
Autonomous Vehicles for Independent Living of Older Adults
Insights and Directions for a Cross-European Qualitative Study
Shane McLoughlin
1
, David Prendergast
2
and Brian Donnellan
1
1
LERO, School of Business, National University of Ireland Maynooth, Maynooth, Ireland
2
Intel Labs Europe, Intel Corp, Leixlip, Ireland
Keywords: Older Adults, Autonomous Vehicles, Driverless Cars, 65+, IT Adoption, User Experience, Business Models.
Abstract: Autonomous Vehicles (AV) are expected to have a revolutionary impact on future Society, forming an integral
component of future Smart Cities & regions. ‘Impacts’ range from changes in mobility, environment,
planning, infrastructure, employment, leisure time to disruptive business models etc. Designing user centred
mobility experiences for citizens ensuring trust, adoption and enhanced experience of emerging AV systems,
products and services is an important emerging research challenge today. It is projected that ‘older adults’
(65+) will encompass approximately one third of the mobility marketplace by 2060, with the broader ‘Silver
Economy’ set to provide enormous potential for new forms of product/services and related business models.
AV’s have the potential to prolong independent living of ‘older adults’ (OA) thus enhancing overall quality
of life. For example, driving cessation and mobility barriers correlate with poorer health outcomes. Ensuring
future AV adoption requires designing mobility experiences addressing the differing life contexts (i.e. health,
financial, mobility needs etc.) of OA. This paper presents context, motivation and initial findings from a
qualitative pilot study of Irish Older adults that informs the design of a cross-European study to support
‘Independent Living of Older adults’ in a future AV marketplace that encompasses new Mobility As A Service
offerings.
1 INTRODUCTION
Autonomous vehicle technologies are expected to
lead to a disruptive and eventually transformative
change on mobility in society over the next 30 years,
allowing humans to move away from manual control
of vehicles to supervisory control and eventually no
control. This transformation is anticipated to include;
a reduction in transport related accidents, a freeing up
of driving time for other in-vehicle pursuits, changes
to traffic congestion and road infrastructure, new
business models of vehicle ownership/mobility,
evolving insurance models, changes to vehicle
driving licencing, new modes for delivery of goods
and services, new mobility opportunities for the
disadvantaged and disruptive changes to the
workforce. In essence, the transformative change on
mobility will have a larger lasting transformative
change on society overall, with humans mental
models of the car and mobility shifting in the coming
years and AV systems and services envisaged as
forming a core component of ‘Smart Cities’ and
‘Smart Regions’ of the future. The key research
challenge will be ensuring that AV technology will
ultimately have positive consequences for the human
condition overall, i.e. improving quality of life for all
citizens. Thus, creating ‘inclusive’ or ‘human’ ‘Smart
City’ and regions requires integrating AV systems
and services which consider differing and complex
citizen needs and preferences.
One segment of the human population seen as
potentially benefiting the most from AV technologies
are older adults. In this respect, older drivers are said
to represent ‘an innovation paradox when purchasing
vehicles’ (Yang & Coughlin 2014). New advanced
vehicle technologies first become available in
relatively expensive vehicles whereby it is often older
adults who have the resources to purchase them.
Thus, older drivers can be seen as a critical test
market for new automotive technologies. However,
whilst older and disabled people are portrayed as lead
use case for the development of the partial and fully
autonomous vehicles, OA are seldom early adopters
of new technology and are the market segment most
sceptical about dependability and surrendering
control to a full autonomous system. For example, a
294
McLoughlin, S., Prendergast, D. and Donnellan, B.
Autonomous Vehicles for Independent Living of Older Adults.
DOI: 10.5220/0006777402940303
In Proceedings of the 7th International Conference on Smart Cities and Green ICT Systems (SMARTGREENS 2018), pages 294-303
ISBN: 978-989-758-292-9
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

recent MIT related online survey of US adults (N =
2094) found older adults have the lowest propensity
to adopt fully autonomous vehicles (Abraham et al.
2016). Importantly, the number of fatalities per
million miles travelled increases the older we get
(IIHS 2016). There is a proven close correlation
between Driving Cessation and poorer health
outcomes, and the risks of clinical depression doubles
once an older adult surrenders their driving licence
(Chihuri et al. 2016). In Europe, EU-28 will see a
doubling of those aged 80+ from contemporary levels
of 5.3% to 10.9% by 2050 (Eurostat 2015).
Cumulatively, it is projected that ‘older adults’ (65+)
will encompass approx. 1/3 of the mobility
marketplace by 2060 (Harbers & Achterberg 2012).
In sum, given the unique health, behaviours and
technological ability of OA etc., “the successful
design, implementation, and marketing of these
technologies will require special consideration of the
unique needs, attitudes, and capabilities of older
drivers” (Eby et al. 2015). How can we build trust and
encourage older people to become lead users of AV?
This paper presents initial findings from an
exploratory pilot study on suburban and rural ‘Older
Adults’ in Ireland, to inform the research direction
and design of a cross-European qualitative study on
‘Older adults’. The initial guiding research question
is as follows: How can AV systems and services
support independent living of Older Adults in the
advancing Silver economy? The paper is structured as
follows: We begin by presenting the context and
motivation for this study based on a scoping review
of the literature. Next, we present our method chosen
followed by the findings section overviewing our
participant’s unique contexts and presentation of
thematic areas and themes emerging from analysis.
We then discuss findings according to the five
interrelated work streams identified and conclude by
highlight relevance of findings to existing prominent
technology adoption models as well as outlining the
next steps in the research project.
2 CONTEXT & MOTIVATION
According to Strategy Analytics, Level 4 high
automation will grow to 42% by mid Century
(Strategy Analytics 2017). L1-3 systems offer
opportunities prolong driving and L4 & 5 systems
may help promote and lower the costs of independent
living and solve many of the mobility and social
loneliness issues associated with ageing. From a
market perspective, the ‘silver economy’ is set to
grow rapidly. Europeans over 65 already have a
spending capacity of over €3 Trillion and the number
of citizens with age related impairments will reach 84
million by 2020 (Iakovidis 2015). The needs and
spending power of this market segment will greatly
expand as Europe moves from 4 working age people
per older adult to 2 by 2060 (Eurostat 2015).
Existing evidence on the unique mobility
challenges of older adults encompasses key factors
such as location, living arrangements, health
characteristics, Tech Literacy and gender etc. AV
systems present unique opportunities to address each
of these factors thereby improving QoL for older
adults (by increasing active and independent living),
as well as unique challenges in designing AV
mobility systems and mobility services that cater for
OA particular needs.
In Europe 29% of ‘older adults’ live alone, with
higher proportions of OA living in rural and isolated
areas and a higher proportion of OA living alone in
urban areas (Holley-moore & Creighton 2015). This
is despite the reality that sufficient public transport
offerings are lacking in rural compared to urban areas
(Holley-moore & Creighton 2015). For example, in
the USA, older adults’ reliance on automobility
increases with age in part due to ‘last mile’ mobility
deficits and ‘arm to arm’ care requirements. In
Ireland, rural public transport options have declined
due to reduced population density in rural regions
caused by out-migration of younger adults to urban
areas. This is despite the reality that in Ireland alone
38% of the population are classed as ‘rural’ according
to the most recent national census (Connolly et al.
2011). Furthermore, half of the world’s population
reside in rural areas (Westlund & Kobayashi 2013)
and this is similarly the case in Europe (EU, 2015).
Older adults have unique health characteristics
compared to younger age cohorts resulting in
differing driving patterns and behaviours, the
reduction and cessation of driving, and the ability to
access and utilise adequate transport options. Studies
show OA’s in general have slower reaction times,
decreased flexibility and co-ordination with
significant reductions in strength and muscle mass
(Eby et al., 2015). Collectively, these characteristics
mean OA’s tend to have difficulty entering and
exiting vehicles, difficulty driving for prolonged
periods and engaging in certain driving behaviours.
Furthermore, as age increases so too does; the
proportion of adults with physical and cognitive
disabilities the proportion of adults with multiple
disabilities and the proportion of adults with health
conditions requiring hospital & doctor visits and
medications. In the US, 39% of those aged 65+ suffer
with one or more disabilities ranging from, Hearing,
Autonomous Vehicles for Independent Living of Older Adults
295

Vision, Cognitive, Ambulatory to the ability to self-
care and live independently (Wan, He; Larsen 2014)
whilst 44% of 65+ Europeans report one or more
disabilities, reaching 60% for those aged 75+ . In this
respect, declines in health characteristics are a leading
cause of driver cessation, despite a well-documented
association between driving cessation and declines in
well-being and other important health measures
(Chihuri et al. 2016). Aside from the vicious cycle of
health and driving cessation outcomes, health as a
differentiator of OA from younger cohorts leads to
unique challenges in designing AV product services
that can be adopted by OA, and designed with OA
needs in mind. The higher prevalence of disabilities
presents challenges of ‘door to door’ or ‘arm to arm’
assistance, as well as the design of in-vehicle systems
that cater for OA needs where one or more disabilities
are present etc.
Research has found that the majority of trips taken
by OA are for shopping, family visits, recreation,
social engagements as well as medical related
journeys (Duncan et al. 2015), with discretionary
travel most limited by circumstances of aging.
Currently health and other factors means OA driving
behaviours and patterns tend to differ to younger
adults. OA tend to self-regulate their driving, avoid
travelling at busy times, alter their travel routes and
decrease their journey times (Shergold et al. 2015).
Thus, OA mobility is constrained even for those who
still drive.
Furthermore, access & use of in-vehicle
technologies differ to younger users. Older adults are
more likely to have difficulty using advanced in-
vehicle systems, taking longer to learn these systems,
and to misunderstand in-vehicle technologies purpose
and full capabilities (Eby et al. 2015; Shaw et al.
2010). Some studies suggest older adults do show
willingness to adopt some ADAS systems (Souders &
Charness 2016). Although older adults may not be
adverse to learning new technology granted they are
informed of their benefit (Yang & Coughlin 2014) it
is well established that learning new skills and
changing routines is more difficult (Craik et al. 1996).
Older adults also tend to have less technological
ability and understanding of features. Furthermore,
some studies have suggested older adults learn to use
these systems differently, relying more on vehicle
manuals, car-salesmen and less on trial-and-error to
younger drivers (Eby et al., 2015; Shaw et al., 2010).
Finally, gender has arisen as a significant variable
in the literature with women more likely to expect to
cease driving due to aging and men with Mild
Cognitive Impairment less likely to cease driving than
women. Prior research also suggest ‘Trust’ towards
technology differ by OA gender, with females more
wary of technological advancements (Shergold et al.
2015).
Given the insights presented above, surprisingly
little research on the potential for adoption of assisted
and autonomous vehicles and AV design
requirements has occurred for this important
demographic. Recent studies have identified a gap in
our understanding of Older Adults and the design of
future AV systems including In-vehicle Communica-
tion Systems (IVCS) and In-Vehicle Human
Computer Interface (IVHCI). For example, according
to Young et al
(2017)
, a comprehensive review of
automotive HMI design guidelines (from 2000 to
2015) revealed guidelines do not address design
issues related to older driver impairments .
Thus, the aim of this project will be to contribute
to this knowledge gap and deliver ethnographic, User
Experience and market insights about how the needs
and behaviours of drivers in different geographies
change through the later life course and how best AV
systems and services can cater for this important
demographic.
3 METHOD
A qualitative research approach was chosen to
explore the main research question. Qualitative
methods can be particularly valuable in such cases
where a research topic is new and little understood, as
is the case with ‘Older adults’ and ‘AV’.
Furthermore, qualitative methods better ensure
capturing the rich context of a phenomena, by using
techniques designed to allow participants freedom to
impart experience and evidence in their own words,
language, circumstances and surrounding context.
This allows for unforeseen themes and insights to be
generated not possible in positivist studies. For
example, the initial scoping review found disabilities
amongst older adults and health issues pose
significant challenges for driving and mobility. The
pilot stage allows us to understand health and
disabilities in greater detail such as how it affects
respondents’ current mobility scenarios.
The method chosen for this initial stage of the
study was the ‘open ended in-depth interview’ to
explore the context of older adults in relation to
current and future mobility requirements and their
surrounding life context. An interview schedule was
designed to generate themes surrounding such aspects
as lifestyle, health, mobility needs and mobility
experience etc. Theories of technology adoption were
reviewed (i.e. UTAUT
2 and TAM3 (Venkatesh &
SMARTGREENS 2018 - 7th International Conference on Smart Cities and Green ICT Systems
296

Bala 2008; Venkatesh et al. 2016)) and questions
reflected core concepts including Habit, Hedonic
Motivation and External Variables etc. (Ghazizadeh
et al. 2012). The pilot stage serves the purpose of
generating insights and themes to inform the design
of the main study and its objectives. Pilot Interview
questions were designed to explore the thematic
areas: a. Participant Profile and Lifestyle b. Driving
status & history c. Driving/Passenger experience d.
Public Transport/ride-sharing e. Health & Aging f.
Technology g. Vehicle technology. Examples of
questions included; a) “If you have ceased or reduced
driving, could you tell me about the circumstances
and/or decisions that led to stopping/reducing
driving?” b) “Can you talk about a recent experience
as a passenger, and how it felt?.” C. “What is the
most pleasurable thing about driving?”
Interview question responses were aided with
additional prompts to ensure consistency amongst
respondents. The ‘critical incident technique’ was
employed to aid recall and encourage story telling.
Recruitment of participants was through third party
community organisations, and interviews took place
in rural and suburban environments in September
2016. Ten older adults were recruited for the pilot
study based on availability and variation, whereby
variation in participants included; age, gender,
marital status, location, driving status, disability,
living arrangements etc. Interviews typically lasted
from 1 ¼ to 1 ½ hours, and were subsequently
transcribed and inductively thematically analysed
using MaxQDA software. The pilot captured data
according to four categories 1) active drivers 2) self-
limiting drivers 3) older adults who have ceased
driving, and 4) older people who have never driven.
The sample ages ranged between 68 and 91 (M =
78) with 6 males and 4 females. There were 7 married,
2 widows and 1 widower. 5 participants resided in
rural areas whilst 5 resided in a suburban town or
village. 2 of the respondents lived alone, with 8 of the
respondents having one or more disabilities covering
visual, cognitive, hearing, speech, ambulatory, self-
care and independent living etc. Three of the
respondents currently drive, whilst 3 reported driving
reduction, 2 had ceased driving and 2 had never
driven on public roads.
4 FINDINGS
We begin by providing a brief profile of each
participant to sensitise the unique contexts of OAs’,
followed by presentation of initial thematic areas and
themes emerging from pilots conducted. An ‘audit
trail’ is provided for transparency by presenting some
examples of participant responses corresponding to
themes generated.
4.1 Profiles
Pauric is a former school teacher and lives alone in a
rural bungalow. He is a widower with two children.
He has regular contact with his children and
grandchildren as well as his brother who he holidays
with. Pauric likes driving, and drives a recent (2016)
vehicle with the latest ADAS features. Living in a
rural area, Pauric relies heavily on his car. The nearest
train and bus stations are not accessible by walking.
Pauric has hearing difficulties and lower back
problems for which he uses a ‘back roll’ in the driver
seat for relief.
James is a retired bus/lorry driver living in a
suburban area. James has three daughters whom he
regularly drives for. He lives with his wife and ‘likes
to keep busy’ which includes driving for his family
and a ‘meals on wheels’ scheme. James likes driving
and describes it as a, ‘hobby in a way’. He drives a
2008 saloon diesel car. James endures a studder and
some back problems.
Peter is also a retired bus/lorry driver living in a
suburban area. He lives with his wife and recently
divorced son. Peter often drives his wife as well as
sometimes driving his sister who has MS. Peter drives
a 2011 small size 1l petrol car. He has become less
active overall due to health episodes up until last year.
Tommy is a retired airport worker and is married
with his second wife. He has 8 children and 23
grandchildren. Tommy lives in a rural area, and has
reduced his driving to occasional short journeys. He
is losing his eyesight in his left eye, and his hearing is
poor. He lost his hearing aids and struggles with the
1000 euro cost of getting new ones. Tommy drives a
small 2014 petrol car. Most of Tommy’s transport is
via his children, the community (Third Age) bus
scheme, and occasionally his wife. The nearest public
transport is 2 miles away in the nearest town.
Orla lives with her husband in a suburban semi-
detached house, along with her son. Orla developed
Parkinson’s disease and has reduced driving as a
result. She hides her illness in the community as is
afraid of ‘stigma’. Orla finds reversing difficult as her
‘neck is not great’. She notices her husband’s
concentration is not as good as it used to be on the
road. Orla relies on her husband and public transport
for most of her mobility.
Cara is a farmer in rural Ireland. She lives with her
husband and daughter and has 6 children. Cara is
afraid of driving on public roads. Her ‘nervousness’
Autonomous Vehicles for Independent Living of Older Adults
297

about driving has increased as she has aged. She relies
on her children and taxi’s for transport, as her
husband stopped driving 2 years ago. As she lives
over 10km from the nearest town, taxis are expensive.
She describes herself as a passenger driver,
particularly as a result of monitoring her husband
driving as his health failed. Cara is in good health.
Gene has 3 children and lives with her son in a
rural area. She is widowed, and was previously a
nurse. Gene had done all the driving due to her
husband having an accident in the late 80s. He died
approx. 5 years ago. She had to give up driving due
to deteriorating health, and greatly misses driving, as
she is isolated as a result. Gene suffers with
Glaucoma. She also experiences arthritis, resulting in
tactile issues. She requires frequent toilet breaks due
to incontinence. She relies on a combination of her
son, taxis and the goodwill of others for lifts.
Nora lives in a private nursing home because of
significant health issues. Nora is wheelchair bound
after suffering a series of health events including
kidney problems that left her on dialysis for a period.
She has 3 children, one who lives in Ireland as a taxi
driver. Nora has never driven due to nervousness, and
eventually poor health. She is widowed, and
experiences money problems, as her available income
is spent on nursing home arrangements. She relies on
her son for transport. She also suffers agoraphobia
and arthritis and has tactile issues with her hands.
Nora feels isolated and spends her days in the
smoking room on her own in the nursing home.
Sam gave up driving two years ago due to
deteriorating health. He drove all his life for his job
as he ran his own ‘Plant Hire’ business. He lives at
home in a rural area with his wife and daughter and
relies on his children and taxi’s for transport. Sam still
feels he can drive, and is aggrieved that his doctor did
not sign off on a renewal of his driving licence. Sam
has arthritis in his arms, legs and neck. He is on a lot
of medication that leaves him confused and
disoriented at times. He suffers poor hearing and
vision, and his verbal speech is poor at times. Sam
experiences some memory problems and requires
frequent bathroom breaks. He requires help putting
on in seat belt. His travel is reduced to essential travel
only (e.g. medical appointments) due to availability
of his children and costs of taxis.
Cathal is a retired police officer and lives in a
suburban area with his wife. He has drastically
reduced his driving due to a cancer diagnosis five
years ago. He relies on his wife and public transport
for mobility needs. They have a 2004 hatchback
model. Cathal does not miss driving because he is no
longer comfortable doing so. His main health issues
now is lingering cancer in the urinary area. He has a
uretic catheter bag attached for urine. Con says he can
read without glasses but used to have glasses for
driving.
4.2 Themes
4.2.1 Mobility and Family
The older adults we spoke to in most cases had an
interdependent relationship with their family when it
came to mobility. Thus, mobility was an important
space and rationale for social interaction with family
from spouses, siblings, children, to grandchildren.
Whereas most participants who reduced/creased
driving or had never drove were reliant on their
children for transport needs, those who drove were
often called upon by siblings, or children to drive. For
example, John has a daughter with sight difficulties
so he ‘has to drive her around here and there' as well
as the grandchildren. This resulted in OA having a
needed ‘role’ or ‘purpose’ in the family for those who
drove, whereby for those who did not drive the car
was a space for social interaction with their family.
4.2.2 Health & Aging
Through the course of the interviews, participants
talked about their health, from difficulties and
disabilities to short and long term medical conditions.
Responses were elicited on a range of physical and
cognitive disabilities that older adults experienced
ranging from ‘eyesight’, ‘speech’, ‘cognitive’,
‘fragility’, ‘tactility’, ‘Incontinence’, ‘hearing’,
‘ambulatory’ and ‘medication’ etc. For example, Sam
spoke about a number of medications he is on which
affected his lucidity, memory and concentration
depending on the time of day or other factors. Orla,
Nora and Gene lives with arthritis that affected their
mobility and tactility. Gene and Tommy had severe
sight difficulties affecting their mobility and
awareness. Sam and James had speech problems
inhibiting communication. Several respondents also
had hearing difficulty. For example, according to
Pauric, ‘it is a bit of a burden, people in the back
assume I can hear what they are saying but I don't…
looking at people makes it easier’. For some, health
issues affected where they needed to sit in the vehicle
i.e. ‘seat preference’. As such, according to Nora, ‘I
like to a front seat passenger, I can't sit in the back
because of travel sickness, even short journeys',
whilst Gene responded that, ‘'it always has to be the
front seat if I can because you have more space for
my legs underneath’.
SMARTGREENS 2018 - 7th International Conference on Smart Cities and Green ICT Systems
298

4.2.3 Impact of Not/Reduced/Ceased
Driving
Whereas almost all the suburban respondents we
interviewed referred to at least some availability of
public transport alternatives, as well as community
organisation alternatives (e.g. Third Age Foundation
minibus), rural participants mobility was impacted
the most whereby public transport options were
limited to taxi services with associated costs
involved. For example; Cara remarked, ‘There are
places I want to go that I can’t go and I have to leave
it for another week and another week and so delayed
circumstances getting things done.., I can’t go when I
want to go when I decide I’m going’ (Cara), whilst
Gene said‘it impedes people not only me and confines
them to their homes and increases mental distress’
(Gene)
4.2.4 Technology
Only half of the respondents used the internet. Non-
users cited, ‘a lack of interest’, lack of ‘digital
literacy’, ‘cognitive impairments’ such as memory
problems, ‘eyesight’, and ‘tactility’ issues due to
arthritis. Whilst 4 of the respondents had a
smartphone, just two used the internet on their
smartphone. As several of the respondents suffered
arthritis, this caused tactile problems that became a
barrier for some in using even basic features of a
phone. For example, according to Gene, 'The buttons
are bigger, and if I get a text message… I keep having
to press it to get the text message, I wouldn't be able
to text back… with my fingers’
4.2.5 Changed Driving Behaviours
Changed driving behaviour themes which emerged
were increased ‘tiredness’, ‘cautiousness’,
‘concentration’ and ‘distraction’, as well as reduced
‘speed’ and tolerance for ‘motorway’. For example,
Pauric’s response echoed the sentiment of several
participants we spoke to; ‘I seen my daughter and my
son there and I'd say you are going too fast but they
probably aren't, so more caution would be one thing,
you have to keep alert and watch more because you
can lose your focus '. Such themes highlighted aging
and driving experience results in differing
perceptions and attitudes towards driving by OA.
Furthermore, the need to stick to ‘familiar roads’,
avoid ‘night time’ driving and certain ‘times of the
day’ also emerged confirming findings from prior
studies (Shergold et al. 2015).
4.2.6 Pleasant Journey
Several questions were posed to elicit what
participants consider a good driving/passenger
experience. We posed the questions, ‘What is the
most pleasurable and frustrating thing on a journey’,
‘What makes you more nervous and less nervous as a
driver/passenger’ and ‘Can you describe what you
consider an ideal or pleasant experience driving?’
The most frequent responses for a pleasant or
pleasurable drive were ‘good road conditions’,
‘music’, ‘Scenery’, ‘breaks on long journeys’, the
‘destination’ and ‘good drivers’ (which for one
participant meant, ‘decisive drivers’).
In terms of what makes respondents ‘frustrated’
or ‘more nervous’ on journeys, the most common
responses referred to ‘perceived speed’, the driving
behaviour of ‘other road users’ and ‘bad traffic’.
Some responses referred to ‘perceived speed’ in terms
of driving too slow and not being ‘assertive’ on the
road. For example, according to Gene, ‘I don't like
somebody driving too slow, that annoys me because I
didn't drive like that’. For other respondents what
makes them frustrated or nervous was driving too
fast, such as for Nora, ‘to me if they are going fast
they are going fast, I don't look at the speedometer I
just say [person] you are going too fast’. What
emerged from respondent interviews was the
perception of speed had changed for several of the
respondents. What they considered fast when they
were younger had changed as they aged. For example,
according to Cathal, ‘as you get older you don't have
the same, the speed of the other car is the speed that
confuses most I think'.
In terms of ‘other road users’, whilst some
responses referred to obeying the rules of driving
such as obeying road signs and correctly using
roundabouts, other responses referred to what they
considered good driving etiquette or conscientious-
ness of other road users. For Cara, this meant not
‘hogging the roads, and not making any effort to
move in and let other passengers by for miles and
miles, that’s frustrating’. Gene remarked, ‘people
who blow horns behind you, that annoys me', whilst
James referred to drivers weaving between lanes,
where ‘common courtesy doesn't exist'. Overall,
respondents reported that as passengers, what made
them less nervous was the ‘assertiveness’, the
‘steadiness’, the ‘awareness’ and the ‘patience’ of the
driver. Examples of the aforementioned themes are as
follows:“when the person who is driving is confident
when he goes to move” (Cathal) “I like a steady
driver with no jerks” (Pauric) “To drive easy and not
to push.” (James) Over the course of the interview, it
Autonomous Vehicles for Independent Living of Older Adults
299

should be noted that many of the respondents had
strong views on driving etiquette and the driving
behaviour of other road users.
4.2.7 Passenger Activities
As passengers, the most significant themes to emerge
were in terms of observing ‘scenery’, ‘having
conversation’ and ‘watching the road’. Cara likes to
look at the scenery, houses, landscape whilst
travelling. She is interested in understanding who is
living where, what land is being used for, and things
she has not spotted before. She will also talk on the
journey and make conversation. Whilst Pat likes to
'see what happens along the line, what changes are
being made as you go along, when you driving a car
you never get that view... I like that' (Pat). The
participants we spoke to (both when referring to
private vehicles and public transport (like buses and
trains)) in almost all cases emphasised the activity of
observing and looking around on journeys as well as
conversation, rather than activities such as reading,
browsing etc. For example, according to John when
referring to public transport, 'there is no such thing as
conversation anymore because everyone has their
earpieces in or are texting’. Instead, several of the
participants placed emphasis on observing changes to
the landscape and buildings, and recalling and
associating memories to places they observed.
4.2.8 Passenger Drivers
In terms of ‘watching the road’, most of the
participants we spoke to could be considered
‘passenger drivers’. For example, James noted, 'I am a
driver all the time' even though he is only a passenger,
‘I take note of what people are doing, isn't that what
you do!', Gene believes, 'as a passenger you have a
different perception of things than a driver', whilst Orla
remarked, ‘Nowadays I don’t sleep, I just keep my eye
on the driver’. When asked to talk, ‘about your
experience being a passenger in a car transport?’,
respondents referred to the ‘deteriorating health’ or
‘concentration’ of their spouse, their own ‘prior driving
experience/history’, and the need for a ‘sense of
control’ in reasoning why they watch the road and alert
the drivers to potential dangers/hazards. In terms of
‘sense of control’, several passengers engage in
‘passenger driving’ to relieve anxiety and maintain a
sense of control of their safety and the driver.
4.2.9 Public Transport and Ridesharing
Participants’ motivation to use public transport like
buses and trains referred to ‘convenience’, ‘Traffic’,
‘Cost’, ‘Parking’ and ‘lack of alternatives’. In terms
of ‘Parking’ and ‘Cost’, examples include, ‘the car is
a liability in town, you have to find parking and pay
for parking, sometimes very highly'. Convenience
was cited for some in terms of close and frequent
availability of options, for example, ‘we are lucky
enough here…there are eight buses leaving every day
and eight buses back' (Cathal). ‘Traffic’ was cited by
several participants for those who still drove, in terms
of the ‘the flow of traffic and busy streets’ in the city.
Finally, some participants referred to ‘lack of
alternatives’ such as for Cara who took a taxi to catch
a train into the city when her sons and daughters
weren’t available. In terms of taxi’s and taxi ride-
sharing, most participants showed reluctance or
avoidance citing, ‘trust’, ‘cost’, ‘Lack of need’ or
‘lack of alternatives’. In terms of ‘trust’, whilst some
showed an aversion to taxi’s altogether such as for
James, ‘I've heard from alot of people over the years
that a taxi man will bring you around and go the long
way' (James), others referred to their use in short city
trips only; 'I wouldn't get in to it for a long journey…
I would be very wary of taking a taxi out from Dublin
to where I live with a stranger, I would not be
comfortable enough… I wouldn't even be aware if
they are on drugs or not.' (Gene). Whilst Cara and
Orla limited taxis mainly to drivers they knew. For
example, Orla replied she would feel uncomfortable
getting into a taxi with a male driver who she does not
know. Reluctance was also shown for taxi ridesharing
in terms of lack of ‘trust’ in sharing with strangers.
According to Tommy, ‘there’s always a maniac who
wants to put his hand in your pocket’. Finally, some
participants cited a ‘lack of need’ due to alternative
transport options, whilst the ‘cost’ of taxis was raised
for some living in rural areas.
5 DISCUSSION
Initial analysis of pilot data led to 5 proposed
interrelated work streams. (1) Impact of AV's on
Independent Living (2) Adoption factors for AV (3)
In-Vehicle design requirements (4) Mobility As a
Service Capabilities (5) MaaS Business Models for
OA. Initial findings from thematic analysis in relation
to each work-stream are presented as follows:
5.1 Impact of AV’s on Independent
Living
Findings suggest that the greatest positive impact on
Independent Living of Older Adults may be for rural
citizens, whereby AV’s may increase social
SMARTGREENS 2018 - 7th International Conference on Smart Cities and Green ICT Systems
300

interaction, ability to travel and reduce isolation for
this cohort. Irish rural citizens we spoke to are
constrained by reductions in available public
transport options, with the ‘cost’ of taxi’s and issues
of ‘trust’ an inhibitor for more frequent travel.
However, currently ‘ride sharing’ is not a norm for
rural citizens we interviewed due to unfamiliarity
with the concept as well as issues of ‘trust’. As it is
expected that future AV service models will emphasis
ride-sharing due to cost, whilst ‘country-road’ driving
poses challenges for AV design, this requires further
research attention.
Findings suggest that we do not yet know what
the net consequences for social interaction with
family members for older adults will be as we
transition to autonomous vehicles. Currently an
interdependent relationship with family exists around
mobility for OA. Whether AV’s lead to increased
mobility for Older Adults that increases overall
family interactions/engagement or results in the
further breakdown of family ties is a pertinent
research question looking forward.
Consistent with prior work linking driving
cessation with poorer health outcomes (e.g.
Depression, declining physical health etc.), a key
reason participants we interviewed ceased driving
was due to declining health. However, some
longitudinal studies tracking ‘Older Adults’ health
before and after driving cessation (e.g. Edwards,
Lunsman, Perkins, Rebok, & Roth, 2009) have found
steep declines in health after cessation. Furthermore,
a recent study suggests that increased cognitive
decline is shown after driving cessation (Choi et al.
2014). Given the practice of driving for elderly people
innately requires the practice of Cognitive Control,
from concentration, memory, peripheral awareness,
reasoning, decision making etc., the transition to
autonomous driving for this cohort could potentially
have ramifications for aspects of cognitive health of
‘Older adults’ unless counterbalanced through other
activities. A research challenge will be to understand
how the transition to AV’s influences OA overall
health, and whether in-vehicle activities can be
designed to compensate.
5.2 Adoption Factors for AV
What emerged through the pilot findings was that the
older adult cohort’s willingness to adopt AV’s may
well go beyond the reported safety of AV vehicles
and extend to perceived/observed driving etiquette
and behaviours of AV on the road. Thus,
‘Performance Expectancy’ measures should reflect
such aspects. Whilst driving etiquette may relate to
AV ‘courteousness’ to other road users, for example
heavy vehicles and slow driving vehicles pulling in to
let other vehicles pass or to warn other vehicles about
hazards ahead, driving behaviours could also relate to
conscientiousness to older adult’s ‘cautiousness’,
‘perception of speed’ or their ‘fragility’ relative to
younger drivers. Furthermore, many of the OA we
spoke with had strong views on what they perceived
as ‘good driving’ and ‘bad driving’, referring to some
drivers ‘rushing’, ‘weaving between lanes’, ‘breaking
tightly’ etc. Naturally, as AV’s begin to appear on
roads in the future, such views will translate across to
how OA view AV driving. As AV’s will be capable
of multiple driving behaviours/styles depending on
user demands, the challenge will be linking OA
perception of how the AV drives back to the user of
the vehicle.
5.3 In-Vehicle Design Requirements
Findings suggest that focusing on health and location
rather than age provides a better lens to understand
OA and mobility. The unique requirements of OA in
terms of health issues/conditions including
medications have consequences for the design of the
AV’S particularly IVCS and IVHCI. Separate or
combined participant disabilities/conditions acted to
limit one or more activities of making a journey, from
using satellite navigation, to hands free voice, to
memory problems related to the route, purpose or
distribution of a journey. Figure 1. below outlines the
health themes emerging and shows how one or more
of these themes have one or more consequences for
OA ability to adopt and use an AV. For example,
‘Incontinence’ suffered by several participants meant
they were unable to ‘manage long journeys’, without
requiring frequent toilet breaks, whilst ‘cognitive’
impairment could mean a passenger forgets the
purpose of the journey or is unclear where they have
arrived and why. How will AV systems accommodate
and address these issues? and perhaps do so when
there are multiple OA in the vehicle each with their
own unique set of health conditions/issues.
Most of the participants we spoke to could be
considered ‘passenger drivers’ in terms of watching
the road on journeys and alerting the driver to
potential dangers. A theme emerged that doing so
provided a ‘sense of control’ thereby reducing
passenger anxiety. AV systems could provide
visibility of identified dangers to passengers or
respond appropriately to passenger alerts, thereby
maintaining passenger ‘sense of control’ as they
transition to AV systems/services.
Autonomous Vehicles for Independent Living of Older Adults
301
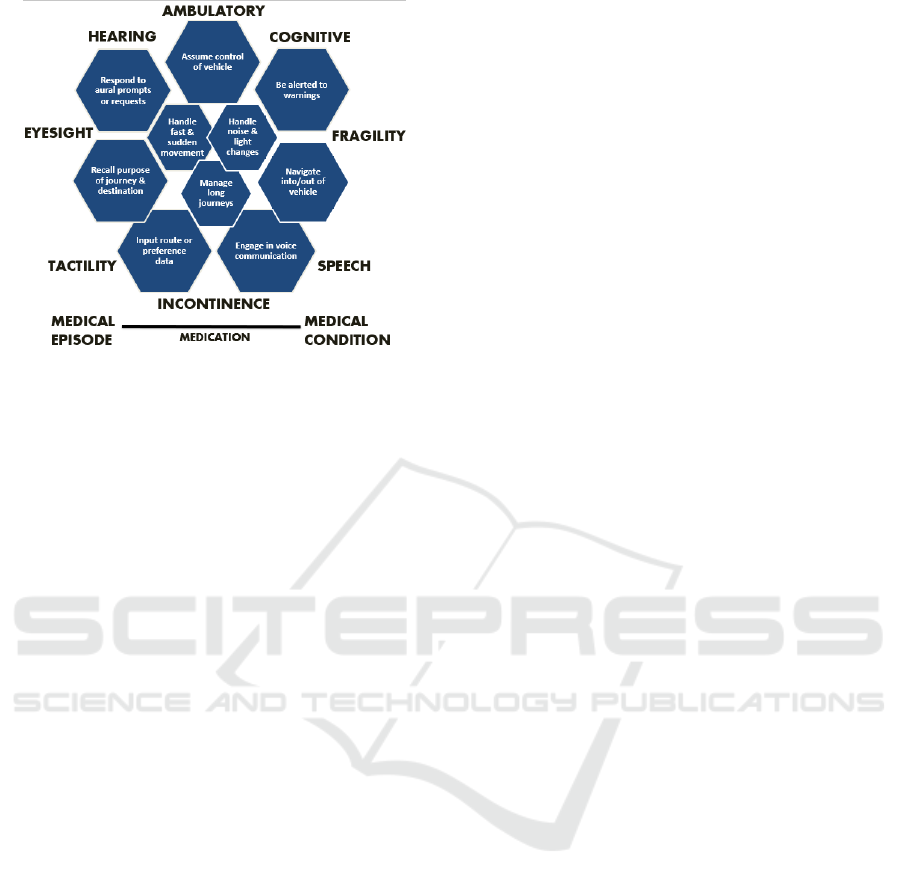
Figure 1: Disability/Condition informing AV design.
5.4 Mobility as a Service Capabilities
A number of findings in terms of passenger activities
and health issues etc. serve to inform the capabilities
and thus Value Proposition of future MaaS offering
for OA. Firstly, the desired passenger experience of
OA appears to differ to other population cohorts
suggesting MaaS offerings may need to cater
exclusively to OA adults on a designated trip. In this
regard, pre-passenger profiling to ensure OA are
suitably matched for customer journeys appears a
fruitful capability of future offerings. For example, an
AV journey may entail passengers are matched by
age, health conditions and interest. Furthermore, an
available passenger to assist other OA passengers
could make redundant the need for additional manned
AV journey assistance. A mechanism to incentivise
an available customer to assist other OA passengers
through reduced fares etc. or a passenger capable of
assuming control of the AV may need to be incenti-
vised and mandatorily available for each journey.
Furthermore, OA may have certain pre-requirements
for the journey in addition to needing assistance, such
as ‘seat preference’, ‘journey breaks’ etc.
5.5 MaaS Business Models for OA
Finally, MaaS business models will need to be
developed (taking into account MaaS capabilities) to
offer solutions to shortcomings in existing ‘Public
transport’ and ‘community organisations’ offerings.
Whilst services such as Uber, Lyft and Mytaxi in
Ireland offer urban services with some ‘ridesharing’
services being rolled out, they are currently
unavailable to suburban and rural customers due to
current shortcomings in economies of scale. The
comparatively limited population density of suburban
and rural areas requiring a rethink of how expected
customer experiences can be met. Furthermore,
findings suggest that norms of ride-sharing and trust
are not yet established in rural areas of Ireland.
Whether such norms and ‘trust’ issues are cultural or
exist in other regions in Europe will require careful
cross-country analysis and future comparative studies
of OA in differing regional territories.
6 CONCLUSION
This paper presented context, motivation and initial
findings from an exploratory qualitative pilot of
suburban and rural OA in Ireland. Findings suggest
that as AV systems assume driving control from
humans, existing technology adoption models such as
TAM2 and UTAUT2 (Venkatesh & Bala 2008;
Venkatesh et al. 2016) are currently inadequate in
predicting conditions for adoption of future complex
AV systems and services by Older Adults. This is due
to such aspects as ‘Trust’ (vehicle driving safety,
ensuring passenger safety with unique requirements,
ride-sharing safety etc.), ‘Transparency’
(communicate identification of hazards,
communicate the journey etc.), ‘Social Etiquette’
(consider and be conscientious to different passengers
and road users) and ‘Capability’ (accommodate
physical and cognitive disabilities/impediments etc.)
as being potentially important variables to
considering realising robust models. Discussion
highlighted several important research directions and
challenges in OA AV research looking forward
applicable to multiple research domains. For instance,
the social impact of AV on family relations, the
impact on OA cognitive ability/deterioration and the
design of MaaS business models for regions, are just
some of the research challenges raised.
Initial thematic findings presented will inform the
research focus and design of a cross-European
qualitative study of Older Adults in urban, suburban
and rural regions. The next step will be refinement of
an interview protocol based on insights and thematic
findings according to the 5 interrelated work streams
identified. The countries chosen for this study will be
Ireland, Italy, Germany and the UK. Final themes will
furthermore inform automotive HMI/HCI design
guidelines as well as proposing a technology
acceptance model of Older Adult acceptance of
Autonomous Vehicles.
This research project was supported by funding
from Science Foundation Ireland (SFI) and Intel
Corp.
SMARTGREENS 2018 - 7th International Conference on Smart Cities and Green ICT Systems
302

REFERENCES
Abraham, H. et al., 2016. Autonomous Vehicles, Trust and
Driving Alternatives : A survey of consumer
preferences. AgeLab, MIT.
Chihuri, S. et al., 2016. Driving cessation and health
outcomes in older adults. Journal of the American
Geriatrics Society, 64(2), pp.332–341.
Choi, M., Lohman, M. & Mezuk, B., 2014. Trajectories of
cognitive decline by driving mobility: evidence from
the Health and Retirement Study. International Journal
of Geriatric Psychiatry, 29(5), pp.447–453.
Connolly, S., Finn, C. & O’Shea, E., 2011. Rural Ageing in
Ireland: Key Trends and Issues, Irish Centre for Social
Gerontology, NUI Galway. Retrieved January, 10,
p.2017
Craik, F. et al., 1996. Aging and memory: Implications for
skilled performance. In Aging and skilled performance:
Advances in theory and applications, (4) pp. 113–137.
Duncan, M. et al., 2015. Using Automated Vehicles,
Enhanced mobility for aging populations using
automated vehicles (No. BDV30 977-11). Florida.
Dept. of Transportation.
Eby, D.W. et al., 2015. Keeping Older Adults Driving
Safely: A Research Synthesis of Advanced In-Vehicle
Technologies. Washington, DC: AAA Foundation for
Traffic Safety
Edwards, J.D. et al., 2009. Driving cessation and health
trajectories in older adults. Journals of Gerontology -
Series A Biological Sciences and Medical Sciences,
64(12), pp.1290–1295.
Eurostat, 2015. People in the EU – population projections.
Available at: http://ec.europa.eu/eurostat/statistics-ex
plained/index.php/People_in_the_EU_–_population_p
rojections.
Ghazizadeh, M., Lee, J.D. & Boyle, L.N., 2012. Extending
the Technology Acceptance Model to assess
automation. Cognition, Technology & Work, 14(1),
pp.39–49.
Harbers, M. & Achterberg, P., 2012. Europeans of
retirement age : chronic diseases and economic activity.
Bilthoven: RIVM
Holley-moore, G. & Creighton, H., 2015. The Future of
Transport in an Ageing Society. Age UK, London.
Iakovidis, I., 2015. The Silver Economy Opportunities for
European Regions,
IIHS, 2016. Older drivers. Available at: http://www.
iihs.org/iihs/topics/t/older-drivers/fatalityfacts/older-
people.
Shaw, L. et al., 2010. Seniors’ perceptions of vehicle safety
risks and needs. American Journal of Occupational
Therapy, 64(2), pp.215–224.
Shergold, I., Lyons, G. & Hubers, C., 2015. Future mobility
in an ageing society - Where are we heading? Journal
of Transport and Health, 2(1), pp.86–94.
Souders, D. & Charness, N., 2016. Challenges of Older
Drivers ’ Adoption of Advanced Driver Assistance
Systems and Autonomous Vehicles. In International
Conference on Human Aspects of IT for the Aged
Population.
Strategy Analytics, 2017. Accelerating the Future: The
Economic Impact of the Emerging Passenger Economy,
Available at: www.strategyanalytics.com.
Venkatesh, V. et al., 2016. Unified Theory of Acceptance
and Use of Technology: A Synthesis and the Road
Ahead. Jais, 17(5), pp.328–376.
Venkatesh, V. & Bala, H., 2008. Technology Acceptance
Model 3 and a Research Agenda on Interventions.
Decision Sciences, 39(2), pp.273–315.
Wan, He; Larsen, L., 2014. Older Americans With a
Disability: 2008−2012. Available at: https://www.
census.gov/content/dam/Census/library/publications/2
014/acs/acs-29.pdf.
Westlund, H. & Kobayashi, K., 2013. Social Capital and
Rural Development in the Knowledge Society. Edward
Elgar Publishing
Yang, J. & Coughlin, J. F., 2014. In-vehicle technology
for self-driving cars: Advantages and challenges for
aging drivers. International Journal of Automotive
Technology, 15(2), pp.333-340.
Young, K. L., Koppel, S. & Charlton, J. L., 2017. Toward
best practice in Human Machine Interface design for
older drivers : A review of current design guidelines.
Accident Analysis and Prevention, 106, pp.460–467.
Autonomous Vehicles for Independent Living of Older Adults
303
