Reliability of a Screening Tool to Prevent Running Injuries
The RunningSmart Tool
Justien Cornelis
1
, Rudi Frankinouille
1,2
, Filip Stremersch
1
, Stig Vaerewijck
1
and Dirk Vissers
1
1
Department of Rehabilitation Sciences and Physiotherapy, University of Antwerp, Universiteitsplein 1, Wilrijk, Belgium
2
Department of S.P.O.R.T.S, Antwerp University Hospital, Wilrijkstraat 10, Edegem, Belgium
Keywords: Screening Tool, Running Injuries, Prevention, Reliability.
Abstract: The goal of this research was to assess inter- and intra-rater reliability of the RunningSmart screening tool,
developed to determine weak-links at baseline in novice, recreational and athlete runners. The tool provides
a selection of exercises targeting the identified weak-links. Overall, the tool had a fair to good inter- and
intra-rater reliability for the separate clinical tests based on the kappa value. The RunningSmart Tool
focusses mainly on recreational runners or people that initiate running. Therefore the tool is designed in a
practical and easy to apply way that can be used in a clinical setting. These data indicate that the
RunningSmart Screening tool can be confidently applied by trained individuals and used to assess the
movement patterns of recreational start-to-runners in order to make decisions related to interventions to
decline the injury risk and enhance physical activity.
1 OBJECTIVES
In the last decade, running gained popularity as a
readily accessible recreational sport and leisure. It is
estimated that 10%-20% of Americans run regularly
as it is considered to be the most efficient way to
achieve fitness (Fields et al., 2010).
In Belgium, many novice untrained runners
participate in a start-to-run program in an attempt to
resume physical activity. It is a 10 weeks
programme that should be continued after. However,
a drop-out of 31,5% was reported after 10 weeks.
Moreover, 40% of the participants reported an injury
(Cloes and Pétré, 2012).
An injury due to running is a capital reason to
renounce a running program. In literature, incidence
rates of 19,4% to 79,3% were reported (van Gent et
al., 2007).
In a healthy active adult population the most
frequently reported lower extremity injuries were
hamstring strain, anterior cruciate ligament injury,
Achilles tendon pathology and ankle sprain (Zazulak
et al., 2007). Authors state that a previous injury is
the greatest risk factor for future injury caused by
changes in proprioception, decreased mobility,
increased flexibility, etc.(Fulton et al., 2014) These
biomechanical factors are modifiable in order to
decrease the initial risk on an injury.
General biomechanical screening tools such as
the Functional Movement Screen (Minick et al.,
2010, Teyhen DS, 2012) and the Nine-test Screening
Battery (Frohm et al., 2012) were suggested in
literature and were stated to be reliable. However,
these tools were developed to screen athletes.
RunningSmart is a new clinical and
biomechanical screening tool developed to
determine individual weak-links at baseline in
novice, recreational and athlete runners. Based on
the outcome of the screening, the tool provides a
selection of exercises targeting those identified
weak-links in order to reduce the drop-out ratio. The
aim of this study was to assess the inter- and intra-
rater reliability of the RunningSmart tool.
2 METHODS
2.1 Description of the Tool
A questionnaire was implemented in order to screen
for exercise limiting pathologies.
The screening tests for running injuries described
Cornelis, J., Frankinouille, R., Stremersch, F., Vaerewijck, S. and Vissers, D..
Reliability of a Screening Tool to Prevent Running Injuries - The RunningSmart Tool.
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
in the tool are scientifically grounded universal
clinical tests to investigate biomechanical and
musculoskeletal disorders. An overview of these test
is given in Table 1.
Table 1: Overview of the implemented clinical tests.
Test 1 Inspection and Palpation
Test 2 Single Leg Squat
Test 3 Single Leg Jump
Test 4 Single Leg Heel Raise
Test 5 Foot Mobility
Test 6 M. Gluteus Medius Strength
Test 7 Mm. Hamstrings Length
Test 8 Abdominal Strength
Test 9 Mm. Hamstrings or Mm. Glutei
Dominance
Test 10 Mm. Quadriceps Length
Test 11 Bridging
Test 12 Iliotibial Tractus Length
Test 13 Hip Mobility
2.2 Protocol
Eligibility criteria for the subjects were (1) 18-25
years old, (2) healthy, (3) BMI 18,5-24,9 kg/m²
(male) or 17,5-23,9 kg/m² (female), (4) no
biomechanical physical injury in the past (5)
performed no severe physical activity 48 hours
before measurement, (6) not pregnant.
Both raters (A and B) were physiotherapists and
had the same clinical experience and education.
At first, participants were tested randomly by
assessor A or B, immediately followed by a retest
(the other assessor) to compare inter-rater reliability.
After seven days, all participants were tested
again by assessor B to compare intra-rater reliability.
The outcome of the movement evaluation
criterion for each test was evaluated by three
categorical observational possibilities e.g. “yes”,
“no” or “more or less”.
The ethics committee of the University Hospital
in Antwerp approved the trial, and a written
informed consent was obtained for each participant.
2.3 Statistical Analysis
The reliability of the overall final score was
evaluated using the Interclass Correlation
Coefficient (ICC) in SPSS 22.0 (Statistical Package
for the Social Sciences, IBM Corporation, NY,
USA).
The reliability of each clinical test was analysed
by the Cohen’s Kappa with a 95% Confidence
Interval (95%CI). Given the paradox of high
agreement and low Kappa values (Cicchetti and
Feinstein, 1990), the positive Proportion of
Agreement (PoA) and 95%CI was also calculated in
the Excel spreadsheet.
3 RESULTS
Twenty-nine participants met the afore mentioned
inclusion criteria (male (n=15; 22,8 kg/m²) and
female (n=14; 20,3 kg/m²)).
Overall ICC scores for inter- and intra-rater
reliability were 0.652 and 0.686 respectively.
The inter-rater and intra-rater reliability results
for the individual clinical tests, are listed in Table 2.
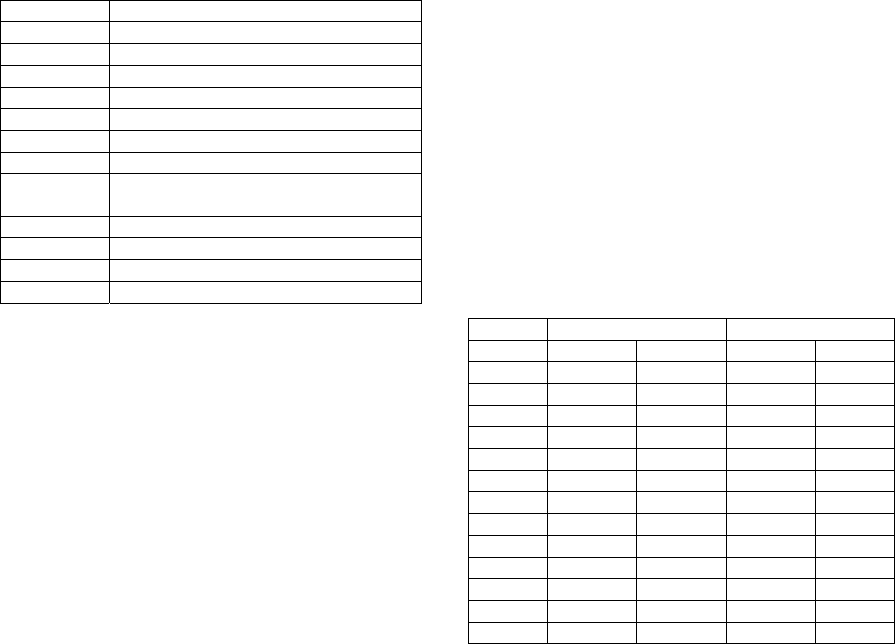
Table 2: Inter-rater and intra-rater reliability for the
different tests described by the Proportion of Agreement
(PoA) and Cohens’ Kappa.
Inter-rater Intra-rater
Test PoA Kappa PoA Kappa
1 0,741 0,381 0,862 0,585
2 0,483 0,193 0,776 0,293
3 0,707 0,266 0,776 0,267
4 0,759 0,425 0,707 0,239
5 0,793 0,491 0,793 0,555
6 0,759 0,100 0,690 0,385
7 0,845 0,691 0,879 0,753
8 0,931 0,164 0,828 0,328
9 0,672 0,367 0,690 0,204
10 0,793 0,430 0,776 0,510
11 0,828 0,253 0,810 0,230
12 0,931 0,558 0,879 0,294
13 0,879 0,734 0,810 0,460
4 DISCUSSION
The purpose of this study was to investigate the
inter- and intra-rater reliability of the RunningSmart
testing protocol, a new screening tool to assess weak
biomechanical links that could induce running
injuries in novice runners.
Overall, the tool had a
fair to good inter- and
intra-rater reliability (Rosner, 2010). The inter-rater
and intra-rater reliability for the separate clinical
tests based on the kappa value was average to good
(Altman, 1990). Moreover, the PoA was moderate to
excellent for inter-rater reliability and good to
excellent for intra-rater reliability.
Since the applied algorithm to obtain the final
score remains unclear e.g. different scores on
individual tests, it is assumed possible that a
different score on the subtests was obtained between
two assessors although the final score was the same.
This is the same limitation as reported in other
screening protocols (Teyhen et al., 2012). Creators
of these screening tools could provide researchers
more information about the score implementation.
The majority of the afore mentioned screening
protocols focus on athletes while the RunningSmart
Tool focusses mainly on recreational runners or
people that initiate running. Therefore the tool is
designed in a practical and easy to apply way that
can be used in a clinical setting.
The researchers in this study had the same
experience and educational level. Moreover, they
were trained as a RunningSmart Coach (two days
practical education), however their practical
experience as a therapist in a clinical setting was
limited. The clinicians tested individually and in
separate rooms. No video recordings were made.
The screening battery is easy to use for familiarized
professionals and requires minimal equipment.
The possible learning effect of the participants
was limited as the researcher did not give feedback
about the outcome.
Further research towards reliability and validity
of screening protocols to prevent running injuries is
mandatory. Moreover, randomized long-time
follow-up trials could be conducted to estimate the
incidence of running injuries in participants that
initiate running as the effect of the screening
protocol and proposed exercises could be evaluated.
These data indicate that the RunningSmart
Screening tool can be confidently applied by trained
individuals and used to assess the movement
patterns of recreational start-to-runners in order to
make decisions related to interventions to decline the
injury risk and enhance physical activity.
REFERENCES
Fields KB, Sykes JC, Walker KM, Jackson JC (2010)
Prevention of running injuries. Current sports
medicine reports 9 (3):176-182
Cloes M, Pétré B Characteristics Of Participants To'Start
To Run'Programme. Comparison Between
Maintenance And Drop Out Groups. In: Congrès
ICSEMIS 2012 «Sport… Inspiring a Learning
Legacy»(congrès scientifique Pré-Olympique), 2012.
van Gent BR, Siem DD, van Middelkoop M, van Os TA,
Bierma-Zeinstra SS, Koes BB (2007) Incidence and
determinants of lower extremity running injuries in
long distance runners: a systematic review. British
journal of sports medicine
Zazulak BT, Hewett TE, Reeves NP, Goldberg B,
Cholewicki J (2007) Deficits in neuromuscular control
of the trunk predict knee injury risk a prospective
biomechanical-epidemiologic study. The American
journal of sports medicine 35 (7):1123-1130
Fulton J, Wright K, Kelly M, Zebrosky B, Zanis M, Drvol
C, Butler R (2014) Injury risk is altered by previous
injury: a systematic review of the literature and
presentation of causative neuromuscular factors.
International journal of sports physical therapy 9
(5):583
Minick KI, Kiesel KB, Burton L, Taylor A, Plisky P,
Butler RJ (2010) Interrater reliability of the functional
movement screen. The Journal of Strength &
Conditioning Research 24 (2):479-486
Teyhen DS SS, Lorenson CL, Halfpap JP, Donofry DF,
Walker MJ, Dugan JL, Childs JD. (2012) The
Functional Movement Screen: a reliability study. J
Orthop Sports Phys Ther Jun;42(6):530-540
Frohm A, Heijne A, Kowalski J, Svensson P, Myklebust G
(2012) A ninetest screening battery for athletes: a
reliability study. Scandinavian journal of medicine &
science in sports 22 (3):306-315
Cicchetti DV, Feinstein AR (1990) High agreement but
low kappa: II. Resolving the paradoxes. Journal of
clinical epidemiology 43 (6):551-558
Rosner B (2010) Fundamentals of biostatistics. Cengage
Learning,
Altman DG (1990) Practical statistics for medical
research. CRC press,
Teyhen DS, Shaffer SW, Lorenson CL, Halfpap JP,
Donofry DF, Walker MJ, Dugan JL, Childs JD (2012)
The functional movement screen: A reliability study.
journal of orthopaedic & sports physical therapy 42
(6):530-540
