
Robotics Enabled Augmented Health
Artur Arsenio
IST-ID, Universidade da Beira Interior, YdreamsRobotics
Edifício A Moagem - Cidade do Engenho e das Artes, Largo da Estação 6230-311 Fundão
{artur.arsenio}@ydreamsrobotics.com
Abstract. Nowadays it is increasingly important, for social and economic rea-
sons, to provide augmented health assistance for people at home. This will
mostly benefit some specific user groups, such as elderly, patients recovering
from physical injury, or athletes. This chapter describes the application of ro-
botics, under the scope of the Augmented Human Assistance (AHA) project, for
assisting people health. Two complementary and interacting approaches are de-
scribed. The first consists on a mobile robot nurse, that assists patients and el-
derly on their daily lives, such as for advising on medicine intake, or providing
complementary biomedical sensing equipment for health monitoring. The other
approach consists of multimodal feedback assistance through augmented reali-
ty, haptic sensing and audio, in order to guide and assist people on the execu-
tion of exercises at home.
1 Introduction
The world population is aging rapidly. There is an increasing need for health assis-
tance personnel, such as nurses and physiotherapeutic experts, in developed countries.
On the other hand, there is a need to improve health care assistance to the population,
and especially to elderly people.
The World Health Organization estimates that sedentarism is the 4
th
main factor in
worldwide mortality, and is associated with several diseases, such as breast and colon
cancer, obesity, diabetes, and ischemic strokes. For instance, childhood obesity origi-
nates other health problems such as hypertension related to left ventricular hypertro-
phy, atherosclerosis and diastolic dysfunction. It is therefore important to identify
children in risk, through continuous health monitoring (e.g. body temperature, blood
pressure, electrocardiogram). Concerning elderly, estimates indicate that by 2030,
~4% of the USA population will have experienced a stroke, with related costs ex-
pected to rise from $71.55 billion to $183.13 billion between 2012 and 2030.
Hence, sedentarism is not only a social problem, but also economical, threatening
the sustainability of current health systems. New technologies are required for ena-
bling treatment at home, reducing pressure for health care personnel at hospitals.
Furthermore, automated systems at hospitals will enable significant cost reductions
and improved efficiency. Information technology has also been playing an increasing
role in the health care area throughout the years, aiding it to be more accurate, faster
to respond, and less susceptible to human errors. There is therefore the need not only
to develop technological solutions that promote active aging and prevent sedentary
behaviors, but also to find new technologies for assisting a growing, aging population.
Arsenio A.
Robotics Enabled Augmented Health.
DOI: 10.5220/0006162300330052
In European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems (EPS Lisbon 2015), pages 33-52
ISBN: 978-989-758-095-6
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
33

In this context, the advances in information, robotic and assistive technologies
have the potential to increase quality of life and change health care delivery models,
reducing costs, and improving monitorization. The “AHA: Augmented Human Assis-
tance” project is a novel, integrative and cross-disciplinar approach combining inno-
vation and fundamental research in the areas of human computer interaction, robotics,
serious games and physiological computing. AHA’s goal is to develop a new genera-
tion of ICT based solutions that have the potential to transform healthcare by optimiz-
ing resource allocation, reducing costs, improving diagnoses and enabling novel ther-
apies, thus increasing quality of life. The project proposes the development and de-
ployment of a novel Robotic Assistance Platform designed to support healthy life-
style, sustain active aging, and support those with motor deficits.
The AHA project will develop a novel and modular set of ICT based solutions that
in isolation or integrated as a Robotic Assistance Platform will address:
- Physical (re)training: Building on the existing expertise on Augmented Reality
(AR) and serious games, we propose to develop adaptive AR physical training
tools that deliver online feedback on performance to prevent sedentarism, sup-
port active aging and provide personalized tools for function re-training in motor
impaired patients.
- Increasing self-awareness: Monitoring of user state by means of biosensors,
computer vision systems and exercise performance data. User state will be as-
sessed in a transparent manner and data will be visualized through friendly user
interfaces, and shared with patients, clinicians and/or relatives.
- Augmented assistance: The above systems will be integrated on a mobile robotic
platform with indoor navigation capabilities (in environments such as senior
houses and hospitals) that will interact through a virtual coach system to assist
patients, provide reminders on tasks, guide patients through exercises, and sup-
port them in daily routines.
These technologies may be very useful in other scenarios, such as those of MOnarCH
project (Multi-Robot Cognitive Systems Operating in Hospitals). This CE FP7 project
is focused on introducing a fleet of social robots that will interact with sick children
and collaborate with medical staff on the pediatric ward of a hospital, the Portuguese
Oncology Institute of Lisbon (IPOL).
1.1 The Need for Robots
There are several scenarios in which robots and augmented reality are very useful in
the two aforementioned environments corresponding to these two abovementioned
projects.
• Teaching, for robots to supporting human teachers by projecting augmented
reality content on a wall or on objects.
• Patient rehabilitation exercises support, by projecting augmented reality con-
tent during physiotherapeutic activities in which the patient receives in real-
time visual feedback and corrective postures
• Information providers, such as projection of AR content informing people that
a new activity is about to start, or calling then with visual signs, or even mov-
ing along with people to places where action is going to take place (e.g. using
projected directional arrows), or informing someone to stop performing an
34
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
34

exercise.
• People protection, such as projecting augmented reality content (for instance a
stop sign) if a person moves into a forbidden zone or door, or performs a for-
bidden rehabilitation exercise or movement
• People entertainment: robots can play games with children or elderly people,
according to content projected into the floor. In another scenario, a patient re-
habilitation can involve game playing (serious games).
Furthermore, robots can perform several supporting activities at home, such as:
• support safe medicine delivery and intake. A robot may carry the medicine,
and at the appropriate time, take it to the patient.
• In addition, the robot may also carry on board medical equipment, such as
thermometer, arterial pressure measurement device, or electrocardiogram
(ECG) equipment, making it available to patients at home.
1.2 Remote Health Assistance
Ageing population has an enormous economic and social impact in a various areas,
especially healthcare systems. Elderly people are more vulnerable to physical or men-
tal impairments, disabilities and chronic illnesses. Falls and problems with muscle
bone can also limit the daily routines. Hence, such problems increase the potential
need for assistance of elderly people.
Patient health monitoring was traditionally done through periodical visits to the
doctor in order to undergo on-site tests for blood pressure, pulse, temperature, or
sugar level. The alternative is stationary monitoring, upon internship at a health care
provider. Currently, patients have the possibility to take home sensors attached on a
belt, usually for a specific time period, to collect biosignal data for that period. How-
ever, the patient still has to move to the health care provider to get the sensor, and
afterwards, he/she has to return to remove the sensor and deliver the data. Nowadays,
we are reaching seamless health monitoring by placing a mobile sensor on the patient,
executing biosignal collection, and transmitting data through a wireless access tech-
nology interface to a storage facility for further medical analysis [1].
On the other hand, medical assistance personnel play a very important role on pa-
tient recovery. In physical therapy, for instance, the therapist helps patients fighting
their pain and recovering from injury. His role is fundamental on therapy planning. In
addition, he not only demonstrates the correct execution procedure for the exercises,
but he also makes sure afterwards the exercises are executed correctly. With this goal
in mind, the therapist can intercede during the session and adapt the exercise schedule
according to the patient’s feedback [2]. However, the patient might perform incorrect
movements at home, without the therapist presence, to avoid pain [3]. Hence, there is
a need to provide assistive solutions that do monitor remotely the patients’ execution
of exercises, but also support, motivate and advise the patient to correctly perform the
exercises. The former is accomplished through biosensors, augmented reality and
haptic technology, that should monitor continuously the patient, transmitting wireless-
ly information concerning its health state and providing feedback. An interacting
mobile robot should provide the patient motivation and guidance.
35
Robotics Enabled Augmented Health
35

1.3 Chapter Structure
This chapter will start by presenting a review of previous relevant literature for aug-
mented health assistance. Afterwards, section 3 overviews the Augmented Human
Assistance project, namely its structure and challenges. Section 4 addresses the de-
sign of robot assistants targeting the AHA project user groups, which will act as nurs-
es for elderly people and patients in recovery of physical injury. It will be also shown
that robotics and augmented reality can provide further functionalities for providing
visual or haptic feedback to users, as described on section 5. Finally, section 6 will
draw the main conclusions, together with directions for future work.
2 Background Review
Various studies show evidence physically active elderly having lower rates of chronic
conditions such as cardiovascular diseases, diabetes, cancer, hypertension and obesity
[4]. There is the need, therefore, to develop solutions that promote healthy habits and
prevent sedentarism. Since chronic patients experience loss of autonomy and low self-
esteem, it is also important to provide assistance to patients with age related chronic
conditions. With these goals in mind, hereafter we overview previous research works
and discuss the most relevant strategies.
2.1 Service Robotics
Research interest in service robotics for active aging and health care has grown in the
last few decades with potential applications on healthy people, elderly, children or
patients. Robotic devices in elderly care [5][6], rehabilitation [7], autism diagnosis
and therapy [8] and weight loss applications [9] have been empirically demonstrated
to be effective. Hence, robotics raised great expectations on the use of robots as per-
sonal assistants. On such robot is the Nursebot platform, able to interact residents,
remind or accompany them of an appointment, as well as provide information of
interest to that person [10].
Intouch Health deployed their robot in a Neurology Intensive Care Unit. A study
suggested improvement in critical care nursing team satisfaction [11]. The robot Paro
in Japan (a robot resembling a baby seal, with expressive eyes) was reportedly able to
improve the mood of elderly people, and simultaneously reduced stress not only to
patients but also to their caregivers [12]. This has been demonstrated more recently to
treat some cases of depression suffered by the survivors of the devastating earthquake
and tsunami in the northeast coast of Japan in March of 2011.
Several solutions employing devices exist to support self-administration of medi-
cine and manage personal medicine administration [13]. The Kompai robot has been
tested for elderly assistance using a diary application for monitoring the medication
and give information about daily events [11]. The autom robot is a weight-loss social
robot [9] that asks questions concerning what a person ate, or how it exercised. It also
provides personalized, helpful suggestions and feedback using facial expressions and
a simple touchscreen interface. In Europe, the EMOTE (Robotic Tutors for Empathy
based Learning) research project explores the usage of social robots for teaching chil-
36
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
36

dren, using the NAO robot. This project has shown that the robot appearance, as well
as its motion, and functionality, plays a very important role on engaging the attention
of the learner [14]. Other authors incorporated the strict functional constraints im-
posed by complex environments (such as hospitals) and specific groups of users, into
the robot design process [15].
2.2 Biomedical Signal Analysis and Human State Estimation
Biomedical signal analysis is nowadays of greatest importance for data interpretation
in medicine and biology, providing vital information about the condition and affec-
tive/emotional states of subjects. In patients with neuromuscular diseases, a constant
monitoring of the patient’s condition is necessary [16]. Heart rate variability, respira-
tion, muscular and electrodermal activity signals are extremely important, since they
indicate when a muscular crisis is occurring.
Tracking devices are important to infer the human state, such as the posture and
motion of the human body during an activity (such as playing a sport or a therapeutic
exercise). Usually, several tracking points are used to represent human body joints
(with respect to both both position and velocity). Cameras have been used to detect
and estimate the pose of human subjects [17] and body parts [18], detect faces [19]
and their expressions [20] and, at a close range, detect eye movement and gaze direc-
tion [19]. Hidden Markov Models have been successfully used in gait recognition
[21].
One approach consists of using anthropometric proportions of human limbs and the
characteristics of gait, to achieve view-independent markerless gait analysis [22].
Microsoft’s Kinect is a markerless tracking device with an acceptable accuracy in
comparison with other motion tracking alternatives [23][24]. It provides full skeleton
tracking at low price. It is also easily portable, especially when compared to other
solutions requiring special equipment (e.g. markers) on the human body. A large
number of applications based on such sensors are addressing some of the difficulties
in unsupervised rehabilitation [25][26]. For instance, Gama et al. [27] proposed a
Kinect based rehabilitation system that tracks user position. The user sees himself on
the screen with overlaying targets representing the desired position. Real-time feed-
back using visual messages is provided in case of incorrect postures.
2.3 Rehabilitation Systems
Various rehabilitation systems have been proposed to improve patient recovery. Many
focus on specific injuries, e.g., stroke [25], or limbs rehabilitation [28][29]. Such
systems may have an important impact on patient’s rehabilitation on an ambulatory
scenario (e.g. at home). Enabling the patient to comfortably exercise at home im-
proves his motivation [25].
A patient’s rehabilitation is affected by exercise repetition, expert feedback, and
patient’s motivation [30]. The repetitive nature of rehabilitation exercises can quickly
become boring for a patient [28][31], therefore, there is a need of turning these exer-
cises into something less tedious. Indeed, successful patient recovery depends on
adherence to the scheduled planning [32].
37
Robotics Enabled Augmented Health
37

Repetitive exercises should be divided into several sub-goals, so the patient
achieves incremental success through each repetition. This improves motivation com-
pared to the approach where success is only achieved after finishing the whole task
[30]. Feedback can be given in two different ways, during the execution (concurrent
feedback) and at the end of exercise execution (terminal feedback) [2]. Concurrent
feedback is given in real-time for offering guidance or corrections in exercise execu-
tion. It allows the patient to have Knowledge of Performance (KP). Terminal feed-
back gives patients only Knowledge of Results (KR), since the patient receives feed-
back after fully executing the task [33][30]. Sigrist [2] suggests a temporal evolution
along the recovery phases. It proposes to gradually reduce KP, giving more emphasis
to KR, to stimulate patient’s autonomy.
2.4 Motor Training on Rehabilitation
The term exergaming is used for gaming approaches that motivate players to engage
in physical activity. Previous research [34] showed evidence that commercial tools
can produce physical, social, and cognitive benefits [35].
Unfortunately, these current tools are not suited to elderly or motor (re)training.
Motor rehabilitation, or motor re-learning, is an extensive and demanding process for
a patient, requiring discipline. Moving injured body parts may produce discomfort or
even significant pain [36]. Physical therapy sessions may be performed several times
both at a clinical and at home, or on either one of them. Later on, the patient might
have to continue therapy exercises at home [37] to avoid suffering a setback on reha-
bilitation [25] (or to decrease recovery time). This requires patients to learn the ap-
propriate recovery exercises. Furthermore, these exercises should be executed correct-
ly, to prevent an aggravation of the injury [3].
Repetition of specific movements is important for rehabilitation, whether at a clinic
or at home [30]. However, this is one of the main causes of deteriorated rehabilitation
at home, since patients tend to get bored and lose focus, due to the repetitive nature of
the task [36]. A mobile robot nurse should play a very important role here in order to
replace the therapist presence to guide and motivate the patient.
2.5 Augmented Reality
Augmented Reality (AR) is considered a promising technology in the rehabilitation
field. Several studies presented evidence for the benefits of employing Augmented
Reality (AR) techniques for supporting functional motor recovery [38], enabling ef-
fective motor training [39]. AR based approaches potentiate the combination of inter-
esting features such as training customization, extended multimodal feedback, quanti-
fiable therapy measures, extra motivation, among others [40].
Interactive AR applications have been proposed for different applications. Shader
Lamps [41] is a seminal work on AR. Its purpose was to augment an existing blank
model with computer-generated graphics to make the model exhibit realistic lighting,
shadow and even animation effects, thus providing it with characteristics previously
inexistent. Dynamic Shader Lamps [42] allows users to interactively change the gen-
erated graphics, and to digitally paint onto objects with a stylus.
38
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
38

There are various spatial augmented reality (SAR) projects with different applica-
tions. iLamp [43] supports SAR by casting the pre-distorted image of virtual objects
from the projector, which can capture the 3D environment based on structured pat-
terns. An interactive SAR system is described in [44] with multiple depth cameras
and a projector. The system detects the information of the surrounding environment
along with the users motion through depth cameras, and displays images on the sur-
face objects in a planar, real world table for the user to interact with. Pixelflex [45]
adopted an array of multiple projectors to make a huge screen space. Automatically
self-configured projectors are able to create a huge projection area.
A projection-based information display system was proposed in [46], which dis-
plays virtual images in a room with a series of sensors. The robot tracks the user
viewpoint with the sensors, and then the robot can generate anamorphic (i.e., projec-
tion format in which a distorted image is stretched by an anamorphic projection lens
to recreate the original aspect on the viewing screen), properly distorted images for
users on flat- surfaces. WARP [47] allows designers to preview materials and finished
products by projecting them onto rapid prototype models. The system uses a standard
graphical interface, with a keyboard and mouse used for user interface. The projection
is not restricted to a fixed area; all feedback is projected onto the tools. Surface Draw-
ing [48] allows a user to sculpt 3D shapes using their hands. Spray modeling [49] uses
a mock-up of a physical airbrush to allow the user to sculpt 3D models by spraying
matter into a base mesh. The system enhances physical tools by projecting status
information onto them allowing the overload of a single tool with several functions.
LightGuide [50] proposed projection mapping onto the user, using his body as a
projection screen. Different type of real-time visual cues are projected onto the user’s
hand to guide him for performing 3D movements. This way, the user is less suscepti-
ble to be distracted by external factors.
3 The Augmented Human Assistance Project
This section described the Augmented Human Assistance project. It is presented the
project structure of partners, its focus areas, as well as the main challenges and ex-
pected impact.
3.1 Project Partners
A consortium of key partners, addressing a large scope of technology fields, forms the
AHA project. IST-ID is the project coordinator. The Computer and Robot Vision Lab
(Vislab) research group at IST/Institute of Systems and Robotics addresses research
on Robotics, Computer Vision, and Cognitive Systems. The Carnegie Mellon Univer-
sity (CMU) team is part of the Quality of Life Technology Centre, at the Robotics
Institute, working on Artificial Intelligence and Human Computer Interaction. The M-
ITI NeuroRehabLab at University of Madeira addresses Serious Games, Interactive
Technology, and Rehabilitation. Two groups are specialized on biosignals data acqui-
sition and processing. The team at FCT/UNL works on Signal Processing, Machine
Learning, and Electrophysiology. And PLUX Biosignals, a company that creates
innovative solutions for Sports, Healthcare and Research, by integrating biosignals
39
Robotics Enabled Augmented Health
39
processing and miniaturized wireless sensor devices. YDreamsRobotics is another
company specialized in robotics, mechatronics and the internet of things, which is
addressing Augmented Reality, Robotics Design, and Haptic Feedback, for building a
therapeutic robot and for providing patient feedback through actuation. Finally, the
Interdisciplinary Centre for the Study of Human Performance (CIPER) at Faculdade
de Motricidade Humana (FMH) is specialized in the main areas addressed by the
project, namely Sports Science, Therapeutic exercises, and Human Function and Per-
formance.
The project targets three main environments (clinical, sports, and home assistance),
as described in the next subsection. Supporting external partners collaborate by
providing solution requirements, on-going feedback, as well as facilities for empirical
evaluation, as described in Table 1.
Table 1. External partners and their focus areas on the project.
Area External partners
Rehabilitation
HealthSouth of Sewickley
Clinical Physiology Translational Unit, IMM
Sports
Associação da Madeira de Desporto Para Todos
Via Activa Animação Turistica
Elderly
Comfort Keepers
Public Administration
Camara Municipal da Ponta do Sol
3.2 Project Focus Areas
The AHA project addresses three main target groups, as shown in Fig. 1. The Elderly
People group, addressed both on a clinical setting as well as at home. The goal is to
enable simultaneously sustainable care and active aging. New technologies are pro-
posed, such as medicine and medical equipment delivery by a mobile robot, and re-
mote assistance on therapeutic exercises using multimodal feedback and augmented
reality. Remote assistance on therapeutic exercises is also proposed for a second tar-
get group, those with motor deficits. Serious games, emotional and haptic feedback,
are among the technologies proposed to support patients on their recovery. Finally,
the project addresses sports for supporting a healthy lifestyle. It aims to improve ath-
letes’ performance, and to facilitate their learning, training and performance evalua-
tion using new technologies.
Fig. 1. User groups targeted by AHA: patients, athletes, and elderly people.
40
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
40

The three main target environments, namely clinical, sports facility, and home assis-
tance at a senior house, have different characteristics.
The clinical environment is more accessible but it is often a more complex envi-
ronment. A virtual coach module is proposed to interact with the patient, guiding him
throughout the exercises and providing positive and corrective feedback.
Sports facility is characterized by large indoor open spaces where robot navigation
is facilitated. The Robotic Assistance Platform will be able to identify an adequate
surface for the projection of the Augmented Reality Training Games, and provide its
users with the gaming training experience. Users will be able to challenge remote
users to a competitive game, while playing the training games.
At a senior house, the Robotic Assistance Platform will visit some of the residents
at specific times. The robot reminds the elder about the pills he needs to take, and also
asks him to take heart rate measurements with the on board sensors of the robot. Fur-
thermore, it will help the elder through his/ her gaming exercises, and it will provide a
feedback summary on performance, making this information also remotely available
to their clinicians.
3.3 Innovations and Impact
The AHA project proposes the development of novel robotics assistive platforms for
health exercise program management. Several functionalities will be provided, such
as user engagement, execution monitoring, and supporting therapists in patients’ re-
habilitation tasks. These functionalities will be developed considering the target user
groups, with the aim to promote a healthy lifestyle, a sustainable active aging of the
population, and supporting those with motor deficits. This should be accomplished
using several interdisciplinary technologies, and combining these in innovative ways.
For instance, it is proposed advanced “exergaming” and assistive technologies based
on human-computer interaction, robotics, serious games, multimodal sensing, physio-
logical computing, among other fields. The goal is to employ technology to help to
prevent sedentarism related diseases, to facilitate therapy of chronic conditions related
to aging and rehabilitation of motor deficits. Therefore, the project will tackle users
with special needs, focusing on elderly and patients with motor deficits, as well as on
athletes. It will provide customization and personalized tools for increasing motiva-
tion and engagement, using augmented reality, online feedback, gamification, social
networking, and interactive interfaces. It is also proposed a better measurement and
monitoring of user condition through multi-modal sensing (biosensors, computer
vision) and multi-modal feedback (haptic devices, sound feedback, augmented reali-
ty). Augmented assistance will be provided by a nurse mobile robotic platform, to-
gether with virtual coaching, for guiding patients in their exercises and daily routines.
The project also proposes to support clinicians through personalized user profiles and
advanced display of information.
The project outcomes aim to impact significantly different entities:
• Society: Reduce effects of sedentarism related diseases and aging conditions.
• Elderly: Increase physical fitness, independence, autonomy, self-esteem.
• Patients: Can exercise independently at home, adherence to schedule.
• Clinicians: Follow patient progress remotely, customize therapies.
41
Robotics Enabled Augmented Health
41
• Science & Technology: New algorithms and systems for eHealth technologies.
• Education: Formation of highly skilled human resources in close cooperation
with technology integrators and end-users.
• Companies: Close to market technologies; large exploitation opportunities.
3.4 WorkPlan
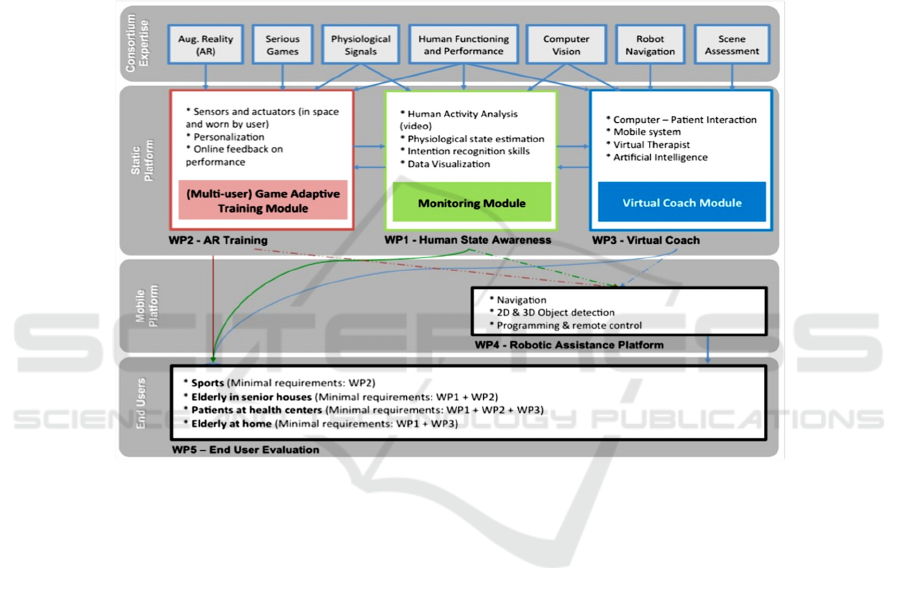
AHA project work plan is shown in Fig. 2. It represents the platforms, the modules to
be integrated on them, as well as the interactions among modules.
Fig. 2. Project workplan according to the different workpackages.
Human State Estimation (WP1) employs state of the art wearable technology and
training, for the integration of vision based activity monitoring and emotion detection
modules into a core technological and scientific component of the Robotic Assistant
Platform - the human monitoring module. Augmented Reality Training (WP2) inte-
grates AR technology that will serve as the basis for the development of a set of novel
serious games for physical training. Integration of Virtual Coaches (WP3) on a physi-
cal context is aimed for the improvement of the quality of life of those with special
needs. It includes (see fig. 3) user interaction aspects of the system, as well as interac-
tions of the virtual coach and the human monitoring modules. Robotic Assistance
Platform (WP4) consists of the sensing and software robot architecture. It includes
integration of the monitoring, AR training, and virtual coach modules into the final
Robotic Assistive Platform. User evaluation (WP5) will consist of the solution’s ex-
perimental validation with real data on a clinical context.
42
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
42
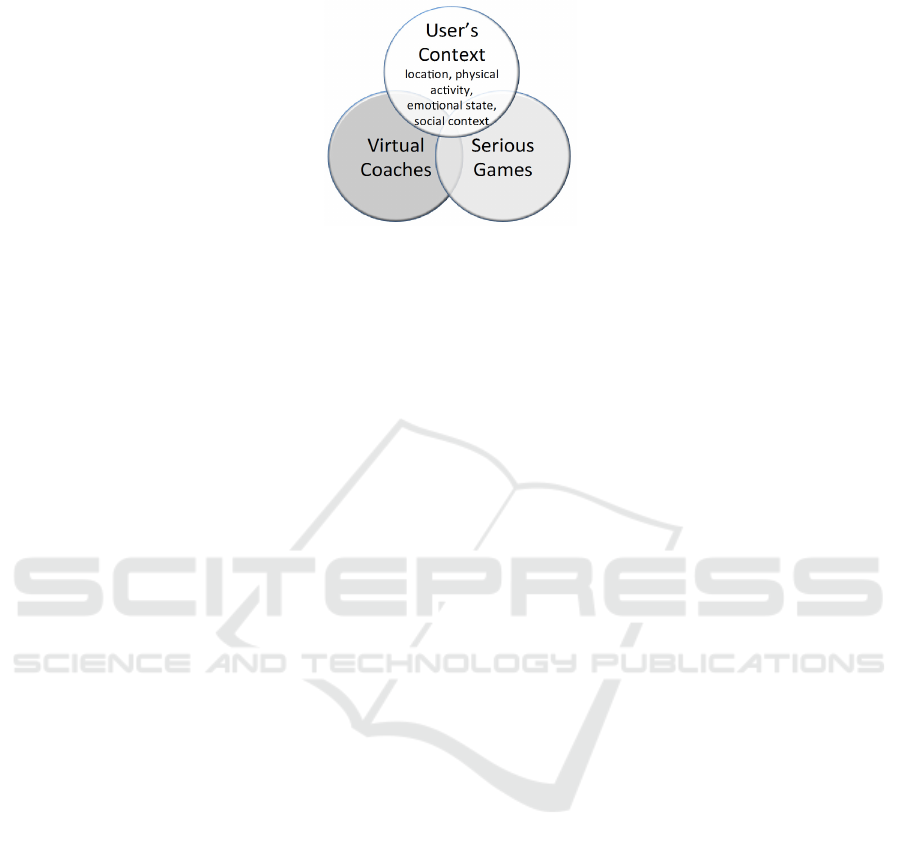
Fig. 3. Integration of interdisciplinary technologies on the AHA project.
4 Robot Design for Human Augmented Assistance
Recently, there is a trend for bringing robots into operations among people, helping
people. Elderly people, athletes and patients constitute challenging groups for robot
interaction. Addressing athletes’ needs is challenging due to their energy and high
performance requirements. Elderly people and patients pose strong safety concerns.
These challenges need to be tackled on the design process. This is essential for the
robots to be able to operate safely, while interacting socially with people.
Gonçalves and Arsenio [15] proposed a formal design process for building socially
interacting robots within a group of children with special needs in a hospital environ-
ment. The design takes into consideration the input of the project partners. This is
incorporated on the robot specifications during the development process. Robots de-
sign needs to account with several security factors. Under the scope of the AHA pro-
ject, we have been applying this process to the design of mobile robots targeting new
user groups. This “nurse” mobile robot, although posing similar challenges as the
ones described by Gonçalves and Arsenio [15], also adds new requirements. Elderly
people, athletes and patients poses specific requirements that often differ from those
for children in hospitals. Concerning security factors and human-robot interaction
features (see Fig. 4):
• Sick children often carry medical equipment carried, like wheeled structure to
carry serum bags. This still applies to some groups of elderly people. It may also
apply in less extent to patients on recovery from physical injury.
• No sharp surfaces that may cause injury to children. Although a less stringent
requirement for elderly people and patients, it is still an important issue.
• Avoid geometries that may invite children to step up the vehicle or insert fingers
on holes. This is not relevant for the group of users under consideration.
• Emotional expressions and engagement behaviors. A nurse robot targeting adults
should pose a professional stance, compared to a more character like concept for
children.
• Avoid inspiring fear and disgust: should instead induce comfort and trust, which
applies for all user groups (except in specific niches, such as military)
• An appealing aesthetics to children often has a different meaning than for an
adult.
43
Robotics Enabled Augmented Health
43
Fig. 4. Comparative analysis of security factors and human-robot interaction features, for ro-
bots to interact with children versus elderly people.
4.1 Shell Development Process
The shell development process is divided into several stages, and here briefly re-
sumed. It started by an analysis of the environment and the way elderly people, ath-
letes and patients should interact with the robots. At this stage we also performed
research related to existing robots, and “soft” and “clean” materials prone to be used
at clinical, hospital and sport facilities. With this information we concluded that
rounded shapes, soft materials, and neutral, light colors should be used, together with
active colors (red) on very small information symbols.
Different options were analyzed taking into account aesthetic properties, emotional
feelings provoked by the robot, its the actual expression, feasibility constraints and
functionality inherent to the robot, so that it could perform the envisioned tasks.
Afterwards, the material developed so far became the basis for the CAD model de-
velopment. The CAD model and photo-real imagery was also developed taking into
account the different production methods available, the assembly procedure, the
maintenance operations, the cost involved, and of course the aesthetics and functional
requirements defined at the early stages.
4.2 Operational Environment Analysis
The shell development process started by performing an analysis of the environments
where the robots will operate, including the deployment space, targeted groups of
people, and tasks to be executed by the robot, in order to define a set of features tak-
ing references on other existing and relevant systems.
The features to apply include rounded shapes and soft touch feeling materials, due
to the danger of fall by elderly people or patients recovering from physical injury.
This issue is also present in sport facilities due to high energy placed into activities.
The robots were given a dynamic stance, although this requirement has much more
relevance on sport facilities than on the senior houses or hospital/clinical environ-
ments.
The features to avoid include mechanical type shapes, which are more aggressive,
and not appealing for the target user groups. Exposed components, salient from the
robot body, are potentially dangerous and should be avoided as well. Robots outfit
Consider medical equipment carried out by elderly
Avoiding sharp features that may cause harm for elderly
step up the vehicle or insert fingers on holes.
special handles on the robots for guiding elderly people,
helping them moving around.
• Human-robot Interactions
emotional expressions
inspiring comfort and trust
playful aspects.
• The aesthetics must now be appealing to elderly people,
taking references on a professional therapeutic or a butler.
44
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
44

should inspire users for interacting with them.
4.3 Ergonomics and Human Factors
Lets now consider the ergonomics and user factors, since problems can arise from bad
positioning and dimensioning of the robot components.
According to Fig. 5, we opted for: i) a non-threatening overall stance; ii) no arms;
iii) touch screen for better conveying user feedback, as well as to provide a simpler
user interface for elderly people.
Fig. 5. Mobile robot platform – the nurse.
Similarly to the Monarch robots (see Fig. 6), these should have a modern and cool
appearance. And since they operate in a hospital setting, there is a preference for
lighter colors (such as white color, common in hospitals), since it is easier to identify
dirty surfaces on robot and to clean them. Contrary to the Monarch robots, there is no
multifunctional face on the nurse robots.
Fig. 6. Mobile robot platform for children at hospitals, developed under the Monarch project
[15]. In contrast to the professional look and feel for the nurse robot, the monarch robots are
character-like, but not resembling any particular known artificial character.
5 Assistance Robotics for Augmented Health
Novel approaches have taken Augmented Reality (AR) beyond traditional body-worn
or hand-held displays, pushing such capabilities into mobile robots [51]. Spatial
Augmented Reality (SAR) uses digital projectors to render virtual objects onto 3D
45
Robotics Enabled Augmented Health
45
objects located in the robot’s navigation environment. When mounting digital projec-
tors on robots, this collaboration paves the way for unique Human-Robot Interactions
(HRI) that otherwise would not be possible. This is especially useful for supporting
patients performing recovery exercises, or for providing additional information to
elderly people (e.g. time for medicine intake).
5.1 Augmented Reality for Robotic Assistants
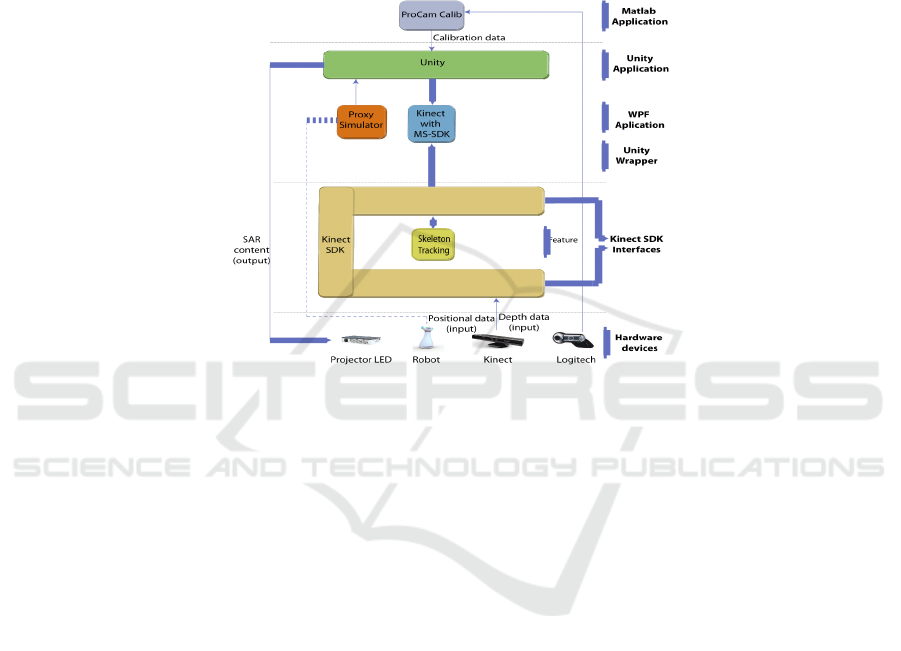
Fig. 7. Architecture of the proposed solution. The line in dash represents the connection to the
mobile robot localization system.
The architecture for SAR enabled robots is represented in Fig. 7. It is comprised of six
main categories:
• The hardware includes a projector, a camera, and a Kinect depth camera for hu-
man-robot interactions;
• The Kinect SDK interface, which allows direct access to Kinects RGB and depth
sensors. One of Kinects’ key features we used was skeleton tracking;
• Unity wrapper, which enables the use of Kinect SDK internal functions within
Unity;
• A Windows Presentation Foundation application (WPF) was developed in order
to simulate positional information retrieved from a robot localization system;
• Unity, the game engine on top of which the main applications were developed;
• The camera-projector calibration application, which makes use of ProCamCalib,
developed on Matlab.
A collection of modules (given by a series of scripts in Unity) were designed to per-
form specific tasks:
• Homography matrix update: updates the matrix associated with each projection
scene and apply that transformation in OpenGL’s vertex pipeline;
• Tracking: Controlling each projection surface position in the virtual scene;
• Intrinsic Setting: Alters Unity’s default projection matrix so that the values ob-
tained from the projection calibration process can be properly applied;
46
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
46
• Update Unity’s camera position: based on localization (position/pose)
information provided by an exterior application (on the robot or elsewhere);
• Save and load: of projection surface positional data from an XML file;
• Human-Robot Virtual Interface (HRVI): Updates the game logic of an
interactive AR game based on input received from Kinect’s skeleton tracking
information.
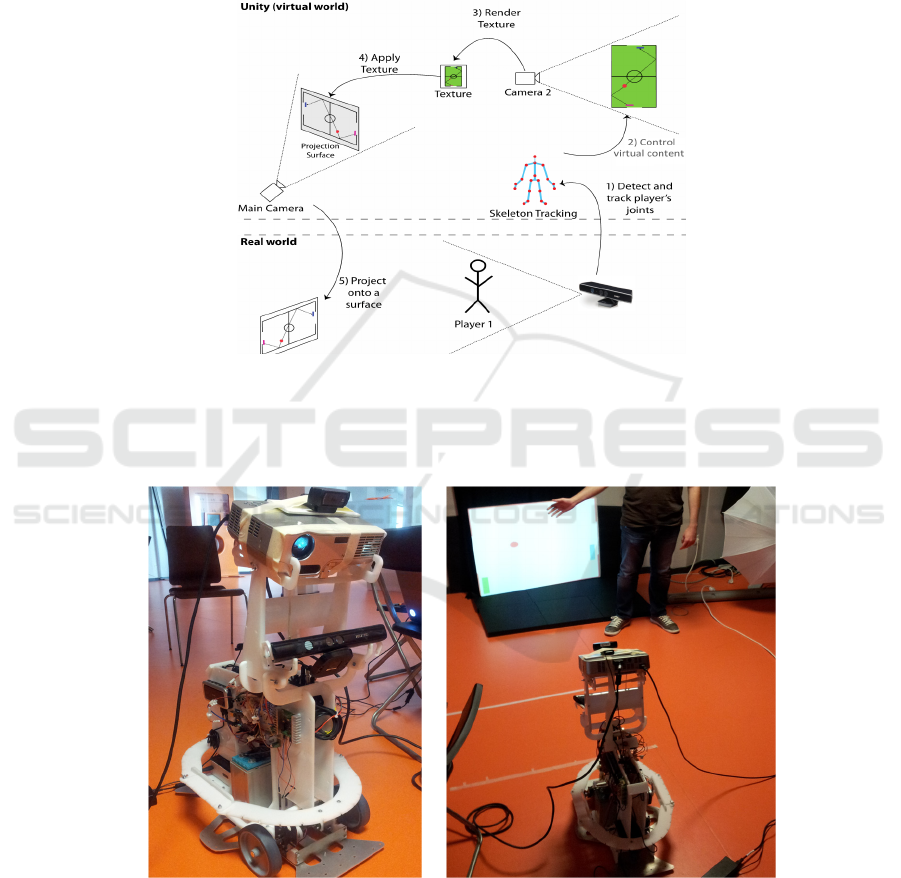
Fig. 8. Human interactions. One or two humans are tracked simultaneously using Kinect’s
skeleton tracking (step 1). The corresponding joint, for each player, controls the respective
virtual object (step 2). Camera 2 renders the texture containing the view of the camera (step 3)
that is then applied to one of the projection surfaces and updated in runtime (step 4). The final
step can now take place: project onto one real world surface (step 5).
Fig. 9. Augmented reality on Wheels – Content is projected onto multiple surfaces in order to
help user perform actions, or to play games with users (such as the Air Hockey game, as shown
in the right image).
47
Robotics Enabled Augmented Health
47
The goal is to project augmented reality content according to objects physics, or other
entities. As such, we introduce the human interactions feedback in order to adapt the
augmented reality content, and to achieve virtual-real objects integrated behavior, as
represented in Fig. 8.
Hence, the application integrates augmented reality information, with projection
distortion compensation, and human gestures recognition to enable interactions be-
tween people and undistorted augmented reality content. Virtual content is projected
onto the real world where humans interact with such content through movements (see
Fig. 9), as detected by Microsoft Kinect’s skeleton tracking feature.
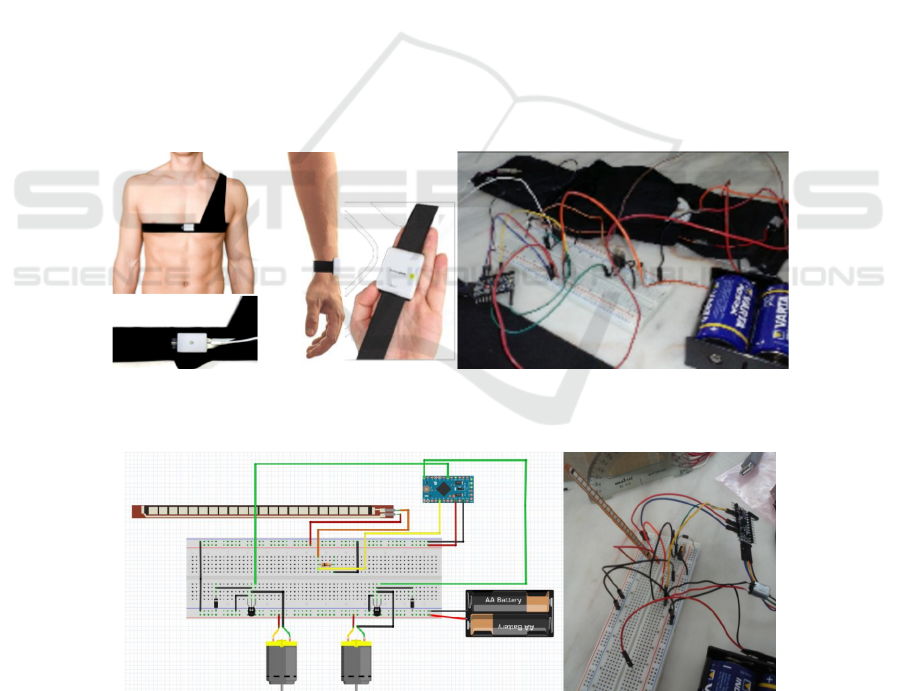
5.2 Haptic Feedback
The AHA project is also investigating the usage of robotic elements, behind the nurse
mobile robot. Besides biosignal sensors on the human body (see Fig. 10a), actuators
are being investigated to provide real-time feedback concerning movements to be
executes, or corrections to imperfections on the execution of the exercises. Such actu-
ators include an elastic sleeve (see Fig. 10b), enabled with a sensor to measure joint
rotation and an array of motors to provide haptic feedback.
Currently two sensors have been tested: a Flex Sensor (see Fig. 11), a flexible strip
that senses rotation, as well inertial sensor based on gyroscope and accelerometer.
Other devices are planned to be tested, such as mobile phone gadgets (like Pebble),
that are able to generate controlled vibrations.
a) b)
Fig. 10. a)Biosignal sensing devices, to acquire data concerning biological variables on the human
body; b)Elastic sleeve prototype with a SensorFlex and two vibration motors for haptic feedback.
Fig. 11. Prototype schematics and testing, using a Flex sensor and two motors.
48
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
48

6 Conclusions and Discussion
This chapter presented some of the robotics technologies being developed for Aug-
mented Health Assistance, under the scope of the AHA project.
It has been shown that one of the problems with remote rehabilitation is the correct
execution of recovery exercises by the patient. Furthermore, due to the repetitive
nature of such movements, there is consequently a motivation problem for keeping
the patient engaged with the exercise program. The first issue can be addressed by the
usage of augmented reality and haptic feedback for providing corrective feedback to
the patient. The later issue can be addressed employing nurse robots. These replace
the role of the human therapeutic on providing advice and motivation. The nurse
robot also plays a very important role on supporting elderly people on their daily
activities. For instance, these robots can take medicine to elderly at intake times, or
make available medical equipment.
The AHA project proposed to develop new algorithms, and virtual as well as robot-
ic systems for eHealth technologies. It expects to have a significant impact on the
health and sport sectors, by employing interdisciplinary technologies at the service of
elderly, athletes and patients with physical injury (both at home or on a clini-
cal/hospital environment). Innovative approaches will bring benefits to society, by
reducing negative effects of sedentarism, such as related diseases and aging condi-
tions. It proposes as well to improve the quality of life of elderly people. Besides
developing a mobile robot acting as a companion nurse to elderly (reducing the prob-
lem of elderly isolation and loneliness), it also aims to increase elderly physical fit-
ness, independence from human nurses and family, and consequently improving their
autonomy and self-esteem.
Concerning patients in recovery of physical injuries, the AHA project proposes to
improve these patients quality of life. This is acomplished by enabling them to per-
form independently exercises at home, while receiving corrective feedback and moti-
vational incentive to adhere to scheduled exercises.
The project promotes however to keep clinicians in the loop (even remotely) to fol-
low patient progress. The clinician is also able to customize patients therapies, as well
as to provide of-line, or real-time, corrections to therapies or exercise execution.
The combination of a large set of interdisciplinary technologies is expected to ena-
ble a new level of health assistance to different user groups, improving their quality of
life and reducing government economic burden.
Acknowledgements. This work has been funded by CMU-Portuguese program
through Fundação para a Ciência e Tecnologia, project AHA-Augmented Human
Assistance, AHA, CMUP-ERI/HCI/0046/2013.
References
1. Arsenio, A., Andrade, J., Duarte, A.: Non-invasive Wireless Bio Sensing. Accepted for
publication at Lecture Notes in Computer Science, series Communications in Computer and
Information Science (CCIS), Springer-Verlag (2015)
2. Sigrist, R., Rauter, G., Riener, R., Wolf, P.: Augmented Visual, Auditory, Haptic, and multi-
modal feedback in motor learning: A review. Psychonomic bulletin & review 20, 1
49
Robotics Enabled Augmented Health
49

(Feb. 2013), 21–53
3. Tang, R., Alizadeh, H., Tang, A., Bateman, S., Jorge, J. Physio@Home: design explora-
tions to support movement guidance. CHI ’14 Extended Abstracts on Human Factors in
Computing Systems (2014)
4. World health statistics 2012. World Health Organization, 2012
5. Bemelmans, R., Gelderblom, G., Jonker, P., de Witte, L.: Socially assistive robots in elder-
ly care: A systematic review into effects and effectiveness. Journal of the American Medi-
cal Directors Association 13.2 (2012), 114-120
6. Broekens, J., Heerink, M., Rosendal, H.: Assistive social robots in elderly care: a review.
Gerontechnology 8.2 (2009), 94-103
7. Matarić M., Eriksson J., Feil-Seifer D.: Socially assistive robotics for post-stroke rehabilita-
tion. Journal of Neuro Engineering and Rehabilitation 4.5 (2007)
8. Scassellati, B.: How social robots will help us to diagnose, treat, and understand autism.
Robotics research. Springer Berlin Heidelberg, (2007), 552-563
9. Cory, K., Breazeal. C.: Robots at home: Understanding long-term human-robot interaction.
IEEE/RSJ IROS International Conference on Intelligent Robots and Systems, IEEE (2008)
10. Pineau, J., Montemerlo, M., Pollack, M., Roy, N., Thrun, S.: Towards robotic assistants in
nursing homes: Challenges and results. Special issue on Socially Interactive Robots, Robot-
ics and Autonomous Systems 42.3 (2003), 271-281
11. Rincon, F., Vibbert, M., Childs, V., Fry, R., Caliguri, D., Urtecho, J., Rosenwasser, R.,
Jallo, J.: Implementation of a model of robotic tele-presence (RTP) in the Neuro-ICU: ef-
fect on critical care nursing team satisfaction. Neurocritical care 17.1 (2012), 97-101
12. Wada, K., Shibata, T.: Robot Therapy for Elders Affected by Dementia. Engineering in
medicine and biology magazine, 27 (2008), 53–60
13. Wong, B., Norman, D.: Evaluation of a Novel Medication Aid, the Calendar Blister-pak,
and its effect on drug compliance in a geriatric outpatient clinic. Journal of the American
Geriatrics Society (1987)
14. Castellano, G., Paiva, A., Kappas, A., Aylett, R., Hastie, H., Barendregt, W., Nabais, F.,
Bull, S.: Towards Virtual and Robotic Empathic Tutors. 16
th
International Conference on
Artificial Intelligence in Education (AIED’13), Memphis, USA. In H.C. Lane & K. Yacef
(eds), Artificial Intelligence in Education Springer-Verlag, Berlin Heidelberg (July 2013)
15. Gonçalves, D., Arsenio, A.: Human-driven multi-robot design process for social interac-
tions with children on complex environments. 2015 6
th
International Conference on Auto-
mation, Robotics and Applications (Feb. 2015), 70–76
16. Pinto, A., Almeida, J., Pinto, S., Pereira, J., Oliveira, A., de Carvalho, M.: Home telemoni-
toring of non-invasive ventilation decreases healthcare utilisation in a prospective con-
trolled trial of patients with amyotrophic lateral sclerosis. Journal of Neurology, Neurosur-
gery & Psychiatry (2010)
17. Lim, J., Zitnick, C., Dollár, P.: Sketch Tokens: A Learned Mid-level Representation for
Contour and Object Detection. CVPR, Portland, Oregon (2013)
18. Girshick, R., Felzenszwalb, P., Mcallester, D.: Object detection with grammar models."
Advances in Neural Information Processing Systems (2011)
19. Arsenio, A.: Cognitive-developmental learning for a humanoid robot: a caregiver's gift.
MIT. PhD thesis (2004)
20. Yang, Y., Ge, S., Lee, T., Wang, C.: Facial expression recognition and tracking for intelli-
gent human-robot interaction. Intelligent Service Robotics 1.2 (2008), 143-157
21. Saponaro, G., Salvi, G., Bernardino, A.: Robot Anticipation of Human Intentions through
Continuous Gesture Recognition, CR-HRI (2013)
22. Goffredo, M., Seely, R., Carter, J., Nixon, M.: Markerless view independent gait analysis
with self-camera calibration, In Proceedings of International Conference on Automatic Face
and Gesture Recognition (2008)
23. Chang, C., Lange, B., Zhang, M.: Towards Pervasive Physical Rehabilitation using
Microsoft Kinect. 6
th
International Conference on Pervasive Computing Technologies for
50
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
50

Healthcare (PervasiveHealth) (2012), 159–162
24. Scano, A., Caimmi, M., Malosio, M., Tosatti, L.: Using Kinect for upper-limb functional
evaluation in home rehabilitation: A comparison with a 3D stereoscopic passive marker
system. 5
th
IEEE RAS/EMBS International Conference on Biomedical Robotics and Bio-
mechatronics (Aug. 2014), 561–566
25. Borghese, N., Mainetti, R., Pirovano, M., Lanzi, P.: An intelligent game engine for the at-
home rehabilitation of stroke patients. IEEE 2
nd
International Conference on Serious Games
and Applications for Health (SeGAH) (May 2013), 1–8
26. Kitsunezaki, N., Adachi, E., Masuda, T., Mizusawa, J.: KINECT applications for the physi-
cal rehabilitation. IEEE International Symposium on Medical Measurements and Applica-
tions (MeMeA) (May 2013), 294–299
27. Gama, A., Chaves, T., Figueiredo, L., Teichrieb, V.: Guidance and Movement Correction
Based on Therapeutics Movements for Motor Rehabilitation Support Systems. 14
th
Sympo-
sium on Virtual and Augmented Reality (May 2012), 191–200
28. Burke, J., McNeill, M., Charles, D., Morrow, P., Crosbie, J.,McDonough, S. Serious
Games for Upper Limb Rehabilitation Following Stroke. Conference in Games and Virtual
Worlds for Serious Applications (Mar. 2009), 103–110
29. Sadihov, D., Migge, B., Gassert, R.: Prototype of a VR upper-limb re-habilitation system
enhanced with motion-based tactile feedback. World Haptics Conference (WHC) (Apr.
2013), 449–454
30. Schonauer, C., Pintaric, T.: Full Body Interaction for Serious Games in Motor Rehabilitation.
Proceedings of the 2
nd
Augmented Human International Conference, ACM Press (2011), 1–8
31. Rego, P., Moreira, P., Reis, L.: Serious games for rehabilitation: A survey and a classification
towards a taxonomy. 5
th
Iberian Conference on Information Systems and Technologies
(CISTI 2010).
32. Adherence to long-term therapies: evidence for action. World Health Organization (2003)
33. Huang, H., Ingalls, T., Olson, L., Ganley, K., Rikakis, T., He, J.: Interactive multimodal
biofeedback for task-oriented neural rehabilitation. 27
th
Annual International Conference of
the Engineering in Medicine and Biology Society, IEEE-EMBS (2005), 2547–2550
34. Garn, A., Baker, B., Beasley, E., Solmon, M.: What are the benefits of a commercial exer-
gaming platform for college students? Examining physical activity, enjoyment, and future
intentions. Journal of physical activity & health 9.2 (2012), 311-8
35. Staiano, A., Calvert, S.: Exergames for physical education courses: Physical, social, and
cognitive benefits. Child Development Perspectives 5.2 (2011), 93- 98
36. Singh, A., Klapper, A., Jia, J.: Motivating people with chronic pain to do physical activity:
opportunities for technology design. Proceedings of the SIGCHI Conference on Human
Factors in Computing Systems (2014), 2803–2812
37. Lohse, K., Shirzad, N., Verster, A.: Video Games and Rehabilitation: Using Design Princi-
ples to Enhance Engagement in Physical Therapy. Journal of Neurologic Physical Therapy
37, 4 (Dec. 2013), 166–75
38. Laver, K., George, S., Thomas, S., Deutsch, J., Crotty, M.: Cochrane review: virtual reality
for stroke rehabilitation,” Eur J Phys Rehabil Med, 48.3 (Sep. 2012), 523–530
39. Cameirão, M., Bermúdez, S., Verschure, P.: Virtual reality based upper extremity rehabili-
tation following stroke: A review. Journal of CyberTherapy & Rehabilitation, 1.1 (2008)
40. Lucca, L.: Virtual reality and motor rehabilitation of the upper limb after stroke: a genera-
tion of progress?. Journal Rehabilitation Medicine, 41.12 (Nov. 2009), 1003–1100
41. Raskara, R., Ziegler, R., Willwacher, T.: Cartoon dioramas in motion. Proceedings of the
2
nd
international symposium on non-photorealistic animation and rendering (2002), 7-13
42. Bandyopadhyay, D., Raskar, R., Fuchs, H.: Dynamic Shader Lamps: Painting on Movable
Objects. IEEE/ACM international symposium on mixed and augmented reality (2001)
43. Raskar, R., van Baar, J., Beardsley, P., Willwacher, T., Rao, S., Forlines, C.: iLamps: Geo-
metrically Aware and Self-Configuring Projectors. ACM Transactions on Graphics (TOG),
ISSN: 0730-0301, 22.3 (July 2003), 809-818
51
Robotics Enabled Augmented Health
51

44. Wilson, A., Benko, H.: Combining Multiple Depth Cameras and Projectors for Interactions
On, Above, and Between Surfaces. In Proceedings of ACM UIST '10 (2010), 273-282
45. Yang, R., Gotz, D., Hensley, J., Towles, H., Brown, M.: Pixelflex: A reconfigurable multi-
projector display system. Proceedings of the conference on Visualization (2001), 167-174
46. Azuma, K., Miyashita, S.: Anamorphosis Projection by Ubiquitous Display in Intelligent
Space. Proc. int. conf. universal access in human-computer interaction (2009), 209–217
47. Harris, C.: Tracking with rigid models. In Active vision, MIT Press Cambridge, MA, USA
(1993), 59-73
48. Schkolne, S., Pruett, M., Schröder, P.: Surface drawing: creating organic 3D shapes with
the hand and tangible tools. Proceedings of SIGCHI Conference on Human Factors in
Computing Systems (2001), 261–268
49. Jung, H., Nam, T., Lee, H., Han, S.: Spray modeling: Augmented reality based 3D model-
ing interface for intuitive and evolutionary form development. Proceedings of the Interna-
tional Conference on Artificial Reality and Telexistence (2004)
50. Sodhi, R., Benko, H., Wilson, A.: LightGuide: projected visualizations for hand movement
guidance. Proceedings of the SIGCHI Conference on Human Factors in Computing Sys-
tems (2012)
51. Costa, N., Arsenio A.: Augmented Reality behind the wheel - Human Interactive
Assistance by Mobile Robots. 6
th
International Conference on Automation, Robotics and
Applications (Feb. 2015), 63 - 69
52
EPS Lisbon January 2015 2015 - European Project Space on Intelligent Systems, Pattern Recognition and Biomedical Systems
52
