
Electrohysterogram Signals from Patients with Threatened Preterm
Labor: Concentric Ring Electrode Vs Disk Electrode Recordings
Javier Mas-Cabo
1
, Yiyao Ye-Lin
1
, Carlos Benalcazar-Parra
1
, José Alberola-Rubio
1
, Alfredo Perales
2
,
Javier Garcia-Casado
1
and Gema Prats-Boluda
1
1
Centro de Investigación e Innovación en Bioingeniería (Ci2B), Universitat Politècnica de València, Valencia, Spain
2
Servicio de Obstetricia, Hospital Universitari I Politècnic la Fe, Valencia, Spain
Keywords: Electrohysterogram, Preterm Labor, Concentric Ring Electrodes.
Abstract: Recording of electrohysterogram (EHG) has emerged as a non-invasive method for monitoring uterine
dynamics during pregnancy. Usually EHG is picked up using conventional disk electrodes placed on the
abdominal surface resulting in a limited spatial resolution due to the blurring effect of the volume conductor.
In this respect, concentric ring electrodes have been proposed to pick up uterine myoelectrical activity in term
patients so as to improve spatial resolution and to reduce physiological interferences embedded in these
records. The aim of the present work is to check the feasibility of recording EHG signals using concentric
ring electrodes (BC-EHG) in patients with threatened preterm labor and to compare their capability to
discriminate true preterm labor from false alarms with that of conventional EHG bipolar recording. For this
purpose, 50 sessions with simultaneous EHG recordings with conventional disk electrodes and concentric
ring electrodes were conducted in 26 patients. Compared to conventional bipolar EHG recording, the BC-
EHG presents smaller amplitude and similar spectral characteristics. Statistically significant differences
between women who delivered preterm and those that delivered at term were found for both the average peak-
peak amplitude and the dominant frequency in the frequency range 0.2-1 Hz from BC-EHG recordings.
Nonetheless no EHG parameter from simultaneous conventional bipolar recording showed statistically
significant differences. These results suggest superior performance of BC-EHG recordings in patients with
threatened preterm labor for discriminating true preterm labor from term labor.
1 INTRODUCTION
Preterm birth (<37 weeks of gestation, WG) is one of
the major cause of early neonatal mortality. The
incidence of preterm birth has risen over the last
decades, representing around 12% of all labors
nowadays (Beck, 2010). Preterm labor also
implicates around 85% of newborn deaths and 50%
of newborns’ neurological disorders (Beck, 2010).
Currently due to the lack of specific tools, the
diagnosis of preterm labor is one of the most complex
problems faced by clinicians.
The gold standard for monitoring uterine
dynamics is the use of an intra-uterine catheter, which
provides a quantitative measure of intra-uterine
pressure associated to the uterine contractions. It is an
invasive technique which requires ruptured
membranes and entails risks such as infection, and
thus it is unsuitable for predicting preterm labor
during pregnancy. In common practice, obstetricians
use tocodynamometry (TOCO) for assessing uterine
contractility and evaluating the risk of preterm labor.
This technique measures non-invasively the uterine
pressure transmitted to the abdominal surface.
However, it suffers from recurrent signal failure,
needing re-positioning by a midwife (Miles, 2001,
Schlembach, 2009), and may also fail in obese
patients (Euliano, 2013). Furthermore, TOCO is not
able to distinguish effective contractions which lead
to preterm delivery, from non-effective ones (
Schlembach, 2009, Garfield, 2007). Recording of
electrohysterom (EHG) has emerged as an alternative
technique for non-invasively monitoring uterine
contractility (Devedeux, 1993, Garfield, 2005,
Maner, 2007). The electrohysterogram corresponds
to the uterine myoelectric recordings and it is made
up of action potential bursts (EHG-burst), associated
to uterine contraction, and basal activity. EHG signals
78
Mas-Cabo J., Ye-Lin Y., Benalcazar-Parra C., Alberola-Rubio J., Perales A., Garcia-Casado J. and Prats-Boluda G.
Electrohysterogram Signals from Patients with Threatened Preterm Labor: Concentric Ring Electrode Vs Disk Electrode Recordings.
DOI: 10.5220/0006155000780083
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 78-83
ISBN: 978-989-758-212-7
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
present different characteristics along the gestation
and depending on the proximity of labor (Garfield,
2007, Marque, 2007), which could provide
information for estimating the time horizon of labor.
Some parameters extracted from EHG signals, such
as those related with conduction velocity or
propagation patterns, are very promising for the
prediction of term and preterm delivery (Lucovnik,
2011, Euliano, 2009, Rabotti, 2009, Rabotti, 2010).
Nevertheless, the estimation of conduction velocity
depends on the direction of propagation of
contraction in relation to the electrodes position
(Rabotti, 2011). Moreover, it can also be influenced
by the poor spatial resolution associated to
conventional disk electrodes due to the blurring effect
of the volume conductor (Ye-Lin, 2015).
In this sense, concentric ring electrodes (CRE)
have been proposed to improve the spatial resolution
achieved with conventional disk electrodes and to
reduce physiological interferences embedded in EHG
recordings (Alberola-Rubio, 2013). Specifically,
these electrodes have proven to pick up uterine
myoelectrical activity in patients at term (≥ 37 WG),
(Ye-Lin, 2015). Nonetheless, since the EHG-burst
amplitude of patients at earlier WG is expected to be
lower than those obtained from patients at term
(Devedeux, 1993, Garfield, 2005), the utility of CRE
for predicting preterm labor in patients with
threatened preterm labor still needs to be proven.
Therefore, the first aim of the present work was to
determine if concentric ring electrodes are able to
pick up the EHG in patients at early gestational age
(< 37 WG). Secondly, it was aimed to explore the
possibility to discriminate true preterm labor from
false alarms of patients with threatened preterm labor
based on BC-EHG and bipolar EHG records.
Specifically, in this first approach it was studied the
possible differences in EHG temporal and spectral
parameters of patients who end up delivering preterm
and those who did it at term.
2 MATERIALS AND METHODS
2.1 Data Acquisition
50 recording sessions were conducted in 26 patients
with singleton pregnancies at the Hospital
Universitario y Politécnico La Fe de Valencia. This
study adheres to the Declaration of Helsinki and was
approved hospitably the Institutional Review Board.
The patients were informed about the nature of the
study and the recording protocol and they signed an
informed consent form. The criteria for inclusion in
this study were: women with a gestational age
between 25 and 36 weeks with symptoms of preterm
labor, such as regular uterine contractions and/or
cervical effacement. Patients’ obstetric information
was collected, as shown in Table 1, and patients were
followed up to obtain the details of their final
delivery. It should be highlight that cervical length
shows a shortening as labor approaches, and higher
values of this parameter can be observed for the term
group in comparison to preterm labor group.
Term and preterm labor patients were grouped
into two subgroups depending on the gestational age
at recording moment: term [28, 31[ WG group (6
patients and 8 records), term [31, 34[ WG group (10
patients and 14 records), preterm [28, 31[ WG group
(4 patients and 5 records) and preterm [31, 34[ WG
group (6 patients and 23 records). Patients who
presented threatened preterm labor but did not initiate
labor spontaneously were excluded from the study.
Besides the EHG registers were performed under
common clinical practice conditions, this implies that
most patients were under tocolytic drugs effect. For
each recording session, the abdominal skin was
carefully prepared using an abrasive paste in order to
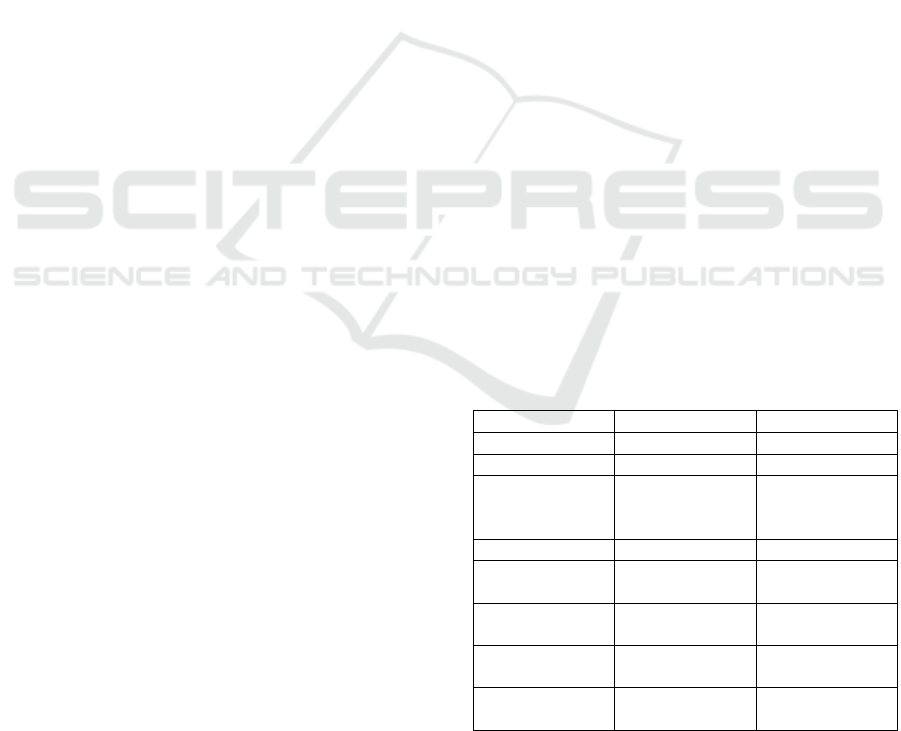
reduce skin-electrode impedance. Two disposable
Ag/AgCl electrodes (EL501, Biopac SystemsInc,
Santa Barbara, CA, USA) were placed
supraumbilically, symmetrically arranged with
respect to the uterine median axis being the inter-
electrode distance 8 cm (see Figure 1). Furthermore,
a custom-made concentric ring electrode was placed
on the uterine median axis in the subumbilical zone
(see Figure 1).
Table 1. Patients’ obstetrical information at the recording
moment.
Term labor Preterm labor
Gestations 1.59 ±1.10 1.50 ±1.10
Parity 0.23 ±0.43 0.23 ±0.43
Voluntary
Interruption of
Pregnancy
0.13 ±0.47 0.07 ±0.36
Abortions 0.22 ±0.68 0.20 ±0.76
Cesarean
Sections
0.09 ±0.29 0.00 ± 0.00
Maternal age
(years)
32.55 ± 5.70 30.47 ±5.16
Gestational Age
(weeks)
31.05 ± 2.54 31.87 ±1.55
Cervical length
(mm)
24.95 ± 10.17 15.37 ± 11.28
Electrohysterogram Signals from Patients with Threatened Preterm Labor: Concentric Ring Electrode Vs Disk Electrode Recordings
79
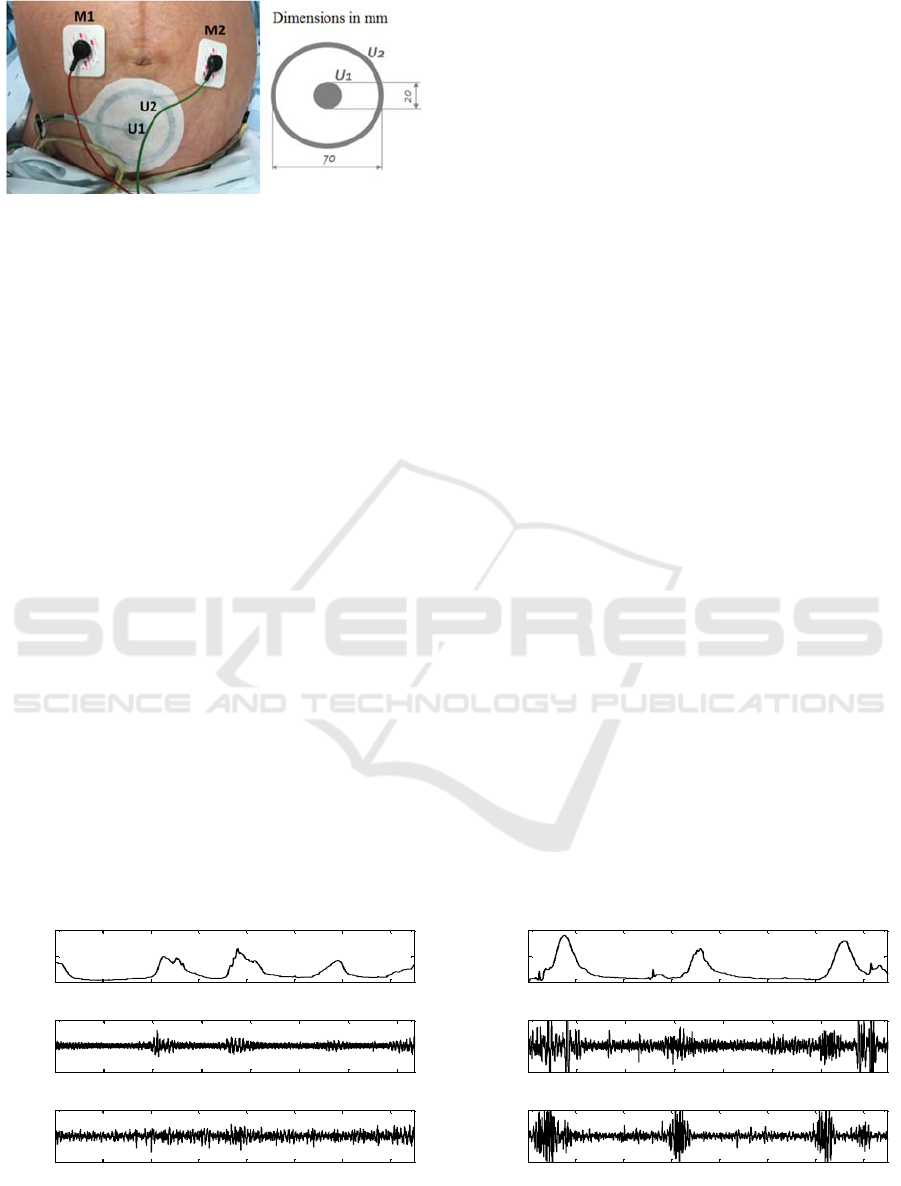
Figure 1: Scheme of the electrodes’ placement on a
woman’s abdomen (left) and CRE dimensions (right).
Taking into account that the EHG-burst amplitude
acquired using CRE with an outer ring of 36 mm was
about 42 V in patients at term (Ye-Lin, 2015), in this
work it has been designed a CRE with an outer ring
of 70 mm so as to facilitate picking up the uterine
electrical activity during early pregnancy whose
amplitude was expected to be smaller than that
associated to term patients. Furthermore, two
disposable Ag/AgCl electrodes were placed in each
hip, as reference and ground electrodes. In this work,
the bipolar recording estimated from the two
monopolar raw signals from conventional disk
electrodes and one bipolar concentric-EHG (BC-
EHG) signal obtained by means of CRE were
analysed (see Figure 1).
Bipolar = M1 – M2; BC-EHG = U2-U1; (1)
Where M1 and M2 are the biopotentials picked up
by conventional disk electrodes and U1 and U2 are
the biopotentials corresponding to the central disk and
external ring respectively. Two custom-made
amplifiers which provide a 2059 V/V gain in the
frequency band between 0.1 and 4 Hz were used for
signal conditioning (Alberola-Rubio, 2015).
The implementation details of the bioamplifier
were described in a previous work (Ye-Lin, 2016).
Signals were digitalized using a 24 bits ADC and
sampled at 20 Hz. TOCO signal was simultaneously
acquired by means of a Corometric 170 from GE
Medical Systems and the digitalized data were
transmitted to a PC with a sampling frequency of 4
Hz.
2.2 Data Analysis
Most studies in this field are focused on the analysis
of the EHG-burst (Garfield, 2005, Maner, 2007),
which usually requires manual segmentation of the
EHG recordings. This process depends on the
experts’ subjectivity and it is a time-consuming task
(Fele-Zorz, 2008). In this work, it was preferred to
analyse the whole EHG recording which greatly
simplifies the signal analysis process. Signal
segments corresponding to motion artefacts were
discarded from the analysis. Subsequently a set of
temporal and spectral parameters was calculated for
the EHG signals: average peak to peak amplitude,
mean frequency, dominant frequency in frequency
range 0.2-1 Hz (DF
1
) and in frequency range 0.34-1
Hz (DF
2
), normalized subband energies in frequency
ranges 0.2-0.34 Hz (NE1), 0.34-0.6 Hz (NE2) and
0.6-1 Hz (NE3) and H/L ratio, which is the ratio
between the energy in high frequency range (0.34-1
Hz) respect to the energy in low frequency range (0.2-
0.34 Hz) (Ye-Lin, 2015). Specifically, the peak-peak
amplitude was worked out over a moving window of
120s length and 50% overlapping, and then the
average value of all analysed windows was
calculated. Similarly, for the estimation of the
spectral parameters, the Welch periodogram was
worked out in moving analysis windows of 120 s with
50% overlapping.
Figure 2: Simultaneous recording of TOCO, bipolar, BC-EHG performed in two patients at 33 WG. Left: recordings from a
woman who delivered at term. Right: recordings from a woman who delivered preterm.
0 100 200 300 400 500 600 700
0
50
100
TOCO (mmHg)
Term Labor
0 100 200 300 400 500 600 700
-200
0
200
Bipolar (
V)
0 100 200 300 400 500 600 700
-20
0
20
BC-EHG (
V)
Time (s)
0 100 200 300 400 500 600 700
0
50
100
TOCO (mmHg)
Preterm Labor
0 100 200 300 400 500 600 700
-200
0
200
Bipolar (
V)
0 100 200 300 400 500 600 700
-50
0
50
BC-EHG (
V)
Time (s)
BIOSIGNALS 2017 - 10th International Conference on Bio-inspired Systems and Signal Processing
80
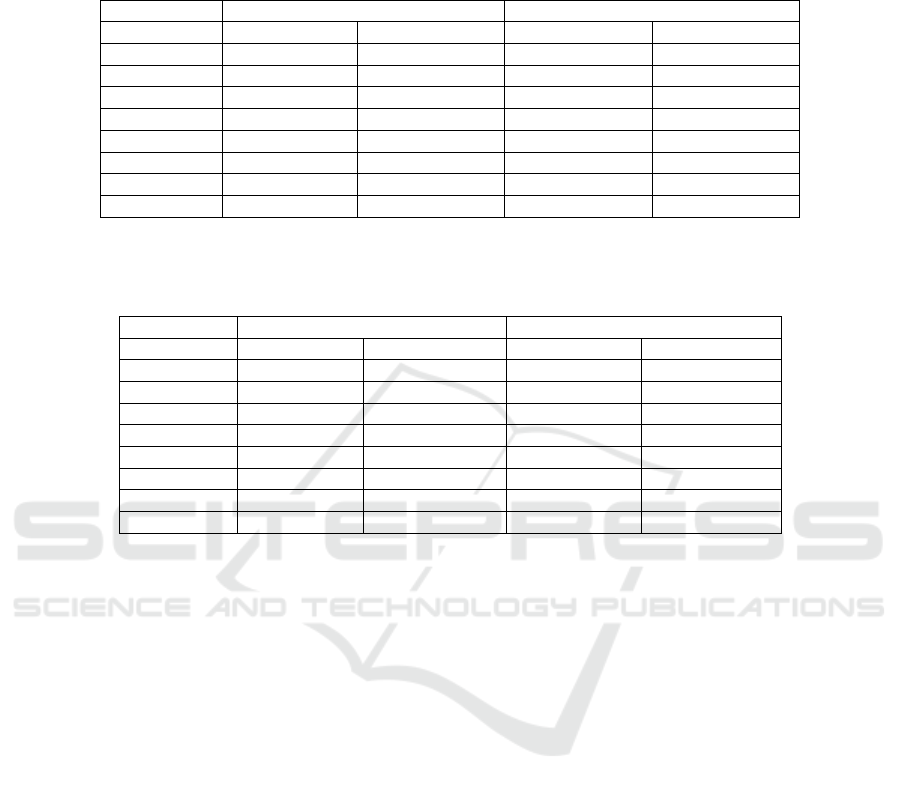
Table 2: EHG Parameters obtained from conventional bipolar recordings for both term labor and preterm labor groups,
separated into two sets depending on the gestational age at the recording session. ‘*’ indicates statistically significant
differences (p<0.05) between term labor and preterm labor groups for the same set of WG; and ‘’ indicates statistically
significant differences (p<0.05) between conventional bipolar record and BC-EHG (table 3) for each of the 4 subgroups.
Bipolar
Term labor Preterm labor
Parameter [28, 31[ WG [31, 34[ WG [28, 31[ WG [31, 34[ WG
App (µV) 98.85 ± 35.3 127.56 ± 31.33 157.18 ± 41.34 151.46 ± 77.92
MF (Hz) 0.366 ± 0.018 0.338 ± 0.021 0.381 ± 0.034 0.353 ± 0.025
DF1 (Hz) 0.237 ± 0.023 0.234 ± 0.021 0.229 ± 0.037 0.241 ± 0.035
DF2 (Hz) 0.367 ± 0.031 0.357 ± 0.012 0.355 ± 0.012 0.366 ± 0.024
NE1 0.56 ± 0.12 0.65 ± 0.11 0.53 ± 0.1 0.63 ± 0.08
NE2 0.35 ± 0.12 0.27 ± 0.08 0.36 ± 0.07 0.28 ± 0.06
NE3 0.09 ± 0.02 0.09 ± 0.07 0.11 ± 0.04 0.09 ± 0.03
H/L Ratio 0.85 ± 0.38 0.6 ± 0.35 0.93 ± 0.34 0.6 ± 0.19
Table 3: EHG Parameters obtained from BC-EHG recordings for both term labor and preterm labor group, separated into two
sets depending on the gestational week at the recording session. ‘*’ indicates statistically significant differences between term
and preterm labor groups for the same set of WG.
BC-EHG
Term labor Preterm labor
Parameter [28, 31[ WG [31, 34[ WG [28, 31[ WG [31, 34[ WG
App (µV) 52.72 ± 17.18 60.86 ± 37.96 97.68 ±18.49* 90.1 ± 46.16*
MF (Hz) 0.387 ± 0.017 0.358 ± 0.022 0.379 ± 0.025 0.365 ± 0.031
DF1 (Hz) 0.224 ± 0.029 0.212 ± 0.008 0.234 ± 0.028 0.237 ± 0.044*
DF2 (Hz) 0.378 ± 0.031 0.381 ± 0.026 0.391 ± 0.042 0.371 ± 0.026
NE
1
0.54 ± 0.06 0.60 ± 0.08 0.53 ± 0.05 0.58 ± 0.09
NE
2
0.33 ± 0.04 0.31 ± 0.08 0.35 ± 0.04 0.32 ± 0.07
NE
3
0.13 ± 0.03 0.09 ± 0.03 0.11 ± 0.04 0.10 ± 0.04
H/L Ratio 0.87 ± 0.17 0.70 ± 0.24 0.89 ± 0.17 0.76 ± 0.3
Wilcoxon test was performed in order to
determine if there were statistically significant
differences between the EHG parameters derived
from preterm labor group and term labor group for
both [28, 31[ WG and [31, 34[ WG subgroups.
3 RESULTS
Figure 2 shows 750 s of simultaneous recordings of
TOCO, bipolar and BC-EHG signals performed in
two patients at 33 WG, one who delivered at term and
other who delivered preterm. Firstly, each uterine
contraction observed in the tocographic signal was
associated to an increase of signal amplitude in
bipolar recording for both patients. In the case of the
patient who delivered preterm, it can be clearly
identified the presence of uterine contractions in BC-
EHG signals. By contrast, for the patient who
delivered at term, only uterine contractions around
400 s and 700 s, which are of greater intensity, can be
observed in BC-EHG recording. The contractions
around 200 s and 600 s are hardly noticeable, being
imbedded in the basal activity. Secondly, the
amplitude of EHG signals acquired with CRE was
smaller than that from signals obtained using
conventional disk electrodes. Finally, it can also be
clearly observed that the amplitudes of the EHG-
bursts of the patient whose labor was preterm is
higher than those of the patient that delivered at term
(false alarm), even when both records were made at
the same WG.
Tables 2 and 3 show mean and standard deviation
of the EHG parameters calculated from Bipolar and
BC-EHG recordings respectively. Firstly, it can be
noticed that BC-EHG signals presented lower peak-
peak amplitude than conventional bipolar ones. In
fact, the amplitude is the only parameter that shows
statistically significant difference between BC-EHG
signals and bipolar signals (squares) for both [28, 31[
WG and [31, 34[ WG groups. Comparing EHG
parameters in the sets of same ranges of WG, the
average amplitude of preterm labor group was higher
than those of term labor group for both bipolar and
BC-EHG recording. However, such difference was
statistically significant only for BC-EHG. Regarding
spectral parameters, it is noticeable that only DF1 for
the set [31, 34 WG] presented statistically significant
differences between term labor and preterm labor,
and again only for BC-EHG signals.
Electrohysterogram Signals from Patients with Threatened Preterm Labor: Concentric Ring Electrode Vs Disk Electrode Recordings
81

4 DISCUSSION
In the present work, it was tested and confirmed the
feasibility of picking up the uterine electrical activity
using CRE at early gestational ages. No statistically
significant differences were found between EHG
parameters derived from bipolar and BC-EHG
recording, apart from the peak to peak amplitude.
Conventional bipolar EHG signals presented higher
amplitude than BC-EHG, which may be due to the
fact that CRE presented a relatively smaller
interelectrode distance. This result agrees with other
authors who has acquired both bipolar and BC-EHG
in patients at term (> 37 weeks of gestation) (Ye-Lin,
2015). Moreover, bipolar and BC-EHG signals
presented similar spectral characteristics in the target
signal bandwidth.
Then it was explored the capability of bipolar and
BC-EHG recordings to discriminate between women
with threatened preterm labor who will deliver
preterm of those who deliver at term. In comparison
to term group, bipolar EHG signals from preterm
group presented higher peak to peak amplitude and
greater spectral content in high frequency range. This
result is accordance with other authors that computed
temporal and spectral parameters to characterize the
EHG recording
(Garfield, 2005, Maner, 2003,
Marque, 2007
). Nevertheless, our data did not show
statistically significant differences in spectral
parameters obtained from bipolar recording as
reported by other authors (Maner, 2003, Maner, 2007,
Fele-Zorz, 2008). Maner et al. focused on the DF2
estimated from the EHG-burst associated to uterine
contractions. In that work DF2 of preterm labor group
presented significantly higher values than those of
term labor group. The fact that in the present work the
whole EHG recording is analysed, including not only
the spikes burst but also the basal activity, could
mitigate the difference of EHG parameters between
preterm and term labor group. On the other hand,
other authors who have also analysed the whole EHG
recording have found statistically significant
differences in the median frequency calculated in
frequency range 0.3-3 Hz (Fele-Zorz, 2008). Firstly,
the target bandwidth of data analysis of our work was
slightly different. Besides, EHG recordings in this
work were performed under common clinical practice
conditions, which implies most of them were carried
on patients under tocolytic drugs effect. This can also
affect the obtained results, but it is closer to real
clinical conditions of patients with threatened of
preterm labor after preliminary explorations in
emergency rooms.
As for BC-EHG signals capability to distinguish
between preterm and term group, it was found
statistically significant difference in both peak to peak
amplitude and DF1 parameters. This result may
suggest that concentric ring electrodes not only can
be used for picking up uterine electrical activity in
patients with threatened preterm labor, but also could
have superior performance for discriminating true
preterm labor from false alarms in comparison to
bipolar recordings with conventional disk electrodes.
This may be associated to a higher spatial resolution
of CRE that permits to discriminate better between
normal local activity during pregnancy and
coordinated global electrical activity as labor
approaches, although this hypothesis has to be
confirmed in further studies with a larger database.
The main limitation of this work is the small size
of the actual database, which on one hand limits the
robustness of the results and the derived conclusions,
and on the other hand binds the study only for patients
with gestational weeks at recording moment between
[28, 34]. When the size of this database is increased,
it will allow us to extend the present analysis to
patients with wider ranges of gestational age [24-36]
WG. It can also be considered a limitation of the
study, the above mentioned use of tocolytic drugs in
most patients. These drugs can modify the spectral
content of EHG signals, since they are intended to
alter uterine contractility in order to delay or prevent
preterm labor. Despite these limitations, CRE have
been proven their capability for monitoring uterine
electrical activity in early gestational ages, suggesting
its potential clinical use for predicting preterm labor.
5 CONCLUSIONS
In conclusion, it has been proved CREs’ capability for
picking up uterine electrical activity during early
weeks of gestation. Moreover, BC-EHG signals
present smaller amplitude but similar spectral
characteristics when compared with conventional
bipolar EHG recordings. Finally, average peak-peak
amplitude and DF1 estimated from BC-EHG
recordings showed statistically difference between
preterm term and term labor group and not from
bipolar EHG, suggesting better performance of the
CRE to disk electrodes for predicting preterm labor
based on EHG records. This prediction capability will
be evaluated in future work since a more
comprehensive database is needed for the
implementation and testing of classifiers.
BIOSIGNALS 2017 - 10th International Conference on Bio-inspired Systems and Signal Processing
82

ACKNOWLEDGEMENTS
This work was supported in part by the Ministry of
Economy and Competitiveness of the Spanish
Government and the European Regional
Development Fund (DPI2015-68397-R,
MINECO/FEDER).
REFERENCES
Alberola-Rubio J., Prats-Boluda G., Ye-Lin Y., Valero J,
Perales A, Garcia-Casado J., 2013. Comparison of non-
invasive electrohysterographic recording techniques for
monitoring uterine dynamics. Medical Engineering &
Physics, 35(12):1736-43.
Alberola-Rubio J., Prats-Boluda G., Ye-Lin Y., Bueno-
Barrachina J.M., Valero J., Desantes D., Perales A.,
Garcia-Casado J., 2015. New clinically friendly EHG
recording system. 37th Annual International
Conference of the IEEE Engineering in Medicine and
Biology.
Beck, Stacy, Wojdyla, Daniel, Say, Lale, Betran, Ana Pilar,
Merialdi, Mario, Requejo, Jennifer Harris, Rubens,
Craig, Menon, Ramkumar, & Look, Paul FA Van.,
2010. The worldwide incidence of preterm birth: a
systematic review of maternal mortality and morbidity.
Bulletin of the World Health Organization, 88(1), 31-
38.
Buhimschi, C., Boyle, M. B., & Garfield, R. E., 1997.
Electrical activity of the human uterus during
pregnancy as recorded from the abdominal surface.
Obstetrics & Gynecology, 90(1), 102-111.
Devedeux D, Marque C, Mansour S, Germain G, Duchêne
J., 1993. Uterine electromyography: a critical review.
Am Journal of Obstetrics and Gynecology,
169(6):1636-53.
Euliano T. Y, Marossero D, Nguyen MT, Euliano N. R,
Principe J, Edwards RK., 2009. Spatiotemporal
electrohysterography patterns in normal and arrested
labor. Am Journal of Obstetrics and Gynecology,
200(1):54.
Euliano, T. Y., Nguyen, M. T., Darmanjian, S., McGorray,
S. P., Euliano, N., Onkala, A., & Gregg, A. R., 2013.
Monitoring uterine activity during labor: a comparison
of 3 methods. American journal of obstetrics and
gynecology, 208(1), 66-e1.
Farina, D., & Cescon, C., 2001. Concentric-ring electrode
systems for noninvasive detection of single motor unit
activity. IEEE transactions on biomedical engineering,
48(11), 1326-1334.
Fele-Žorž, G., Kavšek, G., Novak-Antolič, Ž., & Jager, F.,
2008. A comparison of various linear and non-linear
signal processing techniques to separate uterine EMG
records of term and pre-term delivery groups. Medical
& biological engineering & computing, 46(9), 911-922.
Garfield, R. E., Maner, W. L., MacKay, L. B., Schlembach,
D., & Saade, G. R., 2005. Comparing uterine
electromyography activity of antepartum patients
versus term labor patients. American journal of
obstetrics and gynecology, 193(1), 23-29.
Garfield, R. E, Maner W. L., 2007. Physiology and
Electrical Activity of Uterine Contractions. Seminars in
cell & developmental biology. 18(3), 289-295.
Lucovnik M, Maner W. L, Chambliss LR, Blumrick R,
Balducci J, Novak-Antolic Z, Garfield R. E., 2011.
Noninvasive uterine electromyography for prediction
of preterm delivery. Am Journal of Obstetrics and
Gynecology, 204(3):228.
Maner, W. L., Garfield, R. E., Maul, H., Olson, G., &
Saade, G., 2003. Predicting term and preterm delivery
with transabdominal uterine electromyography.
Obstetrics & Gynecology, 101
(6), 1254-1260.
Maner W. L, Garfield R. E., 2007). Identification of human
term and preterm labor using artificial neural networks
on uterine electromyography data. Ann Biomed Eng
35(3):465–473.
Marque CK, Terrien J., Rihana S., Germain G., 2007.
Preterm labour detection by use of a biophysical
marker: the uterine electrical activity. BMC Pregnancy
and Childbirth. 7(1): S5.
Miles AM, Monga M, Richeson KS., 2001. Correlation of
external and internal monitoring of uterine activity in a
cohort of term patients. American Journal of
Perinatology, 18(3):137-40.
Rabotti C, Mischi M, van Laar JO, Oei GS, Bergmans JW.,
2009. Inter-electrode delay estimators for
electrohysterographic propagation analysis.
Physiological Measurement, 30(8):745-61.
Rabotti C, Mischi M, 2010. Two-dimensional estimation of
the electrohysterographic conduction velocity. Annual
International Conference of the IEEE Engineering in
Medicine and Biology, 4262-5.
Rabotti C, Oei SG, van 't Hooft J, Mischi M, 2011.
Electrohysterographic propagation velocity for preterm
delivery prediction. Am Journal of Obstetrics and
Gynecology, 205(6):9-10.
Schlembach, D., Maner, W. L., Garfield, R. E., & Maul, H.,
2009. Monitoring the progress of pregnancy and labor
using electromyography. European Journal of
Obstetrics & Gynecology and Reproductive Biology,
144, S33-S39.
Ye-Lin, Y., Alberola-Rubio J., Prats-Boluda, G., Perales,
A., Desantes, D., Garcia-Casado, J., 2015. Feasibility
and analysis of bipolar concentric recording of
electrohysterogram with flexible active electrode.
Annals of biomedical engineering, 43(4), 968-976.
Ye-Lin Y., Bueno-Barrachina J.M., Prats-Boluda G.,
Rodriguez de Sanabria R., Garcia-Casado J., 2016,
Wireless sensor node for non-invasive high precision
electrocardiographic signal acquisition based on a
multi-ring electrode, Measurement, Volume 97, 195-
202.
Electrohysterogram Signals from Patients with Threatened Preterm Labor: Concentric Ring Electrode Vs Disk Electrode Recordings
83
