
Anaís: A Conceptual Framework for Blended Active Learning in
Healthcare
Adriano Araujo Santos
1
, José Antão Beltrão Moura
2
, Joseana Macêdo Fechine Regis de Araújo
2
and Marcelo Alves de Barros
2
1
Graduate Program in Computer Science from the Federal University of Campina Grande – UFCG,
Higher Education and Development Center – CESED, Campina Grande, Brazil
2
Systems and Computing Department, Federal University of Campina Grande, DSC/UFCG, Campina Grande, Brazil
Keywords: Anaís Conceptual Framework, Active Learning, Learning Process, Active Learning System, Blended
Learning, Medicine, Healthcare.
Abstract: The guarantee of the right to quality education is a fundamental principle for policy and management
education. In addition to the organizational processes and regulation, as well as for citizenship, currently the
student satisfaction plays a key role for the adequacy of actual courses and the needs of the educational
community who depend on them. This way, interest on active methodologies has intensified with the
emergence of new strategies that may favour the autonomy of students. Active Learning (AL) becomes an
important strategy in healthcare to the extent that theory and practice go hand in hand in the training of
health experts. This paper proposes a conceptual framework (Anaís) for active learning in healthcare studies
and summarizes a qualitative research with healthcare experts and students on the feasibility and
applicability of Anaís and its potentially positive results. Statistical tests and descriptive analysis of the
collected data indicate Anaís could indeed bring a contribution to the healthcare area in terms of benefits to
use it as an AL tool for professional training of physicians and other healthcare professionals and specialists.
1 INTRODUCTION
One of the great challenges of this new century is
balancing development of individual autonomy in
relation to that of the collective. Exploring
innovative methods that admit a pedagogical and
ethical practice at the same time that they offer
critical, reflective and transformative instruction
seems popular in the current context of education
and university curricula. Such methods are expected
to exceed the limits of purely technical training to
create new challenges that motivate students. In this
context, active methodologies studies have
intensified with the emergence of new strategies that
favour the autonomy of students, from those with the
simplest requirements to those who need physical or
technological readjustment of educational
institutions (Farias et. al, 2015
).
Active Learning (AL) instructional strategies
include a wide range of activities that share the
common element of involving students in doing
things and thinking about the things they are doing
(Bonwell and Eison, 1991). AL systems can be
created and used to engage students in (a) thinking
critically or creatively, (b) speaking with a partner,
in a small group, or with the entire class, (c)
expressing ideas through writing, (d) exploring
personal attitudes and values, (e) giving and
receiving feedback, and (f) reflecting upon the
learning process (ElDin, 2014). These interactive-
learning strategies offer students opportunities to
connect new information to their own experiences,
providing them with models for applying new
knowledge, and promoting cognitive skills.
Numerous models or strategies for clinical
teaching have been described in the medical
education literature. Recently, the inseparability of
theory and practice, the integral vision of man and
the expansion of careful design have become
essential for proper work performance (Souza,
Iglesias and Pazin-Filho, 2014).
Day after day, specialist physicians carry out
complex health analyses and must make decisions
which might be fatal, in case they are erroneous.
Santos, Moura and Araújo (2015) propose a
conceptual framework (“Anaís”) for helping in the
Santos, A., Moura, J., Araújo, J. and Barros, M.
Anaís: A Conceptual Framework for Blended Active Learning in Healthcare.
In Proceedings of the 8th International Conference on Computer Supported Education (CSEDU 2016) - Volume 2, pages 199-206
ISBN: 978-989-758-179-3
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
199

analysis and decision-making process of rare clinical
cases. The framework is based on the association of
medical evidence analysis techniques, knowledge
management and collective intelligence in order to
mitigate the risks and uncertainty faced by specialist
physicians. Anaís could also be used as an
educational tool, to help train health professionals.
The educator can set up controlled cases and submit
them to physicians being trained, so that they can
give their opinions, in a simulated environment,
building knowledge by means of interactions among
the students. This paper brings results of a
preliminary investigation on the potentiality and
usefulness of using Anaís as an AL tool for
professional training of specialist physicians.
2 RELATED WORK
The contents of this paper directly relate to Active
and Blended Learning (BL) research efforts in
higher education in general. Of particular interest are
those works that consider audiences that need to
build a knowledge expertise to make complex
decisions such as in medical diagnosis (Dx)
situations (with a computer-supported tool in
special).
The work “Web 2.0 to Support the Active
Learning Experience” showed a discussion of the
active learning literature and the appropriateness of
such strategies with net generation learners is
provided (Williams and Chinn, 2009). The study
also details the implementation of this experience
within the curriculum, and assesses the benefits and
challenges related to enhanced student learning and
engagement as well as literacy outcomes. The
authors observed that increased student engagement
was noted in both instructor and student evaluations
of the assignment.
Parmelee, DeStephen and Nicole (2009) showed
a comparative study of how medical students’
attitudes about the Team-Based Learning process
changed between the first and second year of
medical school with 180 students commenting on 19
statements regarding their attitudes about Team-
Based Learning. The result demonstrated that
students’ attitudes about working within teams, their
sense of professional development, and comfort and
satisfaction with peer evaluation improve a
curriculum using Team-Based Learning.
Cayley (2011) reviewed four specific clinical
teaching strategies and the evidence for their impact
on educational outcomes or office efficiency.
Literature for this review was selected based on the
results of a Pub Med search on the terms “medical
student” and “precepting”, review of references in
retrieved articles, and the author’s personal files.
The research conclusion was that OMP and
SNAPPS are strategies that can be used in office
precepting to improve educational processes and
outcomes, while pattern recognition and activated
demonstration show promise but need further
assessment.
Mitre et. al. (2008) aims to discuss the main
methodological transformations in the education
process of health professionals, with emphasis on
active teaching-learning methodologies. Authors
affirmed that the collective reflection, dialogue,
recognition of context and new perspectives are the
basis for the building of new avenues in the search
for wholeness of body and mind, theory and
practice, teaching and learning, reason and emotion,
science and faith, competence and loveliness. Only
through a reflective practice, critical and committed
can promote independence, freedom, dialogue and
confrontation of resistance and conflict.
Nilsson et. al. (2010) explored how clinical
teaching is carried out in a clinical environment with
medical students, looking for meaning patterns,
similarities and differences in how clinical teachers
manage clinical teaching; non-participant
observations and informal interviews were
conducted during a four month period 2004-2005.
The findings showed that three superordinate
qualitatively different ways of teaching could be
identified that fit Ramsden’s model (Ramsden,
1984).
Zaher and Ratnapalan (2012) had the objective
of identifying the format, content, and effects of
practice-based small group learning (PBSGL)
programs involving Family Physicians. Authors
affirm that there exist two main PBSGL formats
(self-directed learning and specific problems from
practice) and both formats are similar in their
ultimate goal, equally important, and well accepted
by learners and facilitators. Perceptions and learning
outcomes indicate that PBSGL constitutes a feasible
and effective method of professional development.
De Jong et. al. (2012) proposed three cases of
blended, active and collaborative learning, using a
virtual classroom, Second Life immersive virtual
world and discussion forums, blogs and wikis. They
wanted to know if blended learning can be active
and collaborative and the results of the three cases
clearly show that active, collaborative learning at a
distance is possible.
Mubuuke, Louw and Schalkwyk (2016)
proposed exploring students’ experiences of
CSEDU 2016 - 8th International Conference on Computer Supported Education
200

feedback delivery in a PBL tutorial and use this
information to design a feasible facilitator feedback
delivery guide. Individual interviews and focus
group discussions were conducted with students who
had an experience of the tutorial process in an
exploratory qualitative study. The study has
demonstrated that PBL facilitators need to provide
comprehensive feedback on the knowledge
construction process as well as give feedback on
other non-cognitive skills outside the knowledge
domain including effective communication,
adherence to ground rules and maintenance of group
dynamics.
The work “Developing an integrated framework
of problem-based learning and coaching psychology
for medical education: a participatory research”
explored a new framework by integrating the
essential features of PBL and coaching psychology
applicable to the undergraduate medical education
context (Wang et. al., 2016). Five themes emerged
from the analysis: current experience of PBL
curriculum; the roles of and relationships between
tutors and students; student group dynamics;
development of self-directed learning; and coaching
in PBL facilitation. Authors anticipate that their
investigations are useful in two ways. First, the
Coaching + PBL Model could serve to stimulate
consideration and debate as institutions develop their
own PBL concepts and procedures. Second, their
study provides insights into incorporating coaching
skills into professional development programmes for
PBL tutors and PBL curricula for students.
Blended Learning (BL) combines face-to-face
and online learning to create variable sequence of
knowledge acquisition and sharing (Bersin, 2004;
Graham, 2006). BL experiments have since evolved
to deal with richer blending options to produce
“hybrid courses” and have become frequent in
particular in many university and other higher
education courses. (CSEDU, 2010-2014). In these
hybrid courses or “flipped” classrooms, students
engage in content learning before classes in order to
maximize in-class time for active learning. In-class
active learning helps produce significant learning as
learners practice with, engage with, and apply pre-
class learning. Although experimentation with
Blended Learning (BL) is on the rise in all fields of
education, the work of Drysdale et al., (2013)
indicates that much of it is carried out at the
university level as it is the case here with our target
audience of medicine students. The works
considered in (Drysdale et al., (2013) – over 200
graduate dissertations and theses on BL – relate to
this paper in the sense that in one way or another
they investigate the benefit of BL-programs over
traditional face-to-face programs.
Subjective outcomes such as learning
effectiveness, cost effectiveness, institutional
commitment, student satisfaction, faculty
satisfaction, etc. were described (Moore, 2005).
(Arano-Ocuaman, 2010) noted that students
preferred BL classes compared to traditional classes
in the following areas: “(a) accessibility and
availability of course materials; (b) use of web-based
or electronic tools for communication and
collaboration; (c) assessment and evaluation; and (d)
student learning experiences with real-life
applications”. Similar results were found by (Barros
et al., 2015) for an innovative approach that brings
together BL and gamification strategies to a learning
process.
All these approaches suggest that, besides the
computer-based and blended learning approaches,
there is an important role played by the instructor
and students in the learning group or organization:
the role of a knowledge manager that conducts and-
or experiments a tacit-to-explicit-to-tacit knowledge
conversion cycle as preconized by Nonaka and
Takeuchi in their knowledge spiral model (Nonaka
and Takeuchi, 1999). This cycle is made up of four
modes of knowledge conversion: socialization (tacit
to tacit), externalization (tacit to explicit),
combination (explicit to explicit) and internalization
(explicit to tacit). Accordingly, before analyzing the
performance of a specific BL approach, such as that
in Anaís, against face-to-face or other learning
strategies for our target audience, it seems
appropriate to evaluate the acceptance of the
approach by the instructor as a facilitator to create
and validate different blended learning options to a
specific domain course. In this paper, we do that for
Anaís for the case of healthcare studies.
To do this we use Anaís to compose an
innovative BL environment for education in a
healthcare learning context, highlighting the
knowledge management sub-processes. This enables
the combination of tacit-to-explicit-to-tacit
knowledge conversion cycle in routine activities of a
healthcare specialist (e.g. Anamnesis process, Lab
tests) to computational techniques. The combination
thus helps the exchange of experiences amongst
participants of a healthcare team and the support of
the collective learning process.
Anaís: A Conceptual Framework for Blended Active Learning in Healthcare
201
3 ANAÍS CONCEPTUAL
FRAMEWORK
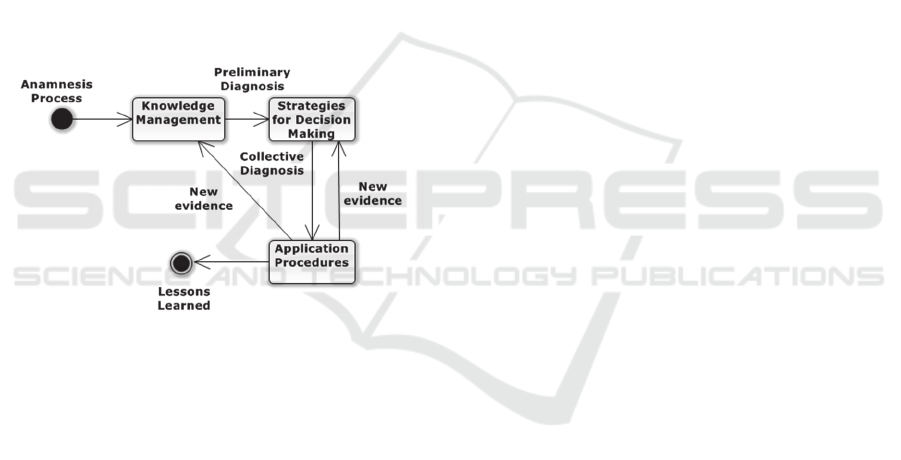
The Anaís Conceptual Framework comprises five
macro stages as illustrated in Figure 1, namely: a)
Anamnesis Process; b) Knowledge Management; c)
Decision Strategy; d) Application of Procedures and
e) Learned Lessons.
Each stage presented in the framework comprises
a set of pooled techniques which receives,
sequentially, the outputs of the previous stages. The
specialist physician in charge of the analysis of the
case is responsible for the Anamnesis, Knowledge
Management and Application of Procedures stages.
The Decision Strategy stage makes use of the Delphi
method in an attempt to achieve convergence of the
opinions of experts in the decision-making process.
The end of the process is the generation of a new
case, which is stored on the Learned Lessons
database (Santos, Moura and Araújo, 2015).
Figure 1: Anaís Conceptual Framework.
To produce the main learning outcome
(diagnosis decision making ability) the hybrid
learning concept supported by ANAÍS is created by
the movement between the three spaces of the
apprentice experience combined with the formal
"spiral" based process of knowledge conversion.
This combination blends 3 learning concepts: a)
syncronous and assyncronous computer suported
online learning experience helped by knowledge
repositories and interactive research processes, b)
active attitude of build knowledge supported by
responsible relationships with coleagues, instructor
and patients, and c) cognitive development produced
in conventional classroom and-or clinical laboratory
activities.
4 METHODOLOGY
This research is classified as an applied and
qualitative research. It aims to get the opinion of a
group of health experts and students (the target
audience of the research) on the feasibility and
applicability of the proposed Anaís framework as a
support tool to blended active problem based
learning (BAL).
We selected 60 persons using a random method
selection, 30 experts who work in Brazil's Northeast
(in the state of Paraíba) as health professionals,
academics and researchers and 30 students of
medicine. In the experiment process, we used the
Think Aloud Protocol (Think Aloud, 2016) to ensure
that all the participants understood the framework.
The reason to select students and experts in health is
analysing two different expertise and if the both
thinks the same form about the solution.
We wanted to know whether experts and
students of medicine believe that the Anaís
conceptual framework can be used as an AL tool for
professional training of specialist physicians. For
this, we developed an Anaís Conceptual Framework
to Active Learning based system. All the
participants used this system and gave their opinions
about it. They answered a questionnaire where
possible responses were in the form of a 4-level
Likert based scale: Strongly disagree = 0; Disagree =
1; Agree = 2; and, Strongly agree = 3. The sentences
presented to them were:
A. I believe that the Anaís conceptual
framework can be used as an AL tool for
professional training of specialist physicians.
B. I am satisfied with the Anaís conceptual
framework based system for active learning
and could identify many effective
contributions for the healthcare area.
C. I consider the model useful and I would
invest (time, specification effort, testing,
etc.) in its evolution.
5 ANAÍS BASED HYBRID
BLENDED ACTIVE LEARNING
The main learning outcome of the Anaís blended
active learning approach is the capability to produce
a diagnosis of a case study. Problem enunciation
(case) is proposed by the instructor and problem
analysis (case study) by the students who offer their
solution (diagnosis) with the possible assistance of
the instructor and invited professional experts on the
CSEDU 2016 - 8th International Conference on Computer Supported Education
202
healthcare case.
Activities are carried out by each group of
students in three spaces: i) the physical space of the
classroom used for intra- and inter-group, lecturer-
mediated communications, including face-to-face
classes and oral exams; ii) a virtual space in the Web
(“Anaís BAL”) that serves to synchronize and
support learning activities, including mandatory
Web lessons; to register discussion contents of the
groups; to filter initial diagnosis proposals; to
research information produced by groups in previous
cases (and saved in the Anaís BAL repository);
research of data available in the linked medical
databases as PubMed –
www.ncbi.nlm.nih.gov/pubmed/; and, iii) the real-
world surroundings of the students´ living spaces.
Students move between spaces as they are exposed
to a sequence of situations during the case study
period defined by the instructor.
The learning process is composed of 5 steps
during which, students: i) receive from the instructor
a case to study. The student leader of a group
conducts the study; ii) go through their living spaces
to carry out an anamneses while entering of data into
the web tool; iii) build collective intelligence by
converting knowledge using a Nonaka and Takeuchi
spiral to produce preliminary diagnoses; iv) make
decisions and produce a collective, convergent
diagnosis from the preliminary diagnoses; v) register
the results of case study in the Learned Lessons
database.
Initially, only cases for cardiology and
ophthalmology domains were considered (Fig 4).
Convergence was facilitated by a Delphi method
(Hsu and Sandford, 2007). Anaís BAL support for
the Nonaka and Takeuchi knowledge management
model spiral is as follows.
Socialization (tacit-to-tacit) – Anaís allows the
instructor, experts and students to share tacit
knowledge through observation, imitation, practice,
and participation in the groups and in the formal and
informal communities created around the 3 spaces of
Anaís BAL environnement. Externalization (tacit-
to-explicit) is supported by making instructor,
experts and students articulate tacit knowledge into
explicit concepts. Since tacit knowledge is highly
internalized, this process is the key to knowledge
sharing and creation to develop the collective
intelligence. Combination (explicit-to-explicit) is an
Anaís process by which students integrate different
registered knowledge used to create their
preliminary diagnoses and the final collective
diagnosis into a new knowledge system, represented
here by a new case registered in the Learned Lessons
repository -that becomes a new tool of knowledge
creation. Finally, Internalization is achieved by
embodying explicit knowledge into tacit knowledge,
by researching and reading the internal and external
sources of registered offered by Anaís BAL
repositories.
The software platform for Anaís BAL was
developed using the Visual Studio 2012 with
Microsoft ASP.NET MVC 4, Entity Framework 4
and SQL Server 2008 Express, Apache Solr 5.1.0
(text indexing), SolrNet, GoldenTrack 2009
(http://lightbase.com.br/tag/goldentrack/),GoldenAc
cess 1.2.4 (authentication system), PubMed API for
.NET, Twitter Bootstrap (UI framework –
http://getbootstrap.com/2.3.2/).
The authentication form is represented in Figure
2. All the system is Web based and the users must
have been added to GoldenAccess System
previously. There are two users’ types: the first is
instructor (with administrator powers) and the
second user type is student. The instructor can add
news cases for analysis by selecting (small) groups
of students to learn and to interact on each study
case in the collective intelligence phase (Figure 3).
The instructor plays the role of mediator in the
construction of collective knowledge. He or she
selects all cases to be studied by the groups of
students and monitors all stages throughout the
process. The student leader has the specialist
function responsible for the case study. She or he
will examine the case of information submitted by
the instructor and will be the first to submit an
Figure 2: Authentication form.
Figure 3: News cases for analysis.
Anaís: A Conceptual Framework for Blended Active Learning in Healthcare
203
assessment of the case study. For this, one could use
sources of external expertise (e.g. PubMed) and
internal (based on lessons learned). The other
students will participate in the collective intelligence
step and will have the role of assistant experts,
sharing knowledge and discussing the solution to the
case study.
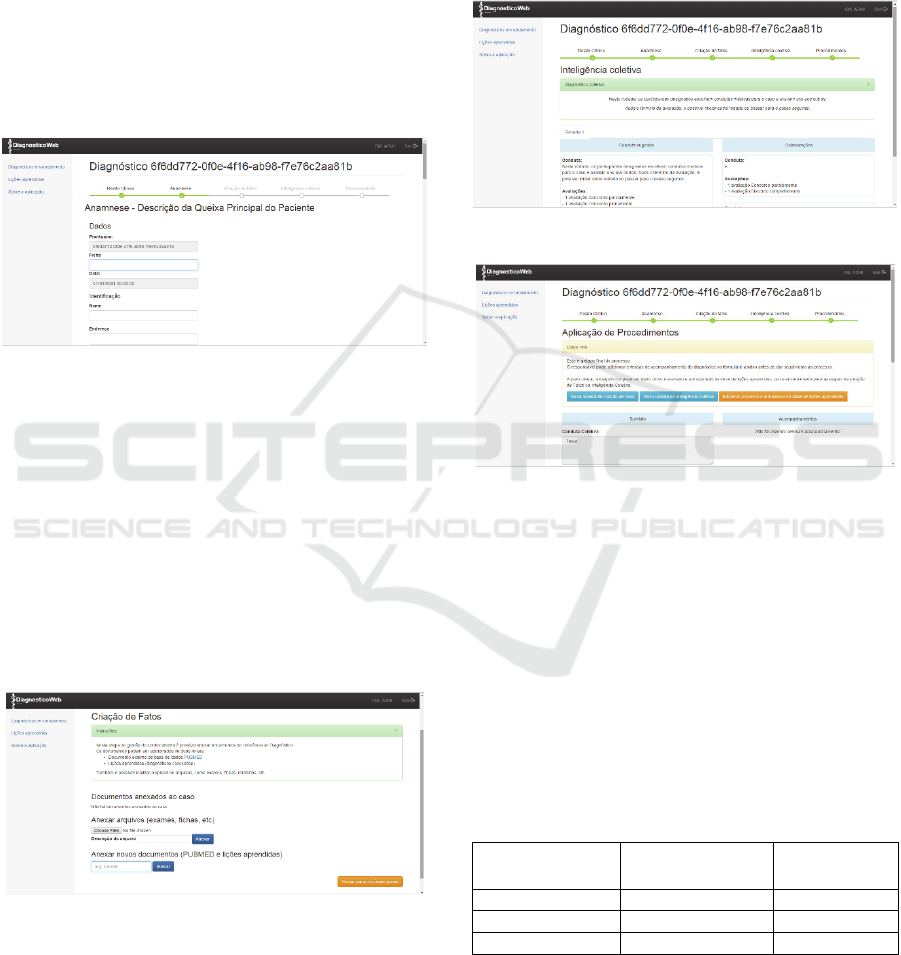
The anamnesis form is represented in Figure 4.
The student leader will add all the patient
information into the system using anamnesis
processes. The anamnesis form is adapts according
to each specialty. Here, we implemented the
anamnesis forms for cardiology and ophthalmology.
Figure 4: News cases for analysis.
Figure 5 presents a form to help tacit-to-explicit
(externalization) and explicit-to-tacit
(internalization) knowledge conversion. In this step,
the student leader user will add all the evidences
(laboratory tests, related papers, images etc.) about
the case study. The user can also look for paper in
the PubMed and in the Learned Lessons databases,
appended to the case study.
At the end of this stage, a student group may
present a preliminary diagnosis for the case study,
which will be submitted to the analysis of other
students participating in the learning process.
Figure 5: Tacit-to-Explicit knowledge conversion forms.
In the Decision Strategy step, helped by the
forms illustrated in Figure 6, for each study case, all
student groups share knowledge about the case being
studied through collective intelligence. This phase is
similar to a web forum, but convergence of all
answers is facilitated by the Delph Methodology
(Hsu and Sandford, 2007). When answer
convergence is attained, a collective diagnosis is
said to have been reached. The student leader will
then produce new evidences or create a new protocol
for saving in the Learned Lessons database (Figure
7).
Figure 6: Decision Strategy forms.
Figure 7: Learned Lessons database.
6 RESULTS AND DISCUSSIONS
This section offers statistics, graphics and
discussions on the research results for the statements
A, B and C of section 4.
We used an ordinal scale that is non-parametric
and independent of the answers to questions A, B
and C. We used the Mann-Whitney test, with
confidence level 95% and alternative no equal. The
results are shown in Table 1.
Table 1: Mann-Whitney test results.
Questions Median
Mann-
Whitney (U)
A 4 (Equals) 0,6627
B 4 (Equals) 1,0000
C 4 (Equals) 0,4965
We wanted to know whether experts and
students of medicine believes that the Anaís
conceptual framework can be used as an AL tool for
professional training of specialist physicians. The
Mann-Whitney tests showed that alternative
CSEDU 2016 - 8th International Conference on Computer Supported Education
204
hypotheses were refused (results should be
approximately the same). This shows that specialists
and students have the same positive opinion about
Anaís.
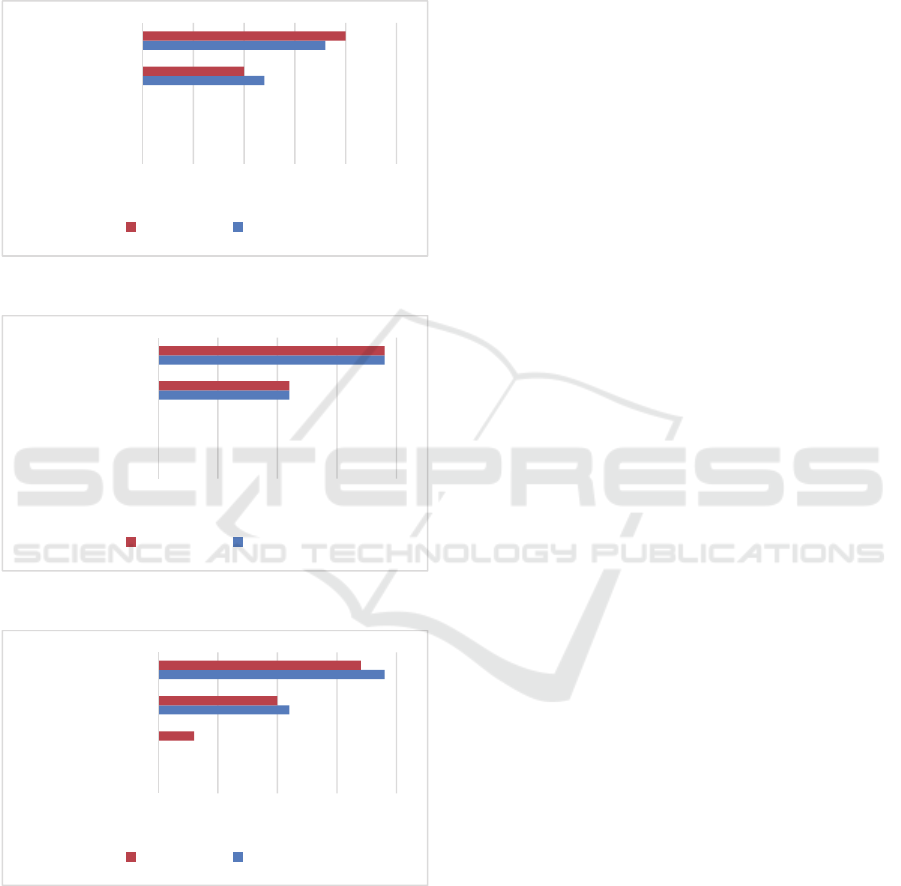
The results of the experiment in graphical form
are shown in Figures 8, 9 and 10.
Figure 8: Question A answers.
Figure 9: Question B answers.
Figure 10: Question C answers.
From Figure 8, “strongly agree” with statement
A is 63.34% (18 students and 20 specialists) while
33.66% “agree” (12 students and 10 specialists) - we
can thus say that 100% of the respondents agree that
the Anaís conceptual framework can be used as an
AL tool for professional training of specialist
physicians.
Equivalent conclusion can be drawn from the
graph in Figure 9 concerning statement B: 100% of
the users are satisfied with the Anaís conceptual
framework and could identify many effective
contributions to healthcare (63.34% - corresponding
to 19 students and 19 specialists who strongly agree,
and 33.66% - 11 students and 11 specialists who
agree with the statement).
Figure 10 shows that 60% (19 students and 17
specialists) strongly agree, 21% agree and 15% (3
specialists) disagree with statement C when they
ponder whether the model is useful and would invest
in its evolution. We believe that these answers are
biased by the time spent by specialists in equivalent
research. Sometimes specialists have their own
research on equivalent topics and students are more
interested in completing subject requirements
quickly.
Results from statistical tests, and also with the
descriptive data analysis, indicate that, in the opinion
of the specialists and the students, Anaís offers a
contribution to the area of healthcare studies and it
will bring benefits to learning as a BAL tool for
professional training of specialist physicians.
7 CONCLUSIONS
Anaís was proposed originally (Santos, Moura and
Araújo, 2015) to apply knowledge management
principles of tacit-to-explicit-to-tacit knowledge in
learning experiences. This research reported in this
paper aimed at eliciting opinions of specialists and
students in the healthcare area regarding the Anaís
conceptual framework as an effective BAL tool for
professional training of specialist physicians.
For that, 60 persons (30 health professionals and
30 students of medicine) were interviewed. They
used the Anaís conceptual framework based system
in a blended active learning scenario, and answered
a questionnaire to assess whether they thought the
proposed framework was valid BAL tool for
professional training of physicians. Preliminary
validation results are promising.
As for future work, we will concentrate on
further evaluating the BAL tool and on studying of
other cases with more specialists and students for
extended validations.
ACKNOWLEDGEMENTS
This work is being carried out with support from the
0
0
12
18
0
0
10
20
0 5 10 15 20 25
Stronglydisagree
Disagree
Agree
Stronglyagree
Specialists Students
0
0
11
19
0
0
11
19
0 5 10 15 20
Stronglydisagree
Disagree
Agree
Stronglyagree
Specialists Students
0
0
11
19
0
3
10
17
0 5 10 15 20
Stronglydisagree
Disagree
Agree
Stronglyagree
Specialists Students
Anaís: A Conceptual Framework for Blended Active Learning in Healthcare
205

Brazilian Agency for the Improvement of Higher
Education Personnel (CAPES).
REFERENCES
Arano-Ocuaman, J., 2010., Differences in student
knowledge and perception of learning experiences
among non-traditional students in blended and face-
to-face classroom delivery. University of Missouri—
Saint Louis, USA.
Barros, M, Moura, A, Borgman, L., Terton, U.:Blended
Learning in Multi-disciplinary Classrooms -
Experiments in a Lecture about Numerical Analysis.
CSEDU (2) 2015: 196-204.
Bersin, J., 2004., The Blended Learning Book:
BestPractices, Proven Methodologies, and Lessons
Learned. John Wiley & Sons.
Bonwell, C., & Eison, J. 1991. Active learning: Creating
excitement in the classroom (ASHE-ERIC Higher
Education Report No. 1). Washington, DC: George
Washington University. Abstract online at
http://www.ed.gov/databases/ERIC_Digests/ed340272
.html.
Cayley WE. 2011. Effective clinical education: strategies
for teaching medical students and residents in the
office. WMJ. 2011;110:178–1.c.
CSEDU 2011, Proceedings of International Conference
on Computer Supported Education [online]. [Accessed
15 October 2014]. Available from:
http://pubs.iids.org/index.php/publications/show/1814.
De Jong, N. et. al. 2014. Blended learning in health
education: three case studies.Perspect Med Educ
3:278–288. DOI 10.1007/s40037-014-0108-1.
Drysdale, J.S., Graham, C.R., Spring, K.J., and Halverson,
L.R., 2013., An analysis of research trends in
dissertations and theses studying blended learning.
Internet and Higher Education, 17., pp. 90-100.
ElDin, Y. K. Z. 2014. Implementing Interactive Nursing
Administrationlectures and identifying its influence on
students’ learning gains. Journal of Nursing Education
and Practice. Vol. 4, No. 5.
Farias, P. A. M. de, et al. 2015. Active Learning in Health
Education: Historic Background and Applications.
Revista brasileira de educação médica.
Hsu, C., Sandford, B. A. 2007. The Delphi Technique:
Making Sense of Consensus. Practical Assessment,
Research & Evaluation. Vol 12, No 10.
Mitre, S. M. et. al. 2008. Active teaching-learning
methodologies in health education: current debates.
Ciênc. saúde coletiva vol.13 suppl.2 Rio de Janeiro
Dec.
Moore, J. 2005. Is Higher Education Ready for
Transformative Learning? A Question Explored in the
Study of Sustainability. Journal of Transformative
Education. Vol. 3: 76-91.
Mubuuke, A. G. Louw, A. J. N. and Schalkwyk, S. V.
2016. Utilizing students’ experiences and opinions of
feedback during problem based learning tutorials to
develop a facilitator feedback guide: an exploratory
qualitative study. BMC Medical Education.16:6. DOI
10.1186/s12909-015-0507-y.
Nilsson, M. S. et. al. 2010. Pedagogical strategies used in
clinical medical education: an observational study.
BMC Medical Education.
Nonaka, I. Takeuchi, H.. The Knowledge-Creating
Company: How Japanese Companies Create the
Dynamics of Innovation. Oxford University Press,
1995.
O’Sullivan DW and Copper CL. Evaluating active
learning. 2003. A New Initiative for a General
Chemistry Curriculum. Journal of College Science
Teaching. 32(7): 448-52.
Parmelee, Dean X. DeStephen, D. Borges, Nicole J. 2009.
Medical Students’ Attitudes about Team-Based
Learning in a Pre-Clinical Curriculum. Med Educ
Online [serial online].14:1 doi;10.3885/
meo.2009.Res00280. Available from http://www.med-
ed-online.org.
Ramsden, P. 1984. The context of learning. In F. Marton,
D. Hounsell & N. Entwistle (Eds.) The experience of
learning (pp. 144-164). Edinburgh: Scottish Academic
Press.
Theexperience of learning (pp. 144-164). Edinburgh:
Scottish Academic Press.
Think Aloud. [Accessed 10 January 2016]. Available
from:http://www.nngroup.com/articles/thinking-aloud-
the-1-usability-tool/.
Santos A. A, Moura J. A, Araújo J. M. de. 2015.A
Conceptual Framework for Decision-making Support
in Uncertainty- and Risk-based Diagnosis of Rare
Clinical Cases by Specialist Physicians. Studies in
Health Technology and Informatics. Volume 216:
MEDINFO 2015: eHealth-enabled Health.
Souza, C. da S. Iglesias, A. G. Pazin-Filho, A. 2014. New
approaches to traditional learning – general aspects.
Medicina (Ribeirão Preto);47(3): 284-92.
Wang, Q. et. al. 2016. Developing an integrated
framework of problem-based learning and coaching
psychology for medical education: a participatory
research. BMC Medical Education. 16:2. DOI
10.1186/s12909-015-0516-x.
Williams, J. Chinn, S. J. 2009. Using Web 2.0 to Support
the Active Learning Experience. Journal of
Information Systems Education, Vol. 20.
Zaher, E. Ratnapalan, S. 2012. Practice-based small group
learning programs. Can Fam Physician;58:637-42.
CSEDU 2016 - 8th International Conference on Computer Supported Education
206
