
Towards a Peer-to-Peer Communication Model for
Mobile Telecare Services
Akio Sashima and Koichi Kurumatani
Human Informatics Research Institute, National Institute of Advanced Industrial Science and Technology (AIST),
2-3-26 Aomi, Koto-ku, Tokyo, 135-0064, Japan
Keywords:
Telecare, mHealth, Peer-to-Peer, Mobile Physiological Sensor, Communication Protocol, UDP Hole Punch-
ing.
Abstract:
In this paper, we describe a peer-to-peer communication model for a mobile telecare service. It is proposed
to reduce the service management costs of a conventional mobile telecare service based on a server-client
communication model. The peer-to-peer mobile telecare service consists of a mobile physiological sensor,
two smartphones, and a connection management server. In the service, when a caregiver, e.g., family member,
requires to know current physiological statuses of a cared person, e.g., elderly person, the smartphone directly
sends the sensing data of the cared person to the caregiver’s smartphone without a central data server. To realize
the peer-to-peer communication model in mobile phone’s infrastructure, which includes private networks, we
propose a communication protocol based on a NAT-traversal technique and a data compression mechanism
for preventing packet loss. We have confirmed that the prototype system works well on the current mobile
phone’s infrastructure that consists of 4G (LTE) and private networks.
1 INTRODUCTION
Recently, mobile health, telemedicine, and telecare
services using smartphones have been drawn atten-
tion of researchers in scientific and industrial com-
munity (Lin, 2012)(Triantafyllidis et al., 2013)(Tri-
antafyllidis et al., 2015). In the mobile health ser-
vices, physiological and behavior data obtained by
wearable smart devices, e.g., watch, phones, glasses,
are used for managements of physical and mental
conditions (Lu et al., 2012) of the persons who take
care of their health.
In mobile telecare services, wearable devices can
be used for remotely monitoring the statuses of older
persons who live alone in their homes (Sashima et al.,
2008)(Vines et al., 2013)(Bellido et al., 2015). The
service provides the obtained sensor data for their
trustworthy persons who take care about the older
person, such as caregivers, family members, doctors,
by using their smartphones. Some services can alert
them when it detects an emergency situation of the
person, such as fall detections (Huang and Newman,
2012)(Sannino et al., 2014).
In this research, we focus on a communication
model which is suitable for telecare services using
smartphones. So far, in order to implement such tele-
care services, most of them have been built based
on server-client communication model; all of sensing
data of the older person are sent to a central server and
the server manages and provides the sensing data for
the community. The model fits for web based services
on the Internet very well. For example, sensing data
are collected on a web server and the caregivers can
see the sensing information, e.g., activity status, as a
web content of the web browser that he/she usually
uses.
Although a telecare service based on the server-
client communication model has been proposed so
far, the approach has some drawbacks to start up and
maintain a practical service in reality. A drawback is
a management cost of the server. For example, using
the server-client model, it is hard to prevent overloads
in the case of increasing users’ traffic accessing the
server because all sensing data are necessarily sent to
and received from the server. Therefore, to handle
the data traffics, it requires that the server has enough
information processing power which typical personal
computers do not have. In addition, because leakage
of the personal data sensed for the telecare service
causes privacy issues, managing a lot of personal data
in the server rises the management costs.
In order to prevent the issues arising from the
server-client model, we propose a peer-to-peer com-
542
Sashima, A. and Kurumatani, K.
Towards a Peer-to-Peer Communication Model for Mobile Telecare Services.
DOI: 10.5220/0005845205420549
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 5: HEALTHINF, pages 542-549
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

munication model (P2P model) for telecare services.
The model assumes that the smartphones of the users
directly communicate with each other in peer to peer
manner. In other words, the sensing data are directly
sent to a smartphone of a caregiver. It is not medi-
ated by a central data server so as to reduce the cost
of maintaining the service.
The P2P communication model appears to be ap-
propriate to the telecare service from the maintenance
point of view. However, it is unclear that the P2P
model works on the current mobile phone’s commu-
nication infrastructure.
In this paper, we describe a prototype system
based on the P2P model which we have developed
as a proof of concept and show experimental results
measuring communication performance of the sys-
tem. We focus here on realizing the on-line peer-
to-peer communication facility on the current com-
munication infrastructure which includes private net-
works, and propose a communication protocol based
on a NAT-traversal technique. A data compression
mechanism for preventing the packet loss of the com-
munication is also proposed. We have confirmed that
the prototype system works well on the current mo-
bile phone’s infrastructure.
2 COMMUNICATION MODEL OF
MOBILE TELECARE SERVICE
In this section, we describe a server-client commu-
nication model and a peer-to-peer communication
model for implementing a mobile telecare service.
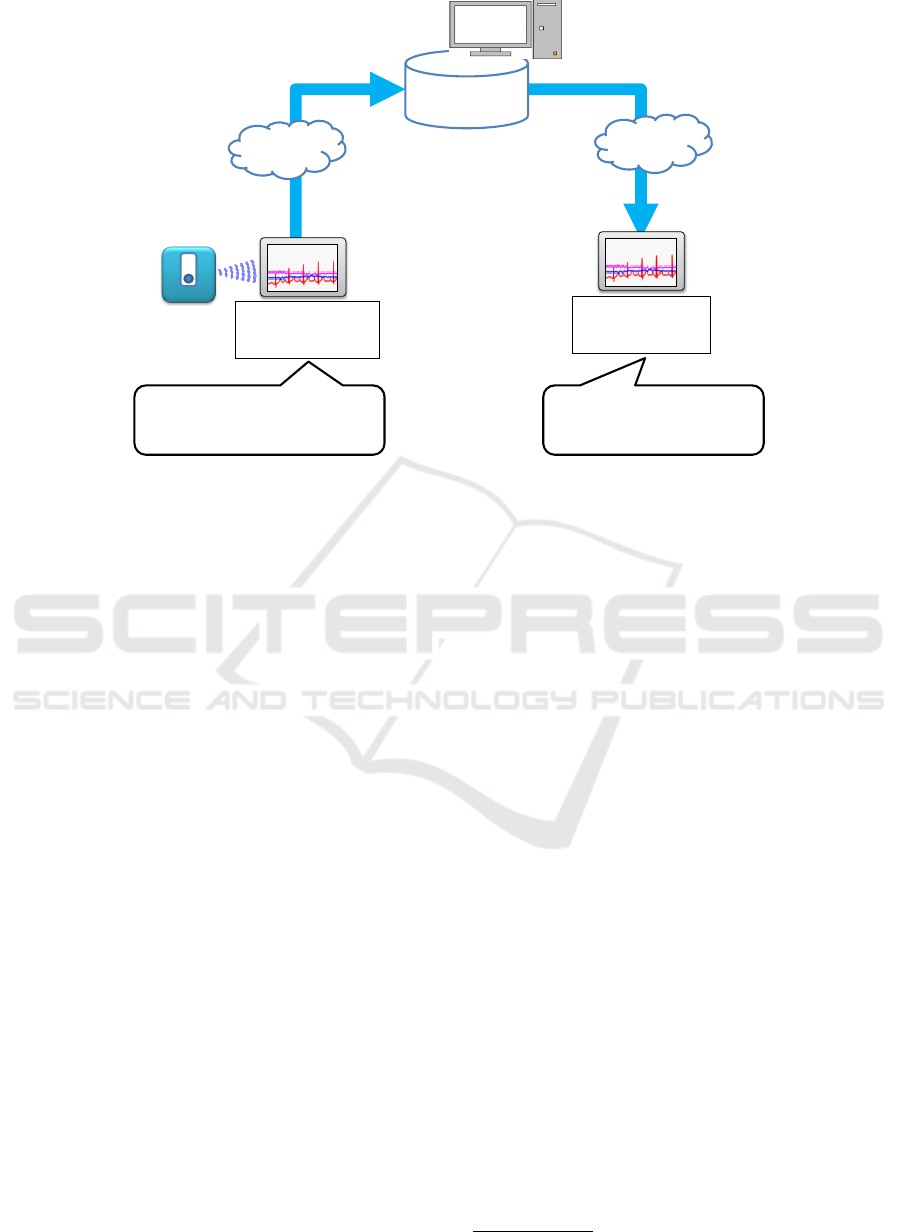
2.1 Server-Client Model
Figure 1 shows an overview of a typical telecare ser-
vice based on a server client model. In this model, we
assume that the service consists of a mobile physio-
logical sensor, two smartphones, and a central data
server. The mobile physiological sensor wirelessly
communicates with a smartphone. All sensor data
from the wireless sensor are sent to a data collection
server by a smartphone (sender). The data can be seen
by a user with a smartphone (receiver) by accessing
the server. It is possible to know the latest status of
the user wearing the sensor.
This model can be easily implemented and the
server can be stored a large amount of data for the data
analysis. However, it has some drawbacks about the
management of the server. Because it is hard to pre-
vent overloads at the server in the case of increasing
the data traffic flows, it should be a high performance
computer that has enough to handle the large traffic
loads. In addition, because personal health data on
the server should be carefully managed, it also rises
the management costs of the server.
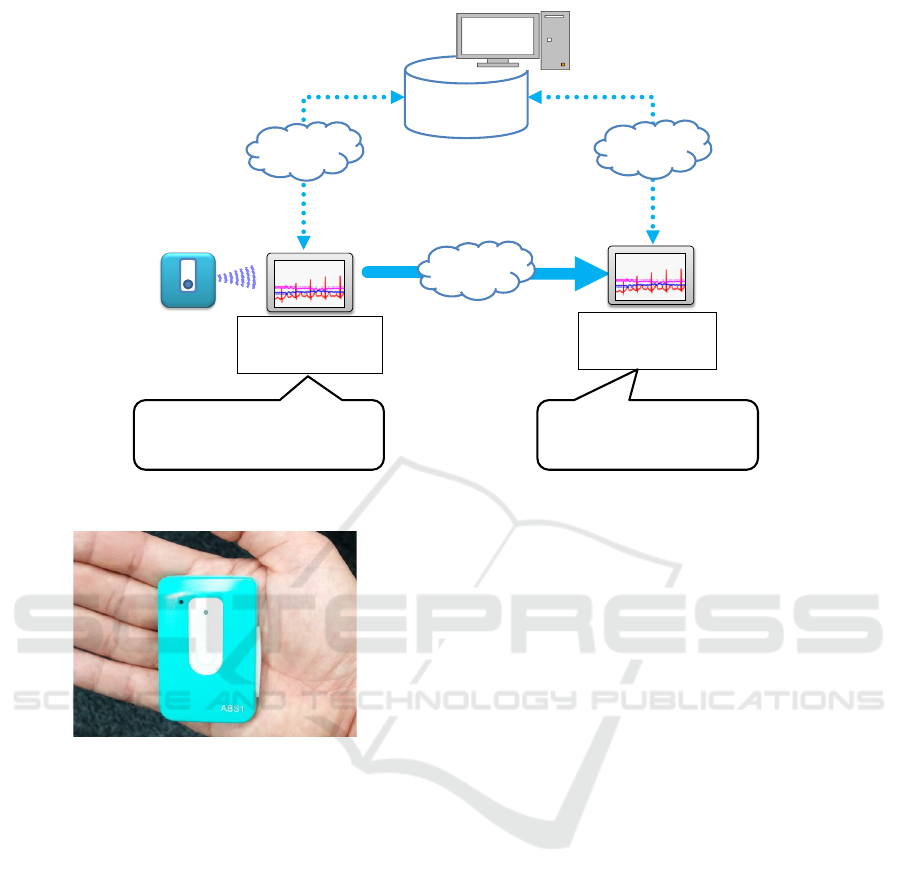
2.2 Peer-to-Peer Model
Figure 2 shows an overview of a telecare service
based on a peer-to-peer model proposed in this paper.
In this model, we assume that the service consists of
a mobile physiological sensor, two smartphones, and
a connection management server. The mobile physio-
logical sensor wirelessly communicates with a smart-
phone. All sensor data from the wireless sensor are
directly sent to a smartphone (receiver) by a smart-
phone (sender) using the connection information at
the connection management server. The sensed data
can be seen by a remote user using her/his smart-
phone. Hence, it is possible to know the latest status
of the user without a central server.
On the current mobile phone’s communication in-
frastructure, however, there are some issues about
handling the network address (IP address and port
number) for realizing the peer to peer communica-
tion. First, the network address of a smartphone is
dynamically changed according to its network envi-
ronments. To enable two smartphones communicate
with each other, the network address of the peer is re-
quired. Second, the smartphone that connects to a pri-
vate network with Wi-Fi, such as at home, uses a local
IP address. The address is converted to a global ad-
dress at the network address translator (NAT) router
of the network. Similarly, most smartphones of the
mobile phone carriers in Japan share and use limited
global addresses of the carrier’s gateway servers for
the communication.
To solve the issues, we introduce 1) a connection
management server and 2) a NAT-traversal technique
in our peer-to-peer communication model.
2.2.1 Connection Management Server
A connection management server stores the network
address of each user’s smartphone, and updates them
when the smartphone starts to connect to the server. It
also tells other smartphones the updated address. By
knowing the latest address of the smartphone that they
would like to communicate with, the smartphones can
communicate each other even if the addresses are dy-
namically changed.
2.2.2 NAT-Traversal Technique
A NAT traversal technique is used to establish a peer
to peer communication channel over a NAT router. It
enables a smartphone in a private network communi-
Towards a Peer-to-Peer Communication Model for Mobile Telecare Services
543
Internet
4G
Data
Management
• Receiving and
sending sensing data
Smartphone
Sender
Smartphone
Receiver
Sensor
Data
Mobile
Physiological
Sensor
Internet
4G
Sensor
Data
• Cared Person
Ex. elderly person
• Caregiver
Ex. family member
Figure 1: Overview of the client-server communication model.
cating with the smartphone in the outside of the net-
work.
We adopt the UDP hole punching as the NAT
traversal technique (Ford et al., 2005)(Rosenberg
et al., 2003). The UDP hole punching is a technique
establishing a connection for User Datagram Proto-
col (UDP) packet streams that traverse the NAT. It
typically uses the connection management server that
enables two smartphones can exchange their network
addresses.
In the communication model, a smartphone (A) in
a private network sends a UDP packet to the server
and waits for the server’s response through the NAT
router. The server knows the networks address of A
by analyzing the received packet and tells the oppo-
nent smartphone (B) the address of the A. The oppo-
nent smartphone (B) knows the address of the A and
sends a UDP packet to the address. The packet is me-
diated by the NAT router and reaches the smartphone
(A) in the private network.
Using the above techniques, we can realize the
peer-to-peer communication through the NAT router.
Details of the communication protocol are described
in Section 3.2.
3 IMPLEMENTATION
In this section, we describe an implementation of a
prototype system of the P2P model. It provides a tele–
monitoring service of user’s statuses, e.g., heart rate,
body acceleration, etc. The prototype system consists
of a wireless physiological sensor which we have de-
veloped (Sashima et al., 2011), two smartphones, and
a connection management server. We implement the
system on the android devices: Google Nexus 5 and
Nexus7.
3.1 Remote Monitoring of
Electrocardiographic data
Figure 3 shows a mobile physiological sensor which
we have developed. The physiological sensor is a
small, wearable, wireless sensor device which in-
cludes a flash memory, a lithium ion battery, and 5
kinds of sensors: electrocardiographic sensor (1 chan-
nel), 3-axis accelerometer, barometer, thermometer,
hygrometer. Its size and weight are as follows: size
6×4×1.5 cm; weight 34.5g. Continuous operating
time is about 6–8 hours for sensing electrocardio-
graphic data. It includes a Bluetooth
1
module can be
communicate with a smartphone.
In this paper, we have evaluated the validity of the
remote monitoring of the Electrocardiographic data
using the sensor device.
The device continuously senses electrocardio-
graphic data of the user and wirelessly sends the data
to the smartphone. The sensing rate is 200 Hz and the
data is represented by 2 byte Integer. The sensor de-
vice is attached to user’s chest by sticking electrodes
with a peel-off sticker.
1
https://www.bluetooth.com/
SmartMedDev 2016 - Special Session on Smart Medical Devices - From Lab to Clinical Practice
544
Internet
4G
Connection
Management
• Receiving and sending
connection data
Smartphone
Sender
Smartphone
Receiver
Sensor Data
Internet
4G
Connection
Data
Internet
4G
Connection
Data
• Cared Person
Ex. elderly person
• Caregiver
Ex. family member
Mobile
Physiological
Sensor
Figure 2: Overview of the peer-to-peer communication model.
Figure 3: Mobile physiological sensor.
3.2 Communication
In current implementation, each smartphone of our
system plays a communication role: sender or re-
ceiver. A smartphone playing sender role wirelessly
communicates with the sensor device. It sends the
sensing data to a smartphone playing receiver role
through the 4G network and Wi-Fi. The sender and
receiver communicate with the connection server for
controlling the peer-to-peer connection. The con-
trolling messages are short texts represented in UDP
packets, and exchange the messages with the server
for the connection management with NAT-traversal
technique.
The server process works on a server machine
which has a global IP address on the Internet. It
opens a UDP network socket (port) which has a stable
port number, 9209, predefined in a service, and waits
for the connection messages from users’ smartphones.
When it receives a message from a user’s smartphone,
it updates the address of the smartphone, and tells the
address to smartphones of the user’s companions to
enable them accessing the user.
When they know their address each other, it can
send and receive the sensing data until one of them
disconnects the network. We have implemented two
methods for sending the sensing data: 1) a method
repeating to send a packet which includes a sens-
ing data, and 2) a method repeating to send a packet
which includes a sequence of sensing data with wait-
ing a corresponding ACK packet.
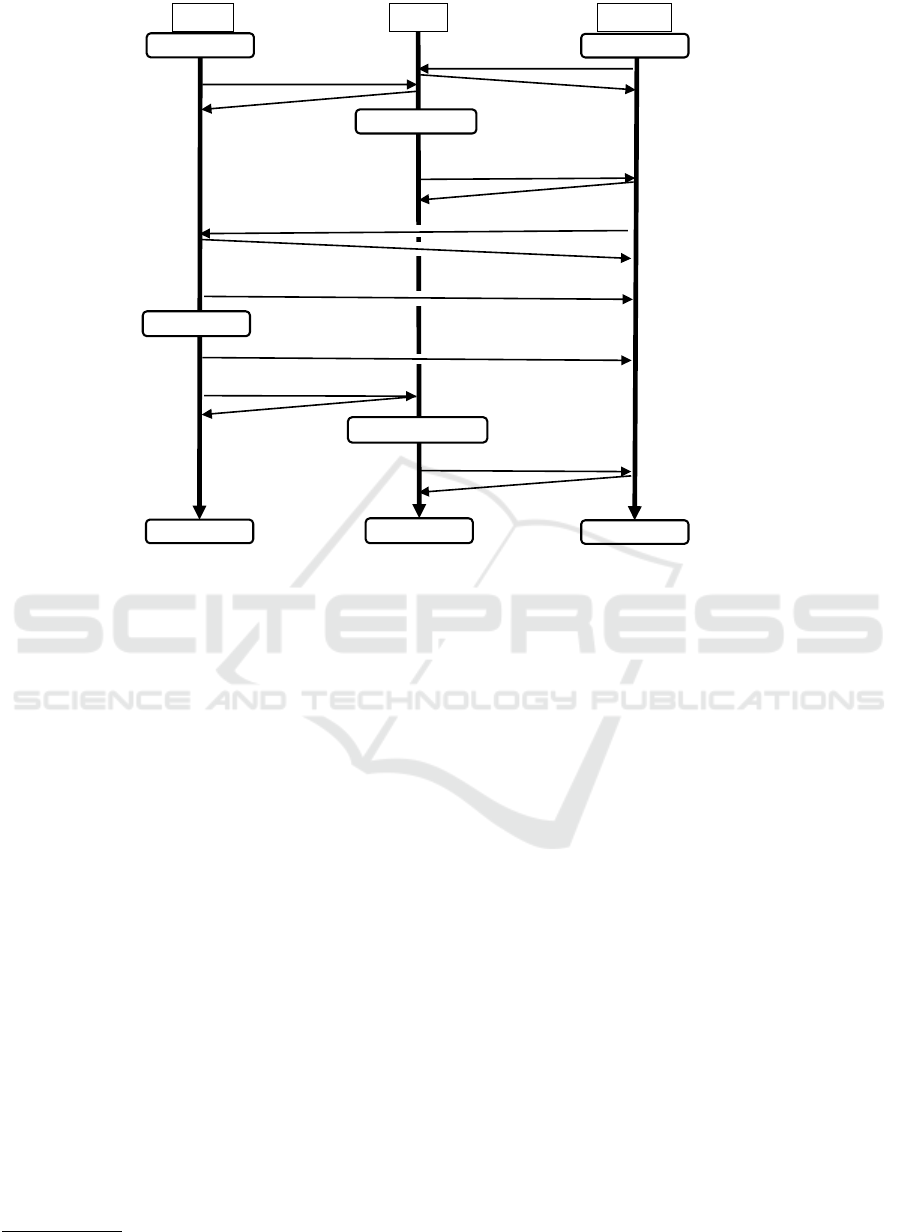
3.2.1 Sending Single Sensing Data without ACK
This method is designed for aiming at fast communi-
cations in a stable network environment, such as a lo-
cal area network (LAN). Figure 4 shows an outline of
the protocol using the method. In the methods, each
sensing data, such as an electrocardiographic value,
received by the sender is wrapped by a UDP packet,
and immediately sent to the receiver. Each packet
becomes short but the number of the packets are in-
creased. When the receiver receives a packet, it does
not send back acknowledge message packets to the
sender.
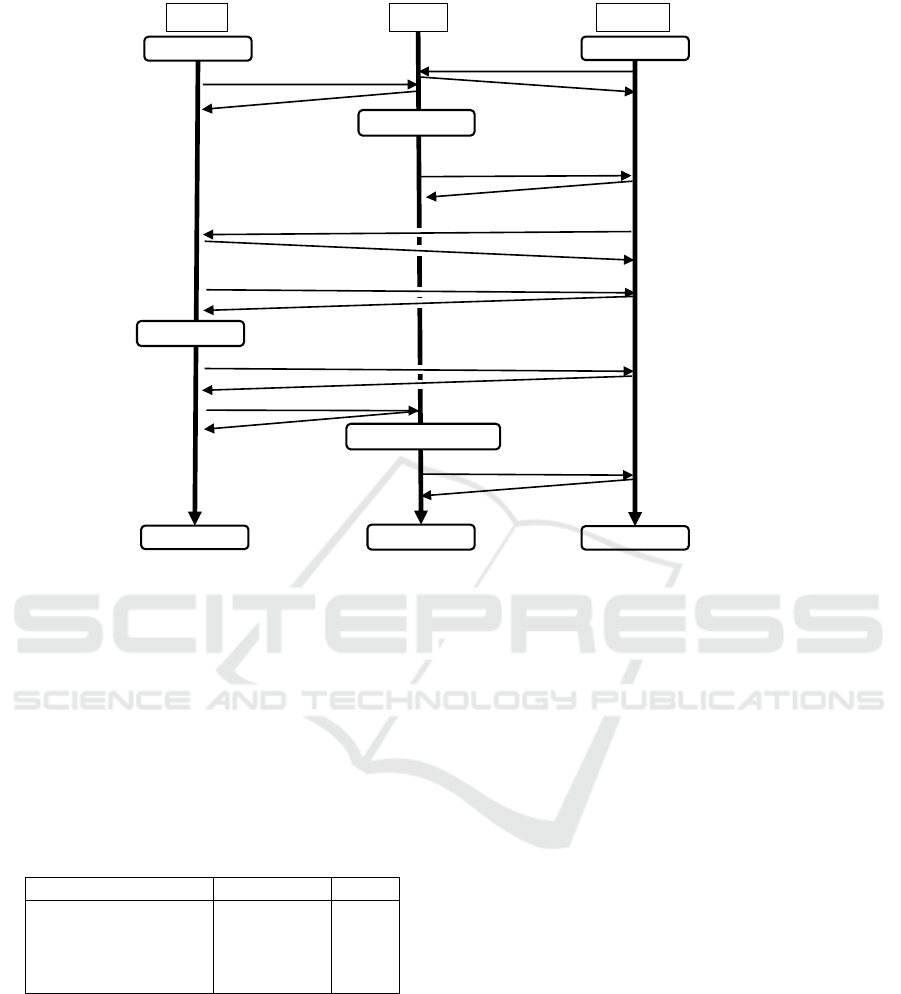
3.2.2 Sending a Sequence of Sensing Data with
ACK
This method is designed for aiming at robust com-
munications in noisy network environments, such as
Towards a Peer-to-Peer Communication Model for Mobile Telecare Services
545
Sender Server Receiver
Login
Login
ACK
ACK
Peer Matching
Telling the sender’s UDP
socket address.
ACK
Data Request
ACK
Sending Single Data (No ACK)
Repeat
Exit
ACK
Telling the sender exits
ACK
Start
Start
End
End
Sending Single Data (No ACK)
Repeat
End transaction
Figure 4: Outline of the protocol of sending raw data without ACK.
wide area network (WAN). Figure 5 shows an out-
line of the protocol using the method. In the meth-
ods, sensing data received by the sender is buffered
in a certain time period. Then the buffered data,
a sequence of sensing data, is cut and divided into
multiple sequences to keep its length within a maxi-
mum value predefined. Default value of the maximum
length is 120. Each divided sequence is wrapped by
a UDP packet, and sent to the receiver. A packet
includes a sequence of the data and becomes larger
than the packet including single value. Hence, we
apply the compression technique to make the packet
smaller. “zlib” library
2
(Deutsch and Gailly, 1996)
is used for the compression. It is a software library
based on a compression algorithm called “deflate”
(Deutsch, 1996).
When the receiver receives a packet, it sends back
an acknowledge (ACK) packet to the sender. The
sender sends a next packet when it receives the ACK
packet. If it does not receive the ACK packet in a cer-
tain time period, it sends the same packet and waits
the ACK packets again. If it repeats the sending pro-
cess five times and still does not receive the ACK
packet, it abandons sending the packet and sends a
next packet. Although waiting the ACK packet may
be a waste of time, it can prevent the packet loss.
2
http://www.zlib.net/
4 EVALUATIONS
We have experimentally evaluated communication
performance of the prototype system. We have specif-
ically investigated the packet loss and delay time be-
tween two smartphones, sender and receiver, in dif-
ferent network environments. The network environ-
ments are a public 4G (LTE) network provided in
Japan, and a Wi-Fi network (LAN), which is a private
network behind a NAT router, in our laboratory. We
have evaluated the two sending methods: 1) sending
single sensing data without ACK, called raw method
here, and 2) sending a sequence of sensing data with
ACK, called compressed method here, in four net-
work conditions: A) the sender and receiver connect
to the same LAN, B) the sender connects to the LAN
and the receiver connects to the 4G network, C) the
sender connects to the 4G network and the receiver
connects to the LAN, and D) the sender and receiver
connect to the same 4G network. We have analyzed
the first 100,000 samples received by the receiver for
each condition.
4.1 Packet Loss
Experimental results about the packet loss are shown
in Table 1. While a few percent of the packet loss oc-
SmartMedDev 2016 - Special Session on Smart Medical Devices - From Lab to Clinical Practice
546
Sender Server Receiver
Login
Login
ACK
ACK
Peer Matching
Telling the sender’s UDP
socket address.
ACK
Data Request
ACK
Sending data sequence
Sending data sequence
Repeat
Exit
ACK
Telling the sender exits
ACK
ACK
Start
Start
End
End
ACK
Repeat
End transaction
Figure 5: Outline of the protocol of sending data sequence with ACK.
curred by using the raw method, no packets were lost
by using the compressed method. We have confirmed
that the compressed method prevents the packet loss
in NAT-traversal situations.
In the results of the raw method, the worst con-
dition was the condition C in which the receiver in
the private network received the packets from the out-
side sender. It seems that the error is caused by net-
work congestions around the gateway of the private
network.
Table 1: Packet loss rate (%).
conditions compressed raw
A) LAN 0.0 0.035
B) From LAN to 4G 0.0 0.014
C) From 4G to LAN 0.0 1.626
D) 4G network 0.0 0.020
Figure 6 shows an image of the electrocardio-
graphic data received by the receiver in the condition
A. In most conditions, the packet loss in the graph
cannot be distinguished by the unaided eye because
the packet losses seldom occur.
4.2 Delay Times
We have measured delay times of the communication
in different network environments. The results of the
raw method are in Figure 7 and the results of the com-
press method are in Figure 8. Before the experiments
the clocks of the sender and receiver are synchronized
based on the clock of the connection server. It can be
said that they work well in the four conditions: the de-
lay times of the raw method are under 100 msec; the
delay times of the compressed method are about 200
msec. Comparing the two methods, the raw method is
two times faster than the compressed method. How-
ever, delay time of the compressed method is not so
bad when we consider their performance of the packet
loss. It is considered that the compressed method is
useful for most situations for providing the telecare
services.
4.3 Changing Packet Size
We have measured the delay times by changing a pa-
rameter related to a packet size of the compressed
method. The parameter is a value of the maximum
length of a sequence in a packet described in Section
3.2.2. In the experiment, the sender and receiver con-
nect to the same 4G network. Figure 9 shows average
delay times of the compressed method by changing
limit length of the sequence in a packet. The figure
shows that changing limited length affects the delay
time and the best value is 120. In the experiments,
the shortest value, which is 60, has shown the worst
Towards a Peer-to-Peer Communication Model for Mobile Telecare Services
547
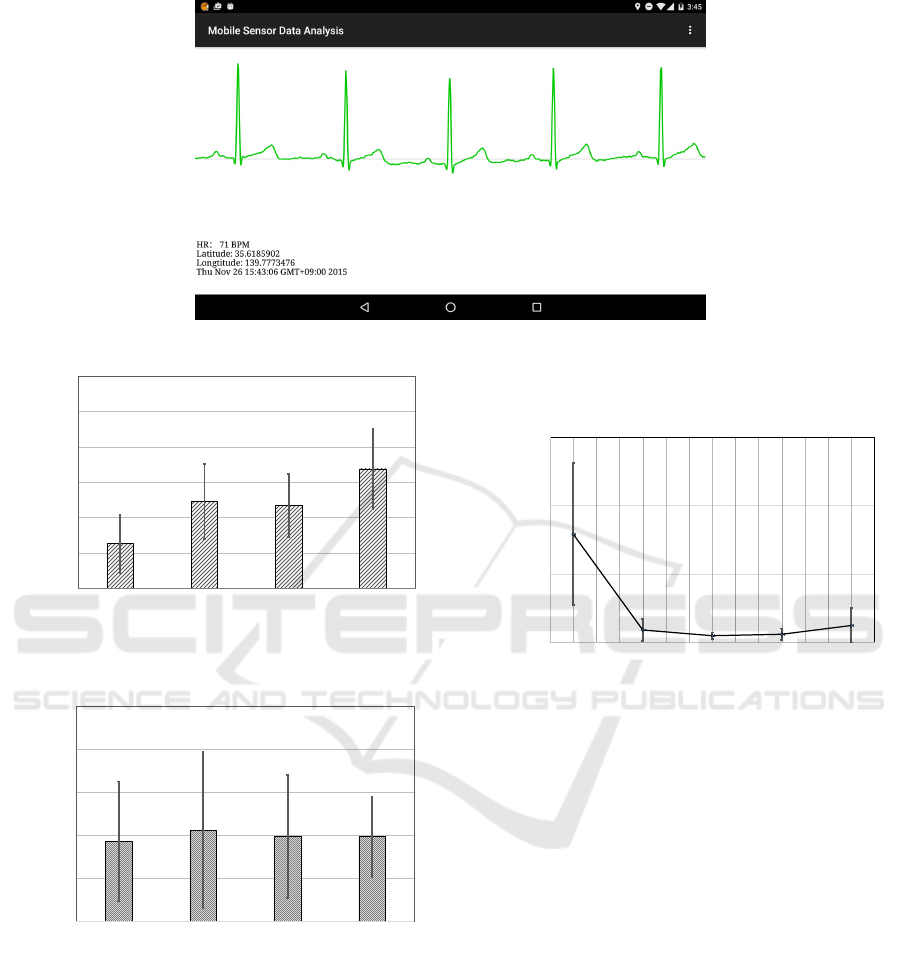
Figure 6: Display image of the received electrocardiographic data.
0
25
50
75
100
125
150
LAN From LAN
to 4G
From 4G to
LAN
4G network
msec
Figure 7: Delay times of the raw method in different net-
work environments.
0
100
200
300
400
500
LAN From LAN
to 4G
From 4G to
LAN
4G network
msec
Figure 8: Delay times f the raw method in different network
environments.
result.
In the compressed method, the sender waits to
send a next packet until it receives an ACK message
of a last sent packet. This is a reason of the packet
delay. If a packet includes a few data, it takes a lot
of time to recover the packet delay because it requires
to send many short packets. On the other hand, if a
packet with a longer sequence is used, it can recover
the packet delay by sending a few packets. Therefore
the longer values tend to show the better results in the
figure.
0
2000
4000
6000
50 70 90 110 130 150 170 190
Delay Time (msec)
Max Sequence Length (n)
Figure 9: Delay times of the compressed method changing
limit length of the sequence in a packet.
5 DISCUSSION AND FUTURE
WORK
The experimental results show that the prototype sys-
tem can establish the communication channel be-
tween the user in a private network and the user in
the outside of the network. However, it is known that
the UDP hole punching technique does not work on
some NAT routers, e.g., symmetric NAT, used in en-
terprise networks. One of our future work is devel-
oping a communication method which is adaptable to
various network environments, for examples, adopt-
ing virtual private network, the combined adoption
of server-client model and peer-to-peer model, and so
on.
As the prototype system is proposed for a proof
of concept of the peer-to-peer communication model,
it only uses general techniques for compressing and
sending the sensing data. In future work, we are go-
ing to develop the method that uses periodical patterns
SmartMedDev 2016 - Special Session on Smart Medical Devices - From Lab to Clinical Practice
548

of the sensing data, e.g., waves of electrocardiogram,
for the compression and sending mechanism. We be-
lieve that such data-driven methods can realize more
efficient communication protocol for the telecare ser-
vice.
In this paper, we focus on the technical issues of
the connection management of the model and do not
discuss security issues. Providing a telecare service
based on the client-server model, a lot of standard
security techniques for managing a Web server, e.g.,
SSL, can be also used. Providing a telecare service
based on the peer-to-peer model, however, there is no
standard way to securely manage the service system.
Designing a secure peer-to-peer telecare service for
practical use will be one of our future work.
6 CONCLUSIONS
We have described a peer-to-peer communication
model of a telecare service. The peer-to-peer tele-
care service model consists of a mobile physiologi-
cal sensor, two smartphones, and a connection man-
agement server. It enables users, such as elderly per-
sons and their caregivers, to share the telecare infor-
mation, such as electrocardiographic data, without us-
ing a central data server of the server-client model.
To realize the service in current mobile phone’s com-
munication infrastructure, we have proposed a com-
munication protocol based on a NAT-traversal tech-
nique and implemented the protocol with a compres-
sion mechanism for preventing packet loss. We have
confirmed that the prototype system works well on the
network environments that include the 4G and private
networks.
ACKNOWLEDGEMENTS
This work was supported in part by JSPS KAKENHI
Grant Number 26330125.
REFERENCES
Bellido, J. C., De Pietro, G., and Sannino, G. (2015). A
prototype of a real-time solution on mobile devices for
heart tele-auscultation. In Proceedings of the 8th ACM
International Conference on PErvasive Technologies
Related to Assistive Environments, PETRA ’15, pages
30:1–30:8, New York, NY, USA. ACM.
Deutsch, L. P. (1996). Deflate compressed data format spec-
ification version 1.3. Internet RFC 1951.
Deutsch, P. and Gailly, J.-L. (1996). Zlib compressed data
format specification version 3.3. Internet RFC 1950.
Ford, B., Srisuresh, P., and Kegel, D. (2005). Peer-to-peer
communication across network address translators. In
Proceedings of the Annual Conference on USENIX
Annual Technical Conference, ATEC ’05, pages 13–
13, Berkeley, CA, USA. USENIX Association.
Huang, Y. and Newman, K. (2012). Improve quality of care
with remote activity and fall detection using ultrasonic
sensors. In Engineering in Medicine and Biology So-
ciety (EMBC), 2012 Annual International Conference
of the IEEE, pages 5854–5857.
Lin, C.-F. (2012). Mobile telemedicine: A survey study. J.
Med. Syst., 36(2):511–520.
Lu, H., Frauendorfer, D., Rabbi, M., Mast, M. S., Chit-
taranjan, G. T., Campbell, A. T., Gatica-Perez, D., and
Choudhury, T. (2012). Stresssense: Detecting stress
in unconstrained acoustic environments using smart-
phones. In Proceedings of the 2012 ACM Conference
on Ubiquitous Computing, UbiComp ’12, pages 351–
360, New York, NY, USA. ACM.
Rosenberg, J., Weinberger, J., and Mahy-Cisco, R. (2003).
STUN-simple traversal of user datagram protocol
through network address translators. Internet RFC
3489.
Sannino, G., De Falco, I., and De Pietro, G. (2014). Effec-
tive supervised knowledge extraction for an mhealth
system for fall detection. In Roa Romero, L. M., edi-
tor, XIII Mediterranean Conference on Medical and
Biological Engineering and Computing 2013, vol-
ume 41 of IFMBE Proceedings, pages 1378–1381.
Springer International Publishing.
Sashima, A., Ikeda, T., Yamamoto, A., Kawamoto, M.,
Kuga, T., and Kurumatani, K. (2011). Developing mo-
bile physiological sensor that works with indoor posi-
tioning system. In Proceedings of the International
Conference on Indoor Positioning and Indoor Navi-
gation.
Sashima, A., Inoue, Y., Ikeda, T., Yamashita, T., Ohta,
M., and Kurumatani, K. (2008). Toward mobile
healthcare services by using everyday mobile phones.
In Proceedings of the First International Conference
on Health Informatics, HEALTHINF 2008, Funchal,
Madeira, Portugal, January 28-31, 2008, Volume 1,
pages 242–245.
Triantafyllidis, A., Koutkias, V., Chouvarda, I., and
Maglaveras, N. (2013). A pervasive health system in-
tegrating patient monitoring, status logging, and social
sharing. Biomedical and Health Informatics, IEEE
Journal of, 17(1):30–37.
Triantafyllidis, A., Velardo, C., Salvi, D., Shah, S.,
Koutkias, V., and Tarassenko, L. (2015). A survey of
mobile phone sensing, self-reporting and social shar-
ing for pervasive healthcare. Biomedical and Health
Informatics, IEEE Journal of, PP(99):1–1.
Vines, J., Lindsay, S., Pritchard, G. W., Lie, M., Greathead,
D., Olivier, P., and Brittain, K. (2013). Making fam-
ily care work: Dependence, privacy and remote home
monitoring telecare systems. In Proceedings of the
2013 ACM International Joint Conference on Perva-
sive and Ubiquitous Computing, UbiComp ’13, pages
607–616, New York, NY, USA. ACM.
Towards a Peer-to-Peer Communication Model for Mobile Telecare Services
549
