
Assessment of Hand Rehabilitation after Hand Surgery
by Means of a Sensory Glove
Giovanni Saggio
1
, Laura Sbernini
1
, Anna De Leo
2
, Mostafa Awaid
3,4
,
Nicola Di Lorenzo
3
and Achille L. Gaspari
3
1
Department of Electronic Engineering, University of Rome Tor Vergata, Via del Politecnico 1, 00133 Rome, Italy
2
Plastic surgery department, John Radcliffe hospital, Oxford university hospitals, Oxford, U.K.
3
Department of Experimental Medicine and Surgery, University of Rome Tor Vergata,
Via Montpellier 1, 00133 Rome, Italy
4
Department of Biomedical Engineering, Higher Technological Institute, 10
th
of Ramadan City, 44135 Egypt
Keywords: Sensory Glove, Hand Rehabilitation, Range of Motion (ROM).
Abstract: The assessment of hand functions after hand surgery treatment is essential to address the optimal rehabilitation
procedures for any patient. To this aim, the current procedures anachronistically rely mainly on manual
goniometers (highly prone to human errors) and know-how of experienced medical staffs (potentially prone
to biased judgment), so that there is room for improvements in objective measurements of hand capabilities
and new technological systems are very welcome. In particular, systems based on sensory glove are gaining
more and more relevance in acquiring hand movement capabilities. Within this frame, in this research the
Range of Motion (ROM) for all fingers and the ability of participants (health vs. patient subjects) to repeat
two ADL (Activities of Daily Living)-based tasks were investigated. As a result, the glove-based system was
evaluated in its feasibility for the assessment of hand function in clinical practice and rehabilitation settings.
1 INTRODUCTION
Hands are fundamental for human body beings in a
huge number of tasks in our everyday life, for self-
caring, acting, expressing, signing etc. (Chen et al.,
2010). This is why, the correct measure of finger
movements can be fundamental in assessing deficits
after injuries of the central nervous system (Gentner
and Classen, 2009), and/or in evaluating the outcome
of hand surgery, so to dispense appropriate
rehabilitation strategies in restoring patients’ abilities
(Borghetti et al., 2013).
Joint range of motion (ROM) measurement is one
of the most important quantitative methods of hand-
function evaluation (Dipietro et al., 2003). Mechanical
goniometers or, more recently, potentiometric- and
electro- goniometers are traditionally used to measure
the passive ROM of each finger joint. The “small”
dimension of finger segments, compared to the
dimensions of the goniometers, makes difficult the
simultaneous measure of the entire finger ROMs
(Carpinella et al., 2006). Therefore, recently other
techniques have been considered, based on optical
technology, such as the analysis of digital
photographic images (Vergara et al., 2003) and the
multi-camera photogrammetry (Lee and Rim, 1991).
These solutions represent improvements, but are
limited only to static measurements. Dynamic and
simultaneous measures are allowed by an
optoelectronic analysis, but the necessary optical
markers are prone to problems of occlusion, low
ambient illumination can affect the result, and the high
equipment cost do not favor their clinical acceptance.
Systems based on sensory glove can represent an
interesting alternative within this frame; this is why
we intend to evaluate their feasibility (Saggio et al.,
2014). Data recorded by means of a sensory glove can
even furnish the possibility to drive an avatar of the
hand, so to replicate the hand movements for further
analysis (Saggio et al., 2009).
By means of a custom made sensory glove, we
investigated all joint finger ROMs, and the ability of
healthy and patient subjects to repeat gestures in
performing two easy grasping tasks.
Saggio, G., Sbernini, L., Leo, A., Awaid, M., Lorenzo, N. and Gaspari, A.
Assessment of Hand Rehabilitation after Hand Surgery by Means of a Sensory Glove.
DOI: 10.5220/0005704201870194
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 1: BIODEVICES, pages 187-194
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
187

2 MATERIALS AND METHODS
2.1 Sensory Glove
Typically, a sensory glove is a cloth glove equipped
with flex sensors (Saggio, 2012). It was proposed for
semi-automated goniometry in order to address the
shortcomings of passive measures and to explore
functional activities (Dipietro et al., 2003; Williams et
al., 2000). Different types of sensory glove have been
proposed, both commercial and research ones.
To best fit our requirements, we developed two
twin indigenously-made sensory gloves (small and
medium sized), equipped with 14 resistive flex sensors
(by Flexpoint Sensor Systems, Inc., Draper, UT)
placed in correspondence of the interphalangeal (IP)
and metacarpophalangeal (MCP) joints of the thumb,
and distal interphalangeal (DIP), proximal
interphalangeal (PIP) and metacarpophalangeal (MCP)
joints, to trace finger flex/extension movements (see
Figure 1). When a sensor is bent, its resistance value
increase proportionally to the bending angle (Saggio,
in press).
Analog signals from the glove fed an ad-hoc
realized electronic circuitry, which send processed
data to a personal computer moving a hand avatar
according to the measures.
2.2 Participants
A group of 11 subjects without hand abnormalities, 9
healthy (6 women and 3 men) averaging 26 years in
age (range 24-32y) and 2 patients (2 women, 17 and
65y respectively), performed the tests. Patient #1
(17y) underwent left hand surgery after an incision
injury for MCP joint of the index finger. Patient #2
(65y) underwent left hand surgery because of carpal
tunnel syndrome and trigger finger (middle finger).
2.3 Experiment Set-up and Test
Protocol
The experiment was divided into three tests termed A,
B, C (detailed in the following), which requested to
place the hand recursively in known positions, with
the glove always kept.
Before each test, the subjects were asked to sit on
a chair in front of a table, the arm and forearm forming
90°. The hand in flat position and the wrist in neutral
position defined the reference for each of the joints at
0°.
The subject donned his/her best fitting sensory
glove (medium or small size) above a latex one.
He/she was then trained to the testing procedures, as
Figure 1: The sensory glove prototype and the experimental
materials.
follows:
Test A Open-Close: the subject placed his/her
elbow joint on the table-top and was asked to
completely open his/her hand (angle of 0°,
without hyperextension) and then completely
close it (the thumb above the fingers).
Test B Grasping Bottle (Transverse Volar Grip):
it started with the hand in flat position. The
subject was asked to grasp (using all fingers), and
to release a spray bottle (diameter 2.5cm, height
15cm, see Figure 1). He/she returned then to the
initial neutral position.
Test C Grasping Dressing Roll (Five-Finger
Pinch): Test C was analogous to Test B, but a
dressing roll (diameter 4.5cm, height 7cm) was
used instead of the bottle.
The bottle and the roll grasps were adopted based
on the most daily used hand-grips (Sollerman, 1995),
and objects’ neutral positions were drawn on the
table-top. No time constraints were given during all
the experiments.
For repeatability evaluation, the subjects
performed each task five times without removing the
glove. For reproducibility evaluation, the subjects
performed again the overall procedure two weeks
after (so that the glove was doffed and donned
between days). For each repetition of each task, data
of all sensors were acquired during the entire
performance: from the starting position to the ending
position of the hand.
Healthy subjects performed the tests by using both
left and right hand; patients performed the tests only
with the injured hand. During the two weeks between
tests, patients followed a rehabilitation program
(extracorporeal shockwave therapy), therefore data
analysis can focus on the assessment of rehabilitation
outcomes.
BIODEVICES 2016 - 9th International Conference on Biomedical Electronics and Devices
188
2.4 Data Processing
An ad-hoc circuitry was designed to acquire data from
sensors and to condition the signals (resistance values
were converted into voltages and analog values into
digital ones), before transmitting them to a personal
computer, which converted incoming data into
original angles for further analysis.
Test A: Angle data was processed obtaining the
average ROM (maximum angle – minimum angle) for
each finger joints. Repeatability of the measures was
assessed considering standard deviation (SD) values.
Test B and C: The repeatability among dynamic
measures was assessed considering the intra-class
correlation coefficient (ICC) (Shrout and Fleiss,
1979), close to 1 for a high reliability, close to 0 for
low reliability. For each measure, the dynamic angle
values were time-normalized, so to calculate the ICC
coefficients comparing curves with the same number
of samples.
2.5 Statistical Analysis
For each day and for each healthy subject, we obtained
a reference value of the entire hand for the two
parameters of repeatability, SD of ROM (Test A) and
ICC coefficient (Test B and C). We calculated the
mean value across all finger joints and a statistical
analysis was performed using these results. An
ANOVA for repeated measures with two within-
subjects factors was conducted to assess if time and
handedness (and their interaction) might influence
measurements repeatability. The level of significance
was set at 0.05.
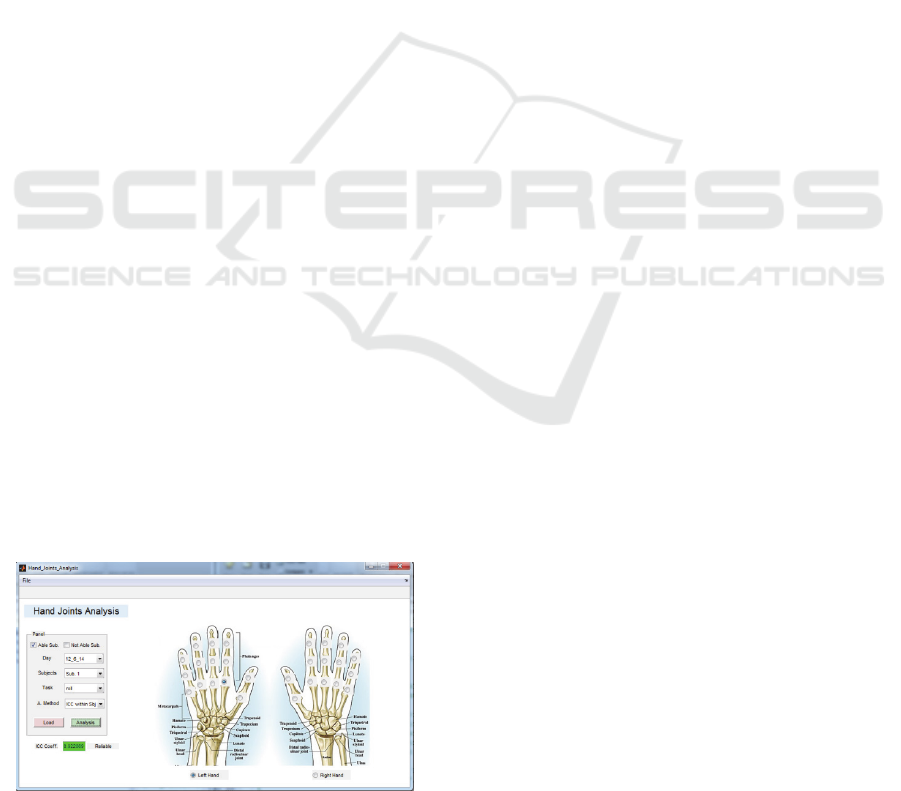
2.6 User Interface
We developed a useful graphical user interface (GUI)
to facilitate usability of our system by clinicians
(Figure 2). The GUI allowed selecting the joint of
interest that the clinician wants to evidence. Also, it
allowed calculating the repeatability of each
Figure 2: System Graphical User Interface (GUI).
sensor/joint during dynamic tasks.
All data processing was performed using Matlab
(MATLAB R2013a, The MathWorks, Inc., Natick,
MA) programs.
2.7 User Feedback Questionnaire
Feedback regarding comfort with handling and
wearing the glove was assessed by a user
questionnaire (Table 1) adapted from (Gentner and
Classen, 2009; Simone, 2007). For each item, subjects
were asked to select one of seven statements from 1
(strongly disagree) to 7 (strongly agree). Item Q12 was
administered only to healthy subjects.
3 RESULTS AND DISCUSSIONS
3.1 Test a: Healthy Subjects
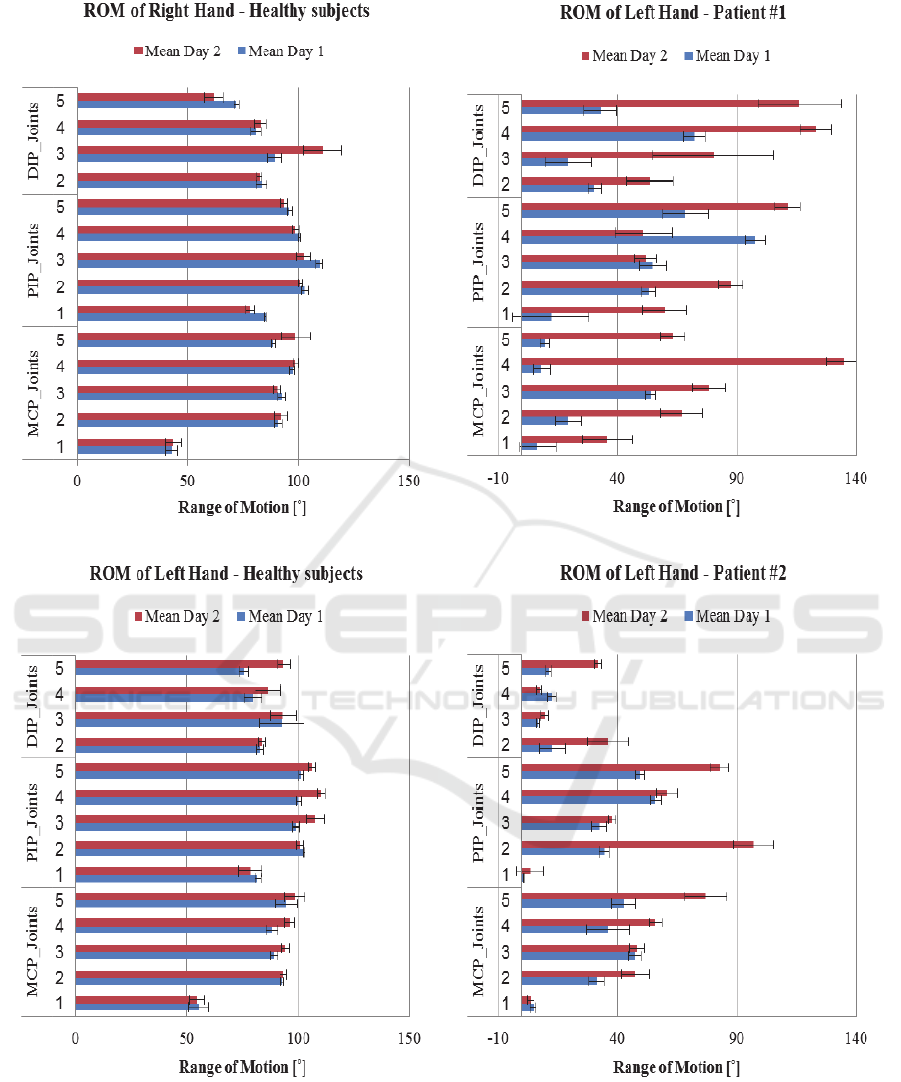
The mean ROM values and their SDs among all the
healthy subjects are shown in Figure 3a,b separately
for each joint. Repeatability of ROM is reported as
standard deviation and all joints showed comparable
SD values. SD for right hand range from 0.36° to 2.93°
(mean value 1.60°) and from 0.92° to 8.49° (mean
value 2.97°) for first and second day respectively; SD
for left hand range from 0.66° to 9.84° (mean value
2.67°) and 1.35° to 5.96° (mean value 3.09°) for first
and second day respectively.
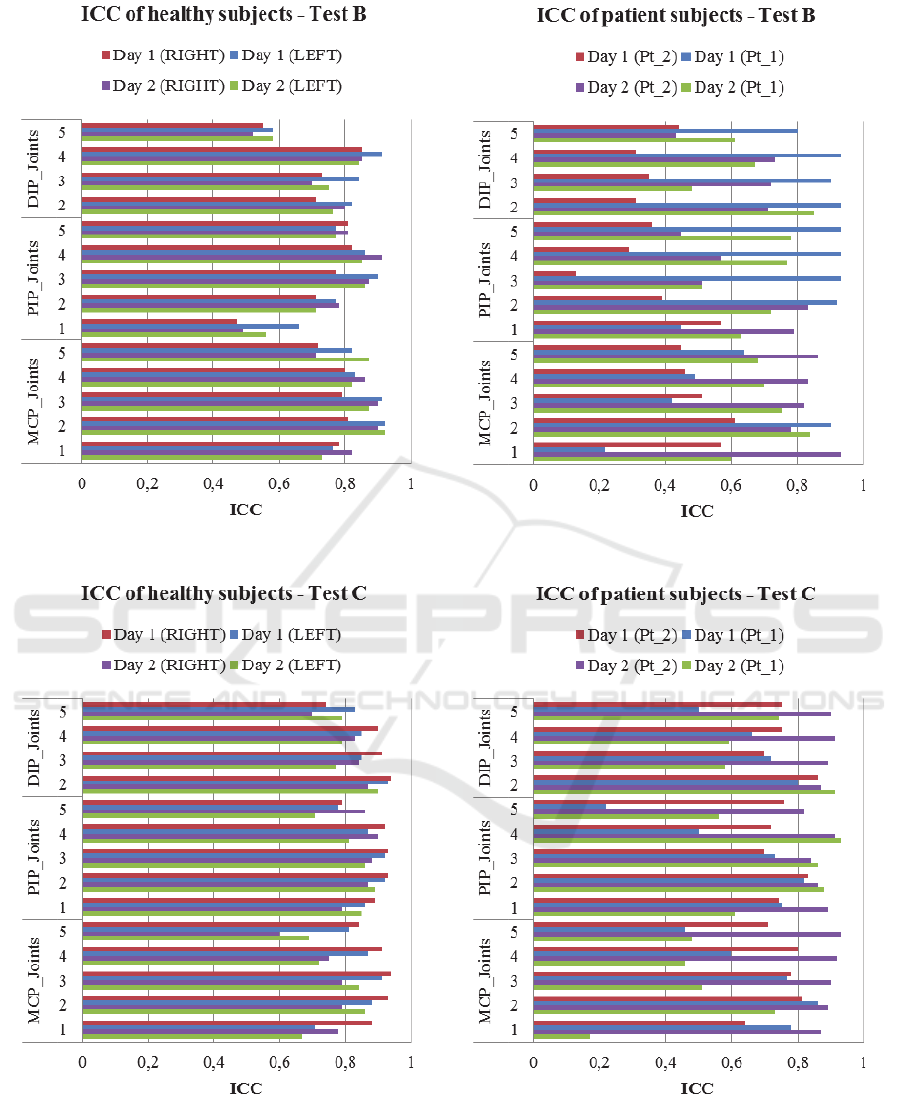
3.2 Test B and C: Healthy Subjects
ICC analysis was performed for Test B and Test C
individually, and for each sensor. For healthy subjects,
the average values of ICC for each joint are shown in
Figure 4a,b.
For Test B, the average ICC across all the fingers
in the two days is 0.76 for the right hand and 0.79 for
the left one. For Test C, the average ICC across all the
fingers in the two days is 0.85 for the right hand and
0.83 for the left one.
The obtained ICC values were consistent with no
particular joint showing markedly lower repeatability
than the mean. Overall, repeatability was
quantitatively assessed by ICC mean values ranging
from 0.74 to 0.89 with a mean across joints of 0.81.
These results were comparable to the ones obtained
with the gloves evaluated by Simone et al. (Simone,
2007) (ICCs from 0.79 to 0.99 with a mean of 0.95),
Dipietro et al., (2003) (ICCs from 0.7 to 1.0), and
Mentzel et al., (, 2001) (ICCs from 0.82 to 0.99, with
a mean of 0.94).
The repeatability and reliability of our sensory
Assessment of Hand Rehabilitation after Hand Surgery by Means of a Sensory Glove
189
Table 1: User feedback questionnaire*
#
.
Q# Question
Q1 I felt comfortable as the glove was put on
Q2 I did not feel like my fingers were put into any uncomfortable position as the glove was put on
Q3 I felt any restriction to movement with this glove
Q4 I felt comfortable performing the activities in this study
Q5 The glove did not feel too tight (it did not make my hands or fingers tingle)
Q6 I feel like I can bend my fingers just like I can without wearing the glove
Q7 The glove did not feel too hot or too cold
Q8 I did not feel a reduction in tactile sensitivity of the fingers with this glove
Q9 I had no trouble during the grasping tasks wearing this glove
Q10 I did not feel like my fingers were put into any uncomfortable position as the glove was removed
Q11 I felt comfortable as the glove was removed
Q12 I did not felt any difference when I was worn the left glove
* Answers were coded as: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = neutral, 5 =
somewhat agree, 6 = agree, and 7 = strongly agree.
#
Adapted from (Gentner and Classen, 2009; Simone, 2007).
glove is similar to other evaluated gloves and also lies
within the measurement reliability of manual
goniometry. This result shows both the reliability of
the used system and the ability of the healthy
participants to repeat the same gesture. These results
allowed us to use the system for further analyses with
patient subjects.
3.3 Statistical Analysis
Statistical analysis showed that time and the
interaction between time and handedness did not
influence standard deviation of ROM values
(respectively p = 0.644 and p = 0.612). On the contrary,
there were significant differences (p = 0.042)
comparing SD data between right and left hand.
For the dynamic repeatability of Test B and Test C,
the statistical analysis was conducted across the ICC
coefficients of the healthy subjects. It showed that
time, handedness and their interaction did not
influence repeatability of Test B (time p = 0.868;
handedness p = 0.295; time*handedness p = 0.234).
For Test C, the statistical analysis showed that time
might influence dynamic repeatability of grasping a
dressing roll (p = 0.002). On the contrary there were
not significant differences due to the dominance of the
hands (p = 0.381). The interaction between time and
handedness did not present statistical differences (p =
0.258).
These results suggest that further investigations
are welcome because of the two significance
outcomes: handedness for the SD of the ROM (p =
0.042 ≈ 0.05) and time for Test C. Grasping a dressing
roll (Test C) might be a gesture not easy to repeat
similarly between two days of measurements because
even a healthy subject gets familiar with the gesture.
3.4 Feasibility Evaluation with Patient
Subjects’ Data
Patient subjects’ results of the ROM (mean ± SD) (see
Figure 3c,d individually for the two participants)
demonstrate how the ROM has changed after two
weeks of rehabilitation.
It is worth to investigate ROM results for the main
joints involved in surgery. For patient #1 (left hand
surgery after an incision injury for MCP joint of the
index finger) values of the ROM of index joints
markedly increase between days: MCP joint range
19.3÷77.3°; PIP joint range 53.1÷136.3°; DIP joint
range 30.4÷63.9°. For patient #2 (middle finger joints
surgery), values of the ROM of middle finger remain
quite unchanged between days: MCP joint range
47.2÷48.3°; PIP joint range 32.3÷37.7°; DIP joint
range 6.8÷9.6°. Patient subjects’ outcome suggests
that motor recovery for patient #1 was quicker than for
patient #2. Actually, the former had easily recovered
hand function abilities while the latter showed a slow
recovery.
The average values of ICC of Test B and Test C for
left hand joints of patient subjects are shown in Figure
4c,d. For Test B, the average ICC across all the fingers
between days is 0.71 for the first patient and 0.56 for
the second one. For Test C, the average ICC across all
the fingers in the two days is 0.65 for the first patient
and 0.82 for the second one. For the first patient, there
was not an increase of the overall ICC values between
the days of measurements, while there was a marked
increment for the second patient. These results suggest
BIODEVICES 2016 - 9th International Conference on Biomedical Electronics and Devices
190
(a) (c)
(b) (d)
Figure 3: Range of Motion (ROM) values: for healthy subjects (a) right hand and (b) left hand; for patient subjects (c) Patient
#1 and (d) Patient #2. Results are presented as mean value and standard deviation separately for each day of measurements.
For each group of joints (MCP, PIP and DIP), fingers are coded as follows: 1 = thumb, 2 = index, 3 = middle, 4 = ring and 5
= small finger.
Assessment of Hand Rehabilitation after Hand Surgery by Means of a Sensory Glove
191
to assess specific tasks for different hand injuries.
Repeatability was quantitatively assessed by ICCs
ranging from 0.64 to 0.74 with a mean across joints of
0.68 for the first patient, and ranging from 0.41 to 0.89
with a mean across joints of 0.69 for the second
patient. Comparing with the results in Figure 4a,b,
ICC values of patients are lower than the mean values
of ICC of the healthy subjects as we expected.
3.5 User Feedback Questionnaire
The questionnaire gave positive responses to most
questions: the average scores across all subjects are
between 4.0 and 7.0 and between 5.0 and 7.0 out of a
maximum score of 7 respectively for the first and
second day (see Table 2). Average responses for all
subjects were positive, the mean and SD being 5.82±
0.60 and 6.09 ± 0.28 for first and second day
respectively. Responses were not significantly
different between the healthy group and the patient
group, so results are shown as average values across
all subjects. Questions 1, 2, 10 and 11 addressed
comfort during donning and doffing the glove and the
average responses for all subjects were positive: 6.08
±0.25 and 6.12±0.06 for the first and the second day
respectively. Questions 3, 4, 5, 6, 7, 8, 9, and 12
captured feedback about the comfort performing the
ADL-based activities wearing the glove and the
positive average responses for all subjects reported a
significant goal: 5.78±0.43 and 6.07±0.26 for first
and second day respectively.
The average responses for all subjects for the
second day is better than ones for the first day
supposedly because of the subjects are being familiar
with using the glove. From a general point of view the
participants reported comfort with the glove and no
relevant obstruction in movements.
4 CONCLUSIONS
The aim of this research was to furnish to the
clinicians a system for measuring finger joints
movement that is accurate, objective, easy to use and
that delivers useful data through an easy user interface.
It focused on the human finger postures and dynamic
function movements during the accomplishment of
ADL-based tasks rather than on the ability to
accomplish these tasks. Furthermore, the proposed
system allows tracking the movements of finger joints
by means of virtual reality during a rehabilitation
plane.
Our system is very easy to use, it can be used in
many applications (e.g. evaluation of patient motor
therapy and rehabilitation process), it can capture
dynamically the full range of motion during finger-
joint bending and it can monitor all the joints of one
finger. Its performances are comparable to ones of
other evaluated gloves, confirming the feasibility of
the system, but to our knowledge, there are not other
examples of applications of sensory gloves to assess
hand surgery follow-up.
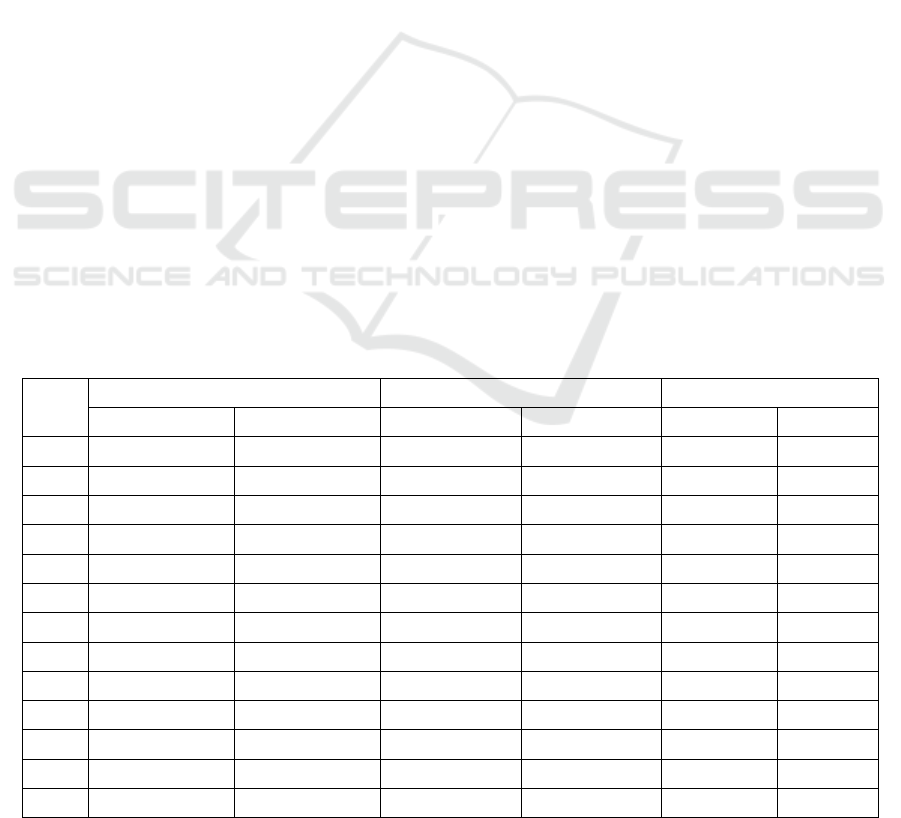
Table 2: User feedback questionnaire: mean scores per question.
Healthy Subjects (N=9) Patient Subjects (N=2) All Subjects
Day 1 Day 2 Day 1 Day 2 Day 1 Day 2
Q1 6.0 6.2 5.0 6.0 5.0 6.2
Q2 5.8 6.1 6.0 6.5 5.0 6.3
Q3 5.3 5.7 4.5 6.0 5.0 5.9
Q4 6.3 6.2 6.0 6.0 6.2 6.1
Q5 6.2 6.2 7.0 6.5 6.6 6.4
Q6 5.4 5.9 6.5 6.0 6.0 6.0
Q7 6.0 6.2 7.0 6.0 6.5 6.1
Q8 5.3 5.8 5.0 6.5 5.2 6.2
Q9 6.1 6.1 6.0 6.5 6.1 6.3
Q10 6.3 6.2 4.0 5.0 5.2 5.6
Q11 6.2 6.1 7.0 7.0 6.6 6.6
Q12 5.4 6.4 - - 5.4 6.4
Total 5.9±0.4 6.1±0.2 5.8±1.1 5.7±1.9 5.7±0.7 6.2±0.3
BIODEVICES 2016 - 9th International Conference on Biomedical Electronics and Devices
192
(a) (c)
(b) (d)
Figure 4: Mean values of Intra-class Correlation Coefficients (ICCs): healthy subjects Test B (a) and Test C (b); patient
subjects Test B (c) and Test C (d). For healthy subjects results are shown separately for the right and the left hand. For each
group of joints (MCP, PIP and DIP), fingers are coded as follows: 1 = thumb, 2 = index, 3 = middle, 4 = ring and 5 = small
finger. Pt_1: patient subject #1; Pt_2: patient subject #2.
Assessment of Hand Rehabilitation after Hand Surgery by Means of a Sensory Glove
193

Through analyzing tasks of healthy subjects, we
were able to study characteristics of the ROM of the
finger joints and movement repeatability. The results
of healthy subjects’ tests might serve as standard
values and help us in evaluating the severity of a
hand functional deficit in the future.
This work presents the preliminary outcomes of
our research, and its positive results encourage
further studies aiming at confirming the present
finding and fostering the proposed system into
clinical practice. Our next steps will be to examine
more patient subjects after hand surgery, to compare
between them, to assess the rehabilitation process
and correspondingly improve the efficiency of
rehabilitation.
REFERENCES
Borghetti, M., Sardini, E., Serpelloni, M., 2013.
Sensorized Glove for Measuring Hand Finger Flexion
for Rehabilitation Purposes. Transactions on
Instrumentation and Measurement. 62(12). p. 3308-
3314.
Carpinella, I., Mazzoleni, P., Rabuffetti, M., Thorsen, R.,
Ferrarin, M., 2006. Experimental protocol for the
kinematic analysis of the hand: Definition and
repeatability. Gait and Posture. 23(4). p. 445-454.
Chen, H., Wang, Q., Cao, L., 2010. Design of the
Workstation for Hand Rehabilitation Based on Data
Glove. In IEEE International Conference on
Bioinformatics and Biomedicine Workshops. p. 769-771.
Dipietro, L., Sabatini, A. M., Dario, P., 2003. Evaluation
of an instrumented glove for hand movement
acquisition. Journal of Rehabilitation Research and
Development. 40(2). p. 179-190.
Gentner, R., Classen, J., 2009. Development and
evaluation of a low-cost sensor glove for assessment
of human finger movements in neurophysiological
settings. Journal of Neuroscience Methods. 178(1). p.
138-147.
Lee, J. W., Rim, K., 1991. Measurement of finger joint
angles and maximum finger forces during cylinder
grip activity. Journal of Biomedical Engineering.
13(2). p. 152-162.
Mentzel, M., Hofmann, F., Ebinger, T., Jatzold, B., Kinzl,
L., Wachter, N. J., 2001. Reproducibility of
measuring the finger joint angle with a sensory glove.
Handchir Mikrochir Plast Chir. 33(1). p. 59-63.
Saggio, G., Latessa G., De Santis, F., Bianchi, L.,
Quitadamo, LR., Marciani, MG., Giannini, F. 2009.
Virtual reality implementation as a useful software
tool for e-health applications. 1th IEEE International
WoWMoM Workshop on Interdisciplinary Research
on E-Health Services and Systems ( IREHSS).
Saggio, G., 2012. Mechanical model of flex sensors used
to sense finger movements. Sensors and Actuators A:
Physical. 185. p. 53–58.
Saggio, G., Bizzarri, M. 2014. Feasibility of
Teleoperations with Multi-Fingered Robotic Hand for
Safe Extravehicular Manipulations. Aerospace
Science and Technology. 39. p. 666-674.
Saggio, G., Riillo, F., Sbernini, L., Quitadamo, L. in press.
Resistive Flex Sensors: a survey. Smart Materials and
Structures.
Simone, L. K., Sundarrajan, N., Luo, X., Jia, Y., Kamper,
D. G., 2007. A low cost instrumented glove for
extended monitoring and functional hand assessment.
Journal of Neuroscience Methods. 160(2). 335–348.
Shrout, P. E., Fleiss, J. L., 1979. Intraclass correlations:
uses in assessing rater reliabiltiy. Psychological
Bulletin. 86(2). p. 420-428.
Sollerman, C., Ejeskär, A., 1995. Sollerman hand
function test: a standardised method and its use in
tetraplegic patients. Scand J Plast Reconstr Surg
Hand Surg. 29(2). p. 167-176.
Vergara, M., Sancho-Bru, J. L., Pérez-González, A., 2003.
Description and validation of a non-invasive
technique to measure the posture of all hand segments.
Journal of Biomechanical Engineering. 125(6). p.
917-922.
Williams, N. W., Penrose, J. M. T., Caddy, C. M., Barnes,
E., Hose, D. R., Harley, P., 2000. A goniometric glove
for clinical hand assessment. Construction,
calibration and validation. Journal of Hand Surgery.
(European Volume) 25(2). p. 200–207.
BIODEVICES 2016 - 9th International Conference on Biomedical Electronics and Devices
194
