
Telephone Intervention for Caregivers
Impacts of an Individualized Telephone Intervention Targeting the Caregiver of a
Person with Alzheimer’s with Nonaggressive Behavioural Symptoms
Anne-Sophie Godbout, Jean Vézina and Chantal Dubé
School of Psychology, University Laval, 2325 Allée des Bibliothèques, Québec, Canada
Keywords: Caregiving, Alzheimer’s Disease, Behavioural Symptoms.
Abstract: Caregiving for a person with Alzheimer’s disease can have a negative impact on the individual who has to
endorse this role. High levels of depressive symptoms, anxiety, caregiver burden, and desire to
institutionalize have been reported in the literature. Those consequences justify the development of efficient
interventions that will diminish the individual and societal repercussions of the role of caregiving for a
person with Alzheimer’s disease. The main objective of this study is to evaluate the impacts of a telephone
intervention for caregivers of a person with Alzheimer’s disease. To do so, 50 caregivers were recruited and
randomly assigned to the control group (n = 25) or the intervention group (n = 25). Results show that
caregivers who were assigned to the intervention group showed significant lower levels of depressive
symptoms, anxiety symptoms, caregiver burden and desire to institutionalize. These results support the
pertinence to develop interventions that can help caregivers cope with their role and with the management
of the symptoms of the care receiver.
1 INTRODUCTION
It is now well documented that caregiving for
someone with Alzheimer’s disease can have major
and deleterious impacts on both the mental and
physical health of the person who takes that role
(Alzheimer’s Association, 2017; Liu, & Gallagher-
Thompson, 2009; Vaingankar et al., 2016). High
levels of anxiety, depressive symptoms, caregiver
burden and desire to institutionalize are observed in
this population (Alzheimer’s Association, 2017).
Research has also shown that out of all
categories of symptoms that are observed in
Alzheimer’s disease, behavioural symptoms are
those that have the most negative impacts on the
caregiver’s health (Feast, Moniz-Cook, Stoner,
Charlesworth, & Orrell, 2016; Shiji, George, Price &
Jacob, 2009).
The main objective of this study is to evaluate
the impact on anxiety symptoms, depressive
symptoms, caregiver burden and desire to
institutionalize a telephone intervention for
caregivers of a person with Alzheimer’s disease with
nonaggressive behavioural symptoms.
2 METHODS
2.1 Participants
A total of 50 caregivers of a person with
Alzheimer’s disease were recruited. They were
randomly assigned to either the intervention group
(IG; n = 25) or the control group (CG; n = 25). To be
eligible to participate in this study, the inclusion
criteria for the caregiver were (1) to be the main
caregiver of a person with Alzheimer’s disease for at
least 6 months before the beginning of the study
(2) to have been living with this person for at least 6
months (3) to have a significant level of caregiver
burden (e.g., a score higher than 6 on Zarit’s
caregiver burden scale), (4) not to have frequented
support group in the last 3 months and (5) not to
have auditive problems that are not compensated by
an auditive aid. The inclusion criteria for the person
with Alzheimer’s disease were (1) to have received
the diagnosis at least 6 months before the beginning
of the study, (2) to be at least 50 years old, (3) to be
living at home, (4) to show nonaggressive
behavioural symptoms such has agitation,
wandering, repetitive mannerism on a weekly basis
Godbout, A., Vézina, J. and Dubé, C.
Telephone Intervention for Caregivers.
DOI: 10.5220/0006670500210025
In Proceedings of the 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2018), pages 21-25
ISBN: 978-989-758-299-8
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
21

for at least 4 weeks, and (5) to have obtained a score
on the Dementia Behaviour Disturbance Scale
(DBDS; Baumgarten, Becker & Gauthier, 1990) that
indicates a high level of disturbing behaviour
demonstrations.
2.2 Assessment Measures
A sociodemographic questionnaire was used to get
information on the caregiver’s health state, their
desire to institutionalize the care receiver, their
support system and the services and resources used
were collected. The caregivers also completed the
Beck’s Depression Inventory (BDI; Beck, 1978) to
evaluate caregivers’ depressive symptoms, the Sate-
Trait Anxiety Inventory (ASTA-65+; Bouchard,
Ivers, Gauthier, Pelletier, & Savard, 1998) to
evaluate anxiety symptoms, and Zarit’s Caregiver
Burden Inventory (IFZ; Zarit, Orr, & Zarit, 1985).
The measures used to evaluate the care receiver
were the DBSD (Baumgarten et al., 1990), the
Modified Mini-Mental State (3MS; Hébert, Bravo,
& Girouard, 1992) and the Functional Autonomy
Measurement System (SMAF; Hébert, Carrier &
Bilodeau, 1988).
2.3 Procedure
Participants were recruited with the help of
community organizations. Their contact information
was given to the research team after the caregivers
gave their authorization. Their eligibility was
validated by phone. Each time 4 participants were
eligible, they were randomly assigned to either one
of the experimental situations: the intervention
group (IG) or the control group (CG). Participants
assigned to the CG group were then told that they
were on a waiting list and that they could expect to
receive the treatment in the next 6 months.
A first face-to-face interview between the
caregiver and a member of the research team was
used as the first time of measure. The caregiver was
interviewed for a second time when the treatment
was completed (T1), and three months after (T2).
2.4 Intervention
The treatment consists of 12 individual sessions.
Those are by phone and have a lasting time of
approximately 45 minutes. The program targets the
strategies that the caregiver uses to deal with the
non-aggressive behavioural symptoms of the
disease.
The member of the research team that gave the
treatment was a trained nurse with a degree in
psychology and who had work experience with older
people. She received training during which she was
also given a manual describing the themes and
objectives of each 12 sessions of the treatment
program.
The first sessions were randomly recorded to
ensure the validity of the protocol. Supervision was
given all through the experiment to make sure the
treatment was followed.
The themes covered during the session were the
Alzheimer’s disease (sessions 1 and 2),
consequences of the disease on the caregiver
(session 3), communication with the care receiver
(session 4), the behavioural symptoms of the care
receiver and the possible solutions (sessions 5 to 10),
the available resources that the caregiver could use
(session 11), and the synthesis of the treatment
(session 12).
2.5 Statistical Analysis
The statistical analyzes were made using the SAS-
PC software. First, t-tests were used to describe
the participants’ sociodemographic characteristics
and to compare the two experimentation groups (IG
and CG) on those variables. Since the desire to
institutionalize is a categorical variable, a chi-square
test was performed. Secondly, an analysis of
variance (ANOVA) was used to compare both
groups of caregivers on the measures of depressive
symptoms (BDI), anxiety symptoms (STAI) and
caregiver burden (ZCBI) at T0. ANOVAs were also
used to compare the two care receivers group on the
measure of the frequency and the severity of their
behavioural symptoms (DBDS), their cognitive
functions (3MS) and their functional autonomy
(SMAF).
Finally, the effect of the intervention was
calculated using a multivariate analysis of variance
(MANOVA) with repeated measures. The dependent
variables were the intervention conditions.
Statistically significant results with the MANOVA
were followed by contrast and tendency analysis.
The same procedure was applied to evaluate the
effect of the program on the caregivers' assessment
of the frequency and severity of behavioural
problems of their Alzheimer's relative and the
measurement of their cognitive and functional. The
significance level used for all the tests was a
bilateral alpha threshold of 0.05 alpha.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
22
3 RESULTS
Table 1 presents the characteristics of the
participants on socio-demographic variables (i.e.
health status and services received by the study
group. The final sample consisted of 28 women
(56%) and 22 men (44%). On average, participants
in the study took care of their loved one for about 5
years and the majority of caregivers were the spouse
of the relatives they cared for. Statistical analyzes
revealed that there is no difference between the two
groups on the different descriptive variables.
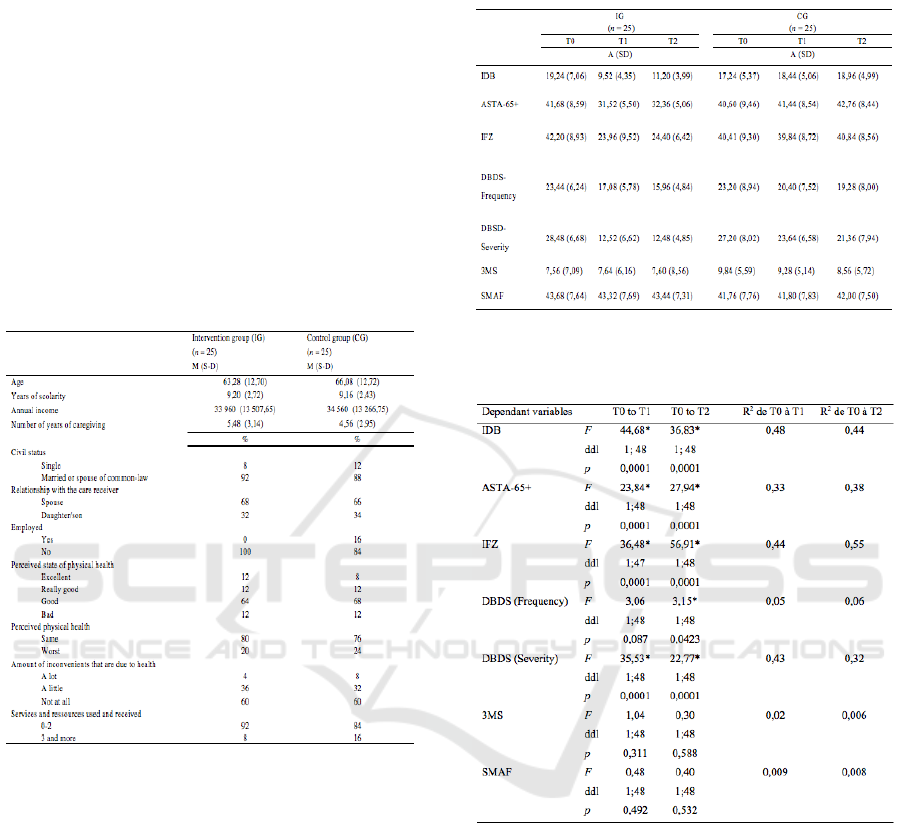
Table 1: Characteristics of caregivers in the IG and the CG
on socio-demographic variables, health status and services
received.
Table 2 shows the results of the three different
measurement time on the instruments evaluating the
dependent variables for the two experimental
groups. Statistical analyzes revealed that at T0 there
was no significant difference between the two
groups over all the variables measured. At T0,
caregivers in both groups have an average IFZ score
that indicates severe levels of burden.
Table 3 shows the results of the multivariate
analysis that compared the scores of both groups on
the dependent variables. The analysis made it
possible to compare the two groups between T0 and
T1 and between the T0 and the T2. Among the
caregivers, significant differences were between the
two groups with the results at the BDI, the ASTA-65
+ and the IFZ, both between the T0 and the T1 and
between the T0 and the T2.
Table 2: Scores on the dependent variables at each time of
measure.
Table 3: Results of the multivariate analysis comparing the
IG and the CG on the dependent variables.
The caregivers in the IG reported significantly
lower scores on all the instruments evaluating their
condition. As for the care receivers, those assigned
to the IG showed statistically significant lower score
compared to the CG group between T0 and T2 on
the frequency of behavioural disorders. Their scores
had decreased. No difference was observed between
the 2 experimental groups between T0 and T1 on
this variable. The severity of the behavioural
disorders were also significantly lower for the IG
between T0 to T1 and T0 to T2.
The Chi-Square test used to evaluate the desire to
institutionalize indicated a significant difference
between the IG and the CG, 2 (2, n = 25) = 16.96, p
= 0.0002 between T0 and T3. The caregivers
Telephone Intervention for Caregivers
23

assigned to the IG had lower scores than the
caregivers in the CG.
No statistically significant differences were
observed between the measuring times on the
instruments evaluating the cognitive functioning
(3MS) and the functional autonomy of the care
receiver (SMAF).
4 DISCUSSION
Caregiving for a person with Alzheimer's disease has
consequences on different aspects of the caregivers’
psychological and physical health. In fact, caregivers
show higher levels of depressive symptoms, anxiety
symptoms and caregiver burden. Those are linked to
earlier institutionalization of the person they are
caring for. The objective of this study was to
evaluate the effectiveness of an intervention
program in determining whether the caregivers who
received an intervention that helps them manage the
nonagressive behavioural symptoms displayed by
the person they take care of would differentiate from
the caregivers who did not receive the intervention
on measures of depressive symptoms, anxiety,
feeling of burden and desire for institutionalization
of the loved one. The following hypothesizes were
evaluated: caregivers in the IG would show less
depressive symptoms, experience a decrease in their
severity of their anxiety symptoms, have a lower
sense of burden, and would have a decrease in their
desire to institutionalize the person they cared for.
The results show that the importance of the
depressive and anxious symptoms of the caregivers
who received the intervention had decreased in a
tangible way compared to caregivers who have not
benefited from the intervention. In addition, the
perception that the caregiver had of the severity of
the behavioural symptoms of the care receiver
decreased significantly at each measurement time.
The hypothesis that the caregivers who received the
intervention would show a lower sense of burden
than those in the CG was also confirmed. The
caregivers assigned to the IG also expressed a lower
level of desire to institutionalize the care receiver
than the caregivers assigned to the CG. This last
finding could have interesting implications in
reducing the economic and societal costs of
Alzheimer’s disease.
The results of this program seem to indicate that
the intervention has improved the participants’
perceptions of their caregiving skills and increased
their sense of control and capacity to manage the
nonaggressive behavioural symptoms displayed by
their loved one.
It has to be mentioned that even though no
differences were observed on the cognitive and
functional symptoms of the care receiver, the
caregivers assigned to the IG showed decreased
symptoms on all the variables on which they were
evaluated after the treatment program was
completed. As a matter of fact, only the perception
that the caregivers had of the severity and frequency
of the behavioural symptoms were significantly
lower at T3. This finding gives support to the idea
that behavioural symptoms have the most negative
impacts on the caregiver’s health.
Three main elements come out of the results
obtained in this study. First, the program was
individualized, allowing a more personalised and
targeted intervention. Although group interventions
have proven to be an effective treatment option, the
results of this study seem to indicate that
individualized interventions are an interesting and
efficient alternative for caregivers that cannot attend
groups. Therefore, this individualized intervention
could be implemented with caregivers that express
specific needs regarding the behavioural symptoms
of the person they care for.
Secondly, the format of the intervention made it
possible to reach a larger number of caregivers.
Transport issues and busy schedules are important
obstacles to treatment seeking that are often inherent
to caregiving. However, this study provides
evidence that the use of technologies (i.e.:
telephone) are useful tools to give caregivers access
to efficient treatment programs.
Finally, the focus on the behavioural disorders
appears to contribute in great part to the efficacy of
the intervention. As mentioned before, the treatment
specifically targeted the nonaggressive behavioural
symptoms of Alzheimer’s disease. The
improvements observed on the different measures
can lead us to believe that interventions addressing
specific symptoms – in this case nonaggressive
behavioural symptoms – can have a positive impact
on the caregiver’s psychological health. In this
sense, the results seem to show that it is important to
address this type of behaviour more systematically
with caregivers, to try to understand the
consequences that they may have on them and to
help them manage these behaviours in order to
improve their psychological health. This finding
could help improve the efficiency of the care
services offered by introducing shorter and targeted
treatment.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
24

5 CONCLUSIONS
On a daily basis, the caregivers are exposed to the
cognitive, functional and behavioural symptoms of
the care receiver. Since it is well documented that
the behavioural symptoms of Alzheimer’s disease
contribute in high proportions to the negative effects
that caregiving can have on the caregivers’ health,
interventions targeting the management of this
category of symptoms could contribute to
diminishing the social, psychological and economic
cost of this disease. The results of this study give
support to the idea that these types of interventions
could benefit the caregivers.
REFERENCES
Alzheimer’s Association. 2017. Alzheimer’s facts and
figures. Alzheimer’s & Dementia, 13, 325-373.
Baumgarten, M., Becker, R., Gauthier, S. 1990. Validity
and Reliability of the Dementia Behaviour
Disturbance Scale. Journal of the American Geriatrics
Society, 38, 221-226.
Beck, A. T. 1978. Depression Inventory. Philadelphia:
Center for Cognitive Therapy.
Bouchard, S., Ivers, H., Gauthier, J., Pelletier, M.H.,
Savard, J. 1998. Psychometric Properties of the French
Version of the Sate-Trait Inventory (form Y) Adapted
for older people. Canadian Journal on aging, 17, 440-
453.
Feast, A., Moniz-Cook, E., Stoner, C., Charlesworth, G.,
Orrell, M. A. 2016. A systematic review of the
relationship between behavioral and psychological
symptoms (BPSD) and caregiver well-being.
International Psychogeriatrics, 28, 1761-74.
Hébert, R., Bravo, G., & Girouard, D. 1992. Fidélité de la
traduction française de trois instruments d’évaluation
des aidants naturels de malades déments. Canadian
Journal of Aging, 12, 324-337.
Hébert, R., Carrier, R., Bilodeau, A. 1988. Le système de
mesure de l’autonomie fonctionnelle. Revue de
Gériatrie, 13,161-167.
Liu, W., Gallagher-Thompson, D. 2009. Impact of
dementia caregiving: Risks, strains, and growth. In:
Qualls SH, Zarit SH, eds. Aging families and
caregiving. Hoboken, N.J.: John Wiley & Sons, Inc.;
85-112.
Shiji, K.S., George, R.K., Prince, M.J., Jacob K.S.
2009. Behavioral symptoms and caregiver burden in
dementia. Indian Journal of Psychiatry, 51, 45–49.
Vaingankar, J.A., Chong S.A., Abdin, E., Picco, L.,
Shafie, S., Seow E., (...), Subramaniam, M. 2016.
Psychiatric morbidity and its correlates among
informal caregivers of older adults. Comprehensive
Psychiatry, 68, 178-85.
Zarit, S. H., Orr, N. K., Zarit, J. M. 1985. The Hidden
Victims of Alzheimer’s Disease: Families Under
Stress. New York: University Press.
Telephone Intervention for Caregivers
25
