnosis, Patient In patient care situations patients can be sometimes afraid and the patient’s
worry about him/herself affects the physician’s decision-making (in diagnosis
and treatments)
E
Patient, Nurse The nurses are checking the child patients before they meet the physician, and
the physician then checks the same things again
F
Patient, Physician A lot of time is used to give information about the disease, how it affects the
patient, and about the medicine in order to make sure that the patients takes the
medicine and follows the instructions at home
G
Physician, ICT
Systems
The physicians have only very basic knowledge of data systems H
Physician, Patient
Data
The diagnosis must be formed in one's mind on the basis of the symptoms. The
physician must react to the things she/he is expecting, such as results, and the
physician must decide him or herself and on the basis of information in the
computer
I
Physician, Patient
Treatment
In acute situations investigations and treatments must be handled quickly,
decisions must be made quickly, and handling acute situations is difficult.
J
Patient Treatment,
Patient
The problem is every treatment cannot be evidence-based because there is not
enough research and there are cases which cannot be based on a proper study.
K
Patient Data, Patient It is not easy to combine patient information from different sources and people,
and too much patient information can be controversial, and one must form
one's own opinion about it
L
ICT Systems,
Patient
The information systems slow down patient work, take time from daily patient
care and take the focus away from the patient
M
Patient Data, ICT
Systems
It is difficult to know what is the fastest way to find information, sometimes
one cannot use one's personal codes, one has to use the clinical codes of the
whole clinic to find something and things are not found from one system, but
in Effica and subsystems.
N
Patient Treatment,
Patient Data
In an emergency situation, electricity failure is crucial because there is not
access to patient data
O
which became the discovered theory for the
phenomenon. The data which confirmed the
emergent relationships enhanced confidence in the
validity of the relationships. The past studies with
similar findings were important because they tied
together the underlying similarities in phenomena
not associated with each other, and stronger internal
validity was achieved.
Several conclusions can be drawn from this
study. First, there is a huge number of knowledge
management problems which affect patient care
work daily. There is a real difference between acute
and emergency situations and normal daily routine
patient care situations. The first ones need a lot of
experience and knowledge which must be learned in
similar situations in a long time period. Therefore, a
junior physician must not be in charge in acute and
emergency situations but should work side by side
with a senior physician in order to learn the right
procedures. The management, leadership, and
treatment paths are important tasks to be solved in
departments in every situation before any patient is
Knowledge Management Problems in Paediatrics and Paediatrics Neurology Departments - A Case Study based on the Grounded Theory
239
involved, so that the interpretation of results and
tests will go right away to the right person who is
able to interpret them correctly. The several similar
investigations by different patient care providers
must be coordinated so that there is no need to do
the same investigations all over again when the care
giver changes. Physicians and nurses on every level
of healthcare must be given proper education and
training so that patients can rely on them in spite of
who is in charge. When doing so, maybe the patients
would also start telling the truth about their
symptoms. The patients could also tell about all their
symptoms better if they could rely on the
confidentiality of the ICT systems, so that cannot
misused by anyone else than the physician in charge.
Finally, the physicians' and nurses' negative attitude
problems towards ICT systems and child patients
must also be taken care of because they can affect
the patient care situation, and also the care providers
themselves. The reasons for the knowledge
management problems may just be too much work
with too many patients with limited knowledge at
hand, which makes the care providers tired,
frustrated or exhausted in their work. On the other
hand, they can also be a consequence of motivation
problems, or missing right knowledge in the work
they are currently doing. This can be seen as
uncertainty in their work, which is full of restrictions
and perhaps a feeling that there is no possibility to
influence one's own work, but it is dictated from
above.
There are several limitations in this study. First,
the results may not be readily applicable to other
departments, as the phenomena were atypical.
Second, the use of only two departments in a central
hospital affected our findings, and thus
generalization of the results can be difficult, but not
necessarily impossible. Third, we performed a
limited number of interviews, and only the chief
physician of the paediatrics neurology department
was interviewed personally. Our analysis provided
better understanding of the different types of
knowledge management problems and their
relationships with each other affecting to patient
safety which lead to better understanding of
problems in healthcare. This is the main research
contribution of our study. Finally, our study was
supported with a study conducted in medical domain
(de la Tassa et al., 2013) concerning the importance
of patient safety and this supports our findings of
knowledge management problems.
REFERENCES
Alavi, M. and Leidner, D.E. (2001) ‘Review: Knowledge
Management and Knowledge Management Systems:
Conceptual Foundations and Research Issues’, MIS
Quarterly, vol. 25, no. 1, pp. 107-136.
Benbasat, I., Goldstein, D.K. and Mead, M. (1987) ‘The
Case Study Research Strategy in Studies of
Information Systems’, MIS Quarterly, vol. 11, no. 3,
pp. 369-386.
Brixey, J.J., Robinson, D.J., Turley, J.P. and Zhang, J.
(2010) ‘The roles of MDs and RNs as Initiators and
Recipients of Interruptions in Workflow‘,
International Journal of Medical Informatics, vol. 79,
no. 6, pp. 109-115.
Burgess, C., Cowie, L. and Gulliford, M. (2012) ‘Patients'
perceptions of error in long-term illness care:
qualitative study’, Journal of Health Services
Research and Policy, vol. 17, no. 3, pp. 181-187.
Chadi, N. (2009) ‘Medical Leadership: Doctors at the
Helm of Change‘, McGill Journal of Medicine, vol.12,
no. 1, pp. 52-57.
Creswell, J.W. (2007) Qualitative Inquiry and Research
Design: Choosing Among Five Approaches,
California: Sage Publications.
Curley, S. P., Connelly, D. P. and Rich, E. C. (1990)
‘Physicians' Use of Medical Knowledge Resources:
Preliminary Theoretical Framework and Findings‘,
Medical Decision Making, vol. 10, issue 4, pp. 231-
241.
de la Tassa, J., Martín, D., Fernández, E., Castro, M. and
Sánchez, G. (2013) ‘Survey on the Culture of Patient
Safety Among Spanish Health Care Residents‘,
American Journal of Medical Quality, pp. 1-9.
Denzin, N.K. (Ed.). (1978) The research act: A theoretical
introduction to sociological methods, New York:
McGraw-Hill.
Dias, L., Chabner, B. A., Lynch, T. J. and Penson, R. T.
(2003) ‘Breaking bad news: a patient’s perspective‘,
The Oncologist, vol. 8, pp. 587-596.
Eisenhardt, K.M. (1989) ‘Building Theories from Case
Study Research’, Academy of Management Review,
vol. 14, no. 4, pp. 532-550.
Eksote. (2013)’Etelä-Karjalan Sosiaali- ja Terveyspiiri’,
Available: http://www.eksote.fi/Fi/Eksote/Hallinto/
raportit/Documents/Terveydenhuollonjarjestamissuun
nitelma.pdf (10 November 2013).
Glaser, B. and Strauss, A.L. (1967) The Discovery of the
Grounded Theory: Strategies for Qualitative
Research, Chicago: Aldine.
Hayes, G.R., Lee, C.P. and Dourish, P. (2011)
‘Organizational routines, innovation, and flexibility:
The application of narrative networks to dynamic
workflow‘, International Journal of Medical
Informatics, vol. 80, no. 8, pp. e161-e177.
Heilmann, P. (2010) ‘To have and to hold: Personnel
shortage in a Finnish healthcare organization’,
Scandinavian Journal of Public Health, vol. 38, no. 5,
pp. 518-523.
Mandl, K.D., Szolovits, P., Kohane, I.S. (2001) ‘Public
KMIS 2015 - 7th International Conference on Knowledge Management and Information Sharing
240
standards and patients’ control: how to keep electronic
medical records accessible but private‘, British
Medical Journal, vol. 322, no. 7281, pp. 283–287.
Martikainen, S., Viitanen, J., Korpela, M. and Lääveri, T.
(2012) ’Physicians’ experiences of participation in
healthcare IT development in Finland: Willing but not
able’, International Journal of Medical Informatics,
vol. 81, no. 2, pp. 98–113.
Miles, M.B. and Huberman, A.M. (1994) Qualitative Data
analysis, Thousand Oaks, California: Sage
Publications.
Myers, M.D. and Avison, D.E. (ed.) (2002) Qualitative
Research in Information Systems: Review, London:
Sage Publications.
Nevalainen, M., Kuikka, L., Sjöberg, L., Eriksson, J. and
Pitkälä, K. (2012) ‘Tolerance of uncertainty and fears
of making mistakes among fifth-year medical students‘,
in Family Medicine, vol. 44, no. 4, pp. 240-246.
Norbert, G.L. and Lwoga, E.T. (2013) ‘Information
seeking behaviour of physicians in Tanzania‘,
Information Development, vol. 29, no, 2, pp. 172-182.
Nykänen, P., Kaipio, J. and Kuusisto, A. (2012)
’Evalution of the national nursing model and four
nursing documentation systems in Finland-Lessons
learned and directions for the Future’, International
Journal of Medical Informatics, vol. 81, no. 8, pp.
507–520.
Pawluch, D. and Neiterman, E. (2010) ‘What is Grounded
Theory and Where Does is Come from?’, in
Bourgeault A., Dingwall, R. and De Vries. R. (ed.)
The SAGE Handbook of Qualitative Methods in
Health Research, London: Sage Publications, pp. 174-
192.
Poskiparta, M., Kettunen, T. and Liimatainen, L. (2000)
‘Questioning and advising in health counselling:
results from a study of Finnish nurse counsellors’,
Health Education Journal, vol. 59, no. 1, pp. 69-89.
Reddy, M.C., Paul, S.A., Abraham, J., McNeese, M.,
DeFlitch C., and Yen, J. (2009) ‘Challenges to
effective crisis management: Using information and
communication technologies to coordinate emergency
medical services and emergency department teams’,
International Journal of Medical Informatics, vol. 78,
no. 4, pp. 259–269.
Räisänen, T., Oinas-Kukkonen, H., Leiviskä, K.,
Seppänen, M. and Kallio, M. (2009) ’Managing
Mobile Healthcare Knowledge: Physicians'
Perceptions on Knowledge Creation and Reuse’, in
Olla, P. and Tan, J. (ed.) Mobile Health Solutions for
Biomedical Applications, New York, New Hersey: IGI
Global, pp. 111-127.
Tucker, L. B. (2007) ‘Review: Making the diagnosis of
systemic lupus erythematosus in children and
adolescents, ’ Lupus, vol. 16, no. 8, pp. 546-549.
Viitanen, J., Hyppönen, H., Lääveri, T., Vänskä, J.,
Reponen, J. and Winblad, I. (2011) ’Nationality
questionnaire study on clinical ICT systems proofs:
Physicians suffer from poor usability’, International
Journal of Medical Informatics, vol. 80, no. 10, pp.
708-725.
Yin, R.K. (2003) Case study research: design and
methods, California: Sage Publications.
Knowledge Management Problems in Paediatrics and Paediatrics Neurology Departments - A Case Study based on the Grounded Theory
241
