A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients
Bel
´
en Rubio Ballester
1
, Alica Lathe
1
, Esther Duarte
2
, Armin Duff
1
and Paul F. M. J. Verschure
1,3
1
Laboratory of Synthetic Perceptive, Emotive, and Cognitive Systems (SPECS), Departament de Tecnologies
de la Informaci
´
oi la Comunicaci
´
o(DTIC), Universitat Pompeu Fabra, Roc Boronat, 138 08018 Barcelona, Spain
2
Servei de Medicina F
´
ısica I Rehabilitaci
´
o, Hospitals del Mar I l’Esperanc¸a,
Institut Hospital del Mar d’Investigacions M
`
ediques, Barcelona, Spain
3
Instituci
´
o Catalana de Recerca i Estudis Avanc¸ats (ICREA), Barcelona, Spain
Keywords:
Stroke, Learned Non-use, Wearables, Motor Rehabilitation, Hemiparesis.
Abstract:
After stroke, many patients experience hemiparesis or weakness on one side of the body. In order to com-
pensate for this lack of motor function, they tend to overuse their non-affected limb. This so called learned
non-use may be one of the most relevant contributors to functional loss after post-stroke hospital discharge.
We hypothesize that frequent exposure to movement related feedback through a wearable bracelet device may
1) increase the patient’s intrinsic motivation for using the paretic limb, and 2) counteract learned non-use,
therefore inducing motor recovery. First, to validate the accelerometers-based measurement of arm use, we
recruited 10 right-handed volunteers without neurological impairments. Second, we explored the acceptability
and clinical impact of a low-cost wearable system on 4 chronic stroke patients with hemiparesis. Our results
suggest that frequent exposure to direct feedback about arm use promotes the integration of the paretic limb
in the performance of instrumental activities of daily living (iADLs). In addition, results from questionnaires
revealed that the use of wearable devices may influence positively the patient’s intrinsic motivation for using
the affected arm. To the best of our knowledge, this is the first study suggesting the benefits of wearable-based
feedback as an intervention tool for counteracting learned non-use.
1 INTRODUCTION
After hospital discharge, up to 55% to 75% of stroke
patients experience persistent motor impairments (Lai
et al., 2002) and may even suffer substantial declines
in function in the following 6 months. A number of
studies suggest that this loss may be due to the lack
of use of the paretic limb (Lai et al., 2002), a phe-
nomenon that has been called learned non-use. Re-
cent work on studying the dynamics of motor recov-
ery after stroke have shown that learned non-use may
emerge as a consequence of decision making for mo-
tor optimization, therefore being dependent on two
main factors: the expected success and the expected
cost of using either effector (Hidaka et al., 2012; Han
et al., 2008; Ballester et al., 2015a). On these basis,
there may exist different strategies for counteracting
learned non-use. For instance, Constrained-Induced
Movement Therapy (CIMT) proposes to reduce the
probability of success and increases the cost of us-
ing the non-affected limb by restricting its movement
and tactile feedback using a mitt (Taub and Uswatte,
2003). Recently, we have shown that Reinforcement-
Induced Movement Therapies (RIMT) may be com-
plementary to CIMT (Ballester et al., 2015a; Ballester
et al., 2015b). In RIMT, visual manipulations during
training increase the probability of success and reduce
the cost of using the paretic limb. However, these re-
habilitation protocols are usually limited to short ses-
sions of intervention and may not be suitable for unsu-
pervised domiciliary environments. In light of these
limitations, the use of wearable devices could be spe-
cially suitable for the persistent monitoring and treat-
ment of leaned non-use.
The current state of research and technological de-
velopment shows a tendency towards the gamifica-
tion of rehabilitation tools, combining various types
of sensors to capture motion and posture. Several
studies have tested the reliability and validity of us-
ing accelerometers for measuring arm use in activities
of daily living (Noork
˜
oiv et al., 2014; Uswatte et al.,
2005). In this vein, significant effort has been made in
evaluating the acceptability of wearable devices that
incorporate accelerometers for the quantification of
motor performance and recovery (Wang et al., 2014).
The application of wearable devices to the rehabilita-
24
Ballester, B., Lathe, A., Duarte, E., Duff, A. and Verschure, P..
A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients.
In Proceedings of the 3rd International Congress on Neurotechnology, Electronics and Informatics (NEUROTECHNIX 2015), pages 24-31
ISBN: 978-989-758-161-8
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
tion field offers a number of advantages, such as im-
proved objectivity, sensitivity, and ease of measure-
ment of therapy outcomes. However, because of their
ubiquity, wearable devices may be also useful as inter-
vention tools. Their design and interface enables the
frequent delivery of multimodal feedback during the
performance of iADLs, which may facilitate the re-
alignment of attention towards the affected limb, thus
encouraging the selection of the weaker arm.
Recently, Markopoulos et. al (Markopoulos et al.,
2011) developed a credibility and usability study on
an experimental wearable device that monitors the
patient’s behavior and displays feedback about the
use of the affected versus unaffected arm. So far,
previous work on wearable devices for rehabilitation
describe prototypes and techniques for the integra-
tion of monitoring hardware in wearable garments
as well as communications systems (Uswatte et al.,
2005). Uswatte et al. conducted a clinical experi-
ment in which 20 stroke patients wore an accelerom-
eter on each arm, the chest, and the more affected
leg. Recordings from each sensor were used to es-
timate the duration of movement as a percentage of
the total recording period. Results revealed a strong
correlation between the accelerometers-derived mea-
surements and the Motor Activity Log (Uswatte et al.,
2006). More recent studies have validated and ex-
tended these findings showing strong correlations be-
tween triaxial accelerometry-derived measurements
and the Quality of Movement scores (van der Pas
et al., 2011) or the National Institutes of Health Stroke
Scale (NIHSS) (Gubbi et al., 2013). However, there
is no evidence yet about the clinical impact of these
types of devices.
The aim of this study is to evaluate the potential
of a wearable system for measuring the amount of
use of the paretic arm in iADLs in chronic stroke pa-
tients with upper extremity hemiparesis. Specifically,
we hypothesize that frequent exposure to movement
related feedback through a wearable device may 1)
counteract learned non-use, and 2) increase the pa-
tient’s intrinsic motivation for using the paretic limb.
This work presents results from a pilot study explor-
ing stroke patients’ acceptance of a wearable device
for independent usage in their home setting and its ef-
fectiveness as an intervention tool for promoting the
use of the paretic limb.
2 METHODS
2.1 Equipment
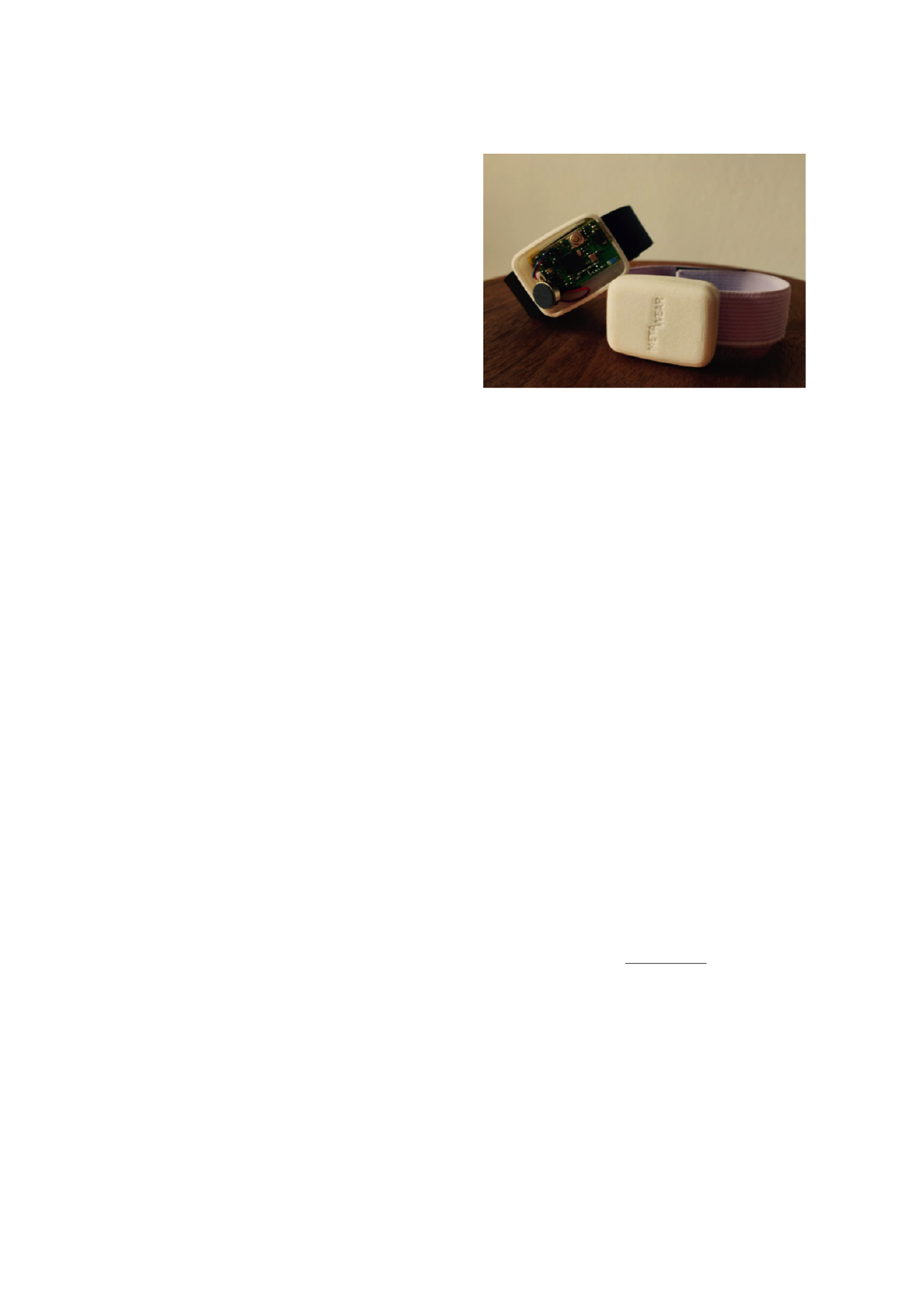
The RGS-Wear is a wearable system for the con-
Figure 1: Prototype wearable bracelets integrating the
MetaWear board and Velcro straps. the MetaWear board
includes a low-power, 3-axial capacitive micromachined ac-
celerometer, RGB LEDs, and a coin vibrating motor.
tinuous monitoring of arm use in hemiparetic stroke
patients. It is composed by a pair of bracelets
and a smartphone (Sony Xperia Z3 Compact).
The bracelets include a coin-sized Bluetooth-Board
(MetaWear, MbientLab, San Francisco, CA.) with in-
tegrated accelerometer, a vibrating motor, an ultra
bright RGB LED, a battery, and a wristband (Fig.
1). The accelerometer is a Freescale MMA8452Q:
a smart low-power, three-axis, capacitive micro-
machined accelerometer with a resolution of 12 bits.
Data recordings from each accelerometer are con-
tinuously monitored and sent through Bluetooth to
a paired smartphone, which demands the patient to
carry the smartphone with him or her throughout the
day. For this purpose the participants were equipped
with a holding bag for the phone to be placed at the
waist.
2.2 Quantification of Arm Use
For monitoring purposes, the acceleration data from
each device (left bracelet, right bracelet, and smart-
phone) is sampled at 50Hz for each directional di-
mension. In order to derive from these data some
meaningful quantification of arm use, we followed a
number of steps. First, over a one minute epoch, we
computed the mean squared sum of the acceleration:
β =
q
α
2
x
+ α
2
y
+ α
2
z
(1)
This measurement represents a rough index of the
amount of movement of the object to which the ac-
celerometer is attached. This method has been shown
to be an adequate approximation of Energy Expen-
diture (EE) in comparison to measurements derived
from the heart’s electrical activity, muscle activation,
and oxygen consumption (van der Pas et al., 2011;
A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients
25
Tsurumi et al., 2002). Next, in order to provide feed-
back to the user, we defined the change in the EE of
the paretic arm as:
δ =
γ
p
− γ
0
γ
p
· 100 (2)
where γ
p
refers to the mean activity of the paretic
arm per hour, γ
0
corresponds to the mean activity
of the paretic arm at baseline, and arm activity is
given by the difference between the activity of the
corresponding arm β
a
and the activity of the body β
b
:
γ = β
a
− β
b
(3)
where [γ]
+
=
γ, if γ > 0
0, if γ < 0
In addition, in order to monitor arm balance, we
compute the ratio between the daily mean activity of
the paretic γ
p
, and non-paretic arm γ
np
. Thus arm bal-
ance is given by:
θ =
γ
p
γ
p
+ γ
np
∗ 100 (4)
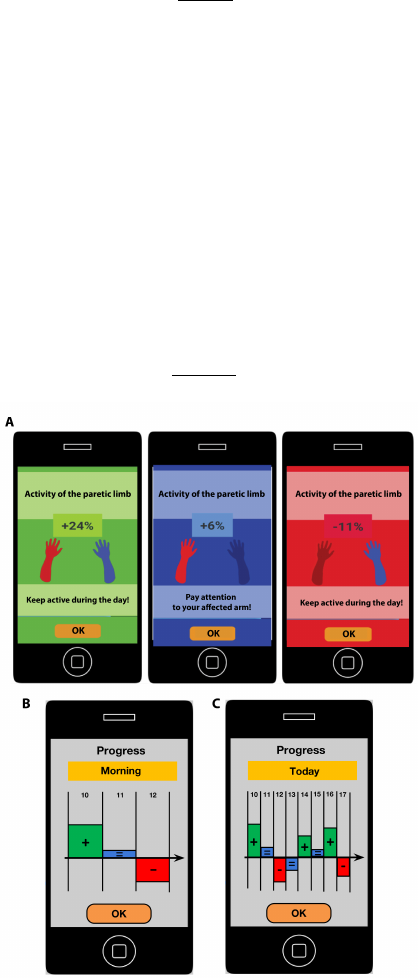
Figure 2: Graphical interface for feedback delivery. A.
Types of feedback according to the change in EE by hour
(Hourly Feedback). B. Example of Review Feedback show-
ing the change in Energy Expenditure (EE) achieved dur-
ing the morning (from 10 to 13 hours). C. Example of Re-
view Feedback delivered at the end of the day, showing the
change in EE by hour along the daily session (from 10 to 19
hours).
2.3 Feedback Design
The main objective of this study was to evaluate the
influence of feedback of performance on arm use.
Therefore, we first explored how to deliver this type
of information to the patient in an efficient and mean-
ingful manner. The design principles shaping RGS-
Wear were derived from the Self-Determination The-
ory proposed by Ryan et al. (Ryan et al., 2008).
This theory defines three main behavioral mediators,
which determine a patient’s self-engagement within
the process of Health Behavior Change:
1. Autonomy: the patient’s degree of Self-
engagement as the willingness to change due to
the self-referenced value of the targeted behavior.
2. Competence: the individual’s capacity to af-
ford a change.
3. Relatedness: the relation of the patient with
the practitioner, who facilitates the other two me-
diators.
Based on these principles, the RGS-Wear was de-
signed to serve as a rehabilitation device for self-
reinforcement. The incoming feedback messages are
delivered through the vibration of both the smart-
phone and bracelets. Additionally, the phone displays
a sound signal, whereas the bracelets’ LEDs blink in
red, green or blue, according to the improvement cat-
egory achieved (Table 1). Every message has a con-
firmation button, which should be pressed to confirm
its reception. The following subsections describe in
detail these feedback messages.
2.3.1 Hourly Feedback
The Hourly Feedback was designed to be simple and
effective as the user derives all information about im-
provement in use with a short glance at his smart-
phone (Fig. 2A). A percentage indicates the mean
change in the EE of the paretic limb in respect to
baseline that was achieved within the previous hour
(mean δ, see Eq.2). This type of messages are accom-
panied by an illustration of the upper-limbs. Beneath,
a comment window shows different motivational say-
ings (e.g. ”Stay active along the day.”). Considering
not to generate pressure, the text appears as a general
request to stay active within the day, regardless of the
numerical result shown.
This feedback was designed to support the pa-
tient’s self-engagement and increase the value of us-
ing the paretic arm in the performance of iADLs. This
type of feedback is thus tightly related to the con-
cept of Autonomy proposed by the Self-Determination
Theory (SDT). In this line, the display of a percentage
NEUROTECHNIX 2015 - International Congress on Neurotechnology, Electronics and Informatics
26
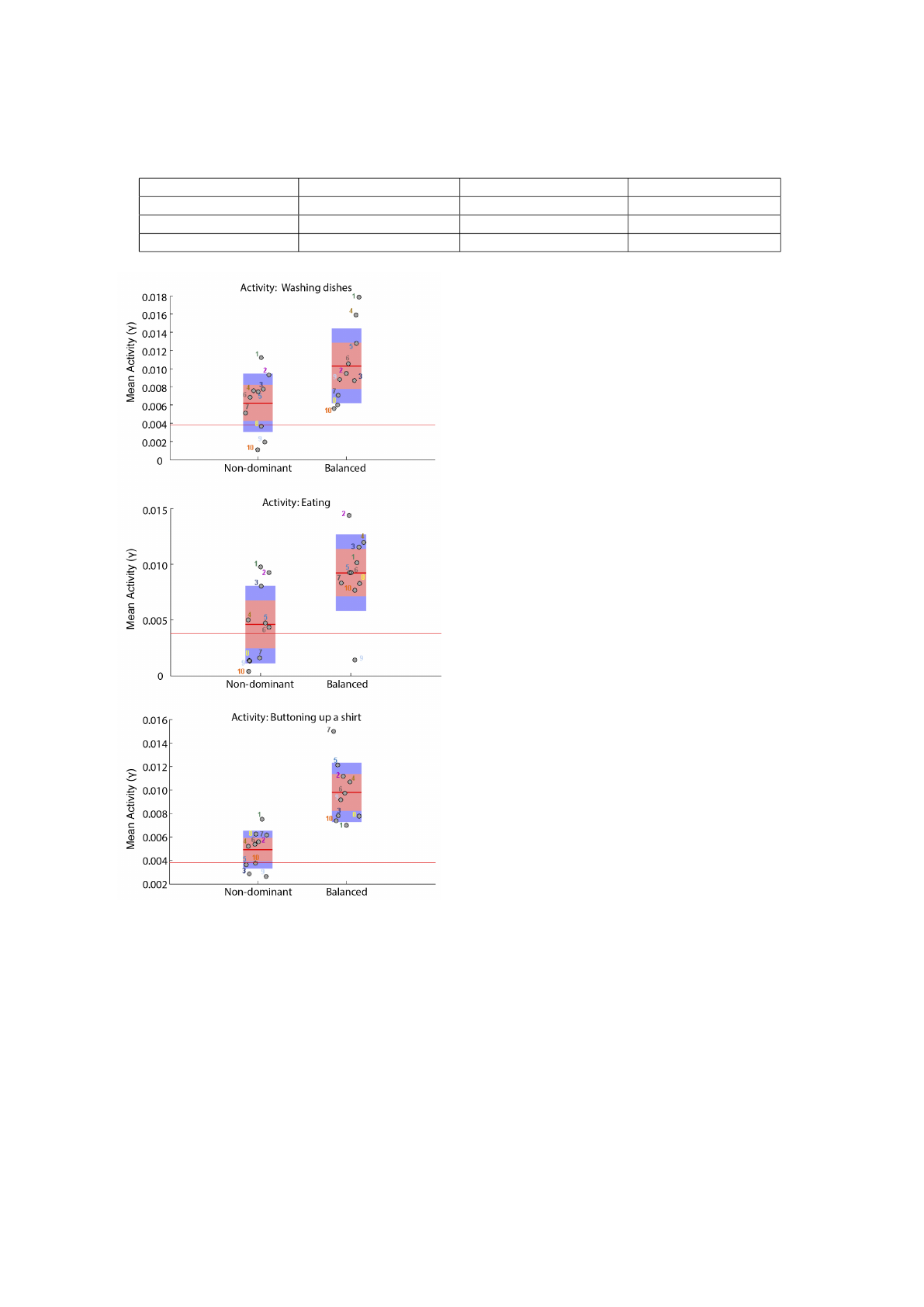
Table 1: Feedback Categories.
Result Above 10% Between 10% and -10% Below -10%
Category Positive Neutral Negative
Signal in bracelets Green blinking light Blue blinking light Red blinking light
Signal in smartphone Positive green operator Positive blue operator Negative red operator
Figure 3: Averaged activity of the non dominant arm, for
each subject, achieved during the execution of three iADLs
(Wash de dishes, eating, and buttoning up a shirt) under two
different conditions. During the Restricted condition, the
use of the left limb was limited. During the Balanced condi-
tion, the participant was encouraged to use both arms. Red
horizontal lines indicate the inactivity threshold.
improvement in use provides a target oriented self-
regulation.
2.3.2 Review Feedback
The Review Feedback displays a summary of the
Hourly Feedback in session intervals (Fig. 2B), thus
providing knowledge of progress. In this study, RGS-
Wear was pre-programmed to monitor 9 consecutive
hours a day. Daily recordings were partitioned in a
morning, afternoon, and night sessions, and each of
them had a duration of 3 hours. Review Feedback was
provided at the end of each session and at the end of
the day, displaying the hourly mean activity level of
the paretic arm in a graphical chart. The rational for
this feedback was to meet the patients’ psychologi-
cal need of Competence by presenting an overview of
performance over time.
2.3.3 Instructions Slides
The RGS-Wear daily protocol is initialized at 10 a.m.
by presenting a number of welcoming slides accom-
panied by an alarm sound that signalizes the begin-
ning of the monitoring.
2.4 Experimental Paradigm
In order to assess the reliability of the RGS-Wear
for capturing differences in arm use, we first con-
ducted an experiment on humans with no neurolog-
ical impairments. We instructed participants to per-
form four iADLs (washing the dishes, eating, button-
ing up a shirt, and walking) while wearing the RGS-
wear bracelets. Each activity had a duration of 3 min-
utes. All activities were performed twice: first, partic-
ipants were asked to use their left arm with reduced
intensity as they would normally do (non-dominant
condition), and second, bi-manual execution was en-
couraged (balanced condition).
After validating RGS-Wear as a monitoring tool,
we designed an experimental paradigm to explore the
potential of RGS-Wear for promoting the use of the
paretic limb in stroke patients. Participants were in-
structed to use the RGS-Wear system at home for five
consecutive weekdays, from 10 to 19 o’clock, except
when bathing. The experiment was divided in three
phases: pre-test, intervention, and post-test. Due to
the ubiquitous presence of the device, the sensation
of being under observation could be cued and may
A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients
27
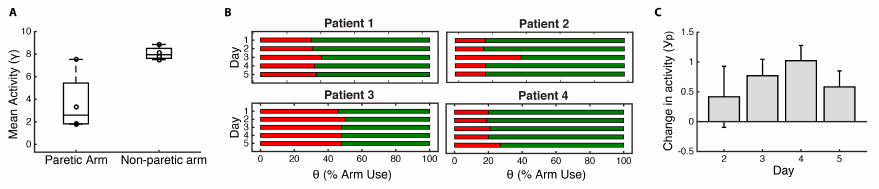
Figure 4: Quantifying behavioral changes. A. Difference between arm activity during baseline (day 1). B. Arm Use Balance
between the paretic (red) and non-paretic arm (green) per day exhibited by each patient. C. Mean change in the activity of the
paretic limb with respect to baseline, across the three days of intervention (day 2-4), and post-test (day 5). The y-axis refers
to the change from baseline averaged across subjects.
lead to an over-encouraged behavior. In order to con-
trol for this effect, patients were instructed to wear
the system everyday but did not receive any type of
feedback at day 1 (i.e. pre-test or baseline) and day
5 (i.e. post-test) of the experimental protocol. From
day 2 to day 4 (i.e. intervention phase), the RGS-
wear system provided Hourly Feedback and Review
Feedback to the patient. Before (day 1) and after the
experiment (day 5), participants fulfilled an Intrinsic
Motivation Questionnaire (IMQ). The IMQ consisted
in 7 statements designed to capture changes in the pa-
tient’s perceived competence and effort when using
the paretic limb (see APPENDIX, Questionnaire on
Intrinsic Motivation). Answers were reported using a
7-point Likert Scale, ranging from Strongly Disagree
to Strongly Agree. In addition, a Usability Question-
naire (UQ) was administered at the end of the experi-
mental protocol (day 5) to assess the system’s accept-
ability in terms of its hardware design, graphical user
interface (GUI), interaction design, and perceived ef-
ficacy (see APPENDIX, Questionnaire on Usability).
In this questionnaire, answers were reported using a
5-point Likert Scale. The ethics committee of clinical
research of the Parc de Salut Mar approved experi-
mental guidelines.
2.5 Participants
For the validation of the accelerometers-based mea-
surement of arm use, we recruited 10 right-handed
volunteers without neurological impairments (5 fe-
males, mean age = 26.6 ± 2.59 years old). Sec-
ondly, in order to explore the clinical impact of the
RGS-Wear, five chronic stroke patients were first ap-
proached by a doctor from the rehabilitation depart-
ment of Hospital Esperanc¸a in Barcelona to determine
their interest in participating in this research project.
Selected patients met the following inclusion criteria:
1) Ischaemic strokes (Middle cerebral artery territory)
and hemorrhagic strokes (intra-cerebral). 2) Mild-to-
moderate upper-limbs hemiparesis. 3) Age between
45 and 85 years old. 4) Absence of any major cogni-
tive impairments. 5) Frequent smartphone user. One
patient refused to participate. The remaining four pa-
tients (4 males, 70.5 ± 6.76 years old) were included
in the study. Prior to the experiment, all participants
signed informed consent.
3 RESULTS
3.1 Accelerometer-based Measurement
of Arm Use
In order to evaluate the reliability and validity
of accelerometry for measuring arm use in non-
impaired subjects, we examined the subjects’ non-
dominant arm activity under 2 different conditions
(non-dominant and balanced), in four different iADLs
(washing the dishes, eating, buttoning up a shirt, and
walking). As we expected, in the non-dominant con-
dition, performance of iADLs was characterized by
the decreased activity of the left hand (Fig. 3). In
the walking task, activity measures fell below the in-
activity level in both conditions, indicating that the
mean acceleration of each hand was not superior to
the mean body acceleration. These results validate
the reliability of the RGS-Wear system for capturing
the amount of use of the upper-limbs in iADLs.
3.2 Effects on Amount of Use
After exploring the use of wearable devices for arm
use monitoring, we proceeded to investigate its appli-
cability as an intervention tool. Since amount of use
and recovery are tightly coupled, using wearable de-
vices to induce an increase in arm use could have a
positive impact in motor recovery. One approach to
pursue this idea is to use wearable devices to expose
the patient to arm movement related feedback, thus
increasing the intrinsic motivation for integrating the
paretic limb in the performance of iADLs.
NEUROTECHNIX 2015 - International Congress on Neurotechnology, Electronics and Informatics
28
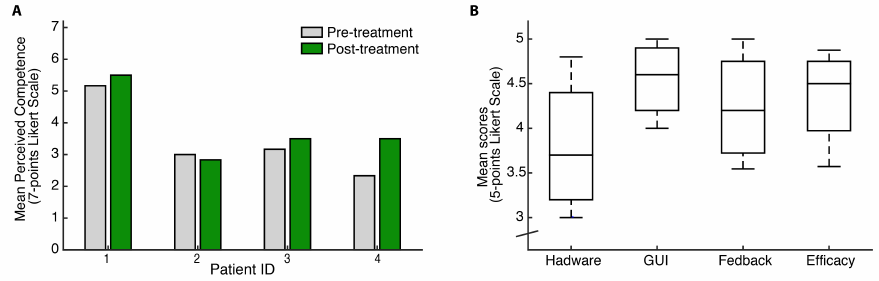
Figure 5: Responses from questionnaires. A. Average scores quantifying the patient’s intrinsic motivation for using the paretic
limb in the performance of iADLs. B. Mean scores for each category assessed by the usability test.
To address this question, we first compared the
mean levels of Energy Expenditure (EE) estimated at
baseline (day 1) for each arm and subject (β in Eq.
1). As expected, we observed that all patients reached
higher EE values when using the less affected limb
(Figure 4A). Patient 3, who presented with mild hemi-
paresis, showed a highly balanced arm use, reaching a
mean EE value of 7.53 for the paretic limb, and 8.85
for the non-paretic limb. These preliminary results
support the use of accelerometry for quantifying arm
use in hemiparetic stroke patients. Next, we analyzed
the change in arm use balance respect to baseline (day
1). Although we observed differences between pa-
tients, the estimation of arm balance values remained
stable within subjects (Fig. 4B). Overall we found
a general increase in the Arm Use Balance, suggest-
ing an increased integration of the affected limb in
the performance of iADLs. However, since Arm Use
Balance is a relative measurement (see Eq. 4), it does
not express the amount of movement. A patient could
therefore achieve positive improvements in Arm Use
Balance by only limiting the movement of the non-
paretic limb. In order to take into account the patient’s
amount of arm movement, we analyzed the change in
the activity of the paretic limb with respect to baseline
(day 1). Interestingly, results revealed an increase in
activity which accumulated along the three days of in-
tervention (Fig. 4C). Even though we observed a drop
in activity at day 5 (post-test), when no feedback was
delivered any more, arm use improvements were still
partially retained.
3.3 Effects on the Patients’ Intrinsic
Motivation
We analyzed the influence of the RGS-Wear paradigm
on intrinsic motivation by comparing the scores re-
ported by the four patients before (day 1) and after
the treatment (day 5). We observed that, after treat-
ment, 3 out of 4 patients exhibited higher intrinsic
motivation to use the paretic limb (Fig. 5A). Accord-
ing to the Self-Determination Theory, this subjective
improvement may emerge from the repetitive expo-
sure to knowledge of progress, a factor tightly linked
to the behavioral mediator Autonomy.
3.4 Usability
We studied the usability aspects of the RGS-Wear
through a questionnaire that was divided into 4 cat-
egories (5 questions each): hardware, graphical inter-
face, feedback, and perceived efficacy. Overall, the
patients’ ratings were above 3 (neutral), suggesting
that the system’s design was generally accepted. In-
terestingly, we noticed that the rating of hardware fea-
tures was notably lower in comparison to the other
categories. When we explored the patient’s answers
in detail, we found that those statements referring to
the comfort of putting the bracelets on received lower
scores from most of the patients.
4 CONCLUSION AND
DISCUSSION
We have presented results from a pilot study support-
ing the benefits of wearable-based feedback on arm
use. Our results suggest that frequent exposure to
direct feedback about arm use promotes the integra-
tion of the paretic limb in the performance of iADLs.
In addition, results from questionnaires revealed that
the use of wearable devices may influence positively
the patient’s intrinsic motivation for using the affected
arm.
The work we presented in this article is the con-
tinuation of our previous work on the use of new
technologies for counteracting learned non-use. In
a recent study, we used a neurologically grounded
A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients
29
computational model of motor recovery (Han et al.,
2008) that can predict the positive influence of
reinforcement-based training on arm use (Ballester
et al., 2015a). In this work, we proposed that hand
selection is modulated by two main parameters: ex-
pected success and effort. We conducted two clini-
cal experiments that suggested that by increasing the
value of using the paretic limb (expected success) and
decreasing its cost (effort) we can promote its spon-
taneous use (Ballester et al., 2015b) and boost recov-
ery (Ballester et al., 2015a). Based on these findings,
we now explore how wearable devices could allow
the ubiquitous delivery of a variant of Reinforcement-
Induced Movement Therapy (RIMT).
Our results suggest that monitoring the amount of
arm use and providing knowledge of progress could
provide multiple benefits: 1) it may allow the pa-
tient to set-up implicit goals, and 2) it may increase
the value of using the paretic limb, therefore bias-
ing effector selection patterns. Thus, the repetitive
exposure to reinforcement-based feedback after per-
formance may modify both the individual’s goals and
self-representation. While the first may provide the
necessary context for the introduction of behavioral
changes, the second may consolidate them. Inter-
estingly, a recent controlled clinical trial including
156 acute stroke patients evaluated the clinical impact
of using wearable triaxial accelerometers at both an-
kles and recording continuously for 8 hours per day
(Dorsch et al., 2015). Once a week, participants in
the experimental group also reviewed the results of
their summary activity graphs with the therapists. Re-
sults indicated that the group receiving the augmented
feedback did not spend a greater amount of time walk-
ing. This findings seem to be contrary to our re-
sults. This difference can be explained by three fac-
tors: 1) the RGS-Wear provided frequent daily feed-
back about performance and progress, 2) the patients
using RGS-Wear reviewed their activity feedback au-
tonomously and 3) the RGS-Wear was applied on the
upper-extremities while Dorsch, et al. focused in gait
and lower-extremities.
Future work aims at validating the impact of RGS-
Wear in arm use by conducting a controlled longitu-
dinal clinical study on acute stroke patients. In this
study we plan to measure the retention of improve-
ments in arm use induced by the RGS-Wear, and its
consequent influence on motor recovery.
ACKNOWLEDGEMENTS
We would like to acknowledge all patients who par-
ticipated in this study. Special thanks to Dr. Boza
G
´
omez for her assistance in recruiting stroke patients.
This project was supported through ERC project
cDAC (FP7-IDEAS-ERC 341196), EC H2020 project
socSMCs (H2020-EU.1.2.2. 641321) and MINECO
project SANAR (Gobierno de Espaa).
REFERENCES
Ballester, B. R., Maier, M., Duff, A., San Segundo,
R., Casta
˜
neda, V., and Verschure, P. (2015a).
Reinforcement-Induced Movement Therapy: A novel
approach for overcoming learned non-use in chronic
stroke patients. In Proceedings of the International
Conference on Virtual Rehabilitation. In press., pages
1–6.
Ballester, B. R., Nirme, J., Duarte, E., Cuxart, A., Ro-
driguez, S., Verschure, P., and Duff, A. (2015b).
The visual amplification of goal-oriented movements
counteracts acquired non-use in hemiparetic stroke
patients. Journal of neuroengineering and rehabili-
tation, 12(1):50.
Dorsch, a. K., Thomas, S., Xu, X., Kaiser, W., Dobkin,
B. H., Emara, T., Edwards, D., Fonzetti, P., Maasch,
J., Lee, S.-G., Owolabi, M. O., Hamzat, T. K.,
LeBlanc, C. J., Morse, R., Swaminathan, N., Karatas,
G. K., Boza, R., Brown, a. W., Miyai, I., Kawano, T.,
Chen, S.-Y., Hanger, H. C., Zucconi, C., Mammi, S.,
Ghislanzoni, C., Juan, F., and Lang, C. E. (2015). SIR-
RACT: An International Randomized Clinical Trial of
Activity Feedback During Inpatient Stroke Rehabili-
tation Enabled by Wireless Sensing. Neurorehabilita-
tion and Neural Repair, 29(5):407–415.
Gubbi, J., Rao, A. S., Fang, K., Yan, B., and Palaniswami,
M. (2013). Motor recovery monitoring using accel-
eration measurements in post acute stroke patients.
Biomedical engineering online, 12:33.
Han, C. E., Arbib, M. A., and Schweighofer, N. (2008).
Stroke rehabilitation reaches a threshold. PLoS com-
putational biology, 4(8):e1000133.
Hidaka, Y., Han, C. E., Wolf, S. L., Winstein, C. J., and
Schweighofer, N. (2012). Use it and improve it or
lose it: interactions between arm function and use
in humans post-stroke. PLoS computational biology,
8(2):e1002343.
Lai, S.-M., Studenski, S., Duncan, P. W., and Perera, S.
(2002). Persisting consequences of stroke measured
by the Stroke Impact Scale. Stroke, 33(7):1840–1844.
Markopoulos, P., Timmermans, A. A. A., Beursgens, L.,
Van Donselaar, R., and Seelen, H. A. M. (2011). Us’
em: The user-centered design of a device for motivat-
ing stroke patients to use their impaired arm-hand in
daily life activities. In Engineering in Medicine and
Biology Society, EMBC, 2011 Annual International
Conference of the IEEE, pages 5182–5187. IEEE.
Noork
˜
oiv, M., Rodgers, H., and Price, C. I. (2014). Ac-
celerometer measurement of upper extremity move-
ment after stroke: a systematic review of clinical stud-
ies. Journal of neuroengineering and rehabilitation,
11(1):144.
NEUROTECHNIX 2015 - International Congress on Neurotechnology, Electronics and Informatics
30
Ryan, R. M., Patrick, H., Deci, E. L., and Williams,
G. C. (2008). Facilitating health behaviour change
and its maintenance: Interventions based on self-
determination theory. European Health Psychologist,
10(1):2–5.
Taub, E. and Uswatte, G. (2003). Constraint-induced move-
ment therapy: bridging from the primate laboratory to
the stroke rehabilitation laboratory. Journal of Reha-
bilitation Medicine, 35:34–40.
Tsurumi, K., Itani, T., Tachi, N., Takanishi, T., Suzumura,
H., and Takeyama, H. (2002). Estimation of En-
ergy Expenditure during Sedentary Work with Up-
per Limb Movement. Journal of occupational health,
44(6):408–413.
Uswatte, G., Foo, W. L., Olmstead, H., Lopez, K., Holand,
A., and Simms, L. B. (2005). Ambulatory monitoring
of arm movement using accelerometry: an objective
measure of upper-extremity rehabilitation in persons
with chronic stroke. Archives of physical medicine
and rehabilitation, 86(7):1498–1501.
Uswatte, G., Taub, E., Morris, D., Light, K., and Thompson,
P. A. (2006). The Motor Activity Log-28 assessing
daily use of the hemiparetic arm after stroke. Neurol-
ogy, 67(7):1189–1194.
van der Pas, S. C., Verbunt, J. A., Breukelaar, D. E., van
Woerden, R., and Seelen, H. A. (2011). Assessment
of arm activity using triaxial accelerometry in patients
with a stroke. Archives of physical medicine and re-
habilitation, 92(9):1437–1442.
Wang, Q., Chen, W., and Markopoulos, P. (2014). Literature
review on wearable systems in upper extremity reha-
bilitation. In IEEE-EMBS International Conference
on Biomedical and Health Informatics (BHI), pages
551–555. IEEE.
APPENDIX
Questionnaire on Intrinsic Motivation: 1- Inte-
grating the affected in the performance of activities
of daily living allows me to be more independent.
2- I’m quite competent when I use my affected arm.
3- It’s really tiring to use the affected arm in my
activities of daily living. 4- I feel secure when I use
the affected arm for eating. 5- I feel secure when I
use the affected arm for washing the dishes. 6- I feel
secure when I use the affected arm for dressing up.
7- How much do you use the affected arm?
Questionnaire on Usability: 1- It was easy to put on
the bracelets without help. 2- It was easy to put on
the smartphone without help. 3- It was comfortable
to wear the bracelets. 4- It was comfortable to wear
the smartphone. 5- It was easy to move the affected
arm while wearing the bracelets. 6- It was easy to
hear the messages alarm on the smartphone. 7- It was
easy to notice the bracelets vibrations and lights. 8- It
was easy to understand the messages on the screen of
the smartphone. 9- It was ease to press the buttons on
the screen of the smartphone. 10- It was easy to read
the texts appearing on the screen of the smartphone.
11- I think I missed more than 3 messages a day. 12-
Sometimes the messages were annoying. 13- Some-
times the messages scared me. 14- The hourly feed-
back about the amount of movement was correct. 15-
Feedback about the amount of arm movement across
days was correct. 16- I think the messages were ac-
curate in reporting my activity. 17- I think the levels
of activity reported by the messages were lower than
my real activity level. 18- I think the levels of activity
reported by the messages were higher than my real ac-
tivity level. 19- There were too many messages along
the day. 20- I would like to receive more messages.
A Wearable Bracelet Device for Promoting Arm Use in Stroke Patients
31
