
Suggestions for the Elicitation of Seniors Involvement in ICT and
Socially Innovative Solutions to Tackle IT
Adrianna Nizinska
1
, Antoni Zwiefka
2
and Karol Kozak
3,4
1
Dean Educational Affairs, University of Lower Silesia, Wroclaw, Poland
2
Departament Polityki Zdrowotne, Urząd Marszałkowski Województwa Dolnoślaskiego, Wroclaw, Poland
3
Medical Faculty, Dresden University of Technical, Fetscherstraße 74, D-01307 Dresden, Germany
4
Data management Center, Fraunhofer IWS, Winterbergstraße 28, 01277 Dresden, Germany
adrianna.nizinska@dsw.edu.pl, antoni.zwiefka@dolnyslask.pl, karol.kozak@uniklinikum-dresden.de
Keywords: Seniors, ICT, Human Computer Interaction, Social
Abstract: Human-computer interaction (HCI) issues for older people are extremely important in the light of the rapidly
ageing population in developed countries. In addition, technology offers great potential for this age group, but
it will be only useful if it can be used effectively by its target users. We will therefore examine how HCI can
address the needs and situations of this increasing older population and how their involvement can be
maximized in order to support participation and empowerment. In recent years, HCI technologies have
manifested their potential to enhance the autonomy and quality of the life of elderly people, through boosting
the elicitation of seniors. This paper is describing a methodology and challenges that will support healthcare
professionals’ action in the further effective usage of systems based on HCI.
1 INTRODUCTION
Innovations in human-computer interaction research
have revealed effective methods for people with
various disabilities to use computers or to receive
computer-aided medical treatment (Hendrick,
Schooley & Gao 2013).
Since the inception of medical computing three
decades ago there has been an extensive discussion of
the value of developing an interactive computer-
based clinical record system for the practitioner, not
only to provide routine decision support for patient
care, but for the capture of both contemporaneous and
longitudinal data important to clinical epidemiology,
quality assurance, risk management, and the
development of increasing varieties of experiential
based reasoning. The goal of regular clinical use
requires to put the user in focus or – as HCI (human-
computer interaction (HCI) researchers would call it
– to adopt a user-centered design approach (Norman,
Draper 1986). This is not what already has been
implemented and is our recommendation.
Human-computer interaction testing is being
commonly used in many commercial settings to form
better human computer interface scenarios (Gosbee,
Ritchie 2007). The users of HCI are both patients and
medical professionals. This means the HCI testing
needs to include both types of users. Patients come
with all levels of background and experience in
technology. Medical professionals are naturally very
patient-focused and not necessarily focused on
medical devices. We suggest that HCI testing needs
to meet the needs of all potential users.
Nevertheless, there has been a growing attention
to the development of more powerful social
methodologies, identifying barriers and focusing on
challenges with new interaction modalities. It is also
crucial for these methodologies to address the issue
of participation and empowerment. Since WHO
Global Strategy for Health for All by the year 2000
(1981) these categories have been of high importance
in improving health and still remaining a challenging
one. This paper is describing a methodology and
challenges that will support healthcare professionals’
104
Nizinska A., Zwiefka A. and Kozak K.
Suggestions for the Elicitation of Seniors Involvement in ICT and Socially Innovative Solutions to Tackle IT.
DOI: 10.5220/0005890201040108
In Proceedings of the Fourth International Conference on Telecommunications and Remote Sensing (ICTRS 2015), pages 104-108
ISBN: 978-989-758-152-6
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

action in further effective usage of systems based on
HCI.
2 PROBLEM DEFINITION
As people get older they will also want to remain
active in ways previous generations did not. They will
want to continue to be a part of the workplace, to drive
and travel the world. Seniors in 15-years´time will
expect and demand from suppliers to be able to use
new technologies as they appear on the market.
Seniors will want to use computer technology to stay
connected to society, work colleagues, friends and
children. They will want them to support their health
and well-being. And as they get older, friends and
family may want computers to keep an eye on their
aging family members. There will be an increasing
number of social communities, where people will be
able to upload their personal health data or send
photos of what they have eaten and a log of their
activities to online doctors who will be able to give
them up-to-date and personalized assessments.
Medical records of physical and psychological health
may also become resources for new ways of sharing
and documenting the medical problems of older life,
allowing for more customized and reassuring health
care.
The last 15 years and the era of smartphones and
IP-based devices have seen not only an enormous
growth in the number of devices, but also an almost
explosive diversification in the nature of these
devices, operating systems and terminals as they have
entered every aspect of our lives. In this paper, we
face senior population where they will need to live
with an ever growing and dynamic set of
interconnected digital devices. End- user interfaces
will be close to seniors and even attached to them,
while others will be invisibly built into their private
ecosystem (home, senior house).
Design recommendations for senior-targeted
technologies or rendering more elderly-friendly
common technologies have been common in the
literature on aging and technology (Discipulus
Project, May 2013). Changes particularly in the
cognitive, sensory and psychomotor functioning of
adults as they grow older mean that the elderly often
require interfaces that correspond their specific needs.
What are the key technological setup guidelines for
designing a computer system for senior users?
The reason can be discussed from two different
points of view. The first is their age-related problems;
the physical and mental decline make it hard to adapt
to new products. Another perspective is a software
logical and interface design; software architects do
not take into account older users’ characteristics and
personalization. For a more specific group of users
such as seniors, it is necessary to find out wider and
deeper design parameters, which should be a more
specific and enchanted version of technological
guidelines.
3 SUGGESTIONS
3.1 Seniors as users and co – designers
of ICT based e-health solutions
Most often the innovative business processes in
health care results in shortening the healing process
through the support areas. This support is mainly
based on effective self-management and integrated IT
systems. Such innovation systems can also include
the implementation of telemedicine Innovations (Fig
1). These methods rely on the analysis of business
processes and organizational structure in terms of
increasing the efficiency of the care organization.
There are many processes for improving the patient
care with the possibility to increase efficiency in
health care. In this group integrated care pathways are
a typical patient-centric approach to the care of frail
people realized by CareWell Project . It is an
innovative approach and consists of a platform
supporting information and communication needs of
the patient. Every service to be active should also be
gathered from the relevant experts. It supports what
needs to be in place for legal, technical,
organizational and financial requirements as well as
the different needs of patients and healthcare
professionals whilst taking into account elements that
may bias them, such as their current access attitude
and knowledge of ICT. It is also important how they
perceive the impact the service will have on them and
what they expect to be the service’s advantages and
disadvantages.
A new vision of elderly care is based on the
patient's focusing and on high-quality equitable
health care for all patients in the Europe. Providing a
strong and integrated service for senior patients in the
area of health, social inclusion and life and personal
fulfillment is possible through the use of e-health
solutions.
Suggestions for the Elicitation of Seniors Involvement in ICT and Socially Innovative Solutions to Tackle IT
105
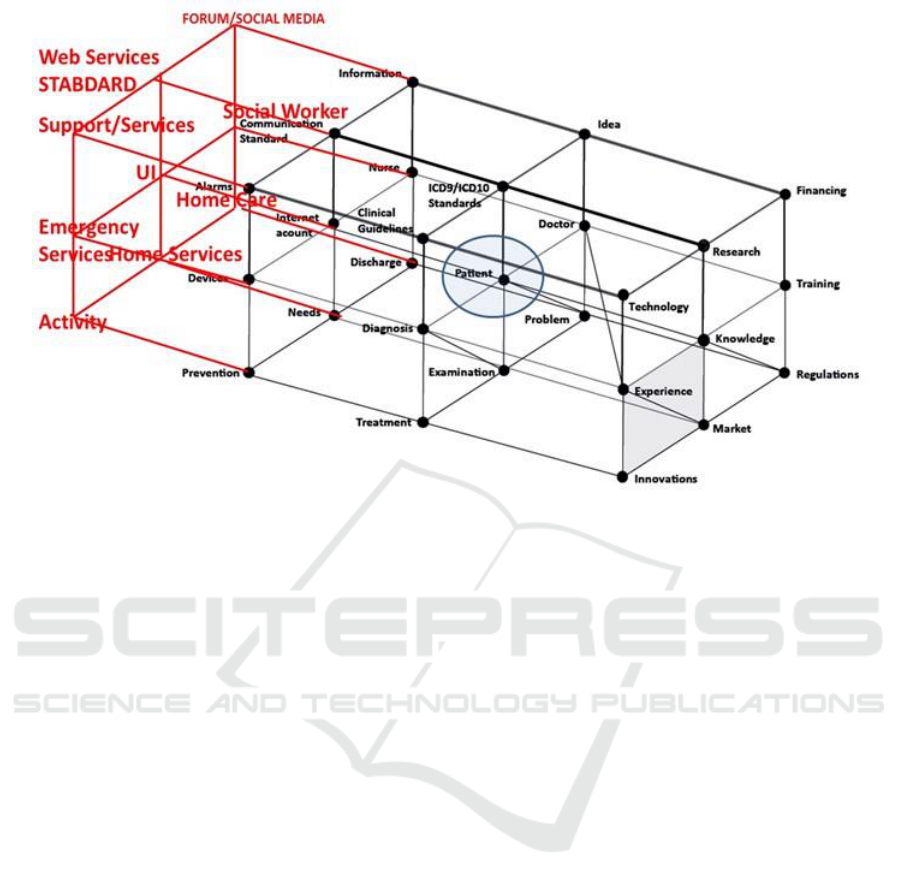
Fig 1. Graphical representation of health care system
According to the EU health policy priorities in the
field of e-health it is necessary to put the patient into
the center of attention and activity. The main risk
factors and efforts in empowering seniors activity are
based on the acceptance by patients and doctor
relationship (with an emphasis on understanding and
trust). Patient empowerment should focus on social
responsibility to take into account long-term costs of
telemedicine (after pilot stage the costs will be shifted
to the patients), and the risk that non-users of
Telehealth will have some serious reservations about
the lack of face-to-face contacts. Telecare in the
future should fully replace "conventional health
care". For the effective implementation of TeleHealth
it is necessary to consider more barriers on the side of
technology than patients. Another influence of
Telecare, which should be considered, is based on
patient safety in communications with healthcare
professionals. This is why many of EU projects, such
as CareWell project, are focused on the impact of e-
health solutions concerning the safety of the patient.
Based on the CareWell experience it is very important
to design networking with other key stakeholders at
the EU level to put the patient at the center of
attention. In accordance with the principles of
equality, prevention is the process by which people
can gain greater control over decisions and actions
affecting their health (WHO 1998). These key issues
in CareWell Projet were mainly based on
collaboration, networking, and mutual talks
according to the knowledge and expertise of patients,
resources and styles of action. Now, patients should
be able to plan what to do next, how to go forward
and how to build their own solutions to health issues.
There is a need to develop initiatives and educational
interventions (Cooper et al. 2011) which utilize the
principles of adult education who wish to have
influence on the feelings, thoughts and behaviour.
According to this, it is necessary to use teaching
strategies to enable patients to make choices, so that
they can transform their knowledge into practice.
Therefore, theoretical models of behavior should be
incorporated into models of education. Interventions
should be designed taking into account the expected
effects such as quality of life, personal models of the
disease and the empowerment regardless of physical
conditions and in accordance with the instructions of
self-care. For the entire patient support process and
education, it is important that the patient is able to
evaluate the quality of life. Therefore, questionnaires
about the quality of life (QoL or QOL) will be filled-
in as a part of patients enrollment in the CareWell
project. Furthermore, the emphasis is put on the
importance of questionnaires, which generally relate
to the quality of everyday life of the individual, or
they asses their well-being (Table 1). This includes all
emotional, social and physical aspects of life of an
individual in connection with health. In healthcare the
quality of life and its assessment is very important.
However, every person may be limited in time
Fourth International Conference on Telecommunications and Remote Sensing
106
through an illness or a disability. In this way it can
influence the interface of the IT system.
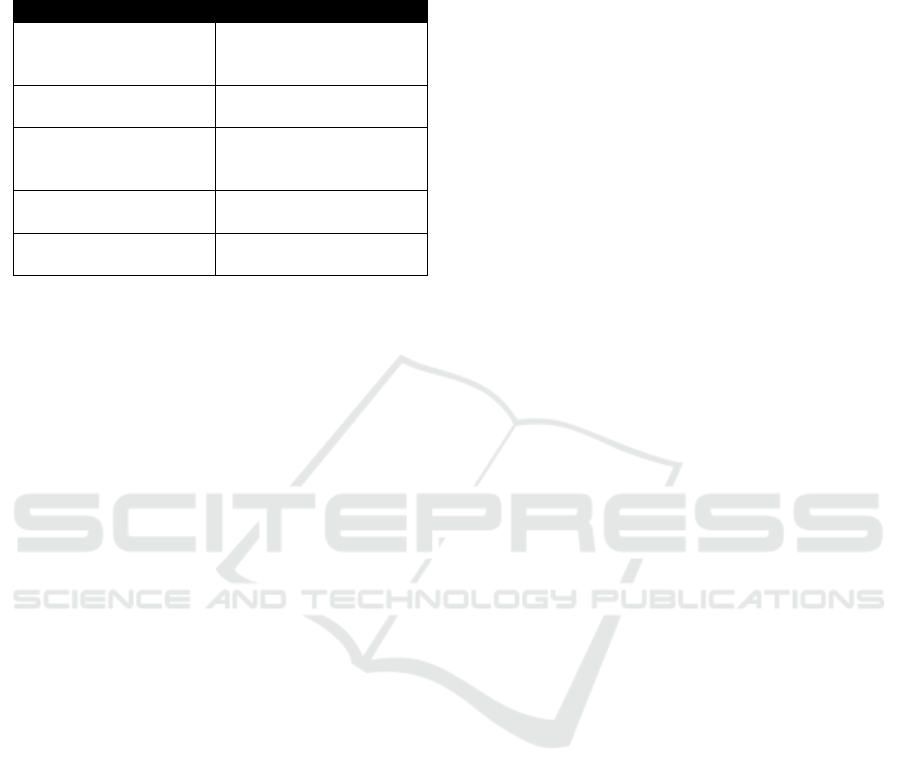
Table 1: List of existing questionnaires.
Questionaire
Description
PIRU
Questionnaire on user
experience of Integrated
Care
GDS
Geriatric Depression
Scale
Barthel Index
Barthel Index Of
Activities Of Daily
Living
IADL
Instrumental Activities of
Daily Living Scale
eCCIS
Questionnaire on service
utility and costs.
On the basis of surveys such as PIRU, GDS, the
patient empowerment initiative was possible to be
taken by the three EU projects: SmartCare,
BeyondSilos and CareWell. Implementation of these
projects will inevitably deepen the possibility of wide
adoption of the technology. Moreover,
partners/regions will implement integrated care
services with adequate incentives. Currently general
care pathways should evolve in the direction of each
individual track. This type of interaction will allow
the patient to improve the integrated care. Integration
is an extremely important aspect of health and social
care for millions of people. It is not about the
structure, organization and roads, it concerns the
achievement of better patient outcomes.
The comprehensive transformation of health care,
which is currently delivered to the patient, is based on
technological innovation. The high demand for
deeper studies concern the improvement of
multidisciplinary IT infrastructure, better
communications, high-quality data and the highest
quality tools. This translational vision is building a
vision of Digital Patient (ang. Discipulus Project
2013 ) .
3.2 Participatory action research
model of seniors involvement in
informing the design and
improving the functionality of the
systems.
One of the ways to respond to the need of profound
empowerment and involvement of elderly people in
designing and using ICT based health systems can be
an exploration of participatory action research (PAR),
which is a methodological approach based on social
sciences. It gives a non- researcher a status of quasi
researcher and increases their involvement in
designing, implementing and maintaining vital social
innovations. Such approaches respond well to the
needs of all adults as a learners, social actors and
proactive beings.
According to Baum, McDougal and Smith (2006)
PAR differs from most other approaches to public
health research, because it is based on reflection, data
collection and action that aims to improve health and
reduce health inequities through involving the people
who, in turn, take actions to improve their own health.
An attempt of applying the PAR approach in ICT-
based health intervention was the idea behind the
design of STAMFoRd concept (consortium of H2020
PHC – 21-2015, Advancing active and healthy ageing
with ICT: Early risk detection and intervention,
http://ec.europa.eu/research/participants/portal/deskt
op/en/opportunities/h2020/topics/2268-phc-21-
2015.html led by Italian company, ENG, currently in
the process of reviewing ). The concept intends to
realize an innovative, unobtrusive, intuitive and cost
effective Indoor Falls Risk Monitoring and
Management System for older adults living in nursing
homes and/or alone at home. The main goal to
achieve is to develop and validate an integrated ICT
solution for predicting indoors falls aimed to tailor
ICT interventions.
In this concept the interests and the balance of
power between the different social groups involved
are decisive in determining whether or not the end-
users become real participants in the design process.
Standard protocols will be developed in STAMFord
according to state of the art in the field:
• the level of regulatory controls will be
commensurate with the potential risks associated with
the technological ecosystem to protect the end-user
while ensuring continued access to new technologies
and an innovation-friendly business environment;
• regulatory framework addressing a life cycle of
the project will include definition and classification
of the end-user devices, essential principles of safety
and performance, quality system requirements,
vigilance system requirements and the use of
international integration standards;
• the use of international nomenclature and
standards will be encouraged, due to the need of
exchange technology between two end‐user locations
of partners in the project. The level of regulatory
control for the end-user should increase with the rise
of the degree of risk, taking account of the benefits
offered by use of the device.
Since real end-user participation is essential for
the successful outcome of the observation and
Suggestions for the Elicitation of Seniors Involvement in ICT and Socially Innovative Solutions to Tackle IT
107

prediction process, another factor will be introduced
- a social-science based PAR approach will be used
to involve seniors, to empower them and to increase
their independence and control over the whole
process of engagement in the project's activities, as a
complementary protocol to the full compliance with
technical requirements.
What would be the added value of PAR, on top of
standard protocols of ensuring end- users
engagement?
- PAR’s main goal is to enable action. Action is
achieved through a reflective cycle, whereby
participants collect and analyze data, then determine
what action should follow.
- PAR’s approach pays careful attention to power
relationships, advocating for power to be deliberately
shared between the researcher and the researched:
blurring the line between them until the researched
become the researchers. The researched cease to be
objects and become partners in the whole research
process.
- unlike other static approaches, PAR does not
remove data and information from their contexts.
Most health research involves people, even if only as
passive participants, as “subjects” or “respondents”.
PAR advocates that those being researched should be
involved in the process actively. The degree to which
this is possible in health research will differ as will
the willingness of people to be involved in research
(Baum at al., 2006 , p. 854)
4 CONCLUSIONS
The recommendation for improving future practices
in the elicitation of seniors´ involvement in ICT-
based health solutions, based on the experiences of
ongoing and future projects in the field can be
summarized as follows. With aging population it is a
vital social and economic purpose to develop
complex and, sophisticated, yet easy to use and
reliable, ICT systems supporting wellbeing,
healthcare and interventions. It calls for sustainable
development: in order to make such systems useful
and productive there is a need for advancement in the
field of technology and a need for advancement in the
methods of involving active seniors in designing such
services. Both fields need to be balanced, but they
cannot be developed separately – there is a call for
synergetic and socially innovative approaches. One of
the ways to achieve that is to take multidisciplinary
approach and equally respect all the sciences:
medical, technical, social and humanities - to build
integrated systems supporting and empowering all
involved participants. The biggest challenge so far is
to successfully communicate between all the
disciplines, while designing, testing and developing
products and services, but without tackling it, the
profoundly integrated approaches will not be
achievable.
REFERENCES
Baum, F., MacDougall, C., & Smith, D. (2006).
Participatory action research. Journal of Epidemiology
and Community Health, 60(10), 854–857.
doi:10.1136/jech.2004.028662
Cooper at all 2001
Barker, M., Baird, J., Lawrence, W., Jarman, M., Black, C.,
Barnard, K., Cradock, S., Davies, J., Margetts, B.,
Inskip, H. & Cooper, C. (2011). The Southampton
Initiative for Health: a complex intervention to improve
the diets and increase the physical activity levels of
women from disadvantaged communities. J Health
Psychol. 2011 Jan;16(1):178-91, doi: 10.1177/
1359105310371397
Digital Patient Roadmap, Discipulus Project,
DISCIPULUS Roadmap for the Digital Patient FINAL
DRAFT, May 2013
WHO (1981). Global Strategy for Health for All by the year
2000. Geneva: World Health Organisation. Retrieved
July 17th, 2015 from: http://whqlibdoc.who.int/
publications/9241800038.pdf
Gosbee, J. and Ritchie, E. (2007). Human–Computer
Interaction and Medical Software, Interactions,
July/August.
Hendrick, E., Schooley, B. and Gao C. ( 2013).
CloudHealth: Developing A Reliable Cloud Platform
for Healthcare Applications, IEEE International
Workshop on Consumer eHealth Platforms, Services
and Applications, 2013 (accepted)
Norman, D.A. and Draper S.W. (1986). User centered
system design: New perspectives on human- computer
interaction. Lawrence Erlbaum Associates, Hillsdale,
NJ.
Martin, L. R., Williams, S. L., Haskard, K. B., & DiMatteo,
M. R. (2005). The challenge of patient adherence.
Therapeutics and Clinical Risk Management, 1(3),
189–199.
WHO (1998).The World Health Report 1998 Life in the
21st century A vision for all Report of the Director-
General, World Health Organization.
Fourth International Conference on Telecommunications and Remote Sensing
108
