
eHealth Context Inference
A Review of Open Source Frameworks Initiatives
Arsénio Reis
1,2
, Dennis Paulino
1,2
, Paulo Martins
1,2
, Hugo Paredes
1,2
and João Barroso
1,2
1
INESC TEC, Porto, Portugal
2
University of Trás-os-Montes e Alto Douro, Vila Real, Portugal
Keywords: eHealth Framework, Context Awareness, Context Inference, Predictive Models.
Abstract: The collection of health and fitness longitudinal data can be used to model disease progression and shape new
algorithms to diagnose and predict health hazards. Continuously tracking vital signs, in particular heart rate
and skin temperature, can be very informative by using models and algorithms to predict and notify the user
about when he might be falling ill. With the current wearable devices and the proper algorithms, the individual
can be permanently monitored, which might be much more interesting than a one-off reading comparison
with the population average, made by a doctor. It would be possible to intervene earlier and to prevent
somebody from becoming seriously ill. From a broader perspective, the knowledge about a user’s health can
be considered as an element of that user’s context and be used by context aware applications to provide higher
value to the user. After the trivialization of the data acquisition sensors, wearable devices, and raw data, the
next logical step is the development of contained software components that can infer and produce knowledge
from the raw data. These components and the knowledge they produce can be used by all sorts of applications
in order to further customize their usage by a specific user. Customization and context awareness, in regard
to health, is a wide field for research and there are a multitude of proposals for models and algorithms. In this
review work we searched for software components (frameworks, software libraries, etc.), freely available and
that can be used as building blocks for other computer systems by software developers.
1 INTRODUCTION
In this work, we conduct a review of the currently
available software systems, freely accessible to
developers, which can be used as software building
blocks, providing functionalities associated to
information inference and knowledge production,
related the user’s health status.
There are currently multiple wearable devices,
equipped with sensors, which can read vital signs
from a user. Some of these devices are not very
accurate, mainly developed and targeted for the low
end recreational and fitness market, others have
medical grade accuracy and are targeted for the high-
performance sports and medical environments.
For a health-related solutions developer, the raw
data must be interpreted according to the specific
purpose of the desire solution. In that regard, data
analysis and knowledge inference is a specific
research domain from which can be produced
software modules, encapsulating all the research and
deep knowledge necessaries to create the inference
functionalities. These modules can be used as
building blocks for other software solutions than will
then benefit from having knowledge regarding their
user’s health.
This work reviews and analyses the currently
available software systems, designed to provide
specific health knowledge and that can be used as
building blocks for more general software solutions.
In this document, we designate these systems as
frameworks and middleware in same sense as the
terms are used in software engineering, although not
being very strict and using the framework term even
when in fact the system doesn’t have all the elements
of a software framework according to the well-known
concept of software framework.
A framework is a structure or conceptual guide to
build an entity by expanding itself into something
useful. In electronic systems a framework, generally,
describes a layered structure of software programs
and hardware devices and how they are built,
interconnected, and interact, to provide a full system
functionality. The framework is comprehensive and
Reis A., Paulino D., Martins P., Paredes H. and Barroso J.
eHealth Context Inference - A Review of Open Source Frameworks Initiatives.
DOI: 10.5220/0006752707070714
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (HEALTHINF 2018), pages 707-714
ISBN: 978-989-758-281-3
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
prescriptive. In computer programming, a software
framework is an abstraction in which a software
system, providing a generic functionality, can be
extended to provide application specific functionality
by building and changing specific elements of the
framework, thus creating a specific solution from a
generic set of elements. The software framework
provides a standard way to build and deploy
applications. It can provide a functionality, as part of
a larger software platform, simplifying the
development of software application and solutions in
a universal and reusable environment, which may
include several types of elements, e.g., programs,
compilers, code libraries, tool sets, and application
programming interfaces (APIs) that can be used for
the development of a system.
Software frameworks have the following key
features that distinguishes them from other software
components. (1) inversion of control, in which is the
framework that controls the overall program's flow
and not the caller library or application; (2)
extensibility, providing mechanisms for the user to
extend the framework, by selective overriding or
addition of specialized user code to provide a specific
functionality; (3) non-modifiable framework code,
meaning the users can’t modify the framework’s code
but must extend it instead.
A software library is a collection of resources used
to develop software and build computer programs. It
includes configuration data, documentation, help
data, message templates, pre-written code and
subroutines, classes, values or type specifications,
etc. Usually these resources have specific behaviors
and are accesses by well-defined interfaces.
In software engineering, an Application
Programming Interface (API) is a set of subroutine
definitions, protocols, and tools for building
application software. It clearly defines the methods of
communication between various software
components. An API provides the methods for the
programmer to develop a computer program by
assembling together different building blocks.
An API usually describes and prescribes the
expected behavior of a software library, while the
library is an actual implementation of the
functionalities. The separation of the API from the
implementation allows programs written in one
language to use a library written in a different one
(Robillard et al., 2012).
Middleware is a software that stands in between
two software layers (in the middle), usually providing
value added services to software applications, on top
of those available from the operating system.
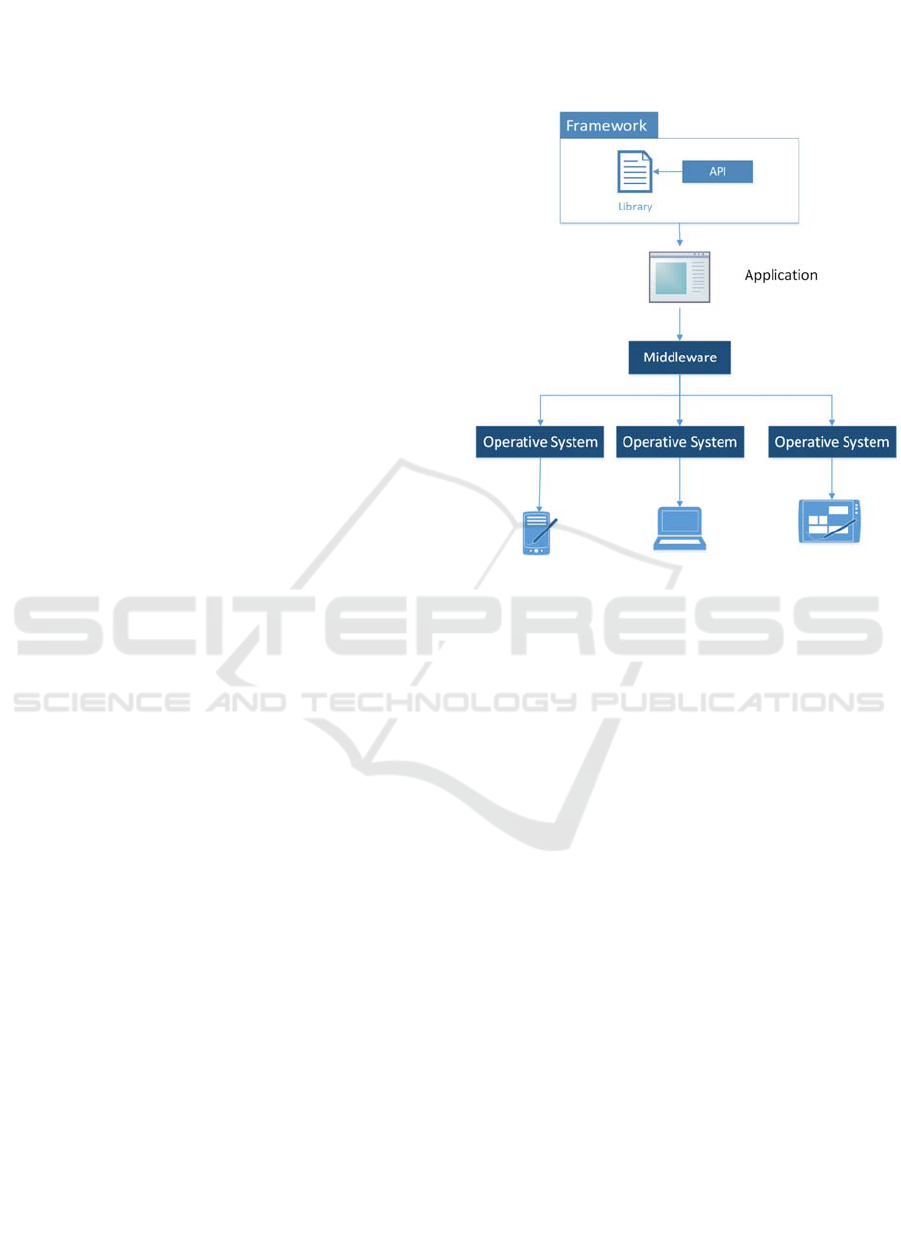
A framework can include a software library,
accessible by means of an API, and freely available
to the programming community as middleware
software, as represented in Figure 1.
Figure 1: Overview of the connections between framework,
middleware and API.
In the context of the software development
elements previously described (frameworks, libraries
and APIs), we are interested in those that can use
health related data, e.g., vital signs and others, and
produce health related knowledge, that can be used as
building blocks by user developed applications.
2 HEALTH DATA AND
PROGNOSTIC MODELS
Currently there are several consumer wearables and
portal services that can monitor some basic vital
signs, e.g., heart rate and skin temperature, allowing
the user to register and view their evolution over time.
Based on this data, models and algorithms can be
developed that will be able to predict the user’s health
status and evolution by computing the longitudinal
data of the basic vital signs. The recent consumer
grade wearables are not really expensive (some
hundred euros per device) and some have good
quality sensors, mainly developed for the fitness
market. These devices have, mostly, an informative
usage. They provide monitoring information to the
users. To have a real impact on the users’ health
management and on the health care system usage,

besides to provide information about the user’s vital
signs, this devices must also be able to analyze and
draw conclusions about the user’s health on his
behalf. It is then necessary to collect data and create
models and algorithms for the interpretation of the
vital signs data.
The abundance of wearable devices, together with
the Internet of Things (IoT) connectivity paradigm,
are very strong drives for the acquisition of real-time
data, particularly, data collection from individuals in
their daily lives, as well as in specific sportive
activities, such as the data of simple vital signs, e.g,
heart rate and skin temperature, as well as, more
complex data, regarding the individual health
evolution, e.g., ECG, surveys (Paulino et al, 2017;
Felisberto et al, 2015). The basic data can be used as
parameters to model specific health phenomena and
the complex data can be used to assess the correlation
of basic data patterns with the health phenomena. It is
then possible to create inference algorithms to predict
the user’s health evolution.
To create health related prediction models, several
techniques can be used, e.g, decision rules, score
systems, Markov processes, decision trees, neural
networks and Baysian networks. To model the
evolution of health phenomena over time, the Baysian
approach is one the most suitable solutions. However,
the adoption of a specific technique must be
considered according to the available data, specific
phenomena, and objective.
There are several techniques currently used to
create prognostic models. The simplest are the
decision rules, which are based on a prognostic score,
classifying the patient in a specific risk category
(Knaus et al., 1991). Also, in decision analysis, the
Markov decision processes, which is a stochastic
process that evolve over time, can be used as basis for
prognostic models (Sonnenberg et al., 1993). More
sophisticated techniques, with support from the
artificial intelligence community, are becoming
popular as prognostic models, including: decision-
trees, neural networks, support vector machines, and
Bayesian networks (Cruz et al., 2006; Ohno-
Machado, 1997). These techniques have much better
performance but require substantial amounts of
quality data.
The Bayesian networks technique have been
successfully used to model health phenomena, and
other natural phenomena, e.g., genomics and ecology
(Jansen et al., 2003), and has become a powerful tool
for the analysis of real-world data, from health and
the environment, leading to the shaping of novel
algorithms (Gerven et al., 2007; Lucas et al., 1995;
Murphy et al., 2002; Pearl et al., 2000). This tool and
the collection of longitudinal data are creating
research challenges for diagnosis and the modelling
of disease progression (Abu-Hanna, 2001).
Wearable devices can be used to track the
individual’s vital signs and detect when he is about to
get hill. In the follow-up of a recent research, by
wearing sensors during a long period (over an year),
Michael Snyder (Snyder, 2017) was able to detect
abnormal readings, showing an increase in heart rate,
when compared with his regular heart rate pattern,
and a rise in skin temperature. On a recent interview,
Snyder would confirm: “A mild fever soon followed,
and Snyder asked a doctor for the antibiotic
doxycycline, which can be used to treat Lyme
disease. His symptoms cleared within a day”.
Subsequent tests confirmed his self-diagnosis. Snyder
and his team are working with more than 40
volunteers, who wore smartwatch devices for up to
two years and have demonstrated a solution to detect
the first signs of illness by continuously monitoring
their pulse and skin temperature (Li et al., 2017;
Klein, 2017).
Several vital parameters can be continuously
monitored using wearable devices. The most frequent
is heart rate, as it is simple to monitor and has been
widely studied, regarding several aspects, e.g., its
levels, patterns, correlation with health, and death risk
(Johansen et al., 2013). Skin temperature can also be
monitor (Nakayama et al., 1977).
Heart rate variability (HRV) is a term that
indicates the level of changes in HR. It was firstly
used in 1846 when Carl Ludwing discovered
Respiratory sinus arrhythmia, through which HR
increases with inspiration and decreases during
exhalation. HR is controlled via the two components
of the autonomic nervous system (ANS):
Sympathetic and parasympathetic indices (Makivic et
al., 2013; Javorka et al., 2001). The sympathetic
component is responsible for the HR acceleration
during physical stress (i.e. exercise) whereas lower
HR (example: Resting HR) is an impact of the vagal
tone (parasympathetic tone) (Makivic et al., 2013).
Consequently, the balance between the two
components affects the time consistency between
Heart beats, which is measured through HRV
(Makivic et al., 2013).
Several studies have shown the correlation
between heart rate data and particular health
conditions. The analysis of heart rate variability
(HRV) and its pattern can provide an insight into the
health of the cardiovascular system (Javorka, 2001).
One of the simplest analysis, using heart rate data,
is the interpretation of the resting pulse rate (RPR),
which can provide useful information. RPR is a key

vital sign measure in clinical practices with widely
available reference data. Resting heart rate is
independently associated with increased risks of all-
cause and cardiovascular mortality, and, as shown by
(Zhang et al., 2016), can be used as a mortality
predictor. Beddhu et al, examined the association of
resting heart rate with insulin resistance,
cardiovascular events and mortality in the moderate
chronic kidney disease (CKD) population and have
demonstrated how higher resting heart is associated
with increased mortality and possibly cardiovascular
events in this population (Beddhu et al., 2009). There
are several other authors using heart rate as a
predictor for several health conditions, e.g., a tool for
risk stratification in primary care (Leistner et al.,
2012), osteoporotic fractures and mortality in older
women (Kado et al., 2012), cardiovascular mortality
in the general population (Hozawa et al, 2004), to
sudden death and all-cause mortality in asymptomatic
men (Adabag et al., 2008), coronary heart disease in
the elderly (Legeai et al., 2011).
In the context of the sports practice, the exercise
intensity assessment is important to inform the athlete
of the correct training effort and prevent overtraining
syndrome (OS) (Dressendorfer et al, 1985; Hedelin et
al., 2000) or sudden cardiac death (SCD) (Savonen,
2006; Batty et al., 2010).
According to (Link and Estes, 2012), SCD rates
in the US reaches 150 cases annually. Such cardiac
complications occur either due to the medical history
of the athlete or because of unmonitored exercising.
If a trainee exercised without exceeding the
endurance limit, then it is said he is in the functional
over-reaching (FO) where the safety is highly assured
and normal stamina can be obtained after hours/day
of recovery. However, ignoring the OR region might
lead to developing Overtraining syndrome (OS),
which is a precursor of SCDs.
The pattern associated with how the heart rate
recovers, after exercising, is a parameter that
represents how fast the heart returns to the normal
state after exercising. Typically, a drop of 12 bpm or
less in the first minute of recovery is considered
abnormal, and greater drop during this period
signifies that the person is fit (Cole et al., 2000; Reis
et al., 2016a).
With the vital signs collected data, e.g., HR and
skin temperature, and with the support of meta data,
it can be created longitudinal models and algorithms,
correlating the health hazards (e.g., physical
exhaustion, developing flu) and the HR patterns.
These models will represent the time progression of
the hazard and the algorithms will position the
individual in a specific time of the model, by
interpreting the patterns on the HR time line.
Although there are, currently available, devices
that can continuously monitor the basic vital signs,
the research, by Bloss et al., suggests: “there are not
large short-term increases or decreases in health care
costs or usage associated with monitoring chronic
health conditions using mobile health or digital
medicine technologies.” (Bloss et al., 2016; Reis et
al., 2016b). That is a disappointing conclusion, and
calls for further work to intelligently analyze the data
and deliver truly valuable information to the user, as
well as make the health-related inference and
knowledge production features available to the
general community of software solutions developers.
Context aware applications should then be able to
use the knowledge about the user’s health as part of
the user’s context. In a very simple example, a context
aware groceries store shopping application, besides
knowing the items that the user needs to buy, could
also know the items the users should avoid buying
due to its health status. Other applications have
proposed the usage of electronic assistants to interact
and accompany elderly people (Reis et al., 2017a;
Marceline et al., 2009; Reis et al., 2017b).
3 METHODOLOGY
For this review we defined the following
methodology in order to identify the software
frameworks to consider and study:
1. An internet search using the terms “software”,
“healthcare”, “health”, “inference”, “system”,
“middleware”, “framework”. The search was
conducted using the “publish or perish” software,
using the google scholar engine data. The search
was limited to 1,000 item and 980 items were
returned.
2. A filter, excluding surveys and literature reviews.
It returned 892 items.
3. A filter, excluding those without the term “health”
on their title. The return list was narrow down to
301 items.
4. A filter, by means of a comprehensive reading by
a researcher, and exclusion of those not related to
a software framework or middleware. The list was
shortened to 45 items.
5. A filter, excluding those not related to this work
theme or not having any bibliographic citation.
This filtered the results to 7 items.
After all the searching and filtering, the items were
carefully analyzed and described, namely regarding:
The inference algorithms (machine learning,
vector learning, deep learning, Bayesian, Rules,
Markov, etc);
The system’s learning strategy;
The types of data necessary for the inference to
work;
The pathologies for which the system can produce
knowledge;
4 ANALYSIS AND RESULTS
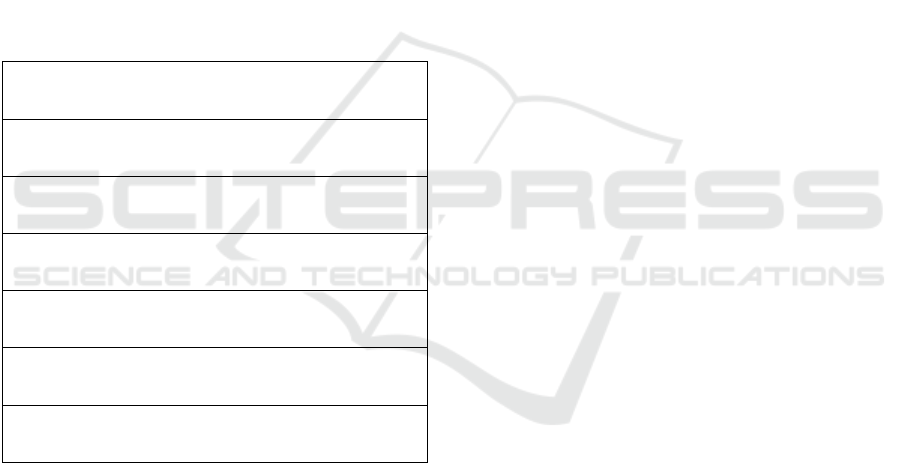
The results are summarized in Table 1, in which are
listed the framework’s titles and their online
information links.
Table 1: Review results.
“Context-aware hybrid reasoning framework for pervasive
healthcare”
(https://link.springer.com/article/10.1007/s00779-013-0696-5)
“Bdcam: Big data for context-aware monitoring-a personalized
knowledge discovery framework for assisted healthcare”
(http://ieeexplore.ieee.org/document/7117389/)
“MediAlly: A provenance-aware remote health monitoring
middleware”
(http://ieeexplore.ieee.org/document/5466985/)
“An integrated multi-sensing framework for pervasive
healthcare monitoring”
(http://ieeexplore.ieee.org/document/5191197/)
“A framework for context-aware home-health monitoring”
(http://www.inderscienceonline.com/doi/abs/10.1504/IJAACS
.2010.030313?journalCode=ijaacs)
“A Middleware Framework for Ambiguous Context Mediation
in Smart Healthcare Application”
(http://ieeexplore.ieee.org/abstract/document/4390866/)
“An Inference System Framework for Personal Sensor Devices
in Mobile Health and Internet of Things Networks”
http://dro.deakin.edu.au/view/DU:30092154)
The following list describes, in more detail, the
analysis of the selected frameworks.
1. “Context-aware hybrid reasoning framework
for pervasive healthcare” (Yuan et al., 2014)
This article main objective is to describe the creation
of a framework to manage the context monitoring of
elderly people on their homes. The inference method
is based on Fuzzy Rules (Wang et al., 1991) and the
system learns by Case Based Reasoning (CBR) (Xu
et al., 1995). The framework uses vital signs data and
infers if the individual has a normal health condition.
2. “Bdcam: Big data for context-aware
monitoring-a personalized knowledge
discovery framework for assisted healthcare”
(Forkan et al., 2015)
This framework is intended to build a system to
monitor a person’s vital signs, inferring the
individual’s current health status from that data. The
system uses the MapReduce Apriori algorithm
(Yahya et al., 2012) that can register the correlations
between distinct variables of the acquired context,
producing a set of rules. It uses data acquired from the
blood pressure and the heart rate.
3. “MediAlly: A provenance-aware remote
health monitoring middleware” (Chowdhury
et al., 2010)
In this framework, the main purpose is to be a
building block of a system based on mobile devices
to monitor the user’s physiological data, which is later
sent to a middleware that infers the user’s health
status by applying a set of rules.
4. “An integrated multi-sensing framework for
pervasive healthcare monitoring” (ElHelw et
al., 2009)
This framework is intended for the implementation of
a system to monitor a person’s vital data as well as
several specific personal activities, e.g., walking,
eating, sleeping, etc. The system uses videos cameras
and wearable devices to collect data. The inference
determines the activity being executed by the person
and is accomplished using Hidden Markov Models
(HMM) (Eddy, 1996).
5. “A framework for context-aware home-health
monitoring” (Esposito et al, 2010)
This article describes the construction of a framework
and a context aware computational system,
implemented in a home-care scenario. The vital data
is collected and used for inference based on a
predefined rule set.
6. “A Middleware Framework for Ambiguous
Context Mediation in Smart Healthcare
Application” (Roy et al., 2007)
In this article it is described the development of a
middleware software system, tailored to deal with the
context ambiguities in health data monitoring. In a
Smart Home scenario it was used wireless sensors
and RFID tags to acquired data, including: location,
activities, and identification of the users. From this
data, inferences are made using Dynamic Bayesian
Networks, with the objective of measuring the
context quality.

7. “An Inference System Framework for
Personal Sensor Devices in Mobile Health and
Internet of Things Networks” (Kang, 2017)
In this thesis the main objective is to create a
framework to monitor vital signs. The framework can
detect and alert when the user’s vital signs have
abnormal readings. The inference is a simple method
based on verification of rules and predefined
thresholds applied to the vital signs data.
5 CONCLUSIONS
Although the health data monitoring subject is widely
spread in the research community, there aren’t many
proposals towards the development and
implementation of health related inference systems
frameworks. There is much more work related to the
acquisition and presentation of vital signs data, which
suggests a gap between the data and the inference and
knowledge production. On that line of reasoning,
knowledge inference is the next logic step to make
sense from all the data.
Comparing the health knowledge inference with
other research areas, (e.g., computer operating
systems, computer vision, statistics analysis, content
management, etc.) for which there are high quality
and freely available frameworks (e.g. linux, android,
java, openCV, R, wordpress, etc), we can’t find
parallel frameworks for health knowledge inference.
That might be because, although there are lots of high
quality research regarding the models and algorithms,
the technology hasn’t mature enough for the arising
of a general software framework.
Unfortunately we did just a review work, but a
deeper analysis, including actual tests would be very
important to verify the quality of the inference
provided by the systems. In a scenario on which the
data acquisition and processing is trivial, it may be the
models and algorithms to determine the quality of a
complete solution.
Reading thought the documentation of the several
frameworks it is clear that to apply some inference
techniques and longitudinal analysis, it is necessary
to have large amounts of data, which might explain
the gap between the available analysis techniques and
their actual usage in actual software frameworks.
ACKNOWLEDGEMENTS
This work was supported by the Project
“NanoSTIMA: Macro-to-Nano Human Sensing:
Towards Integrated Multimodal Health Monitoring
and Analytics/NORTE-01-0145-FEDER-000016"
financed by the North Portugal Regional Operational
Programme (NORTE 2020), under the PORTUGAL
2020 Partnership Agreement, and through the
European Regional Development Fund (ERDF).
REFERENCES
Abu-Hanna, A. and Lucas, P. (2001). Prognostic models in
medicine: AI and statistical approaches. Meth Inform
Med, 40, pp. 1–5
Adabag, A., Grandits, G., Prineas, R., et al. (2008). Relation
of heart rate parameters during exercise test to sudden
death and all-cause mortality in asymptomatic men. Am
J Cardiol; 101: pp. 1437–1443.
Batty, G. Shipley, M., Kivimaki, M., et al. (2010). Walking
pace, leisure time physical activity, and resting heart
rate in relation to disease-specific mortality in London:
40 years follow-up of the original Whitehall study. An
update of our work with professor Jerry N. Morris
(1910–2009). Ann Epidemiol 2010;20:661–9.
Beddhu, S., Nigwekar, S., Ma, X., Greene, T. (2009).
Associations of resting heart rate with insulin
resistance, cardiovascular events and mortality in
chronic kidney disease. Nephrol Dial Transplant.
2009;24(8):2482–8. doi: 10.1093/ndt/gfp057.
pmid:19307229
Bloss, C., Wineinger, N., Peters, M., Boeldt, D., Ariniello,
L., Kim, J., et al. (2016). A prospective randomized trial
examining health care utilization in individuals using
multiple smartphone-enabled biosensors. PeerJ.
2016;4:e1554. doi: 10.7717/peerj.1554.
pmid:26788432
Chowdhury, A., Falchuk B., Misra, A. (2010). MediAlly: A
Provenance-Aware Remote Health Monitoring
Middleware. In Proceedings of Pervasive Computing
and Communications, pp. 124-134, IEEE
Cole, C., Foody, J., Blackstone, E., Lauer, M. (2000). Heart
rate recovery after submaximal exercise testing as a
predictor of mortality in a cardiovascularly healthy
cohort. Annals of internal medicine, 132(7), pp. 552-
555.
Cruz, A. and Wishart, D. (2006). Applications of machine
learning in cancer prediction and prognosis. Cancer
Inform, 2, pp. 59–78
Dressendorfer, R., Wade, E., Scaff Jr, H. (1985). Increased
morning heart rate in runners: a valid sign of
overtraining?. The Physician and Sportsmedicine,
13(8), pp. 77-86.
Eddy, S. (1996). Hidden Markov models, In Current
Opinion in Structural Biology, Volume 6, Issue 3, 1996,
pp. 361-365, ISSN 0959-440X, https://doi.org/10.1016/
S0959-440X(96)80056-X.
ElHelw, M., Mcllwraith, J. et al. (2009) An integrated
multi-sensing framework for pervasive healthcare
monitoring, 3rd Int. Conf. on Pervasive Como.
Technologies for Healthcare, pp. 1-7

Esposito, A., Tarricone, L., Zappatore, M., Catarinucci, L.,
Colella, R. (2010). A framework for context-aware
home-health monitoring. Int. J. of Autonomous and
Adaptive Communications Systems, Vol.3, No.1, pp.75
- 91
Felisberto, F., Laza, R., Fdez-Riverola, F., Pereira, A.
(2015). A distributed multiagent system architecture for
body area networks applied to healthcare
monitoring. BioMed research international, 2015.
Forkan, A., Khalil, I., Ibaida, A., Tari, Z. (2015). BDCaM:
Big Data for Context-aware Monitoring-A Personalized
Knowledge Discovery Framework for Assisted
Healthcare. IEEE transactions on cloud computing,
2015. Retrieved from: http://ieeexplore.ieee.org/
document/7117389/
Gerven, M. (2007) Bayesian networks for clinical decision
support. Radboud University Nijmegen, Nijmegen, the
Netherlands
Hedelin., R., Kenttä, G., Wiklund, U., Bjerle, P.,
Henriksson-Larsén, K. (2000). Short-term overtraining:
effects on performance, circulatory responses, and heart
rate variability. Medicine and science in sports and
exercise, 32(8), pp 1480-1484.
Hozawa, A., Ohkubo, T., Kikuya, M., et al. (2004).
Prognostic value of home heart rate for cardiovascular
mortality in the general population: the Ohasama study.
Am J Hypertens; 17: pp. 1005–1010.
Jansen, R., Yu, H., Greenbaum, D., Kluger, Y., Krogan, N.
J., Chung, S., ... & Gerstein, M. (2003). A Bayesian
networks approach for predicting protein-protein
interactions from genomic data. Science, 302(5644),
pp. 449-453.
Javorka, M., Zila, I., Balharek, T., Javorka, K. (2002). Heart
rate recovery after exercise: relations to heart rate
variability and complexity. Braz J Med Biol Res.;35(8),
pp. 991–1000.
Johansen, C., Olsen, R., Pedersen, L., et al. (2013). Resting,
night-time, and 24 h heart rate as markers of
cardiovascular risk in middle-aged and elderly men and
women with no apparent heart disease. Eur Heart J
2013;34: pp. 1732–1739
Kado, D., Lui, L., Cummings, S. (2002). Rapid resting heart
rate: a simple and powerful predictor of osteoporotic
fractures and mortality in older women. J Am Geriatr
Soc 50: pp. 455–460.
Kang, J. (2017). An inference system framework for
personal sensor devices in mobile health and internet of
things networks, PhD thesis, School of Information
Technology, Deakin University. Retrieved from:
http://dro.deakin.edu.au/view/DU:30092154
Klein, A. (2017). Smartwatches know you’re getting a cold
days before you feel ill. New Scientist. Retrieved from:
https://www.newscientist.com/article/2117854-
smartwatches-know-youre-getting-a-cold-days-before-
you-feel-ill/
Knaus, K., Wagner, D., Draper, E., Zimmerman, J.,
Bergner M. and Bastos, P. (1991). The APACHE III
prognostic system. Risk prediction of hospital mortality
for critically ill hospitalised adults. Chest, 100, pp.
1619–1636
Legeai, C., Jouven, X., Tafflet, M., et al. (2011). Resting
heart rate, mortality and future coronary heart disease
in the elderly: the 3C Study. Eur J Cardiovasc Prev
Rehabil;18: pp 488–97.
Leistner, M., Klotsche, J., Palm, S., Pieper, L., Stalla, G. K.,
Lehnert, H., ... & Zeiher, A. M. (2012). Resting heart
rate as a tool for risk stratification in primary care: does
it provide incremental prognostic information?.
European journal of preventive cardiology, 19(2), pp.
275-284.
Li, X., Dunn, J., Salins, D., Zhou, G., Zhou, W., et al.
(2017) Digital Health: Tracking Physiomes and
Activity Using Wearable Biosensors Reveals Useful
Health-Related Information. PLOS Biology 15(1):
e2001402. doi: 10.1371/journal.pbio.2001402
Link, M., Estes, M. (2012) Sudden cardiac death in the
athlete: bridging the gaps between evidence, policy, and
practice. Circulation 125: pp.2511–2516.
Lucas, P. (1995). Logic engineering in medicine. Knowl
Eng Rev, 10 (2), pp. 153–179
Makivić, B., Nikić, M., Willis, M. (2013). Heart rate
variability (HRV) as a tool for diagnostic and
monitoring performance in sport and physical activities.
Journal of Exercise Physiology, vol. 16, pp.103-131
Marcelino, I., Pereira, A. (2009, September). Elder care
modular solution. In Advances in Human-oriented and
Personalized Mechanisms, Technologies, and Services,
2009. CENTRIC'09. Second International Conference
on (pp. 1-6). IEEE.
Murphy, K. (2002). Dynamic Bayesian networks. UC
Berkeley, Berkeley, CA
Nakayama, T., Ohnuki, Y., Niwa, K. (1977). Fall in skin
temperature during exercise. Jpn J Physiol.;27(4), pp.
423–37. pmid:599738
Ohno-Machado, L. (1997). A comparison of Cox
proportional hazards and artificial neural network
models for medical prognosis. Comput Biol Med, 27,
pp. 55–65
Paulino, D., Reis, A., Barroso, J., Paredes, H. (2017).
Mobile devices to monitor physical activity and health
data. 12th Iberian Conference on Information Systems
and Technologies (CISTI); 06/2017,
DOI:10.23919/CISTI.2017.7975771
Pearl, J. (2000). Causality: models, reasoning and
inference. Cambridge University Press, New York, NY
Reis A., Barroso, I., Monteiro, M., Khanal, S., Rodrigues,
V., Filipe, V., Paredes, H., Barroso, J. (2017a).
Designing Autonomous Systems Interactions with
Elderly People. Universal Access in Human–Computer
Interaction. Human and Technological Environments,
01/2017: pp. 603-611; ISBN: 978-3-319-58699-1,
DOI:10.1007/978-3-319-58700-4_49
Reis, A., Lains, J., Paredes, H., Filipe, V., Abrantes, C.,
Ferreira, F., Mendes, R., Amorim, P., Barroso, J.
(2016a). Developing a System for Post-Stroke
Rehabilitation: An Exergames Approach. Universal
Access in Human-Computer Interaction. Users and
Context Diversity, 1st edited by Margherita Antona,
Constantine Stephanidis, 07/2016: pp. 403-413;

Springer International Publishing., ISBN: 978-3-319-
40237-6, DOI:10.1007/978-3-319-40238-3_39
Reis, A., Morgado, L., Tavares, F., Guedes, M., Reis, C.,
Borges, J., Gonçalves, R., Cruz, J. (2016b). Gestão de
listas de espera para cirurgia na rede hospitalar pública
portuguesa - O sistema de informação dos programas
de recuperação de listas de espera. CISTI 2016, 11.ª
Conferência Ibérica de Sistemas e Tecnologias de
Informação; 06/2016, DOI:10.1109/CISTI.2016.
7521612
Reis, A., Paulino, D., Paredes, H., Barroso, J. (2017b).
Using Intelligent Personal Assistants to Strengthen the
Elderlies’ Social Bonds. Universal Access in Human–
Computer Interaction. Human and Technological
Environments, 01/2017: pp. 593-602; ISBN: 978-3-
319-58699-1, DOI:10.1007/978-3-319-58700-4_48
Robillard, M., DeLine, R. (2012). A field study of API
learning obstacles. Empirical Software Engineering
(EMSE), 16, pp.703-732.
Roy, N., Pallapa, G., Das, S. (2007). A Middleware
Framework for Ambiguous Context Mediation in Smart
Healthcare Application, Proc. IEEE Int'l Conf. Wireless
and Mobile Computing Networking and Comm.
(WiMob '07).
Savonen, K., Lakka, T., Laukkanen, J., et al. (2006). Heart
rate response during exercise test and cardiovascular
mortality in middle-aged men. Eur Heart J
2006;27:582–8.
Snyder, M. (2017). Michael Snyder, STANFORD W.
ASCHERMAN, MD, FACS, PROFESSOR IN
GENETICS. Retrieved from https://med.stanford.edu/
profiles/michael-snyder?tab=bio
Sonnenberg, F. and Beck, J. (1993). Markov models in
medical decision making: a practical guide. Med Decis
Making, 13 , pp. 322–338
Wang, J., Mendel, M. (1991). Generating fuzzy rules by
learning from examples. Proc. 6th Int. Symp. Intelligent
Control, pp. 263-268.
Xu, L. (1995). Case-based reasoning: A major paradigm of
artificial intelligence. IEEE Potentials, vol. Dec 1994-
Jan 1995, pp. 10-13.
Yahya, O., Hegazy, O., Ezat, E. (2012). An Efficient
Implementation of Apriori Algorithm Based on
Hadoop-Mapreduce Model, Proc. of the International
Journal of Reviews in Computing 31st December 2012.
Vol. 12: pp. 59-67.
Yuan, B., Herbert, J. (2014). Context-aware hybrid
reasoning framework for pervasive healthcare. Pers
Ubiquit Comput 18: pp. 865–881. Retrieved from:
https://link.springer.com/article/10.1007/s00779-013-
0696-5
Zhang, D., Shen, X., Qi, X. (2016) Resting heart rate and
all-cause and cardiovascular mortality in the general
population: a meta-analysis. CMAJ: Canadian Medical
Association journal. 88(3), pp.53–63. doi:
10.1503/cmaj.150535. pmid:26598376
