
Health Behavior Models in Utilizing Water Resources to Tidal
Waters Community
Vieronica Varbi Sununianti, Tri Agus Susanto and Diana Dewi Sartika
Sociology Major, Faculty of Social and Political Science, Sriwijaya University, South Sumatera, Indonesia
vieronicavarbis@unsri.ac.id
Keywords: Health Behavior, Tidal Water Community.
Abstract: Water is a basic need of all living things, including human. However, living in tidal areas with large bodies
of water does not necessarily mean a society can fulfill their need for water. This happened in Maura
Padang sub-district, Indonesia. A large number of areas are peat bogs and deltas of the Musi river. The
water sources are acidic, smelly, sticky, and unfit for consumption. This attracted researcher to analyze
public health behavior based on water resource utilization in daily needs. It is descriptive qualitative
research through interviews, FGD, observations, and study documents. Researchers interviewed migrants,
natives, medical workers, communities, and religious leaders. The results found that migrant communities
can survive in this area. Nevertheless, part of them return to their hometown since they’re unable to adapt to
the physical environment. Government programs contribute artificial water reservoirs for families and
communities. Due to limitations of water resources, they use rainwater for household consumption and
ground water (river, well, and ditch water) to flush their yard, wash their food and clothes, and bathe.
Socioeconomic status and environment impact health behavior, including such treatment. This paper is
beneficial for residents in tidal areas, the Banyuasin District health office and the University in providing
socialization, promoting health living and help the fulfillment of clean water.
1 INTRODUCTION
A number of studies discuss the manifestation of
health behavior. The elements that form the
difference in social health behavior is a culture (Fox
and Alldred, 2016; Singer, 2016). According to Fox,
the nature and culture of human beings are a part of
the environment and health. The environment also
affects the interface between human and
environment. It constructs innovative healthcare
(Saidi, 2017) with emphasis on social practices,
structure, and material. Next, health behavior is also
related to lifestyles (Romano and Scott, 2014; Bure,
2016). The arrangement of health education and the
height of the intervention towards a healthier
lifestyle (Romano and Scott, 2014). Individual
lifestyle choices affect physical and emotional
health. (Bure, 2016). Furthermore, study of oral
health behavior using the Health Belief Models
(HBM) (Zetu, 2014) identified there is no significant
difference between genders. However, women are
known to have more perceived severity and self-
efficacy, but have lower perceived barriers. All of
these studies dicussed health behavior on social
aspects of the environment, culture, and lifestyle, but
paid less attention on adaptation and behavior
changes to survive. We deliver this gap by
explaining the tidal society behavior in utilizing
water resources to meet the daily needs.
Water is a basic need and a source of life. It is
useful to support all living beings, especially human.
Unfortunately, water supplies are unable to meet
increasing demand for water. The millennium
development goals (MDGs) 2010 report exposed the
percentage of sustainable access to drinking water in
urban areas is 49,82%, and in rural areas is 45,72%.
It has been predicted that there could be a global
water scarcity. (Shiva, 2002). Even though Indonesia
is an archipelago country, nevertheless it still faces
obstacles in providing clean water. What is unique in
Banyuasin district, is that a large part of the area is
comprised of inconsumable water. Together with the
increase of the development of tidal community’s
health behavior changes in the use of water
resources to meet their daily lives.
Sununianti, V., Susanto, T. and Sartika, D.
Health Behavior Models in Utilizing Water Resources to Tidal Waters Community.
In Proceedings of the 2nd International Conference on Sociology Education (ICSE 2017) - Volume 1, pages 277-280
ISBN: 978-989-758-316-2
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
277

2 CONCEPT
The World Health Organization (WHO) explains
health as a condition that covers one’s state in
complete physical, mental, and social well-being. It
is not only the limited absence of disease or
lethargy. In Indonesia, health legislation number 36
of 2009 states that health covers various health
conditions, such as physical, mental, spiritual, and
social conditions, which allows every person to have
a productive social and economic life.
In medical concepts, a disease is an abnormal
body condition that can be detected by certain
symptoms. But in social science, diseases are bio-
physiology symptoms that affect the human body.
Illness is a social symptom that accompanies disease
to the point where it disturbs feelings of health. In
this case, disease is related with a subjective
meaning.
According to Marshall Becker, health behavior
has three variations, which are healthy life behavior,
illness behavior, and sick role behavior
(Notoadmodjo, 2003; Weitz, 2007). Healthy life
behavior is the effort by someone to maintain and
improve their health. Illness behavior is a someone’s
response towards illness, disease perception, causes
and symptom knowledge, treatment, etc. Meanwhile,
sick role behavior is related to the rights and
obligations of sick individuals which are known by
themselves and by others. According to sociologist
Talcott Parsons, roles and social functions are
interconnected. Consequently, someone is
considered healthy if they have the maximum
capacity to do roles and tasks which are learned
through the process of socialization (Sunarto, 2002).
Thus, sociology’s understanding of health is relative,
and is based on the social role of society.
3 METHODS
This paper is constructed on descriptive qualitative
research (Denzin, 1994; Creswell, 2003; Neuman,
2007) in Maura Padang sub-district, Banyuasin
district, South Sumatera province, Indonesia
(Susanto et al., 2016). This location had been
selected due to their lack of clean water despite their
abundant water resources.
Research sources are sourced from primary and
secondary data. The primary data used unstructured
guidelines when conducting interviews and focus
group discussion (FGD) in five villages. The social
categories are migrants, natives, medical workers,
village officials, religious and community leaders
who have lived at least for five years and have a
family. Analysis was conducted from collecting,
coding, and connecting between data and concepts.
Data validation was conducted internally and
externally.
4 ANALYSIS AND DISCUSSION
Maura Padang sub-district is spread over a wide
area, around 944,60Km
2
in total. Overall, their area
consists of low land, marshes, and peats. The
marshes found are categorized as brackish water. It
is a result of the meeting between fresh water from
the Musi River and salt water from the Bangka sea.
Tidal wave soaks almost all of the marshes. This
result is tidal groundwater is usually salty, acidic,
and brackish, and the color of the water ranges from
brownish to black. This water condition near inland
or low land depends on tidal water from the sea.
This natural water becomes very poor and unfeasible
for consumption. The tropic areas have the most
precipitation in December until January. Meanwhile,
rainfall also affects the quality of ground water.
Generally, the groundwater will be taste saltier than
usual in the dry season. This area also faces tides
which causes the land to be drowned in water from
the tides. This tide also had an impact on
transportation. In the morning, the tides are high,
which means speed boat becomes the popular choice
for transportation. However, ever since road
infrastructure was build in 2000, the resident’s
mobility no longer depends on the tide.
The transmigration program in this area was
implemented by the Indonesian New Order
Government in the 1980s. Most of the inhabitants in
this sub-district originated from Java. These
migrants occupy 12 villages, while native
inhabitants from Palembang occupy a mere three
river-side villages. Migrants make a living by
becoming tidal farmers, while natives usually
become fisherman and freelance plantation workers.
Unlike migrant inhabitant, natives build their houses
on stilt structures, which also influences the culture
and the communal patterns of utilizing water
resources and fulfilling their daily needs.
In the beginning, migrant communities gained
their knowledge about rainwater utilization from the
government. They collected rainwater and used it
carefully. This happened due to the significant
difference topographical areas between Java and
Sumatera. In Sumatera, especially in the Banyuasin
district, ground water is usually impossible to
ICSE 2017 - 2nd International Conference on Sociology Education
278
consume. Meanwhile, rain water supply exists in
limited quantities. The effect of these geographical
situation is that many migrants that failed to adapt to
the environment moved back to their hometowns.
The limited supply of fresh water has been the
center of attention for many stakeholders. For the
first time, the nation’s government gave each family
an artificial water resevoirs. Furthermore, the local
government built water deposits with artificial water
reservoirs for the whole community to access in the
central village and drilled a well in order to access
ground water. Some universities also contributed by
making ground water filters. However, this effort
has yet to be successful.
The community also has local traditions that they
follow in the pursuit of fresh water. They try to find
fresh water by looking for it as far as the deep end of
ricefields, where rain water puddles form. They also
try to make reservoirs for both river water and well
water by using chlorine. They even use religious and
cultural ritual to find water such as fasting, praying
at outdoor villages, and putting many of their fruit
and food near the river in the central villages.
Cultural values and societal norms protect the rivers
and ditch from becoming garbage dumpsters.
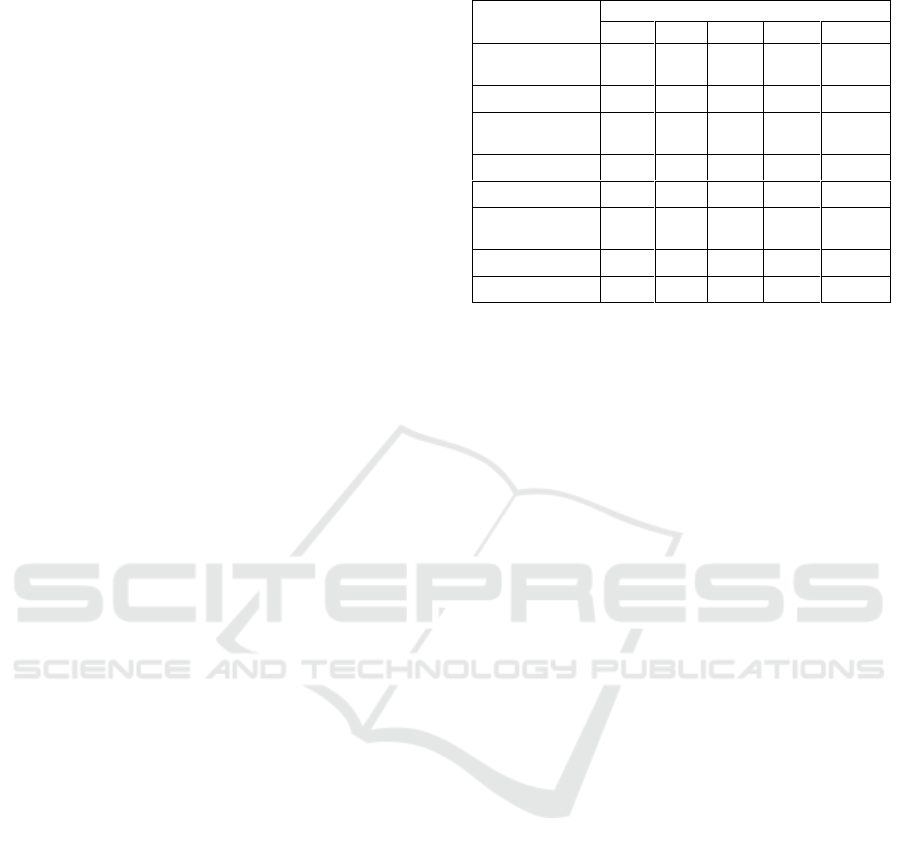
We’ve constructed that they’ve divided the water
functions in order to meet their daily necessities
(Table 1.). The water difference function influences
health behavior in the communities living in the tidal
areas. The behavior patterns aim to maintain and
improve the health conditions of the individual and
their family.
Health behaviour socialization is carried out by
health workers, government, or private institutions.
One of the socialization methods conducted by
government is the promotion of a clean and healthy
lifestyle (“Perilaku Hidup Bersih dan Sehat”). In
fact, many people, especially native residents, still
bathe, wash, and defecate in the river water. As a
result, water-related diseases are often suffered this
community, such as diarrhea, dengue fever, typhus,
vomiting, coughs, lung diseases, and respiratory
diseases. Other diseases are sweet pea, uric acid, and
high blood pressure which are caused by dietary
habits and lifestyle choices. Based on past
experience, some of the residents feel sore when
they consume too much rain water, however there is
still a gap among individual manner in symptoms
that appear in response to diseases.
Table 1: Sources and function water in tidal community.
Water
function
Water sources
rain
well
river
ditch
gallon
Cooking and
consumption
√
-
-
-
√
Washing food
√
√
-
-
-
Washing
clothes
-
√
√
√
-
Bathing
√
√
-
√
-
Flushing yard
-
√
√
√
-
Worship
(‘Wuhu’)
√
√
√
-
Transportation
-
-
-
√
-
Health service
√
-
-
√
-
Source: (Sununianti, 2015)
The variance of knowledge and experience affect
the community’s efforts to deal with disease.
Different disease management methods are also
based on social and economic status. If children are
ailed with illness, seeking treatment is usually a high
priority for parents, compared to when adults are
ailed with similar illnesses. When adults are ailed
with illness, they will only look for treatment if they
can no longer fulfill their societal role, such as
working. The treatment provided by health services
also differ between lower and upper class
communities. Upper class communities usually have
direct access to health services when they are
diagnosed with symptoms of diseases. Lower and
middle class communities that are ailed with illness
usually postpone their search for health services
until their illness reaches a critical condition. Part of
the lower class communities still use “dukun” or
traditional medicine to cure their diseases before
they attempt to go to Public Health Services
(“Puskesmas”), clinics, or hospitals.
Efforts to achieve health have been conducted
through a variety of strategies. Researchers found a
combination of health behavioral model that
emerged in Maura Padang’s tidal community that
was in line with Health Belief Models (HBM)
(Weitz, 2007; Sudarma, 2008; Solhi, 2010; White,
2012; Romano and Scott, 2014). It is based on
experiences, culture, and social structures with the
environment of the residents having an influence on
individual and societal health behaviour.
Communities residing in tidal areas were perceived
to be in a susceptible and severe situation. They face
many difficulties in accessing fresh water and are
susceptible to a wide array of water related diseases.
These communities must get treatment of diseases
caused by ground water, due to the unfeasible
consumption, dire health conditions, and the need
Health Behavior Models in Utilizing Water Resources to Tidal Waters Community
279

for medical assistance. They have felt direcly the
benefits and barriers of shifting from ground water
to rain water. Health behavior changes are through
the form of using rain and gallon water for washing
and consumption, a practice that has been utilized by
many parts of the community except the lower class
society. They also require regular maintainince to
keep, close, and clean reservoir rainwater.
Furthermore, there is an extra expense that needs to
paid for chemical treatment to prevent mosquito
larvae, and for using gallons and packaged water,
which is relatively expensive. In this case, health
behavior towards illness treatment differs from
social status, economic situation, and societal
culture. Meanwhile, sick role behavior is still
relatively dependant on an individual’s role in
society.
Tidal communities have their own medical
system. This medical system includes faith healing
and efforts to improve general health. The health
behavior in this study is formed due to societal
culture and beliefs on susceptibility to illness,
malignant diseases, and general societal costs.
Geographical conditions affect the behavior of the
tidal community in preventing and healing of
disease, as well as in improving their health.
5 CONCLUSIONS
This paper discusses the limited access to clean
water in areas with abundant water resources.
Communities in this areas use different strategies to
fulfill their daily need of water. The obstacles they
face in accessing various water sources will
influence the health behaviour of the community as
a whole. The point is that individual and familial
health behaviors in tidal communities are related to
environmental, social, economic, and cultural
conditions.
ACKNOWLEDGEMENTS
The authors are grateful to anonymous reviewers
that spent their time providing constructive input to
improve this article. The authors also appreciate all
the informants who contributed to this paper. We’d
also like to extend our gratitude to the Ministry of
Research and Technology, Directorate of Higher
Education, Indonesia, and Sriwijaya University, that
funded this fundamental research. We hope this
research will be useful for others in the future.
REFERENCES
Bure, I., 2016. Health-Related Behaviour of Czech
Adolescents. Procedia - Social and Behavioral
Sciences. Elsevier B.V., 217, pp. 1146–1152.
Creswell, J. W., 2003. Research Design Qualitative,
Quantitative, and Mixed Methods Approaches, Sage
Publications. London and New Delhi,
2nd
edition.
Denzin, N. K., 1994. Handbook of Qualitative Research,
Sage Publications. London.
Fox, N. J., Alldred, P., 2016. Sociology, environment and
health: a materialist approach. Public Health. 141, pp.
287–293.
Neuman, W. L., 2007. Basic of Social Research:
Qualitative and Quantitative Approaches, Pearson
Education.
2nd
edition.
Notoadmodjo, S., 2003. Pendidikan dan Perilaku
Kesehatan, Rineka Cipta. Jakarta.
Romano, V., Scott, I., 2014. Using Health Belief Model to
Reduce Obesity Amongst African American and
Hispanic Populations. Procedia - Social and
Behavioral Sciences. Elsevier B.V., 159, pp. 707–711.
Saidi, T., 2017. The Sociology of Space as a Catalyst for
Innovation in the Health Sector. Social Science &
Medicine. Elsevier Ltd. (Social Science and
Medicine), p. 40.
Shiva, V., 2002. Water Wars: Privatisasi, Profit dan
Polusi, Insist Press. Yogyakarta.
Singer, M. K., 2016. Social Science & Medicine Culture:
The missing link in health research. pp. 1–10.
Solhi, M., 2010. The Application of the Health Belief
Model in Oral Health Education. Iranian Journal
Public Health. 39(4), pp. 114–119.
Sudarma, M., 2008. Sosiologi Kesehatan, Salemba
Medika. Jakarta.
Sunarto, K., 2002. Sosiologi Kesehatan, Universitas
Terbuka. Jakarta.
Sununianti, V. V., 2015. Ancaman Privatisasi Air bagi
Masyarakat Pasang Surut. Majalah Sriwijaya. XX No.
12(Sosial Humaniora), pp. 36–47.
Susanto, T. A., Sununianti, V. V., Sartika, D. D., 2016.
Kearifan Lokal Masyarakat Perairan dalam
Memanfaatkan Sumber Daya Air Untuk Kebutuhan
Sehari-hari (Studi di Daerah Perairan Pasang Surut
Kecamatan Muara Padang, Kabupaten Banyuasin,
Sumatera Selatan) (Tahun Kedua), Inderalaya.
Weitz, R., 2007. The Sociology of Health , Illness , and
Health Care: A Critical Approach, Thomson
Wadsworth. USA.
White, K., 2012. Pengantar Sosiologi Kesehatan dan
Penyakit, Raja Grafindo Persada. Jakarta,
3rd
edition.
Zetu, L., 2014. Gender variations in the psychological
factors as defined by the extended health belief model
of oral hygiene behaviors, 127, pp. 358–362.
ICSE 2017 - 2nd International Conference on Sociology Education
280
