
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and
Wearable Sensor for Tele Knee Rehabilitation after Knee Operation
MReza Naeemabadi
1,*
, Birthe Dinesen
1
, Ole Kæseler Andersen
2
, Samira Najafi
3
and John Hansen
4,5
1
Laboratory of Welfare Technologies - Telehealth and Telerehabilitation, Integrative Neuroscience Research Group,
SMI®, Department of Health Science and Technology, Faculty of Medicine, Aalborg University, Denmark
2
Integrative Neuroscience Research Group, SMI®, Department of Health Science and Technology,
Faculty of Medicine, Aalborg University, Denmark
3
Clinical Engineering Department, Vice-Chancellor in Treatment Affairs, Mashhad University of Medical Science, Iran
4
Laboratory for Cardio-Technology, Medical Informatics Group, Department of Health Science and Technology,
Faculty of Medicine, Aalborg University, Denmark
5
Laboratory of Welfare Technologies - Telehealth and Telerehabilitation, SMI®, Department of Health Science
and Technology, Faculty of Medicine, Aalborg University, Denmark
Keywords: Microsoft Kinect, IMU, Accelerometer, Inertial Measure Units, Knee Angle, Knee Rehabilitation, Wearable
Sensors.
Abstract: The Microsoft Kinect sensors and wearable sensors are considered as low-cost portable alternative of
advanced marker-based motion capture systems for tracking human physical activities. These sensors are
widely utilized in several clinical applications. Many studies were conducted to evaluate accuracy, reliability,
and usability of the Microsoft Kinect sensors for tracking in static body postures, gait and other daily activities.
This study was aimed to asses and compare accuracy and usability of both generation of the Microsoft Kinect
sensors and wearable sensors for tracking daily knee rehabilitation exercises. Hence, several common
exercises for knee rehabilitation were utilized. Knee angle was estimated as an outcome. The results indicated
only second generation of Microsoft Kinect sensors and wearable sensors had acceptable accuracy, where
average root mean square error for Microsoft Kinect v2, accelerometers and inertial measure units were 2.09°,
3.11°, and 4.93° respectively. Both generation of Microsoft Kinect sensors were unsuccessful to track joint
position while the subject was lying in a bed. This limitation may argue usability of Microsoft Kinect sensors
for knee rehabilitation applications.
1 INTRODUCTION
Telerehabilitation after knee surgery is recognized as
one of the well-known type of telemedicine.
Nowadays, this service is wildly provided in the
world. Previous studies remarked low-bandwidth
Audio/Video communication improved rehabilitation
program after total knee replacement remotely
(Tousignant et al., 2009; Russell et al., 2011;
Tousignant et al., 2011).
Motion capture systems are utilized to evaluated
improvements in patients’ physical activity
performance beside the subjective rehabilitation test.
However; marker-based motion capture systems are
highly precise and known as a gold standard, they
have several limitations. First, the motion capture
systems are considerably expensive. Moreover, data
acquisition process due to attaching several markers
on the subject’s body and calibration process is
relatively complex. Finally, the marker-based motion
capture systems are not portable, and large space is
required.
Consequently, the marker-based motion capture
systems are not considered as a proper candidate for
tracking human activities during daily rehabilitation
sessions.
Wearable sensors and Microsoft Kinect sensors
are the most common systems are being employed as
low-cost, portable and less complex alternative for
human motion tracking system.
Several studies utilized Microsoft Kinect sensors
as marker-less physical activity tracker for physical
rehabilitation program (Pedraza-Hueso et al., 2015;
128
Naeemabadi, M., Dinesen, B., Andersen, O., Najafi, S. and Hansen, J.
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation.
DOI: 10.5220/0006578201280135
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018) - Volume 1: BIODEVICES, pages 128-135
ISBN: 978-989-758-277-6
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Vernadakis et al., 2014; Lange et al., 2012; Pavão et
al., 2014).
While wearable sensors were also employed as a
human motion capture system for tracking patient’s
performance during telerehabilitation program
(Piqueras et al., 2013; Tseng et al., 2009).
In 2012 Microsoft introduced a RGB-Depth
camera as a part of Microsoft Xbox 360 called
Microsoft Kinect Xbox 360 (or Kinect v1) (Schröder
et al. 2011). Microsoft Kinect SDK v1.8 using the
depth images and embedded skeleton algorithm
provides the geometric positions of 20 joints of each
detected body in the space (Microsoft 2013).
The second generation of Microsoft Kinect was
presented together with Microsoft Xbox One and
known as Microsoft Kinect One (or Kinect v2).
Several improvement in the sensors have been
applied in the Kinect v2 (Sell and O’Connor, 2014).
Microsoft Kinect SDK 2.0 was developed for Kinect
v2 and enables developer to record estimated position
of 25 joints for each detected skeleton (Microsoft,
2014).
Consequently, several studies were conducted to
assess accuracy and reliability of Microsoft Kinect
sensors for static postures(Xu and McGorry, 2015;
Darby et al., 2016; Clark et al., 2012), gait (Mentiplay
et al., 2015; Auvinet et al., 2017; Eltoukhy et al.
2017), body sway (Yeung et al., 2014), and joints
angles in specific physical activities(Anton et al.,
2016; Woolford, 2015; Huber et al., 2015) using gold
standard marker-based motion capture systems.
Wearable sensors such as accelerometers,
gyroscopes and inertial measure units (IMU) are also
being used to track physical activities. Boa et al. used
five biaxial accelerometers to classify 20 activities
with 84% accuracy (Bao and Intille, 2004) while
Karantonis et al., (2006) classified 12 physical tasks
using a tri-axial accelerometer with 90.8% accuracy.
Joints and limb orientation can be estimated by using
accelerometer and gyroscope sensors (Hyde et al.,
2008; Roetenberg et al., 2013) but it still has one
degree of ambiguity in the 3-dimension space.
Accuracy of human body orientation was improved
by using IMU sensors (Ahmed and Tahir, 2017; Lin
and Kulic
́
, 2012).
In this paper, accuracy and usability of both
generation of Microsoft Kinect sensors (Kinect v1
and Kinect v2), IMUs and accelerometer sensors for
seven common exercises in knee rehabilitation
program were investigated by using a gold standard
marker-based motion capture system. The main aim
of this study was to evaluate Microsoft Kinect sensors
and wearable sensors for knee rehabilitation
application.
2 METHODS
2.1 Data Collection
In this study, seven series of recording were
performed to assess accuracy and usability of
mentioned human activity tracking systems
simultaneously while subject doing common
rehabilitation exercises for knee. Eight Qualisys Oqus
300/310 cameras were pointed to the area of interest.
The recordings were carried out using Qualisys Track
Manager 2.14 (build 3180) with 256Hz sampling
frequency. Pelvis markers were placed on the Ilium
Anterior Superior and Ilium Posterior Superior. Knee
joint defined by Femur Medial Epicondyle and Femur
Lateral Epicondyle markers, while Fibula Apex of
Lateral Malleolus and Tibia Apex of Medial
Malleolus landmarks were used for defining ankle
joint. Consequently, TH1-4, SK1-4, FCC, FM1 and
FM5 landmarks were employed to track lower limbs
movement (van Sint Jan, 2007).
Kinematics and kinetics measurement of lower
extremities were worked out using Visual 3D v6
software based on the Qualisys recordings (C-
Motion, 2017).
A pair of Kinect v1 and Kinect 2 were also
utilized to record joint positions. Two custom
applications were developed to capture, and store
estimated skeleton and corresponding joint positions.
Microsoft Kinect SDK version 1.8 and version 2.0
were utilized in the software development. A server
application was also developed to establish global
timing between applications using transmission
control protocol/Internet protocol through the local
network. Sampling frequencies were adjusted at
30Hz, which is highest available rate.
Linear acceleration, angular velocity, and
magnetic field were acquired using embedded
accelerometer, gyroscope and magnetometer sensors
in Shimmer 3 (Shimmer Sensing, 2016). Shimmer
wearable sensors were fixed on thigh, shin and foot
and the data including timestamps were streamed to
the computer using Bluetooth in real-time. Sampling
frequency for sensor were set at 128Hz. Acceleration,
angular velocity, and magnetics field recording range
were set at ±2g, ±500dps, ±1.3Ga respectively.
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation
129
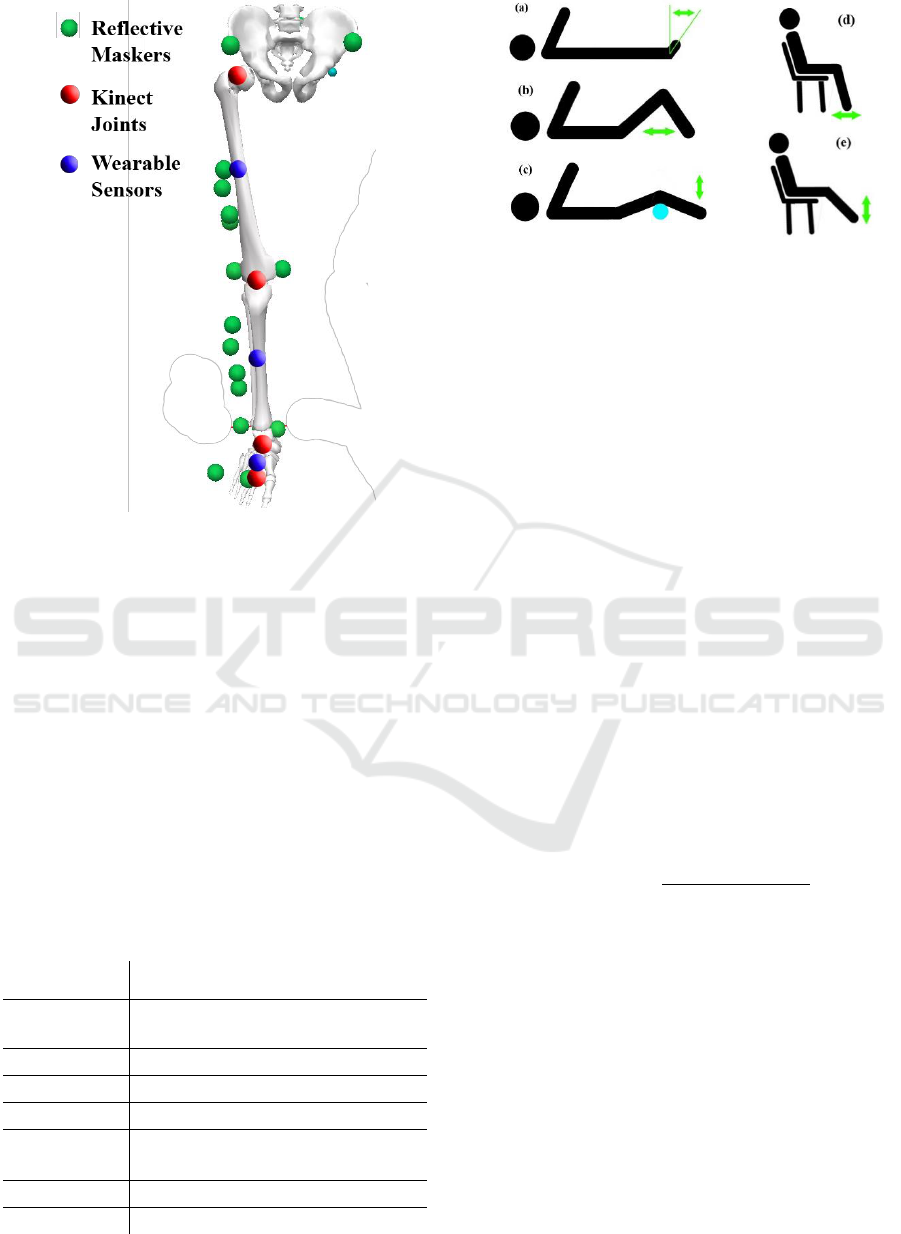
Figure 1: Positions of reflective markers, Microsoft Kinect
virtual landmarks and placement of wearable sensors.
Green circles show position of reflective markers and red
circles show position of estimated joint. Wearable sensors
were fixed at blue circles.
2.2 Procedure
Seven common exercises for knee rehabilitation were
performed during the recordings. These exercises are
mainly involving knee flexion and extension. Table 1
describes each exercise and Figure 2 shows the
exercise visually.
In the first three exercises both Kinect sensors
were mounted on the ceilings while for the rest of
exercises Kinect sensors were place on the table with
1m height. The Z-plane of Kinect sensors was
Table 1: Exercise details.
Posture
Physical Activity
Exercise 1
Laying
Ankle Dorsi/Plantar
flexion
Exercise 2
Laying
Knee flexion/extension
Exercise 3
Laying
Knee flexion/extension
Exercise 4
Sitting
Biking
Exercise 5
Sitting/
Standing
Sit to Stand
Exercise 6
Sitting
Leg bend and stretch
Exercise 7
Sitting
Knee flexion/extension
Figure 2: Visual explanation of exercises including posture
and movement. The green arrow shows direction of
movement. (a) exercise 1, (b) exercise 2, (c) exercise 3, (d)
exercise 6, (e) exercise 7.
perpendicular to coronal plane in all exercises except
exercise four and five (which in these two exercises
the Z-plane of Kinect sensors was perpendicular to
median plane). Figure 3 shows position and
alignment of Kinect sensors corresponding to the
subject’s body.
2.3 Data Analysis
The recorded data were filtered using a 10Hz low pass
filter implemented using a 20
th
order IIR Butterworth
filter. Data were synchronized in two steps. First data
were synchronized using recorded timestamp. In the
second step, small delays due to the data transferring
and processing latency were removed by using
dynamic time warping.
The knee joint in Kinect skeleton data was define
by virtual thigh, shin, and foot bones using position
of hip, knee, ankle, and foot joints position. Equation
1 represents calculated knee angle (
using
virtual bones.
(1)
Similarly, knee angle was calculated based on
acceleration data by using the acceleration vectors of
sensors on the thigh, shin and foot.
The knee angle in the gold standard recorded was
estimated in Visual 3D software by referencing thigh
and shank modelled bones respectively.
Orientation of IMU sensors were calculated using
attitude and heading reference system transformation
algorithm by fusing triaxial acceleration, triaxial
angular velocity, and triaxial magnetic field recording
(Kalkbrenner et al., 2014; Madgwick et al., 2011).
Consequently, orientation of each sensor was
represented by quaternions. Using shin and thigh
BIODEVICES 2018 - 11th International Conference on Biomedical Electronics and Devices
130
quaternions, the knee angle was calculated based on
equation 2.
(2)
2.4 Statistical Analyses
The range of motion (ROM) for all recordings were
calculated based on estimated knee angle. Root-
mean-square error (RMSE) and Pearson correlation
coefficient (R) were calculated. Coefficient of
variation between two systems was also calculated as
a ratio of error to mean comparing the gold standard.
95% limits of agreement (LOA) and bias (B) were
analysed using Bland-Altman analysis.
3 RESULTS
The results showed Microsoft Kinect SDKs (SDK 1.8
and SDK 2.0) were not able to detect body skeleton
and estimated joint positions for those exercises
subject laid in the bed (exercise 1-3). However,
Kinect sensors were place perpendicular to subject’s
coronal plane.
The results indicated the estimated knee angle
using accelerometer presents less RMSE. Mean
RMSE were 2.085° and 3.107° respectively in accele-
rometers and IMUs recordings, while the mean values
for Kinect v1 and Kinect v2 were 13.408° and 4.930°.
The estimated knee angle using IMU sensors
introduced lower RMSE than the provided knee angle
with Kinect v2 except exercise 4 (biking).
According to the table 2, estimated knee angle
was highly correlated with actual knee angle
(correlation > 0.796).
Moreover, the results show accelerometer sensors
represented higher accuracy in estimating lower
boundaries of range of motion in comparison to
IMUs. Whereas, Kinect sensors introduced higher
difference with actual knee angle during biking
exercise (see figure 4).
Bland Altman estimations indicated estimated
angle with accelerometer and IMU had higher
agreement with calculated values using gold standard
comparing with Microsoft Kinect sensor.
4 DISCUSSION
This study evaluated accuracy and usability of
wearable sensors (accelerometers and IMUs) and
Microsoft Kinect sensors (Microsoft Kinect v1 and
Microsoft Kinect v2) as a daily tracking system for
knee rehabilitation applications. Hence, the most
common exercises for knee rehabilitation were
utilized and tracking knee angle and range of motion
in interested knee were emphasized.
Qualisys marker-based motion capture system
was utilized as a gold standard system for tracking
lower limbs activities and C-Motion Visual 3D was
employed to compute joints angle.
Microsoft Kinect v1 introduced lower accuracy in
all the results (more than 10 degrees in average).
While the other recording systems presented
comparable accuracy. The trials showed the wearable
sensors and Microsoft Kinect v2 had acceptable
performance for tracking knee angle during exercises
with higher and more complex physical activities like
biking.
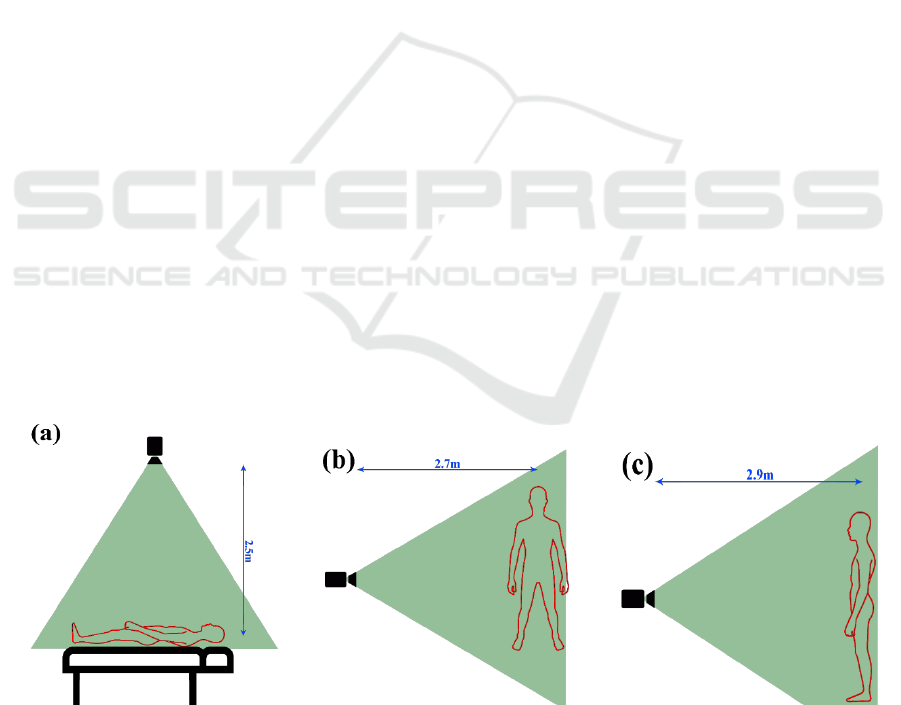
Figure 3: Position and alignment of Kinect sensors corresponding to the subject's body. (a) The subject was lying in a bed for
exercise 1-3 and the Kinect sensors were mounted on the ceiling and facing the floor. (b) In the exercise 4 and 5 the Kinect
sensors were put on a table with 1m height and subject did the exercises which standing sidewise corresponding to the Kinect
view point. (c) In exercise 6 and 7 the Kinect sensors were put on a table with 1m height and subject trained facing the Kinect
sensors.
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation
131
Eltoukhy et al. (Eltoukhy et al. 2017) used Vicon
marker-based motion capture system to evaluated
Microsoft Kinect v2 and showed Kinect v2
measurements on knee ROM presented high
consistency and agreement with the gold standard and
the calculated absolute error for knee angle was 2.14°.
While in this study average RMSE for knee angle was
4.93°. Bonnechere et al. (Bonnechère et al., 2014)
evaluated validity of Microsoft Kinect v1 and the
reported poor to no agreement between gold standard
and Kinect v1 measurement for knee flexion. Bland
Altman calculations for Kinect v1 in this study also
emphasizes on lower agreement with gold standard in
comparison to other systems. Wiedemann et al.
(Wiedemann et al., 2015) used Kinect v2 to estimate
knee angle in 16 different static postures. Median
difference for the left knee was 0.26° where upper and
lower bounds were 16.47° and -11.84°.
Madgwick et al. (Madgwick et al., 2011) and Diaz
et al., (2015) used Vicon motion capture system to
evaluate developed AHRS algorithm using IMU
sensors. The result in this study is comparable with
their finding.
In summary, we can conclude that both wearable
sensors and Microsoft Kinect v2 had acceptable
performance for tracking knee movements while
performing knee rehabilitation exercises, but we need
to keep it in mind Microsoft Kinect v2 has three
noticeable limitation which they may argue usability
of Kinect v2 for tracking daily knee rehabilitation
exercises. First, Kinect v2 skeleton algorithm was not
able to detect skeleton body and estimate
corresponding joints position while the subject was
lying in a bed. The first three exercises in this study
were performed where the subject lying in a bed.
Secondly, subjects should stand in front Kinect v2
sensor with optimal distance (2-3.5m) while the body
is seen by cameras. This may pose issues while
subject is doing the exercise behind a chair or any
other objects may cover the body. Final limitation
may argue required computation resources for
estimating joint positions, while joint angle may
estimate without any external computer using
wearable sensors.
5 CONCLUSIONS
Accuracy and usability of wearable sensors and
Microsoft Kinect sensors as low-cost portable
alternative human body tracking systems for knee
rehabilitation application were evaluated. The
findings indicated that wearable sensors and
Microsoft Kinect v2 have acceptable accuracy.
Whereas, usability of Microsoft Kinect v2 might be
argued due to it is unable to track physical activities
in particular circumstances specifically while the
users laying on the floor or in a bed.
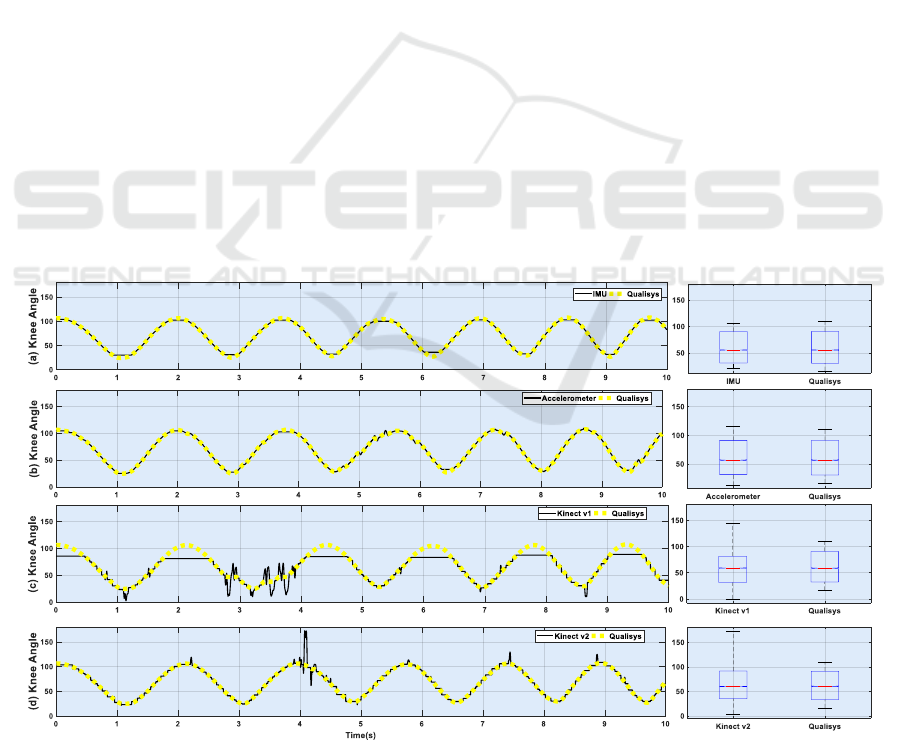
Figure 4: estimated knee angle using gold standard (dotted yellow line), (a) IMUs, (b) accelerometers, (c) Microsoft Kinect
v1, and (d) Microsoft Kinect v2.
BIODEVICES 2018 - 11th International Conference on Biomedical Electronics and Devices
132

Table 2: Summary of results on estimated knee angle using Qualisys, Accelerometer sensors, IMU sensors, Microsoft Kinect
v1, and Microsoft Kinect v2 for each exercise. ROM stands as range of motion and RMSE represents root mean square error.
LOA, B, and CV stand as 95% limits of agreement, bias, and coefficient of variations. Pearson correlation coefficient in this
table is shown by R.
Exe 1
Exe 2
Exe 3
Exe 4
Exe 5
Exe 6
Exe 7
ROM
Qualisys
[20,25]
[22,102]
[2,95]
[16,110]
[21,85]
[22,105]
[19,116]
Acc
[20,24]
[7,98]
[0,93]
[12,115]
[11,89]
[16,101]
[20,114]
IMU
[18,24]
[11,101]
[3,89]
[21,105]
[33,86]
[31,102]
[23, 201]
Kinectv1
-
-
-
[0, 144]
[1,81]
[3,72]
[1,85]
Kinectv2
-
-
-
[ 3,172]
[4,106]
[10,88]
[2,99]
RMSE
Acc
0.46
3.44
0.92
1.00
1.66
2.78
4.34
IMU
0.39
2.73
0.92
3.78
6.74
3.34
3.85
Kinectv1
-
-
-
10.21
12.52
17.61
13.29
Kinectv2
-
-
-
5.31
3.57
6.61
4.23
LOA
Acc
3.86
22.07
78.28
5.8
13.41
8.46
26.21
IMU
3.17
26.51
61.36
35.81
49.04
24.37
26.55
Kinectv1
-
-
-
25.25
33.23
42.63
26.47
Kinectv2
-
-
-
38.66
23.63
14.40
13.84
B
Acc
-0.45
-4.64
14.34
0.09
-1.72
-1.29
6.34
IMU
-0.46
-2.88
11.96
7.81
13.90
3.77
4.67
Kinectv1
-
-
-
-4.86
-10.50
-11.45
-8.53
Kinectv2
-
-
-
7.35
-0.76
-3.70
-1.78
CV
Acc
9
22
280
5
12
6
21
IMU
7
27
210
31
43
18
21
Kinectv1
-
-
-
22
33
35
24
Kinectv2
-
-
-
32
22
11
12
R
Acc
0.894
0.987
0.999
1
0.998
0.994
0.991
IMU
0.920
0.992
0.999
0.996
0.983
0.993
0.994
Kinectv1
-
-
-
0.964
0.908
0.796
0.949
Kinectv2
-
-
-
0.988
0.99
0.973
0.993
ACKNOWLEDGMENT
This study is supported by the Aage and Johanne
Louis-Hansen foundation, Aalborg University and by
the partners. For further information, see http://www.
labwellfaretech.com/fp/kneeortho/?lang=en
REFERENCES
Ahmed, H. & Tahir, M., 2017. Improving the Accuracy of
Human Body Orientation Estimation with Wearable
IMU Sensors. IEEE Transactions on Instrumentation
and Measurement, 66(3), pp.1–8. Available at:
http://ieeexplore.ieee.org/document/7811233/.
Anton, D. et al., 2016. Validation of a Kinect-based
telerehabilitation system with total hip replacement
patients. Journal of telemedicine and telecare, 22(3),
pp.192–197.
Auvinet, E. et al., 2017. Validity and sensitivity of the
longitudinal asymmetry index to detect gait asymmetry
using Microsoft Kinect data. Gait and Posture, 51,
pp.162–168. Available at: http://dx.doi.org/10.1016/
j.gaitpost.2016.08.022.
Bao, L. & Intille, S.S., 2004. Activity Recognition from
User-Annotated Acceleration Data. Pervasive
Computing, pp.1–17.
Bonnechère, B. et al., 2014. Validity and reliability of the
Kinect within functional assessment activities:
Comparison with standard stereophotogrammetry. Gait
and Posture, 39(1), pp.593–598.
C-Motion, 2017. Visual 3D. Available at: http://www2.c-
motion.com/products/visual3d/ [Accessed July 26,
2017].
Clark, R. A. et al., 2012. Validity of the Microsoft Kinect
for assessment of postural control. Gait and Posture,
36(3), pp.372–377. Available at: http://dx.doi.org/
10.1016/j.gaitpost.2012.03.033 [Accessed February 5,
2016].
Darby, J. et al., 2016. An evaluation of 3D head pose
estimation using the Microsoft Kinect v2. Gait &
Posture, 48, pp.83–88.
Diaz, E. M. et al., 2015. Evaluation of AHRS algorithms for
inertial personal localization in industrial environ-
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation
133

ments. In Proceedings of the IEEE International
Conference on Industrial Technology. pp. 3412–3417.
Eltoukhy, M. et al., 2017. Improved kinect-based
spatiotemporal and kinematic treadmill gait
assessment. Gait and Posture, 51, pp.77–83. Available
at: http://dx.doi.org/10.1016/j.gaitpost.2016.10.001.
Huber, M. E. et al., 2015. Validity and reliability of Kinect
skeleton for measuring shoulder joint angles: A
feasibility study. Physiotherapy (United Kingdom),
101(4), pp.389–393. Available at: http://dx.doi.org/
10.1016/j.physio.2015.02.002.
Hyde, R. A. et al., 2008. Estimation of upper-limb
orientation based on accelerometer and gyroscope
measurements. IEEE Transactions on Biomedical
Engineering, 55(2), pp.746–754.
Kalkbrenner, C. et al., 2014. Motion Capturing with Inertial
Measurement Units and Kinect - Tracking of Limb
Movement using Optical and Orientation Information.
Proceedings of the International Conference on
Biomedical Electronics and Devices, pp.120–126.
Available at: http://www.scitepress.org/DigitalLibrary/
Link.aspx?doi=10.5220/0004787601200126.
Karantonis, D. M. et al., 2006. Implementation of a real-
time human movement classifier using a triaxial
accelerometer for ambulatory monitoring. IEEE
Transactions on Information Technology in
Biomedicine, 10(1), pp.156–167.
Lange, B. et al., 2012. Interactive Game-Based
Rehabilitation Using the Microsoft Kinect. Ieee Virtual
Reality Conference 2012 Proceedings, pp.170–171.
Available at: http://www.scopus.com/inward/record.
url?eid=2-s2.0-84860745387&partnerID=tZOtx3y1
[Accessed February 8, 2016].
Lin, J. F. S. & Kulic
́
, D., 2012. Human pose recovery using
wireless inertial measurement units. Physiological
measurement, 33(12), pp.2099–115. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/23174667.
Madgwick, S. O. H., Harrison, A. J. L. & Vaidyanathan, R.,
2011. Estimation of IMU and MARG orientation using
a gradient descent algorithm. In IEEE International
Conference on Rehabilitation Robotics.
Mentiplay, B. F. et al., 2015. Gait assessment using the
Microsoft Xbox One Kinect: Concurrent validity and
inter-day reliability of spatiotemporal and kinematic
variables. Journal of Biomechanics, 48(10), pp.2166–
2170. Available at: http://dx.doi.org/10.1016/j.jbio
mech.2015.05.021 [Accessed June 2, 2015].
Microsoft, 2014. Kinect for Windows SDK 2.0. Available
at: https://www.microsoft.com/en-us/download/details.
aspx?id=44561 [Accessed January 31, 2017].
Microsoft, 2013. Kinect for Windows SDK v1.8. Available
at: https://www.microsoft.com/en-us/download/details.
aspx?id=40278 [Accessed January 31, 2017].
Pavão, S.L. et al., 2014. [Impact of a virtual reality-based
intervention on motor performance and balance of a
child with cerebral palsy: a case study]. Revista paulista
de pediatria : orga
̃
o oficial da Sociedade de Pediatria
de Sa
̃
o Paulo, 32(4), pp.389–94. Available at:
http://www.sciencedirect.com/science/article/pii/S010
3058214000173 [Accessed February 10, 2016].
Pedraza-Hueso, M. et al., 2015. Rehabilitation Using
Kinect-based Games and Virtual Reality. Procedia
Computer Science, 75(Vare), pp.161–168. Available at:
http://www.sciencedirect.com/science/article/pii/S187
7050915036947 [Accessed December 30, 2015].
Piqueras, M. et al., 2013. Effectiveness of an interactive
virtual telerehabilitation system in patients after total
knee arthoplasty: a randomized controlled trial. Journal
of rehabilitation medicine, 45(4), pp.392–6. Available
at: http://www.mendeley.com/catalog/effectiveness-
interactive-virtual-telerehabilitation-system-patients-
after-total-knee-arthoplasty-ra/.
Roetenberg, D., Luinge, H. & Slycke, P., 2013. Xsens
MVN : Full 6DOF Human Motion Tracking Using
Miniature Inertial Sensors. Technical report, pp.1–7.
Available at: http://en.souvr.com/product/pdf/MV
N_white_paper.pdf.
Russell, T. G. et al., 2011. Internet-Based Outpatient
Telerehabilitation for Patients Following Total Knee
Arthroplasty. Journal of Bone & Joint Surgery,
American Volume, 93–A(2), pp.113–120. Available at:
http://ezproxy.lib.ucalgary.ca/login?url=http://search.e
bscohost.com/login.aspx?direct=true&db=s3h&AN=5
7567660&site=ehost-live.
Schröder, Y. et al., 2011. Multiple kinect studies. Computer
Graphics, 2(4), p.6.
Sell, J. & O’Connor, P., 2014. The xbox one system on a
chip and kinect sensor. IEEE Micro, 34(2), pp.44–53.
Shimmer Sensing, 2016. Shimmer3 Wireless Sensor
Platform. Available at: http://www.shimmersensing.
com/products/shimmer3-development-kit [Accessed
November 7, 2017].
van Sint Jan, S., 2007. Color Atlas of Skeletal Landmark
Definitions, Elsevier Health Sciences.
Tousignant, M. et al., 2009. In home telerehabilitation for
older adults after discharge from an acute hospital or
rehabilitation unit: A proof-of-concept study and costs
estimation. Disability and Rehabilitation: Assistive
Technology, 1(4), pp.209–216. Available at: http://
www.ncbi.nlm.nih.gov/pubmed/19260168 [Accessed
February 24, 2016].
Tousignant, M. et al., 2011. Patients’ satisfaction of
healthcare services and perception with in-home
telerehabilitation and physiotherapists’ satisfaction
toward technology for post-knee arthroplasty: an
embedded study in a randomized trial. Telemedicine
journal and e-health : the official journal of the
American Telemedicine Association, 17(5), pp.376–82.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/
21492030 [Accessed January 10, 2016].
Tseng, Y. C. et al., 2009. A wireless human motion
capturing system for home rehabilitation. In
Proceedings - IEEE International Conference on
Mobile Data Management. pp. 359–360.
Vernadakis, N. et al., 2014. The effect of Xbox Kinect
intervention on balance ability for previously injured
young competitive male athletes: A preliminary study.
Physical therapy in sport : official journal of the
Association of Chartered Physiotherapists in Sports
Medicine, 15(3), pp.148–155. Available at:
BIODEVICES 2018 - 11th International Conference on Biomedical Electronics and Devices
134

http://www.sciencedirect.com/science/article/pii/S146
6853X13000709 [Accessed August 24, 2015].
Wiedemann, L. G. et al., 2015. Performance evaluation of
joint angles obtained by the kinect V2. Technologies for
Active and Assisted Living (TechAAL), IET
International Conference on, pp.1–6. Available at:
http://ieeexplore.ieee.org/xpl/articleDetails.jsp?tp=&ar
number=7389248&url=http%3A%2F%2Fieeexplore.i
eee.org%2Fxpls%2Fabs_all.jsp%3Farnumber%3D738
9248.
Woolford, K., 2015. Defining Accuracy in the Use of
Kinect V2 for Exercise Monitoring. Proceedings of the
2nd International Workshop on Movement and
Computing, pp.112–119. Available at: http://doi.acm.
org/10.1145/2790994.2791002%5Cnhttp://dl.acm.org/
ft_gateway.cfm?id=2791002&type=pdf.
Xu, X. & McGorry, R. W., 2015. The validity of the first
and second generation Microsoft Kinect
TM
for
identifying joint center locations during static postures.
Applied Ergonomics, 49, pp.47–54. Available at:
http://www.sciencedirect.com/science/article/pii/S000
3687015000149 [Accessed October 16, 2015].
Yeung, L. F. et al., 2014. Evaluation of the Microsoft
Kinect as a clinical assessment tool of body sway. Gait
& Posture, 40(4), pp.532–538. Available at:
http://dx.doi.org/10.1016/j.gaitpost.2014.06.012.
Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation
135
