
A Kinect-based Monitoring System for Stroke Rehabilitation
Min Hun Lee
1
, Daniel Siewiorek
1
, Asim Smailagic
1
, Alexandre Bernadino
2
and Sergi Bermúdez I Badia
3
1
Carnegie Mellon University, 5000 Forbes Avenue, Pittsburgh, PA, U.S.A.
2
Instituto Superior Técnico, Av. Rovisco Pais, 1, Lisbon, Portugal
3
Madeira Interactive Technology Institute and Faculdade de Ciências Exatas e da Engenharia, Universidade da Madeira,
Caminho da Penteada, 9020-105 Funchal, Portugal
1 OBJECTIVES
Therapists monitor and evaluate stroke patient’s
motor abilities with clinical tests to individualize
clinical interventions. After a clinical session, a
therapist designs task-oriented exercises for a patient
and requests self-reporting of patient’s adherence on
exercise regimen. However, outpatients, who cannot
receive feedback, often show low adherence (Proot
et al., 2005) et al, leading to sparse self-reports. It is
difficult for therapists to follow patient’s progress.
To address this challenge, this paper describes a
Kinect-based monitoring system that evaluates
performance and provides real-time feedback for
four stroke rehabilitation exercises. Our preliminary
study showed that this monitoring system can
accurately monitor in-home stroke rehabilitation
exercises.
2 METHOD
2.1 System Design
We designed a monitoring system for stroke
rehabilitation as shown in Figure 1. Even if a
therapist is not present, this system can perform
monitoring tasks. It provides feedback and guidance
to support achieving therapist’s prescribed exercise
regimen.
During an exercise movement, this monitoring
system tracks body joints in x, y, z coordinates using
a Kinect sensor. Given this time series kinematic
sensor data, it computes physical measurements and
pre-processes coordinates of joint trajectory into
normalized trajectory features. Thus, it reduces the
effect of user’s varying physical characteristics.
This system extracts various features for modelling
performance analysis. Performance analysis involves
three tasks: exercise type recognition, incorrect
movement detection, and performance evaluation.
Exercise type recognizer utilizes normalized
trajectory features and Hidden Markov Models
(HMMs) to recognize which exercise is performed.
After recognizing the type of an exercise,
incorrect movement detectors determine the
correctness of a movement with respect to three
performance metrics: precision, compensation, and
smoothness.
Precision represents the degree of alignment with
the target posture of an exercise. Compensation
calculates the extent of occurring compensatory
movements. Smoothness indicates the degree of
trembling movement patterns. This system models
Decision Trees for the precision and compensation
metrics and HMMs for the smoothness metric.
This system achieves the performance evaluation
by executing a probabilistic reasoning process. It
computes the correctness of three performance
metrics as a performance score.
For user engagement, this system provides
feedback based on performance analysis. Exercise
type recognizer enables to count the repetitions of an
exercise. If any incorrect movement is detected, this
system can correct any detected errors. It motivates a
user with a performance score.
2.2 Dataset
For a preliminary study, we utilize four stroke
rehabilitation exercises (Figure 2). Exercise 1 (E1) is
Figure 1: Overall Flow of Monitoring System for Stroke Rehabilitation.
Lee M., Siewiorek D., Smailagic A., Bernardino A. and BermÞdez I Badia S.
A Kinect-based Monitoring System for Stroke Rehabilitation.
In IcSPORTS 2017 - Extended Abstracts (icSPORTS 2017), pages 8-10
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
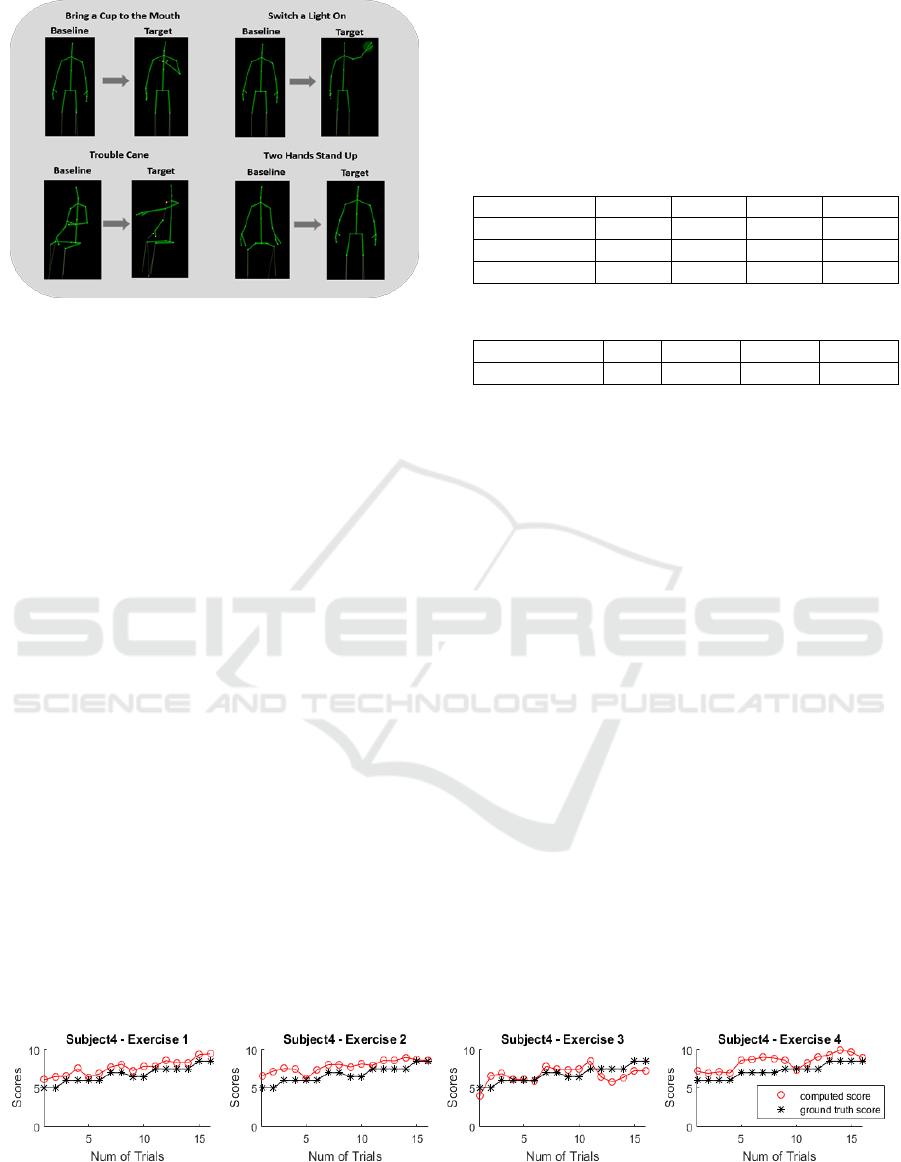
Figure 2: Four Stroke Rehabilitation Exercises.
Bring a Cup to the Mouth, Exercise 2 (E2) is Switch
a Light On, Exercise 3 (E3) is Troubled Cane, and
Exercise 4 (E3) is Two Hands Stand Up.
We collected both “correct” and “incorrect”
datasets of four exercises using a Kinect v2 sensor
(Microsoft, Redmond, USA). It was located at a
height of 0.72m above the floor and 2.5m away from
a subject.
For “correct” dataset, eleven healthy subjects (10
males and 1 female) with the average and standard
deviation age of 32.3 ± 5.81 years participated. Each
subject performed 15 correct repetitions of each
exercise. The “correct” dataset contains 165 sample
movements for each exercise.
For “incorrect” dataset, 5 healthy subjects (4
males and 1 female) with the average and standard
deviation age of 30 ± 3.52 years participated. Each
subject performed the different combinations of
incorrect movements. The “incorrect” dataset
contains 80 sample movements for each exercise.
3 RESULTS
We apply leave-one-subject-out cross validation and
evaluate the monitoring system using “correct” and
“incorrect” datasets. For exercise recognition, we
achieved 96.7% accuracy. Accuracies of incorrect
movement detectors are presented in Table 1. For
the accuracies of performance evaluation, we
calculated the percentage of computed scores within
ground truth scores ± margin in Table 2. Ground
truth scores indicate human observation scores and
margin is selected as 1.
Table 1: Accuracies of Incorrect Movement Detectors.
Metrics
E1
E2
E3
E4
Precision
91.07%
99.69%
94.15%
98.15%
Compensation
94.68%
94.26%
88.16%
95.10%
Smooth
98.00%
97.50%
96.80%
94.25%
Table 2: Accuracies of Performance Evaluation.
E1
E2
E3
E4
Accuracy
95.50%
87.50%
88.75%
91.25%
4 DISCUSSION
According to the preliminary evaluation, this
monitoring system has a potential to accurately
perform three monitoring tasks. This monitoring
system can offer detailed feedback on an exercise
performance without the presence of a therapist.
However, utilized datasets are collected from
healthy subjects, who acted incorrect movements.
Some trials of exercises involve exaggerated
movements, which may be different from post-
stroke survivors. Another limitation of this work is
lack of therapist’s observation scores. It is necessary
to compare ground truth scores from a therapist with
computed scores of this monitoring system. In
future, we plan to validate this monitoring system
using datasets from stroke survivors and therapist’s
observation scores.
ACKNOWLEDGEMENTS
This work was supported by the FCT through the
Augmented Human Assistance project (CMUP-
ERI/HCI/0046/2013) and SFRH/BD/113694/2015.
Figure 3: Plots of Computed Scores and Human Observation Scores.

REFERENCES
Proot, Ireen M., et al. "Stroke patients’ needs and
experiences regarding autonomy at discharge from
nursing home." Patient education and counseling 41.3
(2000): 275-283.
