
Dealing with Perceived Fairness when Planning Doctor Shifts
in Hospitals
Renaud De Landtsheer
1
, Ga
¨
etan Delannay
2
and Christophe Ponsard
1
1
CETIC Research Centre, Gosselies, Belgium
2
GeezTeem, Malonne, Belgium
Keywords:
User Acceptance, Scheduling, Rostering, Fairness, Metaheuristics.
Abstract:
Producing planning of doctors’ roles, including night shifts, on-call shifts (doctor can be called back in case
of need), and regular working day in a hospital is complex and it is often difficult to effectively address all real
world constraints. Furthermore, the produced solution requires a very good user acceptance to be effectively
deployed in production. This paper reports on the application of metaheuristics to solve a planning problem
in an hospital and focuses on user acceptance aspects of an algorithm. One of the key aspects to ensure user
acceptance is to ensure the comprehensibility of the delivered solution. This includes the understanding of
both the algorithm itself and its executions. The algorithm is a composition of local search, greedy algorithms,
tabu search, and a few additional metaheuristic principles, and proved both good and fast enough.
1 INTRODUCTION
In the hospital environment, efficient coordination is
of prime importance, notably to ensure that neces-
sary workforce is available at the required time, with
the required competences. This is because an hospi-
tal has to cope with possibly large flows of patients
that cannot be interrupted, and medical care requires
a set of specific competencies. Medical workforce is
needed at different roles throughout the week. These
include regular working role, on-site night shifts, and
on-call duty. Roles planning must obey a given set of
rules about resting time and cope with peoples’ non-
availabilities. Some equity between people is also re-
quired to maintain a good working atmosphere.
Setting up such planning is time consuming and
can be the source of personal frustrations since plan-
ning composition, when is performed by a human col-
league, can always be perceived as not objective and
thus unfair. Fairness in duty rostering is emphasised
in guidelines of many countries (NSW, 2015; NHS,
2016).
This paper presents a dedicated metaheuristic-
based algorithm that has been developed to automati-
cally compose such planning. The algorithm has been
designed to maximize user acceptance and perceived
fairness of the delivered planning. This means the al-
gorithm produces a “transparent solution”. Together
with the planning it also gives a clear trace explana-
tion of the taken decisions regarding a number of con-
straints or several priorities including constraints im-
pacting the fairness both at short and long term. To
make this trace comprehensible by doctors, the algo-
rithm relies on a relatively simple metaheuristic.
Of course the doctor scheduling problem (DSP)
and also the related nurse scheduling problem (NSP)
have received a large attention and solutions to those
problems have been proposed based on a large spec-
trum of techniques generally based on heuristic ap-
proaches such as tabu search, simulated annealing,
stochastic optimization, genetic algorithms or ant
colony optimization (Burke et al., 2004; Gendreau
et al., 2007; De Causmaecker and Vanden Berghe,
2011). Yet, planning algorithms can always be bi-
ased in one way or another by the person in charge of
the planning, and well-established generic algorithms
such as CP, LNS, or MIP can be perceived by the user
as efficient, but obscure black boxes. This might raise
suspicions regarding the fairness of the tool. A funda-
mental design choice of our approach is to not rely on
an existing optimization framework but to implement
a dedicated search procedure. The risk to reach a sub-
optimal solution was balanced with other constraints
such as the need to fully justify the resulting planning
and also some integration constraints.
This choice of developing an ad-hoc, simple meta-
heuristic is further discussed in the light of the user
feedback collected from real world deployment. The
320
Landtsheer, R., Delannay, G. and Ponsard, C.
Dealing with Perceived Fairness when Planning Doctor Shifts in Hospitals.
DOI: 10.5220/0006657403200326
In Proceedings of the 7th International Conference on Operations Research and Enterprise Systems (ICORES 2018), pages 320-326
ISBN: 978-989-758-285-1
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

deployment was conducted by the MedErgo company
which triggered this research and has integrated the
result in the scope of their product, with name Nice-
Watch (MedErgo, 2016).
The paper is structured as follows: Section 2
presents the considered planning problem and its con-
straints with a focus on equity. Section 3 presents the
technical approach to solve the problem and the con-
sidered metaheuristics. Then, Section 4 discusses on
the different mechanisms that have been deployed in
order to maximize user acceptance. Section 5 presents
related work sharing the same concerns of facilitating
the user acceptance. Finally, Section 6 draws some
conclusions and research perspectives.
2 PROBLEM STATEMENT
This section presents the considered rostering prob-
lem, with a focus on aspects that can cause doctor
frustration.
A planning ranges over a given period of time, and
defines, for each day of this period of time and each
role, who among the set of available doctors will fill
in this role. Roles can be regular workday at a given
place (anaesthetist in operating theatre no 2, emergen-
cies), on-site night duty, or home based on-call duty.
With respect to rostering, doctors are character-
ized by a set of legal and organizational attributes
such as contractual availability, qualification, maxi-
mal number of duty per month, degree of seniority
and assignable duty roles.
Besides, there is also a set of personal constraints
to be considered, including personal days off that
are considered as strong constraints as soon as they
are granted, and personal preferences regarding duty
roles. These can be positive or negative preferences.
Planning must also obey as set of legal rules re-
garding resting times:
• a duty role at the hospital lasts for 24 or 25 hours.
If happening during the week, it starts during the
normal working hour starting at 8 am and lasts
till 9 am the next day. If it occurs on a Saturday,
Sunday or legal holiday, it starts at 9 am and ends
at 9 am the next day. A duty role happening be-
tween and including Sunday to Thursday is auto-
matically followed by a day off. For a duty role
occurring on a Friday, the doctor gets half a day
off that can (s)he can place anywhere. For a duty
role happening on a Saturday, the next Monday is
a day off. Legal holidays are treated as Sundays,
and days before legal holidays as Fridays.
• A doctor can only fulfil a single role at a time.
• At any time, among all roles requiring a given
qualification, one of them at least must be occu-
pied by a senior doctor. For instance, emergencies
and anaesthetist roles.
• A doctor cannot be working or on any form of
duty when on holiday or when off its contractual
working days in case of part time contract.
• There must be at least five days between two con-
secutive duties of the same doctor.
• In any period of four weeks, a doctor can have at
most one duty occurring during the weekend.
• In case of a part time worker, a resting time fol-
lowing a duty cannot happen when the doctor is
not working according to the contract.
• A resting time cannot occur during holiday.
A consequence of the compensation system for
duty roles is that some of them are more attractive
than others. Duty roles happening on a Thursday are
the most attractive, since the doctor gets an extended
weekend of three consecutive days. The least attrac-
tive roles are the ones happening during the week-
end, since the compensation is smaller and they are
not covering regular working hours, so that the doc-
tor loses half a day off at the end. Friday and other
week days duties are in between. This attractiveness
is the main cause of frustration with duty roles as-
signment. Planning composition should therefore
be fair among doctors about this attractiveness of
duties. Inside a large doctor’s team, it’s indeed im-
possible to set up a monthly planning that takes into
account all the loads or attractiveness of this peculiar
month. One must thus figure out a way to spread out
the workload among individuals and over longer time
frames.
To summarize and prioritize, a planning must
comply with the following elements:
1. first, it must comply with the strong constraints
here above;
2. then, the personal preferences must be considered;
3. finally, the attractiveness of the planning must be
evenly spread across all doctors.
Some inequities can be tolerated temporarily, but
they must be compensated the next month. As dis-
cussed in the introduction, the planning must ensure
some fairness between doctors, and must propose
some mechanism to ensure that doctor have a good
perception that the algorithm was fair, even though
the planning might trigger some personal frustration.
There is also a requirement that the algorithm
must be deterministic. This ensures that the person
in charge of triggering the runs of the algorithm does
Dealing with Perceived Fairness when Planning Doctor Shifts in Hospitals
321

not have the possibility to trigger the algorithm on de-
mand to select a solution that better fits some non-
expressed desires. As a consequence, all random
functions used in our algorithm, notably to break ties,
rely on a deterministic pseudo-random generator.
A last non-functional requirement is the efficiency
of the planning engine: it must be able to generate a
complete schedule for a single month within a few
seconds.
3 SOLUTION DESIGN
3.1 Key Design Choices
It is difficult to ensure a good comprehensibility of the
algorithm and its execution using existing scheduling
engines relying on state-of-the-art algorithms. While
they are efficient and can deal with fairness, they are
also quite complex and hard to understand for non
computer scientists, and they are not designed to pro-
vide a traceability of the resulting solution. In order to
deal with this issue, a key decision is to implement a
dedicated search engine not relying on any framework
such as OscaR, Gecode, OR-tools, LocalSolver or any
others (OscaR Team, 2012; Gecode Team, 2017; OR-
tools Team, 2017; Benoist et al., 2011).
Attractiveness of the planning is a key element of
doctor satisfaction, so that it must be quantified in or-
der to reason upon it. The approach is to define a score
of discomfort for each doctor on a given planning. All
duties get a score of discomfort; the less attractive, the
higher is this score. The discomfort of a doctor for a
given planning is the sum of the discomfort of all du-
ties (s)he is assigned to in this planning.
With this mechanism of discomfort score, we can
model attractiveness, and compensate inequities from
one month to another one, by accumulating the score
of discomfort across months.
To find a solution, a greedy approach is used. Be-
cause it might fail to fill in a role, we therefore intro-
duced the notion for a role of being unassigned. The
key points are summarised here and detailed in the
rest of this section.
• The main loop is a simple loop that allocates doc-
tors to roles. It iterates onto unassigned roles, and
assigns them to a doctor.
• The role is selected to be among the unassigned
ones, as the one that has the fewest possible doc-
tors, in view of the strong constraints and with an
ordering based on the expressed preferences (pos-
itive or negative). In case of equality, a random
role is selected.
• Relaxation is used in case the system reaches a
step with no possible assignment. In this case a
role that was assigned to a doctor is unassigned to
generate the necessary degree of freedom.
• Diversification and cycle detection are also used
to avoid the system iterating over the same set of
partial allocations, leading to a dead end.
3.2 Metaheuristic: Greedy Approach
The algorithm itself is a greedy approach, with possi-
bility to undo some of the greedy decisions. At each
iteration a role is picked up, and a doctor is selected
for this role. The algorithm has the possibility to re-
lax an assignment in case of no doctor can be selected
for the considered role. Finally, a tabu component
is added to prevent relaxing assignments too quickly,
and help escape local impossibilities.
Basically, the greedy search iterates on roles is
a well-chosen order, and assign the current role to a
doctor. It is summarised in Listing 1.
Listing 1: Greedy Algorithm for Role Assignment.
w h i l e ( r o l e T o A s i g n i s n o t em pty ){
v a l c u r r e n t R o l e =
s e l e c t r o l e i n r o l e T o A s s i g n
m i n i mizing d egr e eO f Fr e edo m ( r o l e )
v a l d o c t o r T o A s s i g n =
s e l e c t d o c t o r i n a d m i s s i b l e D o c t o r ( c u r r e n t R o l e )
max i miz i ng a f f i n i t y ( d o c t o r , c u r r e n t R o l e )
a s s i g n ( c u r r e n t R o l e , d o c t o r T o A s s i g n )
u p d a t e degr e e o f f ree d om a nd a d m i s s i b l e D o c t o r
}
The iteration on roles is based on the degree of
freedom of the role. Roles with the smallest degree of
freedom are assigned first. The degree of freedom of
a role is the number of doctors that can be assigned to
this role, given the strong constraints and the existing
assignments. It is updated every time an assignment is
performed, or relaxed. A role assignment may impact
the degree of freedom of another role because some
constraints impose a minimal delay between shifts,
notably through a resting period.
Ties for roles as well as doctor selection are bro-
ken based on a deterministic pseudo-random selec-
tion. We deliberately use a deterministic generator
because we want several runs of the algorithm to pro-
duce the same output.
The affinity between a doctor and a role is a
weighted sum involving:
• the preference (positive or negative) between the
role and the doctor.
• the attractiveness of the considered role, based on
weighting along the features of the role.
ICORES 2018 - 7th International Conference on Operations Research and Enterprise Systems
322
• a cumulated satisfaction score of the considered
doctor that sums up the attractiveness of the past
and already assigned role to this doctor.
3.3 Relaxing in Case of Impossibility
In case the algorithm reaches a point where the cur-
rent role cannot be fulfilled by any doctor, one or more
assignments are relaxed to provide the necessary free-
dom to the considered role. These are all related to the
same doctor, who is then assigned to that role.
The doctor is selected such that he can be assigned
to the role after some other assignments are relaxed.
This excludes all doctors that are not available this
day, based on their contract, for instance. The se-
lected doctor also minimizes the number of assign-
ments that are to be relaxed. Ties are broken based
on a deterministic pseudo-random selection, again to
ensure that the algorithm is deterministic.
3.4 Dealing with Allocation and
Deallocation Cycles
The relaxation performed in case of a role cannot
be assigned can lead to the algorithm oscillating in
a closed loop: a role “a” cannot be assigned, so an
assignment involving role“b” is relaxed. In turn to as-
sign role “b” the algorithm can relax role “a”, etc. To
prevent this, each assignment is added to a “tabu list”.
The tabu list is determined by setting a number
of iterations during which the assigned role cannot be
relaxed by the relaxation procedure.
4 PROTOTYPING AND
VALIDATION
The proposed algorithm was implemented for Med-
Ergo, a Belgian company provides a web-based soft-
ware application for doctor planning, called Nice-
Watch (MedErgo, 2016). The system is composed of
a global database containing the actual planning, and
a web-based user interface in which doctors can post
their own constraints, query their planning, interact
with other doctors to barter duty roles, etc. A specific
interface is also available to the coordinator to visual-
ize all individual constraints, and set up the planning.
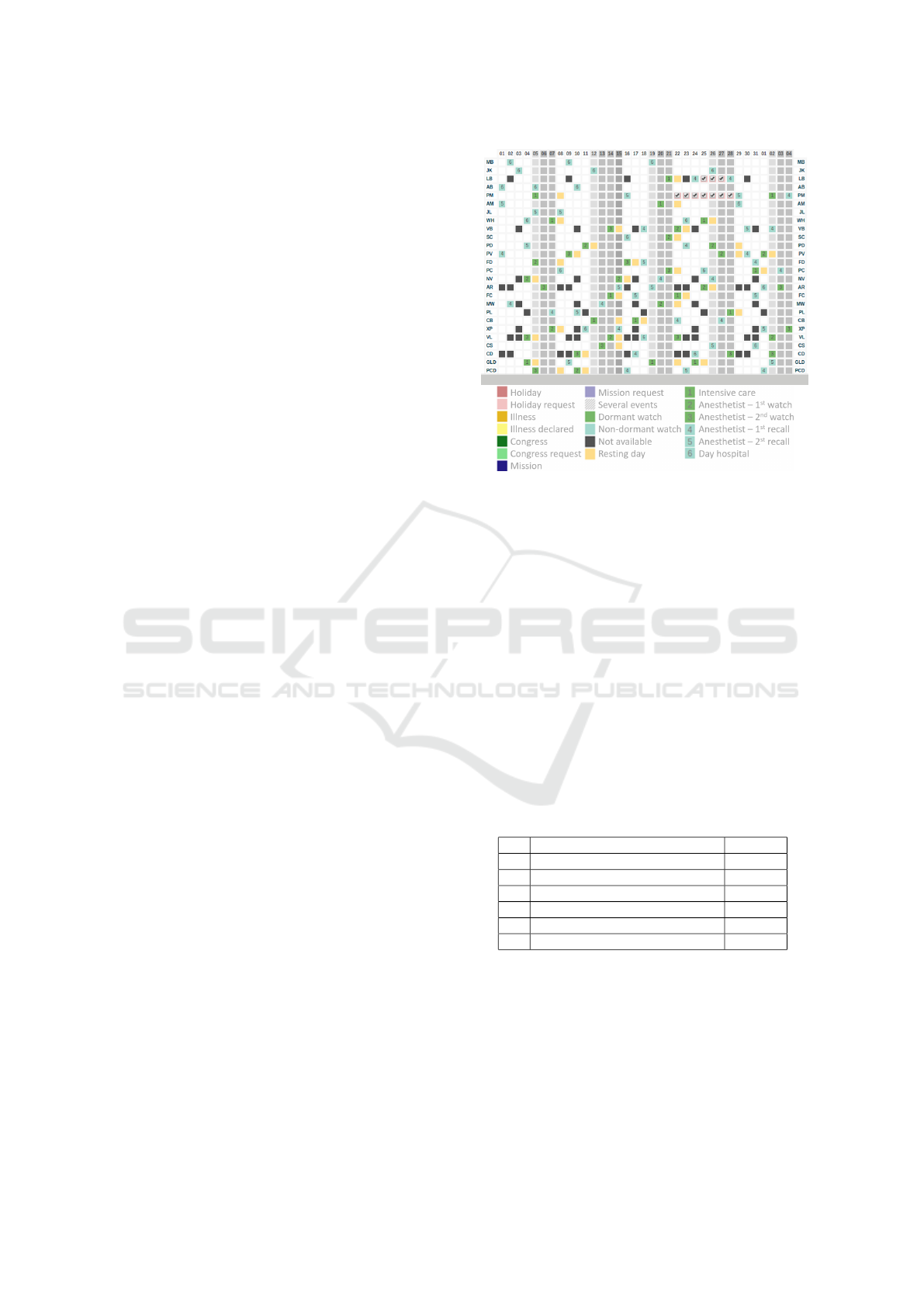
This interface is depicted in Figure 1.
A corollary of the need to implement the full
search procedure is that the algorithm could actually
be developed by a skilled developer not specialist in
optimisation with only some support from an expert.
The implementation was carried out in Python, an
Figure 1: Partial with of the planning interface with possible
constraints and allocations types.
Open Source multi-paradigm programming language
focusing more on expressiveness and ease of integra-
tion than on performance as it is usually interpreted
(van Rossum, 1991). The implementation was per-
formed following an Agile approach. This allowed
us to quickly validate that the algorithm performance
would not be a bottleneck and then to progressively
improve that performance to deal with more complex
constraints and to produce the justification reports.
Shifts are typically scheduled each month based
on the available doctor staff. The validation example
presented here is composed of about 50 doctors which
needs to ensure 5 simultaneous watch roles, some at
every day, some only on week days. Table 1 shows
the staff request for a typical month of 31 days.
Table 1: Typical Role Request for Different Watches.
Watch role # days
1 Intensive care 31
2 Anesthetist 1st watch 31
3 Anesthetist 2nd watch 31
4 Anesthetist 1st watch (recall) 31
5 Anesthetist 2nd watch (recall) 22
6 Day hospital 22
Figure 1 shows the planning interface displaying
both the constraints (coloured square without num-
ber) and the proposed allocation (coloured square
with number). The legend details the full set of pos-
sible constraints and allocations. During the planning
process a full allocation trace is generated and avail-
able for checking the allocation process. A typical
trace is displayed in Listing 2 for the first two slots of
some allocated day.
Dealing with Perceived Fairness when Planning Doctor Shifts in Hospitals
323
Listing 2: Justification Trace.
4 / 0 / 4 P r e f =1 P = 6.53 Av=30 DDC| U n a v a i l a b l e ( o f f )
1 / 0 / 1 P r e f =1 P = 5.90 Av=27 MAF
4 / 0 / 4 P r e f =1 P = 5.74 Av=31 MH
4 / 0 / 5 P r e f =1 P = 8.03 Av=31 DL
4 / 0 / 4 P r e f =1 P = 8.15 Av=31 KS
. . .
Day X − S l o t 1 − A l l o c a t e d t o : MAF
4 / 0 / 4 P r e f =1 P = 8.72 Av=30 CC | U n a v a i l a b l e ( o f f )
4 / 0 / 4 P r e f =1 P = 9.11 Av=31 KB | minDistanceKO
1 / 0 / 2 P r e f =1 P = 3.94 Av=21 RCA| minU nf av DistanceK O
1 / 0 / 2 P r e f =1 P = 4.15 Av=27 SC | mi nD is ta nc eK O
1 / 0 / 2 P r e f =1 P = 4.44 Av=18 WM
1 / 0 / 2 P r e f =1 P = 4.52 Av=22 VN
2 / 0 / 3 P r e f =1 P = 4.86 Av=31 VRP
. . .
Day X − S l o t 2 − A l l o c a t e d t o : WM
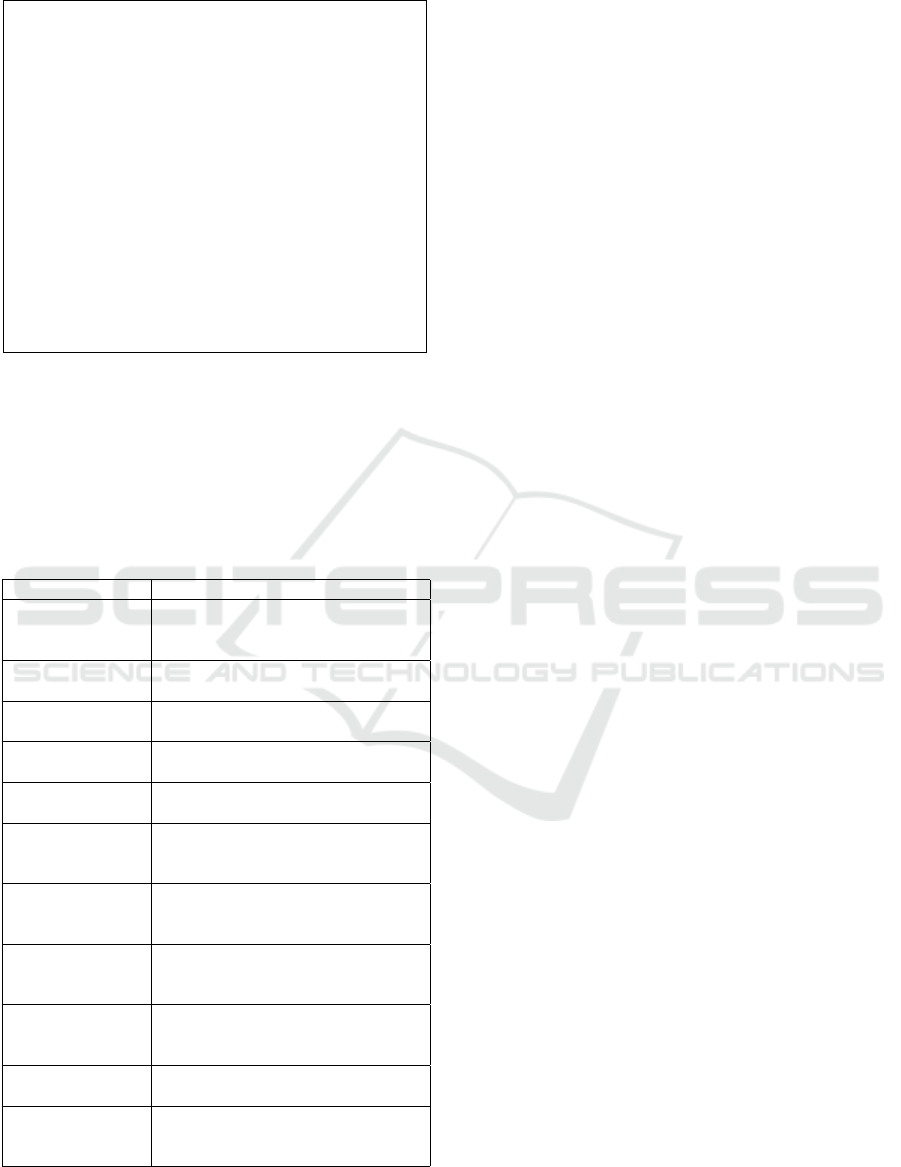
For each slot, a list reviewing possible doctor al-
locations is compiled. The list starts with doctors that
cannot be allocated with a justification code whose
explanation is detailed in Table 2. It is followed by a
prioritised list of doctors using the ranking procedure
described in the previous section. The first available
doctor is the allocated one.
Table 2: List of Justification in Allocation Traces.
Justification Description
Unavailable Date is within the strong constraints
of the doctor (according to work
contract and vacations)
Unwanted Date is within the doctor’s wishes
not to be on duty
MaxFrequency
Reached
Maximum quota is reached for doc-
tor’s wanted watches
MaxFrequency
ReachedOutside
Maximum quota is reached for doc-
tor’s unwanted watches
RecoveryRule
Broken
This day is already assigned or is a
recovery day
MinDistanceKO The minimal delay between two
wanted watches cannot be re-
spected
MinDistance
UnwantedKO
The minimal delay between two
unwanted watches cannot be re-
spected
minUnfavourable
DistanceKO
The minimal delay between two un-
favourable dormant watches cannot
be respected
minUnfavourable
DistanceOutside
KO
The minimal delay between two un-
favourable dormant watches cannot
be respected
noSenior No senior doctor would have been
assigned to a set of paired roles
BlackListed This doctor cannot be assigned here
because it will lead to an impossi-
bility to complete the schedule later
Our tool was deployed in production in August
2016 in different Belgian hospitals, as part of the
NiceWatch web-based platform (MedErgo, 2016). Al-
though our solver is not has been developed using
standard data structures, the overall performance is
quite good as scheduled can be produced within a few
seconds and allow the user to wait for the result.
5 RELATED WORK
In DSP, fairness constraints are identified along other
constraints and typically formulated as the fair dis-
tribution of different types of shifts among doctors
with the same experience in (Gendreau et al., 2007).
Fairness received specific attention in the emergency
room context (Ferrand et al., 2011; Santos and Eriks-
son, 2014; Devesse et al., 2016).
MIP based heuristics have been used to create bal-
anced scheduling from the set of doctors (Devesse
et al., 2016). Integer programming has also been used
to take into account constraints of the schedule, dif-
ferent preference ranks w.r.t. shifts, and the histori-
cal data of previous schedule periods to maximize the
global satisfaction about the proposed shift schedule
(Lin et al., 2014). The resulting shifts and days-off
were fair and met the staff satisfaction.
In local search, an objective function is expressed
as a weighted sum of soft constraint violations. Such
an objective function has the advantage of being both
easy to understand and to implement. However, they
can produce unfair solutions because some high qual-
ity allocations can compensated low quality ones. A
solution proposed by (Smet et al., 2012) is to use a
function where the quality of the worst individual al-
location will directly impact the overall solution qual-
ity. In doing so, a planing will not be improved at the
expense of the worst individual case. Experimental
results have confirmed the resulting solution is more
fair, nevertheless a drawback is that the search seems
less efficient given the new structure of the function.
In addition to the lack of explanation traceability, this
reinforces us about our dedicated approach.
A complete overview of techniques for NSP with
some hint about how to come with personal con-
straints is presented in (Burke et al., 2001). Evolu-
tionary algorithms are quite commonly used and an
approach for the formulation of the fitness function
has proven to be very powerful both to enable ex-
tendibility and to provide a quick and explanatory
mechanism. We achieved the same results using our
own approach and our belief is that the technique used
is not the key point but rather the ability to take into
account the right set of constraints, including histori-
cal data as well as the ability to produce justifications.
The requirement for traceability also favour better ar-
ICORES 2018 - 7th International Conference on Operations Research and Enterprise Systems
324

chitecture which in turn ease the ability to deal with
more complex real-world constraints.
6 CONCLUSION
This paper reports on our research to develop a meta-
heuristic that intertwines mechanisms borrowed from
various technical origins (local search, greedy, tabu
search, etc.) with a specific attention to enable a good
fairness of the produced planning. A key point is that
the transparency on fairness constraints is more im-
portant than the level of optimality of the solution for
user acceptance. While a off-the self solution would
certainly achieve better results (i.e. less discomfort)
than our approach and also cope with fairness, it is
hard to achieve a good level of transparency with them
and hence there is a risk of early rejection. Our ap-
proach on the contrary is able to achieve transparency
about “even discomfort”. It also has the capacity to
evolve to reduce the level of discomfort. In the end,
the overhead of having to implement the algorithms
without relying on a framework is also not so high
when balanced with those advantages.
The proposed solution already proved quite use-
ful and could establish a good level of trust and peace
among users. Of course it can be improved. For ex-
ample, it should be noted that not every discomfort
can be assigned to a single shift but can also result
from a sequence/set of shifts/tasks can also lead to
discomfort. Our present work does not consider this
and could be extended in this direction. In this pro-
cess, the current data structures will probably show
their limits by slowing down the computation. To
cope with this, we could rely on data structures en-
abling incremental evaluation for faster exploration of
the search space as done by local search solvers (Os-
caR Team, 2012). At this point it is interesting to con-
sider switching to such a framework as users are less
challenging the system fairness. In the process we
will also be able to carry out computational compar-
ison between both approaches. We also plan to work
on a traceability feature for this framework.
The proposed approach could also be applied to
other areas of scheduling where fairness and user ac-
ceptance are important issues (e.g. care pathways)
with however the drawback that the underlying frame-
work is not generic and must thus be revisited for each
new problem.
ACKNOWLEDGEMENTS
This research was partly funded by the Walloon regi-
on as part of the PRIMa-Q CORNET project (nr.
1610019). We warmly thanks MedErgo for allowing
us to share this case.
REFERENCES
Benoist, T., Estellon, B., Gardi, F., Megel, R., and Nouioua,
K. (2011). Localsolver 1.x: a black-box local-search
solver for 0-1 programming. 4OR, 9(3):299 – 316.
Burke, E. K., De Causmaecker, P., Berghe, G. V., and
Van Landeghem, H. (2004). The state of the art of
nurse rostering. Journal of Scheduling, 7(6):441–499.
Burke, E. K. et al. (2001). Fitness evaluation for nurse
scheduling problems. In Proc. of the IEEE Congress
on Evolutionary Computation, volume 2, pages 1139–
1146 vol. 2.
De Causmaecker, P. and Vanden Berghe, G. (2011). A cat-
egorisation of nurse rostering problems. Journal of
Scheduling, 14(1):3–16.
Devesse, V., Santos, M. O., and Toledo, C. (2016). Fair-
ness in Physician Scheduling Problem in Emergency
Rooms. In Revista de Sistemas de Informao da FSMA,
pages 9–20.
Ferrand, Y. et al. (2011). Building cyclic schedules
for emergency department physicians. Interfaces,
41(6):521–533.
Gecode Team (2017). Gecode - an open, free, efficient con-
straint solving toolkit. Available under the MIT li-
cence from http://www.gecode.org/.
Gendreau, M. et al. (2007). Physician scheduling in emer-
gency rooms. In Proceedings of the 6th International
Conference on Practice and Theory of Automated
Timetabling VI, PATAT’06, pages 53–67, Berlin, Hei-
delberg. Springer-Verlag.
Lin, C.-C., Kang, J.-R., Liu, W.-Y., and Deng, D.-J. (2014).
Modelling a Nurse Shift Schedule with Multiple Pref-
erence Ranks for Shifts and Days-Off. Mathematical
Problems in Engineering.
MedErgo (2016). NiceWatch - Complex Schedules within
Seconds. http://www.nicewatch.net.
NHS (2016). Good practice guide: Rostering.
https://improvement.nhs.uk/uploads/documents/Rost
ering Good Practice Guidance Final v2.pdf.
NSW (2015). Principles of rostering.
http://www.health.nsw.gov.au/Performance/rostering/
Pages/principles.aspx.
OR-tools Team (2017). OR-tools: Operations re-
search tools developed at Google. Available from
https://code.google.com/p/or-tools/.
OscaR Team (2012). OscaR: Operational Research in
Scala. Available under the LGPL licence from
https://bitbucket.org/oscarlib/oscar.
Santos, M. and Eriksson, H. (2014). Insights into Physi-
cian Scheduling: a case study of public hospital de-
partments in Sweden. International journal of health
care quality assurance/MCB University Press, 27(2).
Dealing with Perceived Fairness when Planning Doctor Shifts in Hospitals
325

Smet, P., Martin, S., Ouelhadj, D., Ozcan, E., and Berghe,
G. V. (2012). Investigation of fairness measures for
nurse rostering. In Practice and Theory of Automated
Timetabling (PATAT), Son, Norway.
van Rossum, G. (1991). The python programming lan-
guage. https://www.python.org.
ICORES 2018 - 7th International Conference on Operations Research and Enterprise Systems
326
