
In-vitro Force Assessments of an Autoclavable Instrumented Sternal
Retractor
Giovanni Saggio
1
, Giuseppe Tancredi
1
, Laura Sbernini
1
, Costantino Del Gaudio
2
,
Alessandra Bianco
2
and Jacob Zeitani
3
1
Dept. of Electronic Engineering, University of Rome “Tor Vergata”, Rome, Italy
2
Dept. of Enterprise Engineering, INSTM Research Unit, University of Rome “Tor Vergata”, Rome, Italy
3
German Hospital Tirana, Tirana, Albania
Keywords: Chronic Chest Pain, Instrumented Retractor, Median Sternotomy, Force Sensor.
Abstract: It is well known that median sternotomy might lead to rib and/or sternum micro/macro-fractures and/or
brachial plexus injuries, eventually resulting in chronic pain with significant impact on patient’s quality
life.Postoperative chronic pain is recognized as a multifactorial complex issue, it has been assessed that
excessive sternum retraction forces can be considered one of these factors. On this basis, the Authors
developed a reliable and sterilizable system potentially able to real-time monitor and control the retraction
forces along the hemisternums. A Finochietto sternal retractor was instrumented by means of ultra-thin
force sensors interfaced with ad hoc electronic circuitry. Two different sets of sensors were adopted, one of
which able to support autoclave operating conditions. In vitro tests were performed by means of a made on
purpose dummy. The instrumented retractor allows monitoring of the force exerted on both the arms during
the opening procedure. Force versus time patterns were real-time acquired and stored, distribution of forces
was determined along with the values of mean, maximum and plateau force. Results demonstrate the
reliability of the instrumented retractor in measuring forces, up to 400N. Cost-effectiveness and feasibility
can be considered further additional values of the proposed instrumented retractor.
1 INTRODUCTION
Persistent postoperative pain following sternotomy
is the Achilles’ heel of surgical procedures because
it can lead to patients’ discomfort, increased
morbidity, prolonged hospital stay, and increasing
costs (Wildgaard, 2001 and Hazelrigg, 2002).
Chronic pain has been defined as pain in the location
of surgery, different from that suffered pre-
operatively, arising post-operatively and persisting
beyond three months. Recently, in a prospective
study, Van Gulik et al. (Van Gulik, 2011) identified
a number of independent predictors for the
development of persistent thoracic pain following
sternotomy including non-elective surgery, re-
sternotomy shortly after the original surgery and
severe pain on the third postoperative day. In this
study, at one year, 42 (35%) patients reported
chronic thoracic pain. Similarly, another study
reported the prevalence of post-operative pain as
high as 39.3% at the mean time of 28 months after
surgery (Bruce, 2003). Meyerson et al. in 2001
(Meyerson, 2001) estimated a 28% overall incidence
of non-cardiac pain one year after surgery. Several
studies assessed that women are substantially more
likely to suffer early and chronic postoperative pain
than men (Van Gulik, 2011 and Ochroch, 2006) and
that the prevalence of post-sternotomy chronic pain
decreases with age (Van Gulik, 2011 and Meyerson,
2001). Chronic post-sternotomy pain can be related
to secondary sternal osteomyelitis, incomplete bone
healing, sternocostal chondritis, and surgical
technique of internal mammary(Bolotin, 2007 and
Aigner, 2013).
Indeed, Aigner et al. 2013 (Aigner, 2013)
pointed artery harvesting (required for myocardial
revascularization) and, particularly, mechanical
trauma associated to improperly applied sternal
retractors that might lead to rib and sternum
fractures (Van Gulik, 2011; Woodring, 1985; Unlu,
2007).Of course the relevance of this issue is
expected to be different for each individual patient
in terms of a number of variables such as weight,
age, osteoporosis and cartilage calcification.
Saggio G., Tancredi G., Sbernini L., Del Gaudio C., Bianco A. and Zeitani J.
In-vitro Force Assessments of an Autoclavable Instrumented Sternal Retractor.
DOI: 10.5220/0006111300250031
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 25-31
ISBN: 978-989-758-216-5
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
25
To access to the mediastinum, retractors are used
to allow adequate surgical field (Steele, 2013).
Hemisternums separation might lead to rib fracture,
eventually associated to brachial plexus injury (BPI)
(Baisden, 1984; Greenwald, 1983; Gumbs, 1991;
Healey, 2013; Suzuki, 1991).
Median sternotomy provides a wide access to the
thoracic cavity. It is considered the standard
approach for open heart surgical procedures, but it is
also a useful incision for a number of other
operations. It is well known that a certain risk of
chronic pain is associated to the extent of the force
impressed during sternum opening due to rib
fractured and/or BPI. Thus, there is an actual clinical
need to provide to the surgeons suitable
instrumented retractors able to monitor in real time
the forces exerted on the two halves during the
sternum opening procedure. Furthermore, with the
increasing interest of shifting the cardiac surgery
procedures from full to partial sternotomy, including
the “J” and “T” incisions, the proposed study might
be useful to evaluate and compare the forces applied
on the sternum in the various surgical approaches to
determine the best access to that supposed to be the
optimal sternum separation allowing at the same
time the optimal surgical view.
Only few data are available for the actual value
of the forces exerted by a retractor on the skeletal
cage and all reported studies have been conducted
on corpses or animal models. Data obtained from
human patients are not presently available in the
literature probably due to the lack of an
instrumented sternal retractor readily suitable for the
translation to surgery.
For this purpose, we designed and realized a
sterilizable system based on a commonly adopted
straight sternal retractor (Finochietto) equipped with
ultrathin force sensors and conditioning electronic
circuitry. The forces experienced during the
retraction were monitored in real-time by means of a
home-made dummy.
The idea is to acquire data on the intensity and
distribution of exerted retraction forces during
hemisternums separation, in view of future
challenging clinical studies aimed at reducing the
risk of chronic post-sternotomy pain.
2 MATERIALS
A commonly adopted straight sternal
retractor,Finochietto type (Figure 1a) was equipped
with ultra-thin force sensors and conditioning
electronic circuitry. This instrument was tested by
means of a home-made dummy.
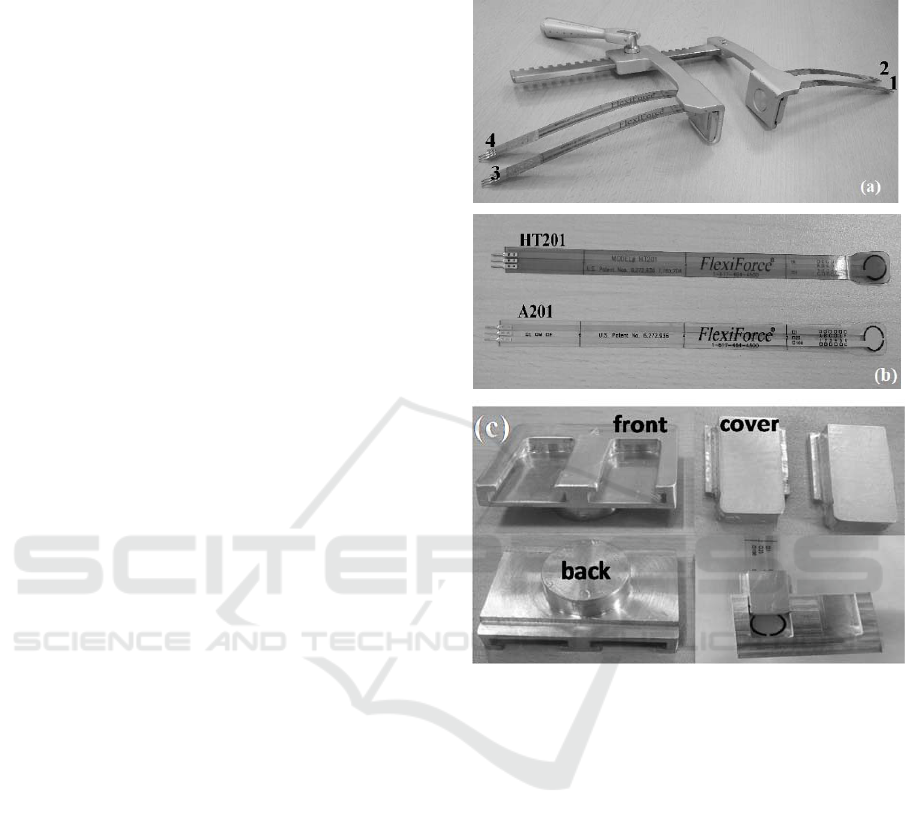
Figure 1: (a) The Finochietto retractor equipped with the
four sensors placed in positions designed from 1 to 4
according to the figure. (b) The ultra-thin force sensors,
HT201 (top) and A201 (bottom) types. (c) Aluminum
sensors’ housings: front, back and cover.
2.1 Force Sensors
We considered two different types of commercial
piezo-resistive flexible ultra-thin (0.203mm,
0.008in.) off-the-shelf force sensors, the
FlexiForce® A201 (these according to Aigner et al.,
2013) and the FlexiForce® HT201 (both types by
Tekscan, Boston, USA), having a circular sensing
area of 9.53mm (0.375in.) in diameter (Figure 1b).
The A201 type, with a polyester substrate, can
measure forces up to 440N, within a temperature
operating range of -9°C to +60°C (15°F to 140°F).
The HT201 type, with a polyimide substrate, can
measure forces up to 445N, within -9°C to +204°C
(15°F to 400°F).
BIODEVICES 2017 - 10th International Conference on Biomedical Electronics and Devices
26
2.2 Electronic Circuitry
The electronic circuitry was developed on the basis
of a previous one, which was made to interface flex
and electromyography sensors (Saggio,2016). In
particular, the electrical resistance values (outputs of
the sensors) were converted into voltages by means
of voltage dividers. Those voltage signals fed an
electronic circuitry, based on Luigino328 (an
Arduino-compatible microcontroller board based on
an ATMega328 MCU), which operated 10bit digital
conversions and sent data to a personal computer via
USB port at a sampling rate of 175Hz. The
following data process was handled by ad-hoc
home-made LabVIEW routines (National
Instruments, Austin, TX, USA).
2.3 Sternal Retractor
An aluminum straight Finochietto retractor (by
Tekno-Medical Optik-Chirurgie GmbH Tuttlingen,
Germany) was equipped with an array of four force
sensors. Two sensors were placed on the blade of the
mobile arm and two on the blade of the fixed arm
(Figure 1a), the size of the blade being 44.4mm
(1.75in.) in length and 30.9mm (1.22in.) in width.
The sum of the single detected forces on each blade
yielded the total force for both the fixed and the
mobile arm. The ultra-thin force sensors were placed
in ad-hoc smooth aluminum housings (Figure 1c).
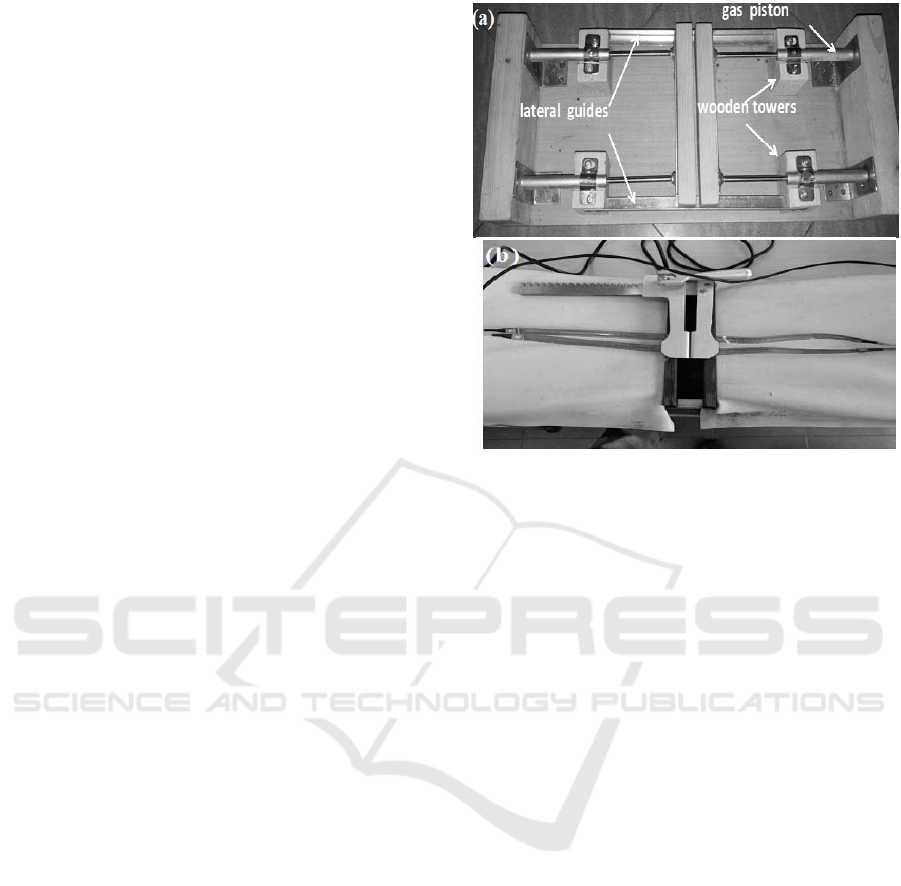
2.4 In Vitro Test
In vitro tests of the instrumented retractor were
performed by means of a made on purposedummy
built up with four gas pistons (manufactured by
Team Pro), two for each side, laterally anchored to a
wooden shell (Figure 2a). Different set of gas
pistons were evaluated, i.e.150N, 100N and 80N.On
the basis of several opening/closing cycles
performed by three different surgeons, the dummy
equipped with the 80N pistons offered the most
realistic feeling with respect to the clinical practice.
The Authors are aware that the mechanics of the
proposed dummy is very simple with respect to the
complex biomechanics of the rib cage. Anyway, the
idea was to realize a dummy able to support the test
of the device and not meant to be taken as a
biomechanical model of the rib cage.
Figure 2: (a) The home made dummy built up using four
gas pistons fixed to a wooden skeleton, the compressible
parts positioned outward in a face-to-face configuration. In
vitro tests: (b) the instrumented Finochietto retractor
positioned into the dummy.
3 METHODS
Beforehand, eight sensors of each type were
characterized in terms of electrical resistance versus
applied force (R vs F), by means of an universal
tensile test machine (LRX, by Lloyd Instruments,
Berwyn, PA, US). In order to investigate if HT201
sensors can effectively support autoclaving
conditions, these sensors were also characterized
following the same procedure after five cycles of
autoclave treatment (VaporMatic 770, AsalSrl,
Milan, Italy).
Test procedure consisted in four opening/closing
cycles of the dummy by means of the instrumented
retractor up to two different fixed widths, i.e.5cm
(1.97in.) and 10cm (3.94in.). On the basis of the
feeling/practice of the surgeons, each
opening/closing cycle was performed at a roughly
constant rate of 2s/cm, that is 10s for 5cm (1.97in.)
and 20s for 10cm (3.94in.). The two final positions
(5cm, 1.97in. and 10cm, 3.94in.) were held for 60s
so to evidence response decay, if any. The response
of all the sensors in term of force (F) versus time (t)
was real-time acquired. Then, mean force (F
mean
),
maximum force (F
max
) and plateau force (F
plateau
)
were evaluated, the latter as the mean value of the
force recorded during 60s in the final rest position.
In-vitro Force Assessments of an Autoclavable Instrumented Sternal Retractor
27
The distribution of the forces exerted along the two
halves of the dummy was also determined.
4 RESULTS AND DISCUSSION
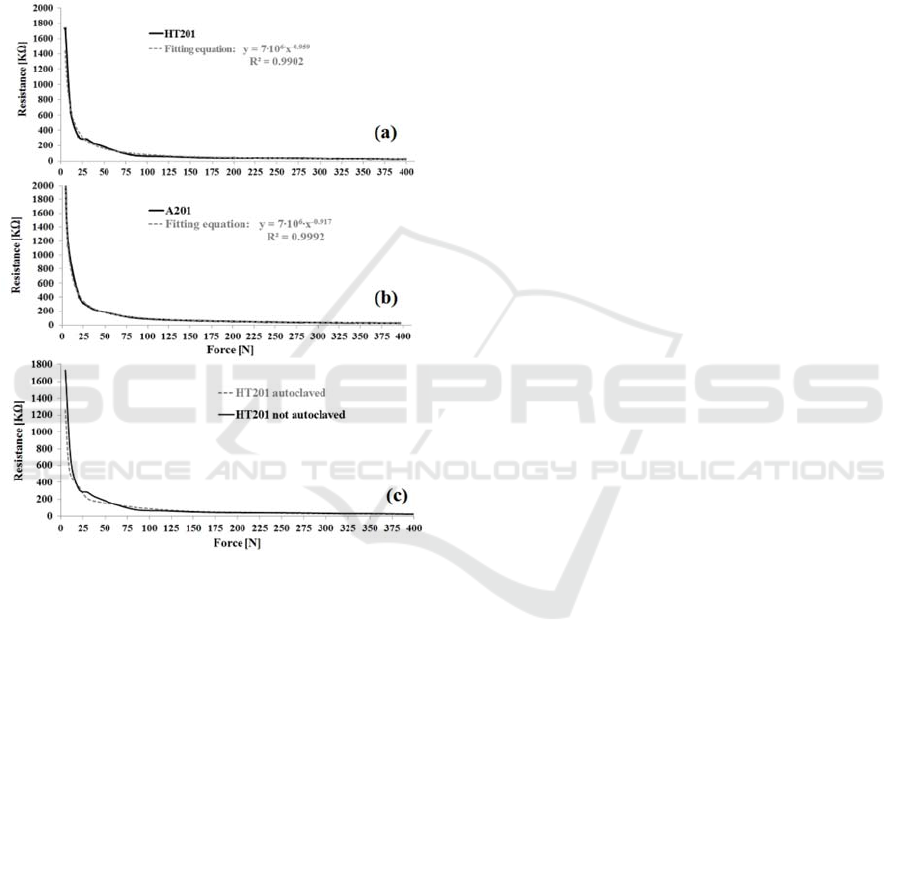
Ultrathin flexible force sensors HT201 and A201
both showed exponential resistance decay with the
impressed force (Figure 3a-b).
Figure 3: Measured resistance versus force (R vs. F) for
different sensor (a) HT201 type, (b) A201 type and (c)
H201 type in comparison before and after autoclave
treatments.
Moreover, HT201 sensors did not show a
significantly different behaviour after five cycles of
autoclave conditioning (Figure 3c), which is
reasonable result since these sensors have been
specifically designed for high temperature
applications (up to 400°F, approximately 200°C). In
any case, in the occurrence of degradation in
performances, those sensors can be easily and
conveniently replaced.
The investigated range of force (i.e. 5-400N)
includes the values reported by Bolotin et al.
(Bolotin, 2007) and by Aigner et al. (Aigner, 2013).
In more details, Bolotin et al. in 2007 reported the
first known successfully attempt to employ an
instrumented retractor to monitor forces during
cardiothoracic surgery. They equipped stainless steel
curved profile retractor blades with strain gauges to
measure applied forces during retraction, and
reported results for lateral thoracotomy and median
sternotomy on cadavers and sheep. The average
force applied during force-controlled retraction was
(77.88±38.85N) and the maximum force displayed
during force-controlled retraction
(323.99±127.79N).
Aigner et al. equipped a straight (SSR) (MTEZ
424 735; Heintel GmbH, Vienna, Austria) and a
curved retractor (CSR) (Dubost Thoracic Retractor
DC30000-00; Delacroix-Chevalier, Paris, France),
with FlexiForce sensors, A201 type (Tekscan Inc).
The blade of the mobile arm of the SSR (length 6.5
cm and width 4.5cm) was equipped with two arrays
of 4 sensors, and the mobile arm of the CSR (length
9.7cm, width 4.8cm, curvature radius 21cm) was
equipped with two arrays of 5 sensors. The sum of
the single sensor forces yielded the total force. Force
distribution, total force and displacement were
recorded to a spread width of 10cm in 18 corpses
(11 males and 7 females). For every corpse, 4
measurement iterations were performed for both
retractors; each retraction was performed in
14.3±6.2s to reach 10cm widespread. The Authors
concluded that the shape of sternal retractors
considerably influences the force distribution on the
sternal incision. On the other side, it is reported that
the total mean retraction force was not significant
different between SSR and CSR (222.8±52.9N
versus 226.4±71.9N). Nevertheless, the recorded
mean total force was remarkably dependent on the
gender. For the first retraction, it was 256.2±43.3N
for males and only 174.9±52.9N for females.
Moreover, in the case of SSR the forces on the
cranial and caudal sternum are significantly higher
than in the median section. For SSR the maximum
total force for full retraction was 349.4±77.9N,
while force distribution during the first retraction for
the cranial/median/caudal part of the sternum was
101.5±43.9/29.1 ±33.9/63.0 ±31.4N.
Aigner et al assessed that the force distribution
did not change significantly for the other 3
retractions, for the different investigated spread
widths (i.e. 5, 7.5, and 10cm) and not gender-
dependent. The maximum force for full retraction
was 493.6N, whereas the smallest maximum force
was 159.0 N.
Results obtained for HT201 sensors are resumed
in Table I and the typical force (N) versus time (s)
patterns are presented in Figure 4-5.
BIODEVICES 2017 - 10th International Conference on Biomedical Electronics and Devices
28
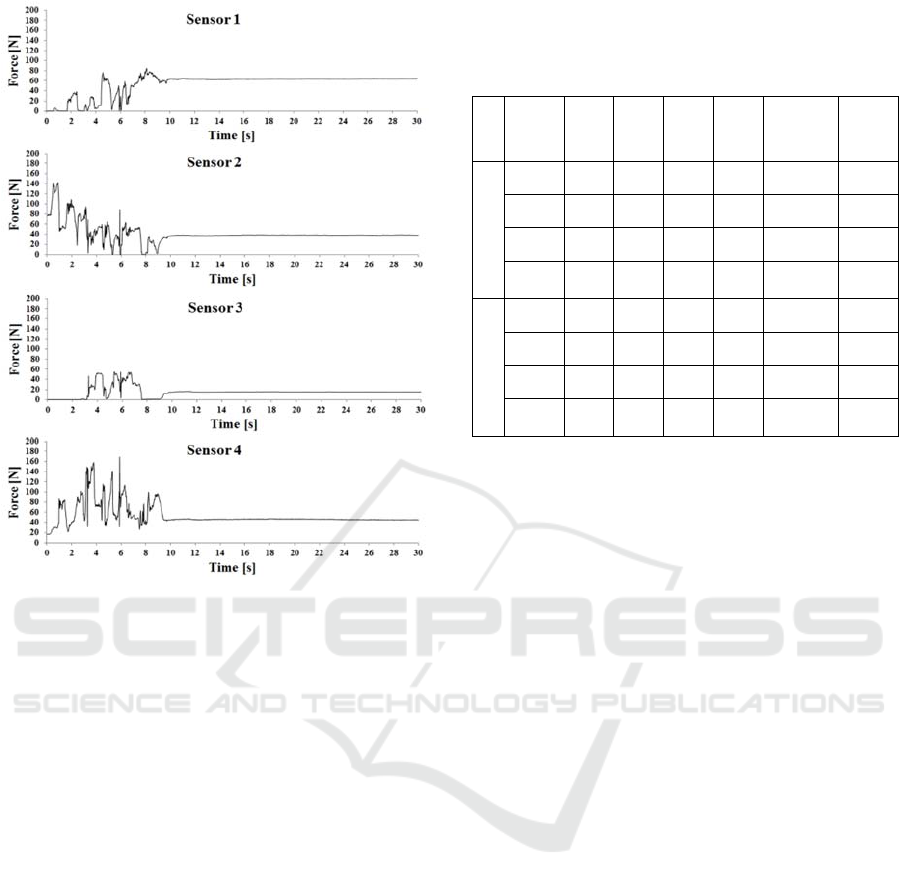
Figure 4: Response of the four sensors (housed as shown
in Figure 1a) in terms of force [N] versus time [s] during
the 5cm opening procedure.
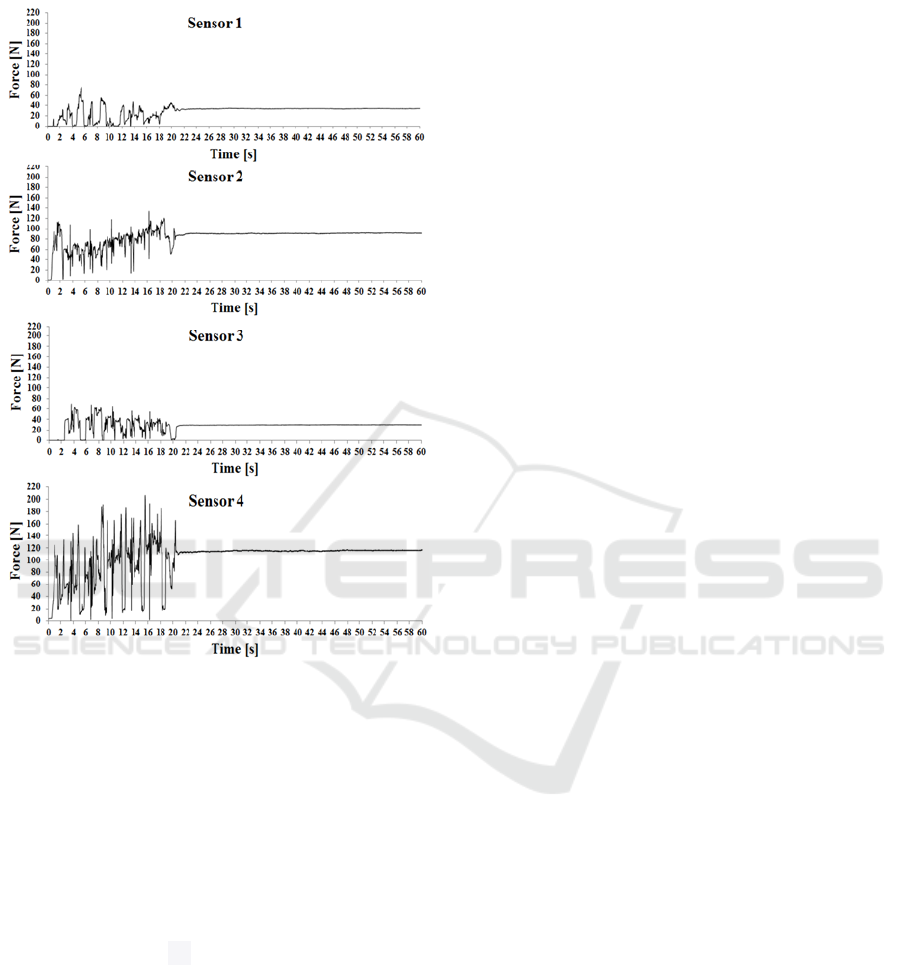
In all cases, a high stability of the response to a fixed
exerted force was evidenced. In fact, the value of
F
plateau
showed a mean standard deviation as low as
0.33±0.16N. Some valuable information can be
obtained from the acquired data. For example, the
total average force for the mobile blade ranged
between 60.1±6.0N for 5cm spread and 98.0±36.5N
for 10cm spread, as expected for a dummy built-up
with 80N gas pistons. The deviation with respect to
this value is also expected and has to be attributed to
the uneven pressure distribution onto the circular
sensors due to the rough surface finishing of the
contact area i.e. wood in the dummy.
It is interesting to observe during the retraction,
the Finochietto experienced along the mobile arm a
total F
max
(sensor#4 + sensor#3) that exceeded 200N,
ranging from 219.1±9.7N for 5cm spread and
266.6±25.4N for 10cm spread.
The force distribution along the retractor blade is
also particularly interesting. In fact, in all cases, the
highest maximum force (F
max
) was detected by
sensor #4 positioned on the mobile arm in proximal
(cranial) position (Figure 4-5), the value ranged
between 156.4±12.5N for 5cm spread and
199.7±21.2N for 10cm spread. The lowest F
max
Table 1: Values of the mean, maximum and plateau forces
(expressed in N) measured by HT201sensors positioned
according to Figure 1a (i.e. S1, S2, S3, S4). The related
standard deviation values are reported in parentheses.
sprea
d
Force
[N]
S1 S2 S3 S4
S1+S2
fixedblad
e
S3+S4
mobile
blade
5cm
mean
60.8
(5.7)
39.2
(4.4)
18.3
(2.1)
41.8
(7.7)
100.1
(8.5)
60.1
(6.1)
max
97.3
(10.6)
115.0
(19.5)
62.7
(5.4)
156.4
(12.5)
212.2 (14.8)
219.1
(9.7)
plateau
63.9
(5.8)
39.4
(4.9)
17.9
(1.8)
38.3
(8.3)
103.3
(9.0)
56.3
(7.2)
max-
mean
36.5
(8.7)
75.7
(21.1)
44.4
(4.0)
114.6
(12.9)
112.2 (12.5)
159.0
(12.6)
10cm
mean
37.6
(8.8)
82.5
(5.60)
15.2
(10.4)
82.8
(26.8)
120.1 (12.8)
98.0
(36.5)
max
79.6
(17.5)
126.3
(6.62)
66.9
(4.3)
199.7
(21.3)
205.9 (20.8)
266.6
(25.4)
plateau
41.2
(6.7)
89.1
(7.02)
13.1
(12.9)
84.7
(32.0)
130.2 (11.7)
97.8
(44.4)
max-
mean
42.0
(14.1)
43.8
(6.98)
54.7
(9.4)
116.9
(16.9)
85.8
(13.6)
168.6
(26.3)
values were 62.7±5.4N for 5cm and 66.9±4.3N for
10cm, registered in correspondence of sensor #3 of
the mobile arm in distal (caudal) position.
Interestingly, median sternotomy in corpses
performed by means of a straight sternal retractor
gave a comparable force distribution (Aigner, 2013).
This result suggests that the made-on-purpose
dummy enable to perform reliable test and thus it
might also be employed by surgeons in order to
assess their own learning curve for each specific
instrumented retractor.
Furthermore, sensor #4 detected also the highest
value of (F
max
-F
mean
), i.e. 114.6±12.9N and
116.9±16.9N, respectively for 10cm and 5cm
opening. For all the other sensors, this value does
not exceed 75.7±21.1N, independently from the
position on the retractor.
On the basis of these results, the presented
implementation system can be considered a valuable
tool to evaluate intensity and distribution of
retraction forces in human patients for conventional
sternotomy procedures. On the basis of our
knowledge, these data are not yet available in the
Literature. As already previously suggested by
Bolotin (Bolotin, 2007), the final goal is to develop
clinical studies aimed at coherently correlating the
biomechanical information obtained for a specific
surgical procedure with the incidence of post-
sternotomy chronic pain. In this respect, for
example, the actual outcomes of cranial versus
caudal positioning of the sternal retractor could be
assessed. On the basis of our knowledge, in the past
decade such kinds of studies have not yet been
performed probably due to the lack of an
In-vitro Force Assessments of an Autoclavable Instrumented Sternal Retractor
29
implemented user-friendly retractor suitable for
conventional clinical sterilization process.
Figure 5: Response of the four sensors (housed as showed
in Figure 1a) in terms of force [N] versus time [s] during
the 10cm opening procedure.
Moreover, the performance of this versatile
design might also contribute to estimate the actual
impact of minimally invasive cardiac surgery
techniques. In fact, since the 1990s, these procedures
are receiving an increasing interest due to a number
of potential advantages with respect to traditional
sternotomy, including reduced operative trauma, less
perioperative morbidity along with improved
aesthetic outcomes, shorter hospital stay and
accelerated rehabilitation (Ward, 2013). According
to recent studies, the overall outcomes and costs are
believed to be comparable with those of
conventional sternotomy (Reser, 2015; Alturi,
2015). It has to be considered that partial
sternotomy, in minimally invasive cardiac surgery
procedures, allows the displacement of only a part of
the hemithorax, the latter might be subject to
increased exerted forces eventually leading to
excessive stress on the “dynamic” chest wall. The
proposed study might be useful in the clinical setting
to determine the optimal balance between surgical
field and sternum separation.
The system can be considered cost-effective and
potentially adaptable to different surgical retractors
simply providing the appropriate housings.
5 CONCLUSIONS
This study demonstrates that the proposed system
allows performing measurements of retraction forces
in the range 5-400N using different models of
flexible force sensors; in particular Flexiforce A201
and HT201, the latter being suitable to operate in a
temperature range compatible with conventional
autoclave procedures. The implemented system was
thus demonstrated to be able to support autoclave
sterilization either removing or keeping in place the
force sensors, thus eventually allowing the reuse of
the HT201 sensors, which is more cost-effective
than a disposable use. In this perspective, we plan in
future work to investigate the maximum number of
autoclaving cycles that preserve the performances of
HT201 and other ultrathin force sensors available on
the market.
The user-friendly and low cost developed system
allowed at instantaneously measuring, displaying
and storing the force versus time pattern for each
sensor, during and after the opening phase. Accurate
and reliable data were obtained, in terms of
maximum force, mean force, total force and force
distribution. Measurements were acquired in real
time and readily available on a computer monitor.
ACKNOWLEDGEMENTS
The Authors wish to thank Antonella Camaioni for
help in autoclaving procedures, Andrea Iovino for
technical support in the early stage of device design.
REFERENCES
Aigner, P., Eskandary, F., Schlöglhofer, T., Gottardi, R.,
Aumayr, K., Laufer, G., Schima, H., 2013.Sternal
force distribution during median sternotomy
retraction.J.Thorac.Cardiovasc. Surg., 146(6), pp.
1381-1386.
Atluri, P., Stetson, R. L., Hung, G., Gaffey, A. C., Szeto,
W. Y., Acker, M. A., & Hargrove, W. C. (2016).
Minimally invasive mitral valve surgery is associated
with equivalent cost and shorter hospital stay when
BIODEVICES 2017 - 10th International Conference on Biomedical Electronics and Devices
30

compared with traditional sternotomy. The Journal of
thoracic and cardiovascular surgery, 151(2), 385-388.
Baisden, C.E., Greenwald, L.V., Symbas, P.N., 1984.
Occult rib fractures and brachial plexus injury
following median sternotomy for open-heart
operations.Ann.Thorac. Surg., 38(3), pp. 192-194.
Bolotin, G., Buckner, G. D., Jardine, N.J., Kiefer, A.J.,
Campbell, N.B., Kocherginsky, M., Raman, J.,
Jeevanandam, V., 2007.A novel instrumented retractor
to monitor tissue-disruptive forces during lateral
thoracotomy. J. Thorac. Cardiovasc. Surg. 133(4), pp.
949-954.
Bruce, J., Drury, N., Poobalan, A.S., Jeffrey, R.R., Smith,
W.C., Chambers, W.A., 2003. The prevalence of
chronic chest and leg pain following cardiac surgery: a
historical cohort study. Pain, 104(1-2), pp. 265-273.
Gjeilo, K. H., Klepstad, P., Wahba, A., Lydersen, S.,
&Stenseth, R., 2010, “Chronic pain after cardiac
surgery: a prospective study,”
ActaanaesthesiologicaScandinavica, 54(1), pp. 70-78.
Greenwald, L.V., Baisden, C.E., Symbas, P.N., 1983. Rib
fractures in coronary bypass patients: radionuclide
detection. Radiology, 148(2), pp. 553-554.
Hazelrigg, S. R., Cetindag, I. B., Fullerton J., 2002.Acute
and chronic pain syndromes after thoracic surgery.
Surg. Clin. North Am., 82(4), pp. 849–865.
Healey, S., O’Neill, B., Bilal, H., Waterworth, P.,
2013.Does retraction of the sternum during median
sternotomy result in brachial plexus injuries?.
Interactive CardioVascular and Thoracic Surgery,
17(1), pp. 151–158.
Meyerson, J., Thelin, S., Gordh, T., Karlsten, R., 2001.The
incidence of chronic poststernotomy pain after cardiac
surgery - a prospective study, ActaAnaesthesiol.
Scand., 45(8), pp. 940-944.
Ochroch, E.A., Gottschalk, A., Troxel, A.B., Farrar, J.T.,
2006. Women suffer more short and long-term pain
than men after major thoracotomy.Clin. J. Pain, 22(5),
pp. 491-498.
Reser, D., Holubec, T., Caliskan, E., Guidotti, A.,
Maisano, F., 2015. Left anterior small thoracotomy for
minimally invasive coronary artery bypass
grafting.Multimed.Man.Cardiothorac.Surg., pp. 1-5.
Riillo, F., Bagnato, C., Allievi, A. G., Takagi, A., Fabrizi,
L., Saggio, G., Arichi, T., Burdet, E., 2016. A Simple
fMRI Compatible Robotic Stimulator to Study the
Neural Mechanisms of Touch and Pain.Annals of
biomedical engineering, 1-11.
Saggio, G., Orengo, G., Leggieri A., 2016. Sensory Glove
and Surface EMG with Suitable Conditioning
Electronics for Extended Monitoring and Functional
Hand Assessment. Proc. 9th Int. Joint Conf. on
Biomedical Engineering Systems and Technologies
(BIOSTEC), co-located 9th Int. Conf. on Bio-inspired
Systems and Signal Processing (BIOSIGNALS), 21-
23 February 2016, Rome, Italy.
Steele, P.R.C., Curran, J.F., Mountain, R.E., 2013. Current
and future practices in surgical retraction. The Surgeon
11(6), pp. 330–337.
Suzuki, S., Kikuchi, K., Takagi, K., Masuda, H., Yoshizu,
H., Tanaka, S., Ogata, T., 1990. Brachial plexus injury
and fracture of the first rib as complications of median
sternotomy. Journal of the Japanese Association for
Thoracic Surgery, 38(9), pp. 1459-1462.
Unlu, Y., Velioglu, Y., Kocak, H., Becit, N., Ceviz, M.,
2007.Brachial plexus injury following median
sternotomy. Interactive CardioVascular and Thoracic
Surgery, 6, pp. 235–237.
vanGulik, L., Janssen, L.I., Ahlers, S.J.G.M., Bruins, P.,
Driessen, A.H.G., van Boven, W.J., van Dongen,
E.P.A., Knibbe C.A.J., 2011. Risk factors for chronic
thoracic pain after cardiac surgery via
sternotomy.European Journal of Cardio-thoracic
Surgery, 40(6), pp.1309-1313.
Ward, A.F., Grossi, E.A., Galloway, A.C., 2013.
Minimally invasive mitral surgery through right mini-
thoracotomy under direct vision. J Thorac Dis., 5( 6),
pp. 673-679.
Wildgaard, K., and Kehlet, H., 2011. Persistent
Postsurgical Pain Syndromes, Chronic post-
thoracotomy pain—What is new in pathogenic
mechanisms and strategies for prevention?.Techniques
in regional anesthesia and pain management, 15(3),
pp. 83–89.
Woodring, J.H., Royer, J. M., Todd, E.P., 1985.Upper Rib
Fractures Following Median Sternotomy. The Annals
of Thoracic Surgery, 39(4), pp. 355–357.
In-vitro Force Assessments of an Autoclavable Instrumented Sternal Retractor
31
