
Acquisition of Confidential Patient Data Over Shared Mobile Device
Petr Vcelak
1,2
, Martin Kryl
2
, Ladislav Racak
2
and Jana Kleckova
1,2
1
NTIS – New Technologies for the Information Society, University of West Bohemia, Univerzitni 8, Plzen, Czech Republic
2
Department of Computer Science and Engineering, University of West Bohemia, Univerzitni 8, Plzen, Czech Republic
Keywords:
Client-server, Data Acquisition, Mobile Application, Patient Data, Security, Shared Mobile Device, Smart-
phones, Tablets.
Abstract:
Mobile devices have already been designed for many applications. Smartphones and tablet computers are
modern, widespread and affordable solutions used for various purposes. Nowadays mobile devices are widely
used in telemedicine. It is usually assumed, that the device is owned and used by a single person. We focus
on security concerns and constraints from a different point of view – when the device is shared. In this paper,
we are proposing a novel approach to prevent leakage of patient’s confidential data when the device is used by
multiple patients at the hospital’s clinic or department. We present a prototype application and discuss its use
case and designed workflow.
1 INTRODUCTION
Our goal is to enable gathering of patient’s data via
shared mobile device. Hospital would lend the con-
figured device to patients and they would be able to
fill out pre-defined medical questionnaires and per-
sonal information forms while waiting for their medi-
cal examination in situation, when medical personnel
is busy examining another patient. Some types of data
can be conveniently collected at this time. The doc-
tor would then pass and verify data, possibly com-
plementing deficiencies. It is not just about gathering
general information like address, contact or health in-
surance situation. Forms could be used to gather more
information about patient’s perceived discomfort dur-
ing the last period. Patient can also provide data for
surveys, data for conducting studies or use mobile
devices to measure additional data such as weight,
blood pressure or pulse through wearable electronics.
At this time, we do not expect the use of additional
equipment like wearable electronics and sensors.
2 STATE OF THE ART
The main target in this paper are mobile phones
such as smartphones and electronic tablets. Nowa-
days mobile phones are used in all healthcare areas
including diagnostics, telemedicine, research, refer-
ence libraries and interventions. (Bastawrous and
Armstrong, 2013) Currently, these devices are easily
available, inexpensive, small, have enough comput-
ing power and provide sufficient space for the devel-
opment of various types of new applications. An ad-
vantage is a user-friendly interface and availability of
installed applications.
Different mobile applications are widely used in
medicine with the aim to provide personalised ap-
proach or just for gathering health data. As Hayes
et al. (2014) said, there were areas where patient-
tailored risk prediction and treatment had been ap-
plied routinely in the clinic over mobile applica-
tions. Nevertheless, authors said, more work would
be required to translate scientific advances into in-
dividualised treatment in other fields. (Hayes et al.,
2014) There were publications regarding that, eg. a
smartphone-centric platform for remote health moni-
toring of health failure (Bisio et al., 2015) or cloud-
based smart health monitoring system for automatic
cardiovascular and fall risk assessment in hyperten-
sive patients (Melillo et al., 2015).
Android is the best selling operation system on
tablets since 2013, and on smartphones it is dominant
by any metric. (Manjoo, 2015) We can cite many arti-
cles and examples describing data acquisition via mo-
bile devices on the Android platform, eg. a portable
physical health monitoring system were proposed in
(Tang et al., 2015) and continuous wireless monitor-
ing of endogenous and exogenous bio-molecules on
an android interface in (Stradolini et al., 2015).
334
Vcelak P., Kryl M., Racak L. and Kleckova J.
Acquisition of Confidential Patient Data Over Shared Mobile Device.
DOI: 10.5220/0006155303340339
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 334-339
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

On the other side, security and privacy issues are
serious topics. Authors Baig et al. discussed mobile
healthcare applications and its critical issues and chal-
lenges. As they said in (Baig et al., 2015), mobile
phones were becoming important in monitoring and
even in delivering of healthcare interventions. Re-
sults of testing mobile health applications on Android
platform was discussed in (Knorr and Aspinall, 2015)
where a number of serious vulnerabilities were dis-
covered in the most popular applications. Dehling et
al. (2015) did an overview of security and privacy
infringements in mobile health applications on An-
droid and iOS. They discovered that the majority of
apps (95.63%, 17,193/17,979; of apps) had posed at
least some potential damage through information se-
curity and privacy infringements. There were 11.67%
(2,098/17,979) of apps that scored the highest assess-
ments of potential damages. (Dehling et al., 2015)
These results lead to belief that private or confidential
information stored in a mobile device/application are
at a risk.
3 SHARED DEVICE APPROACH
3.1 General Information
An obtaining data at own mobile device is an usual
approach. Unfortunately, this may not be a safe way.
Unlike the usual situation where everyone has their
own mobile phone, we start from the opposite as-
sumption. We consider the use of device that is not
owned by the patient. It is only borrowed at a given
moment. We refer to this as a shared device (SD).
The patient has to fill new information or update ex-
isting data (delivered to/from the information system
of the hospital or medical doctor) by the shared de-
vice.
An advantage of the SD approach is the ability to
fully control its system and customise it. We can set
up the environment and install all necessary tools, in-
cluding our own custom applications. Through our
custom application we can provide personalising. It
can be determined in advance what information or
questionnaire needs to be filled by particular patient.
Different type and extent of data might be desired for
different departments, patients, diagnosis or type of
visit.
After the registration at the desk/office/nurse, pa-
tient can get pre-configured shared device, and can
immediately begin checking and filling the form. Op-
tionally, patient may be allowed to switch to other ap-
plications, eg. read news or play some simple games,
while still waiting for examination.
Disadvantages of shared devices are especially the
need to solve the issue of patient’s privacy. Is it really
a disadvantage though? Sensitive or protected data
must not be available to the next patient/personnel us-
ing the device. We have to prevent data leaks when
someone steals the shared device. Of course, data
transfer have to be secured. What about other health
mobile applications? Any kind of health application
has to secure its data as a prevention to data leak, oth-
erwise it leads to security and privacy infringements.
Well, the data privacy have to be solved with any kind
of application that works with patient health infor-
mation. The difference for shared device approach
is, that we are absolutely sure the application will be
used by multiple users, therefore it has to be secured
better.
3.2 Architecture
We have chosen client-server architecture where
client will be responsible for a user interaction. The
business logic will be on the server side only, eg.
form definition and description, form source/input
data and produced output. Client-server communica-
tion is based on REST API with public and private
key-pairs encrypted messages. The HTTPS protocol
is recommended.
3.2.1 Client
Client, as a mobile application, will provide direct in-
teraction with users. User can be a staff member or a
patient itself. We prefer to make client application as
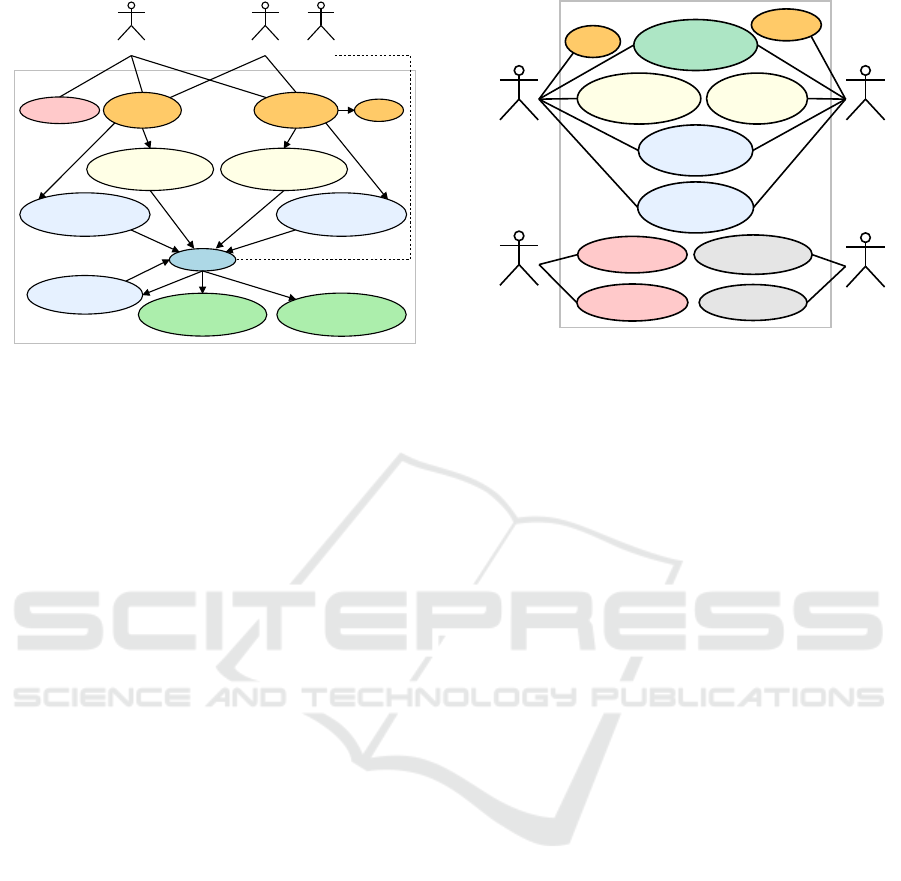
simple as possible. In the figure 1 youcan see use case
diagram. We expect no local configuration stored in
a shared device with the exception of the URL server
address. Security details are described in a separate
section 3.4. Basically, the client application is pre-
pared when URL address of the server is set. The
shared device can operate in two modes:
user have to authenticate by username and password
knowledge,
delegated no user authentication; server sends avail-
able forms and identifies retrieved data by device
ID.
In user mode, there is no list of available users on
SD for a user authentication. Instead an encrypted re-
quest (with username and password) is sent to server
for authentication. After a user is authenticated, forms
(only available to the user) are downloaded , and the
user can choose either to be filled. At the same time
the user can also choose to continue filling up an un-
finished form, that has not been uploaded yet. Client
Acquisition of Confidential Patient Data Over Shared Mobile Device
335
Staff Patient B
Login
(user, pass)
Login
(device ID)
Set server URL Logout
Get list of incomplete
forms (per device)
Form filling
Temporarily store
form data
Send filled form data
to server
Store filled form data
locally in the device
Get list of availaible
forms (per user)
Get list of availaible
forms (per device)
Get list of incomplete
forms (per user)
Patient A
Client
Figure 1: Use case of client.
requests list of available forms for the device directly
when delegated mode is used.
List of available forms is user-dependent and
device-dependent to allow for possible customisation.
This is a quite simple solution for delivering different
forms to the same patient on different clinics.
In the figure 1 you can see use case of delegated
mode by Patient B actor. Shared device is prepared by
Staff (actor) by using Login (device ID) method and
the patient just fills out the form.
The Temporarily store form data use case can re-
solve any distraction (eg. the need to go to the toilet).
Later, a patient can use Get list of incomplete forms
use case (stored per device or per user).
Finally, user can finish completing form by two
methods: (1) send data to the server or (2) store re-
sults data locally in the device. It is preferred to di-
rectly send data to the server. The second method is
a backup solution, eg. when Wi-Fi signal is lost. Lo-
cally stored data is encrypted.
3.2.2 Server
REST API provided by server is the most important
from the perspective of the client. There in the figure
2 you can see all of our actors. A client application
represents both the top use cases, User (logged) and
User (not logged) in the delegated mode. Both ac-
tors can get/download server’s public key S
pub
, list of
available forms and upload/store filled form data. The
form content can be uploaded online over Wi-Fi net-
work or offline by connecting device by a cable.
Server must be properly secured on an operation
system level. All retrieved data from the client appli-
cations will be stored there in an unencrypted form.
For simplicity’s sake, we do not describe details of
server configuration, which may be implementation-
dependent and include all activities related to the ad-
Administrator
User
(logged)
User
(not logger)
Other
System
Login
Logout
Get server’s
public key
Get forms
(per device)
Get forms
(per user)
Store filled
data online
Store filled
data offline
Manage users
Manage forms
Get stored data
Put form data
Server
Figure 2: Use case of server.
ministration of users, forms and a description of their
assignment to users or devices. In this context, Ad-
ministrator and Other System actors use cases are out
of scope of this paper.
3.3 Form Description
There are several ways to describe the form elements,
their labels, groups, description and all the essen-
tials including, eg. validation or enumeration values.
There exist different forms description languages like
XForms 1.1 (2009) and different libraries that helps
building forms. In addition, there are number of dif-
ferences across mobile platforms. We have made our
own way of simplified definition and description of
forms. The same form will need to be viewed and
filled-in on different platforms. Our simplified defini-
tion and description of forms contains:
• form description – ID, name and description
• section – group of form elements has title,
• element – ID, label, data type, validation, default
value, enumeration values,
All text labels may occur multiple times with dif-
ferent language attribute. Supported element data
types are label, text, multi-line text, email, password,
integer, number, currency, phone, boolean check or
switch, date, time, selector box, selector list and URL.
The form definition (description and content) have to
be rendered by client application per mobile platform.
3.4 User Authentication Model
Definition
The most important part of the shared device ap-
proach is communication protocol between client and
HEALTHINF 2017 - 10th International Conference on Health Informatics
336
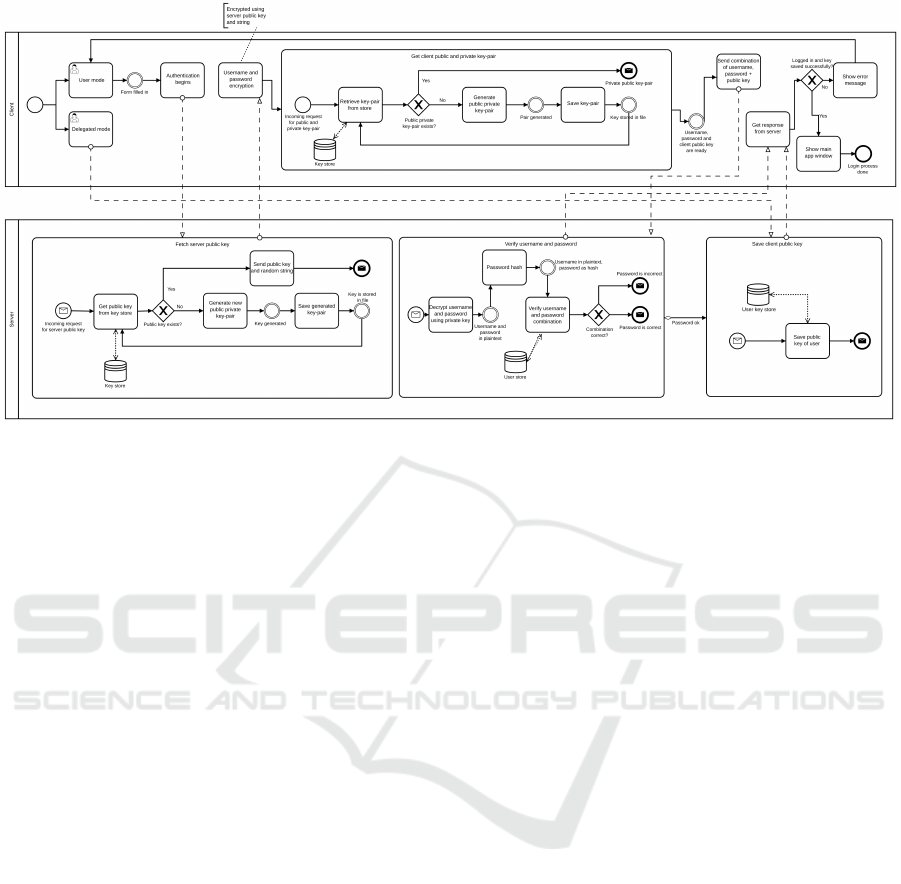
Figure 3: Diagram of the login process – BPMN v2.0 notation.
server. We need to ensure that data in the client appli-
cation is protected against unauthorised access (read)
or modification at the device or during transmission to
the server. For this reason, we describe how user lo-
gin process works on mobile devices. You can see the
login model in the figure 3. Based on the model, en-
cryption is enabled for stored data on client and com-
munications between client and server.
As we mentioned in 3.2.1 and 3.2.2 sections,
client application can login in two ways.
User does not need any username or password
in the delegated mode, unique device ID is used in-
stead. Private and public keys are required on the
device. New key-pair (C
priv
and C
pub
) is generated
and stored in an internal memory of mobile device
when no key-pair exist. Both, device ID D and public
key C
pub
are sent to the server. The client may see
a list of currently-fill forms if the server successfully
processes the request, so device identification and its
public key are stored on a server. If communication
with server fails, the client is informed of the error
message and remains on the login screen.
A user login using username U and password P
method need to have a public key of the server S
pub
.
Client application asks for server’s public key S
pub
.
Server immediately sends an existing key or generates
a new key pair by a configured algorithm. A crypto-
graphic salt (CS) is sent together with the public key
S
pub
. Client stores both in an internal memory. Au-
thentication then follows. Client application encrypts
username U and password P by server’s public key
S
pub
and salt (CS) added. Server receives data and de-
crypts them by its own S
priv
key. Server checks that
the received salt matches the salt sent to the device.
Request is denied if the salt differs or the user does
not exist on the server. A password hash stored on
the server is compared with the one received from the
client. The client’s public key C
pub
is stored in case
of the same password hashes. Client is notified that
the user has logged in successfully and shows list of
possible forms. Otherwise, client is informed of the
error and remains on the login screen.
The salt (CS) is device-dependent. User’s key-pair
(C
priv
, C
pub
) depends on a username U and device ID
D. Each pair of user (as username U) and device ID
D has its own key-pair because of the same key reuse.
4 IMPLEMENTATION AND
RESULTS
As the proof of concept we have created software
corresponding to designed client-server architecture
(3.2) and supporting the user authentication model
(3.4). Server is a service-oriented Java web applica-
tion with REST API and running over HTTPS pro-
tocol. The server needs Java Cryptography Extension
(JCE) Unlimited Strength Jurisdiction Policy Files in-
stalled. We chose the Android platform, the world’s
most popular mobile operating system, for the client
application. The implementation is based on Android
version 7.0 with code name Nougat (API level 24).
The five screenshots are shown on the figure 4.
The client application running on a shared device
does not have any complicated setting, and provides
only a few basic functions. The only configuration
attribute is the server URL address. Mobile applica-
Acquisition of Confidential Patient Data Over Shared Mobile Device
337
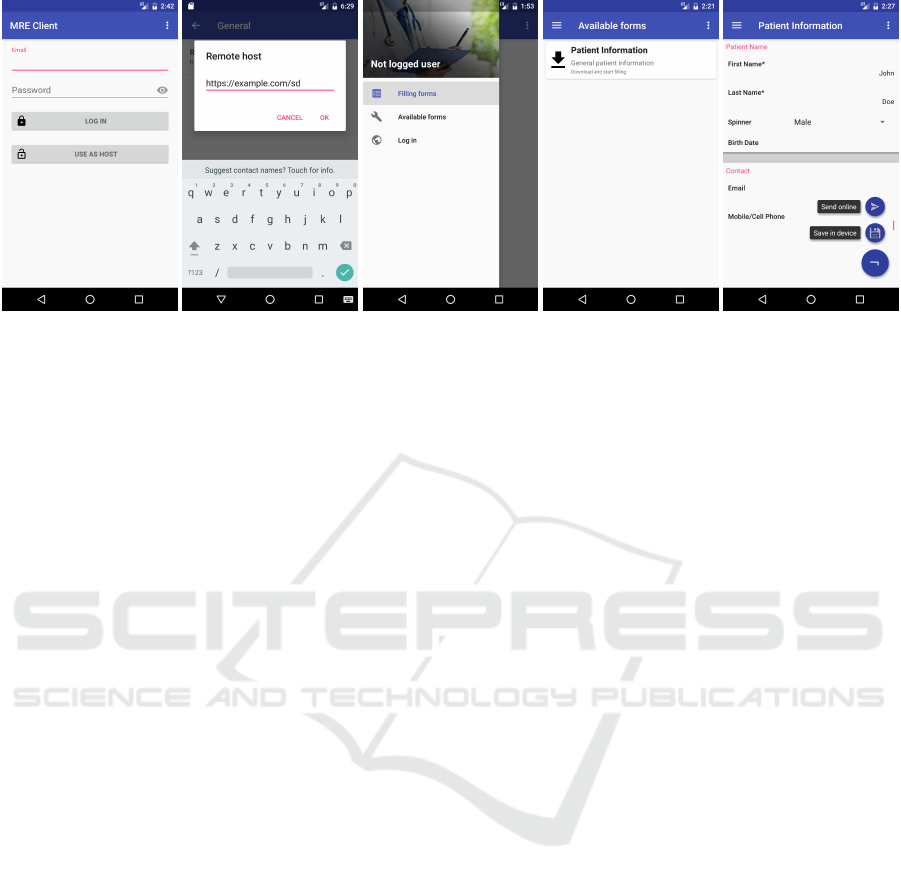
Figure 4: Mobile application (client) screenshots: (1) login screen, (2) configuration – set server URL address, (3) menu of
actions in the delegated mode, user can fill-in per device forms or not finished ones, (4) list of available forms and (5) simple
form/questionnaire generated and menu how to submit a result is shown.
tion has to download corresponding definitions of the
forms that the user can fill in on the shared device.
User cannot directly access data of any hospital infor-
mation systems. Shared device is managed indirectly
by the staff through the server. Staff member can as-
sign a form type to the specific device or patient on the
server. Client application downloads these form defi-
nitions and present an automatically generated forms
to its user.
Retrieved, transmitted and permanently stored
data on the shared device are encrypted. Only the pa-
tient himself can see his own data in a readable way.
Form content is encrypted immediately, when form
is validated and submitted. Online transmission is
the preferred way of data transmission, but encrypted
data can be stored locally when no network access is
available. Data encryption is based on an asymmet-
ric method using private and public key-pairs that are
generated on the server or on the shared device.
5 DISCUSSION
We discuss the results and especially the security of
the proposed shared device approach in this chapter.
The most common and possible attacks include eaves-
dropping or modification of data and identity theft.
Client-server communication is designed to en-
crypt the whole communication, including form def-
initions, because it can contain personal information.
The only unencrypted content is server’s public key,
client’s public key and device ID. An attacker can
get access to communication content on an unsecured
network (eg. public Wi-Fi, HTTP protocol), but it is
not possible to abuse this, because of the way asym-
metric cryptography works (private key is needed for
decryption). Eavesdropping is therefore not possible.
An another attack is by modifying request to ob-
tain data access. It can happen on an unsecured net-
work or when a shared device is infected by malware.
Attacker can spoof the device ID via malware and re-
quest forms available for spoofed ID. Server sends
forms belonging to someone else, however, they are
not accessible, because the private key on attacker’s
device cannot de-crypt them. Attacker would need to
possess private key of the device that is being imitated
by spoofed device ID.
An entire request could be alternated by attacker,
not only the device ID. Server process every request
if its format is valid. Attack would be discovered, be-
cause server attempts to verify the electronic signa-
ture using the sender’s public key. This verification
would fail. Either electronic signature and request
content or public and private key-pair will differ.
We also consider the case of identity theft. At-
tacker can monitor requests and reuse the message to
repeat sending of that request with own fake public
key. This situation is prevented by changing cryp-
tographic salt, which is always used to encrypt user
name and password. Accordingly, the resulting ci-
pher names and passwords vary because of the differ-
ent cryptographic salt.
Our, originally naive, solution of form defini-
tion/description proved to be very flexible. The
form is dynamically generated on the mobile device
(client), according to these definition. It is possi-
ble to dynamically create personalised form definition
on the server which contain patient-oriented data (eg.
different options per age groups or genders).
Mobile devices also have drawbacks. The client
application needs to be online when loading the form
definition. There are also issues with battery life, net-
work availability, breakage or damage of borrowed
device by patients. Network availability is important
HEALTHINF 2017 - 10th International Conference on Health Informatics
338

when submitting form data to the server, but we can
use offline data storage to temporarily alleviate con-
nection problems.
At the testing phase, we identified an issue (oc-
curred only once) with locally stored encrypted form
content. There is a possibility of data loss, when user
logs out of application and logs in again, because key-
pair has to change and server does not store history of
previously used keys. Our approach, originally de-
vised to prevent attacks, may therefore lead to data
loss on this occasion.
The mobile application has fully satisfactory and
fluent response when connected via Wi-Fi. Only
when using large forms (e.g. 1 000 items in select
box) the response time worsened – increased time
needed to download form definition and to render the
form.
6 CONCLUSIONS
In this article we proposed an approach for secure
health data acquisition using shared mobile devices.
The data are confidential in general. The primary
goal was gathering personal data and updating health
status using form-oriented application. The security
problems were discussed. We evaluated risk of data
leak and designed data workflow for mobile devices
that are shared across patients.
We designed a prototype and evaluated it as the
real application on Android device. We identified that
this workflow is properly secured. The discovered
disadvantage is a possible data loss in special case
when data were encrypted and key-pair changed be-
fore data was delivered to the server.
Obtaining data via electronic forms is easily cus-
tomisable and extensible. There is a potential dis-
advantage of impersonal approach. Though, patients
waiting for medical examination are usually feeling
bored, and this interactiveform might be therefore ap-
preciated by them.
In the future we plan to expand the types of data
that can be sent via secure forms and the presented ap-
proach. The logical extension is to support wearable
electronics, sensors and other accessories connectable
with a mobile device that will also acquire more data
types in this way.
ACKNOWLEDGEMENTS
This work was supported by the project PUNTIS (No.
LO1506) of the Ministry of Education, Youth and
Sports of the Czech Republic and by University of
West Bohemia, project Data and Software Engineer-
ing for Advanced Applications (No. SGS-2016-018).
REFERENCES
Baig, M. M., GholamHosseini, H., and Connolly, M. J.
(2015). Mobile healthcare applications: sys-
tem design review, critical issues and challenges.
Australasian Physical & Engineering Sciences in
Medicine, 38(1):23–38.
Bastawrous, A. and Armstrong, M. J. (2013). Mobile health
use in low-and high-income countries: an overview
of the peer-reviewed literature. Journal of the royal
society of medicine, 106(4):130–142.
Bisio, I., Lavagetto, F., Marchese, M., and Sciarrone, A.
(2015). A smartphone-centric platform for remote
health monitoring of heart failure. International Jour-
nal of Communication Systems, 28(11):1753–1771.
Dehling, T., Gao, F., Schneider, S., and Sunyaev, A. (2015).
Exploring the far side of mobile health: information
security and privacy of mobile health apps on ios and
android. JMIR mHealth and uHealth, 3(1):e8.
Hayes, D. F., Markus, H. S., Leslie, R. D., and Topol, E. J.
(2014). Personalized medicine: risk prediction, tar-
geted therapies and mobile health technology. BMC
medicine, 12(1):37.
Knorr, K. and Aspinall, D. (2015). Security testing for
android mhealth apps. In Software Testing, Verifica-
tion and Validation Workshops (ICSTW), 2015 IEEE
Eighth International Conference on, pages 1–8. IEEE.
Manjoo, F. (2015). A murky road ahead for android, despite
market dominance. ISSN 0362-4331. (May 27, 2015)
Retrieved Oct 17, 2016.
Melillo, P., Orrico, A., Scala, P., Crispino, F., and Pecchia,
L. (2015). Cloud-based smart health monitoring sys-
tem for automatic cardiovascular and fall risk assess-
ment in hypertensive patients. Journal of medical sys-
tems, 39(10):1–7.
Stradolini, F., Riario, S., Boero, C., Baj-Rossi, C., Tau-
rino, I., Surrel, G., De Micheli, G., and Carrara, S.
(2015). Wireless monitoring of endogenous and ex-
ogenous biomolecules on an android interface. IEEE
Sensors Journal, 16(9):3163–3170.
Tang, X., Hu, C., and Lin, W. (2015). Android bluetooth
multi-source signal acquisition for multi-parameter
health monitoring devices. In Information and Au-
tomation, 2015 IEEE International Conference on,
pages 1790–1794. IEEE.
Acquisition of Confidential Patient Data Over Shared Mobile Device
339
