
Online Surgery Rescheduling - A Data-driven Approach
for Real-time Decision Support
Norman Spangenberg
1
, Moritz Wilke
1
, Christoph Augenstein
1
and Bogdan Franczyk
1,2
1
University of Leipzig, Information Systems Institute, Grimmaische Straße 12, Leipzig, Germany
2
Wroclaw University of Economics, ul. Komandorska 118/120, Wroclaw, Poland
Keywords:
Online Surgery Scheduling, Decision Support System, Operating Room Management, Real-time Architecture.
Abstract:
The operating room area is still one of the most expensive sections in the hospital due to its high and cost-
intensive resource requirements. Further, several uncertainties like complications, cancellations and emergen-
cies as well as the need to monitor and control the interventions during execution distinguish the operational
planning tasks of surgery scheduling from more tactical and strategical planning activities. However there
are few solutions that support monitoring and decision-making in operating room management at this level
since they focus on creation of initial schedules or the efficient resource allocation. In this paper we describe
a solution approach for supporting online surgery scheduling by a real-time decision support system. It allows
the rescheduling based on intra-surgical information about the current surgical phases and predictions about
remaining intervention times and further allows replanning due to emergent or canceled patients.
1 INTRODUCTION
Many business processes on operational level are
characterized by uncertainties and frequent changes
in the environmental setting. Hence, online opera-
tional planning methods address the monitoring and
control of the process during execution and encom-
pass to react to unforeseen events (Hans and Van-
berkel, 2012). As well in every-day hospitals oper-
ations and especially the operating room (OR) area
are locations where these traits and vaguenesses are
ever-present. The OR manager is responsible for op-
erational planning in the OR area, in particular for the
supervision of all surgery-related resources and the
guarantee of efficient accomplishment of the initially
created surgery schedule according to diverse perfor-
mance indicators. Uncertainties like urgent or emer-
gent patients require the immediate integration in the
schedule and complications or cancellations lead to
time delays and shifting later procedures.
By this reasons, (May et al., 2011) describe the online
surgery scheduling (OSS) as an contemporaneous job
with a very short-term perspective that includes the
execution, monitoring and control of schedules that
were constructed the day before. At the beginning of
each day a surgery schedule exists but is often out-
dated within a few minutes and needs to be modi-
fied on-the-fly as the associated uncertainties and dy-
namics occur. Since complications, cancellations and
emergencies happen frequently it is uncommon that
a schedule stays all day through. For this reasons,
the OR manager needs latest information of the sit-
uations in the ORs as well as predictive information
about future states and the impact of possible deci-
sions. Despite, the well-known and often described
surgery scheduling problem, there are few systems so
far that tackle intra-day surgery scheduling and al-
low OR managers to get necessary information and
support the decisions based on this information. Ac-
cordingly, in this work we address the problem of
rescheduling of surgeries and describe a solution ap-
proach. The corresponding research question reads as
follows: How should a decision support solution be
designed for supporting the online surgery schedul-
ing problem?
In contrast to other approaches, we describe an inte-
grated solution that allows real-time rescheduling and
schedule modification based on intra-surgical infor-
mation about the current surgical status and predicted
future developments.
The paper is organized as follows. In section 2 we
present a state of the art of approaches for operational
support for real-time scheduling as well as for online
surgery scheduling. Section 3 provides a description
of the underlying decision and optimization problem.
Subsequently in section 4 we introduce the solution
336
Spangenberg, N., Wilke, M., Augenstein, C. and Franczyk, B.
Online Surgery Rescheduling - A Data-driven Approach for Real-time Decision Support.
DOI: 10.5220/0006805103360343
In Proceedings of the 20th International Conference on Enterprise Information Systems (ICEIS 2018), pages 336-343
ISBN: 978-989-758-298-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

approach and the inherent components of the deci-
sion support system. Section 5 describe the efforts so
for to validate our solution and give insights into the
use case setting and its impact. Finally we conclude
with a discussion of our results and describe future
research directions.
2 RELATED WORK
Surgery scheduling in general is one of the highly
adapted problems of operations research and schedul-
ing research community. (Demeulemeester et al.,
2013) as well as (Erdogan et al., 2010) state that
operational support for real-time scheduling is not
researched well in contrast to other domains where
real-time approaches can be found. (Atkin et al.,
2008) developed an approach for operational support
for online scheduling of airport runways with a de-
terministic scheduling algorithm. (Ngai et al., 2012)
describe an approach to compose primitive context
information of location sensors to support real-time
accident handling in fleet management use case.
The problem of monitoring and scheduling multiple
production plants is tackled by a information system
including a algorithmic pipeline is described by (Guo
et al., 2015) Since, the OSS problem differentiates
in aspects of uncertainties and unpredictablities to
the characteristics of these domains these approaches
cannot be replicated to the operating room area. E.g.
in manufacturing use cases the production process
can be paused and proceeded within the same state of
the item, which is not possible within a surgery (May
et al., 2011).
Nevertheless in surgery scheduling literature sev-
eral papers address the OSS problem and suggest
approaches for supporting decision makers. (De-
meulemeester et al., 2013; May et al., 2011;
Guerriero and Guido, 2011; Erdogan et al., 2010)
provide comprehensive reviews of existing literature
approaches tackling the various levels of the surgery
scheduling problem. Further, we focus on approaches
that face the OSS and are published after the men-
tioned reviews.
(Dios et al., 2015) provide a decision support sys-
tem for operating room managers to plan different
decision tasks like medium-term and short-term
schedules. Further, it is focused on handling elective
patients so it lacks in supporting very short-term
planning tasks like handling deviations in interven-
tion times or emergency patients.
(Erdogan et al., 2015) describe a stochastic integer
programming model for dynamic sequencing and
scheduling of appointments in hospitals with the
goal to minimize the weighted sum of direct waiting
time and waiting time until appointment for patients.
Though, they include different kinds of uncertainties
like process durations or number of customers,
the model isn’t directly portable to OSS since it
doesn’t involve important surgical characteristics like
urgency.
(Riise et al., 2016) propose an approach for a
generalized operational surgery scheduling problem
that is able to support decision making on different
planning levels and with different characteristics.
Hence, it helps planning elective patients as well
as rescheduling by integrating urgent and emergent
patients. Since, they argue that it is also applicable for
intra-day rescheduling, the evaluation only focuses
on scheduling on a weekly or daily level.
(Samudra et al., 2016) used a discrete event sim-
ulation model for the patient scheduling model
considering uncertainties like varying estimations
and arrivals of unplanned surgeries to avoid excessive
overtimes in the OR area. They handle rescheduling
of elective patients as well as including non-electives
in the current surgery schedule since it represents the
hospitals reality. They also use a estimated surgery
duration model based on mean values of similar
OR sessions but without feature-based machine
learning model. As well it doesn’t include real-time
remaining intervention time estimations based on
current phases.
(van Essen et al., 2012) developed a DSS that is
providing the three best adjusted OR schedules
according to variability in surgery duration and
emergencies. This system is based on a linear integer
programming model with the goal to accomplish
the preferences of all stakeholders and departments
as good as possible. Further, the objective function
includes penalties for canceling surgeries or overtime
minimization. It doesn’t include the reassignment of
surgeries to different ORs which leads to a reduced
flexibility in scheduling and hence reduced efficiency.
The previously presented approaches treat the OSS
problem on an algorithmic level, but don’t take
into account that information collection and DSS
architecture considerations could also show improve-
ments. This research papers assume that necessary
information is already present in the scheduling
system and further exclude the aspect of real-time
information systems.
Online Surgery Rescheduling - A Data-driven Approach for Real-time Decision Support
337
t
0
t
i
Monitor
environment
Rescheduling
Uncertainty
event occur
1
st
elective
planned duration
2
nd
elective 3
rd
elective
planned durationplanned duration
1
st
elective 2
nd
elective 3
rd
elective
real duration real duration
real duration idle
1
st
elective 2
nd
elective emergency
real duration real duration real duration overtime
3
rd
elective
t
oh
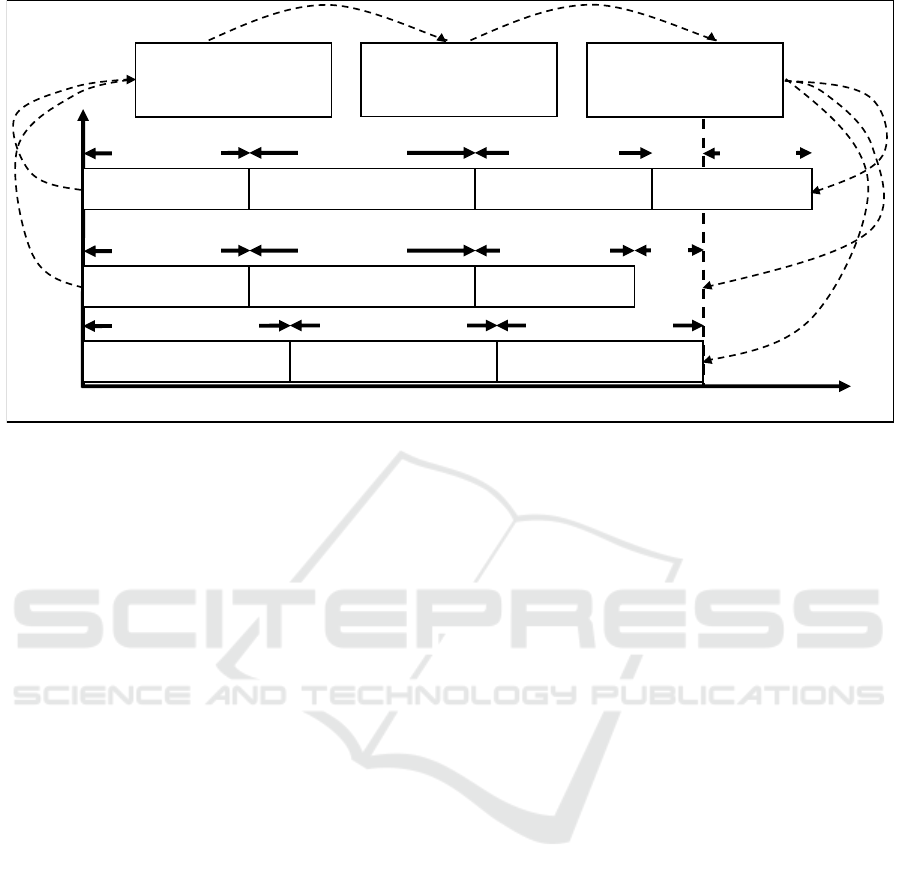
Figure 1: Model of the OSS problem for a single operating room including the challenges due to changing intervention
durations and introducing emergent cases (extension of (Hans and Vanberkel, 2012)).
3 PROBLEM FORMULATION
In this section we give a short formulation of the
OSS (rescheduling) problem for a particular day and
the corresponding mixed integer linear programming
(MILP) model that can be used to generate valid OR
schedules within a surgery day. Since, it is a dynamic
scheduling problem, it implies updating the schedule
defined the previous day in reaction to external effects
like incoming emergencies or internal changes like
deviations (see figure 1). According to the reschedul-
ing framework of (Vieira et al., 2003) the OSS prob-
lem described in this work can be seen as a dynamic
scheduling problem with variable arrivals of patients.
The OSS problem consists of a number of character-
istics, assumptions, resources and constraints that are
introduced next. The corresponding MILP model to
solve the OSS problem is formulated by:
A set of indices with capacities and resource require-
ments:
• I: Set of interventions to be performed within the
day, with elements i ∈ I
• O: Set of operating rooms available for surgeries,
with elements o ∈ O
• S: Set of surgeons, with elements s ∈ S
• T: Set of available time slots within the day, with
elements t ∈ T =1,...,X
A set of parameters describing properties of resources
related to the OSS:
• l
o,t
: Available time of OR o in working hours
• c
s,t
: Time capacity surgeon s is available for per-
forming interventions
• d
i
: Estimated duration of Intervention i
• u
i
: Urgency status of intervention i
• m
i
: Modification status of intervention i
Two planning variables are available to optimize the
schedule according to the given constraints, assump-
tions and resources:
• t
i
: Assigned starting time of intervention i
• o
i
: Assigned OR o of intervention i
The number of surgeries to be scheduled on the
tagged day is not known in advance, since it is likely
that emergencies occur. A surgical intervention i is
characterized by its surgeon s
i
, the estimated duration
d
i
before or during the intervention and its urgency
u
i
according to the scale elective, urgent and emer-
gent. Further, a modification parameter is introduced
to block interventions in a specific OR at a specific
time manually or after start. For each surgeon in-
dexed s, I
s
denotes the set of jobs that are performed
by that surgeon. Several assumptions are made to re-
duce complexity and develop a sparse model of the
OSS problem:
Assumption 1: ORs are interchangeable, e.g.
there are no equipment constraints.
Assumption 2: Unexpected incoming patients
receive preferential treatment in case they have
higher priority than scheduled elective patients.
ICEIS 2018 - 20th International Conference on Enterprise Information Systems
338

Assumption 3: There are enough surgeons and
surgical teams to treat electives, as well as accom-
modate non-electives.
Assumption 4: Surgery durations are estimations
that change during interventions.
The above assumptions and the following constraints
represent some of properties of the rescheduling pro-
cess resulting from the situation in the OR area. Some
hard constraints are defined, which, if they are vio-
lated, lead to an invalid surgery schedule.
Constraint 1: Only one surgery at the same time
in a operating room. A surgery cannot be assigned
to a OR that is occupied.
Constraint 2: A surgeon/surgical team can per-
form only one surgery at the same time.
Constraint 3: Surgeries tagged as not movable
must not be reassigned to other ORs or time slots
Further, four soft constraints are modeled:
Constraint 4: Don’t assign elective intervention
after operating room working hours.
Constraint 5: Do urgent and emergent interven-
tions as soon as possible.
Constraint 6: Avoid reassigning or canceling al-
ready assigned surgeries.
The problem is now to find an assignment σ : I ×T 7→
O of interventions to available time slots of operating
rooms and surgeons according to the intervention du-
ration. Hence, the solver optimizes the rescheduling
result according to the following goals.
The most important optimization criteria for the OR
manager (besides treatment quality) is maximizing
OR utilization of each operating room ω
u
(o
σ
) (1).
Since, there are several methods to calculate OR uti-
lization we use the definition of (Hans and Vanberkel,
2012).
Max ω
u
(o
σ
) =
I
∑
i=1
d
i
l
(1)
The 2nd objective minimizes waiting time ω
w
(σ) and
should lead to fast integration of non-electives:
Min ω
w
(σ) =
I
∑
i=1
uc
w
(2)
c
w
describes the cost efficient for the waiting time
of an intervention, while u means the urgency fac-
tor (higher urgency, higher integer value). The solver
should minimize the penalty costs for waiting, so
more urgent interventions are assigned fast (2). Fur-
ther, all types of surgery are assigned as early as pos-
sible, thus a by-product is minimized overtime ω
o
(σ).
Min ω
o
(σ) =
I
∑
i=1
β
u
l
canc
(3)
Adding penalty costs β
u
for each canceled or reas-
signed intervention should lead to the effect that valid
schedules with fewer reassignments/cancellations are
preferred (3). Canceled interventions have a higher
penalty beta than the reassigned and urgent interven-
tions have higher β
u
then electives.
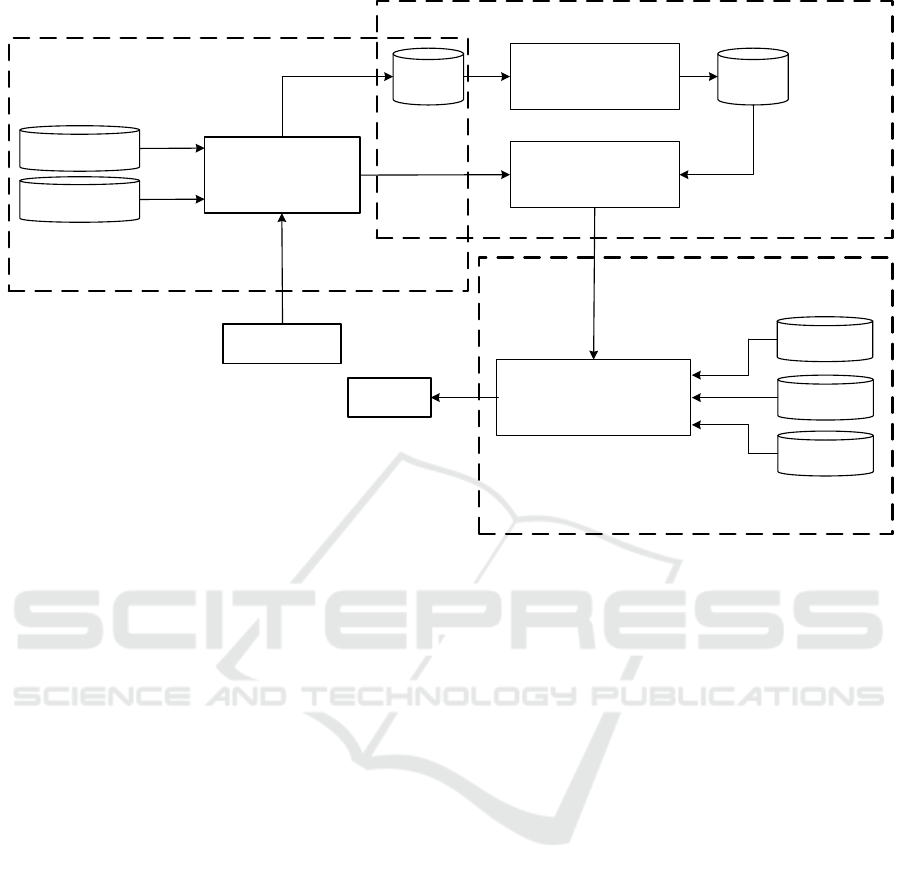
4 SOLUTION APPROACH
According to this problem, formulation a predictive-
reactive rescheduling strategy is utilized and sup-
ported with software tools to generate and partially
update the current schedule based on incoming events
with planning-relevant information. In this section
we propose an architectural approach with an online
surgery rescheduling engine. To realize this approach
several software components are needed to collect and
enhance the necessary information (see figure 2). The
segmentation of the solution approach into three parts
is because of separation of concerns. Nevertheless
they build on top of another each subsystem uses dif-
ferent type of data and information.
4.1 Situation Detection Subsystem
(SDS)
This component supports the information gathering
tasks of the OR manager and automatizes it to
ease and advance this process. Based on low-level
real-time data of e.g. cameras, surgical devices, OR
equipment or other connected devices information
about intra-surgical phases in running interventions
can be gathered. Besides processing the incoming
data streams, SDS realizes methods for the phase
detection. Lots of research exists for surgical phase
detection methods. Some are image- or video-based,
e.g. (Dergachyova et al., 2016). Others relying on
electronic signals of surgical devices are described
for example by (Padoy et al., 2012; Spangenberg
et al., 2017). All of these methods have their pros
and cons, e.g. some detect minimal invasive surgical
phases better then others and vice versa. We used
Complex Event Processing (CEP) for modeling
surgical phases based on surgical device data and
operating room equipment e.g. OR lights. According
to the taxonomy proposed in (Lalys and Jannin,
2014) this component classes into the data-to-model
analysis methods.
Online Surgery Rescheduling - A Data-driven Approach for Real-time Decision Support
339
Rescheduling
subsystem
Situation
detection subsystem
Event Processor
Raw data stream
Prediction
subsystem
Prediction model
computation
Online prediction
component
Model
database
Event
history
database
Phase event
model repository
Phase pattern
repository
Resource
database
Online rescheduling
component
Domain model
repository
Constraint
database
Surgery
schedule
Figure 2: Components of the solution approach and their interactions.
4.2 Prediction Subsystem (PS)
PS utilizes the data of the SDS two-fold: First, a batch
layer that uses historic surgical phases and other fea-
tures to create a machine learning model that predicts
the remaining intervention time of running surgeries.
This model is built with a random forest algorithm
based upon five features: an identifier for the surgery
type based on the official German classification of
medical procedures (OPS), a time stamp representing
the time passed since start and the operating room.
Further, the current phase as well as an event history
based on previously detected phases is factored into
the model. Second, an online prediction layer (speed
layer) that loads the model and aligns detected phases
in running surgeries with the model to update the esti-
mated intervention time. Further, this starts triggering
the rescheduling process.
4.3 Rescheduling Subsystem (RS)
After collecting information of the PS, the RS starts
to adapt the current schedule to events and changes
in surgeries. The RS is responsible for the genera-
tion of valid surgery schedules based on the resources
and constraints described in section 3. Rescheduling
is triggered by several factors, for example changes
in remaining durations of running interventions based
on the machine learning model. Further, the adding of
emergent or urgent patients to the set of interventions
leads to the execution of the rescheduling procedure.
We use a metaheuristics approach for solving the op-
timization problem of the rescheduling task. Meta-
heuristics don’t guarantee finding an optimal solution
for the optimization problem, but find an appropri-
ate solution in a given amount of time, which is nec-
essary for our goal to give real-time decision sup-
port. The search space is defined by two vectors:
One for the OR assignments of each surgery and sec-
ond a vector for non-overlapping time-slots including
surgeons, surgical team and ORs. Hence, the plan-
ning variables are operating room and the combina-
tion of starting time slot and the intervention dura-
tion. The cost function incorporates all cost factors
of the constraints described in 3. Violations of the
hard constraints, e.g. two surgeries at the same time
in the same OR, are not allowed. The quality of a
valid schedule is determined by the minimization of
the soft constraints. Our metaheuristic consists of the
following computational steps, based on the princi-
ple of local search. The used algorithm is Simulated
Annealing, described in more detail by (Kirkpatrick
et al., 1983). Since, it has been successfully used in
dynamic scheduling domain before it is as well scal-
able and finds near optimal solutions (Ceschia and
Schaerf, 2016).
ICEIS 2018 - 20th International Conference on Enterprise Information Systems
340

4.3.1 Initial Solution
To get a satisfying, but non-optimal and mostly not
feasible solution, initial solution of a schedule that af-
terward could be optimized, we use the First Fit Ap-
proximation algorithm. The algorithm assigns the in-
terventions to a available planning value (in our case
ORs and available time slots) and further takes the
already initialized interventions into account. Since,
First Fit doesn’t change an planning entity after as-
signing, it terminates after initializing all interven-
tions.
4.3.2 Move Selection
Moves are chosen indiscriminately as it is common
for Simulated Annealing algorithm. A move is se-
lected if it is equal or greater than the best move.
Furthermore, non-improving moves are also picked
with a certain probability according to its score and
the time gradient. In the early phase of the calcula-
tion process the probability of selecting sub-optimal
moves is higher than in later phases.
4.3.3 Cooling Schedule
Since, an ideal cooling method cannot be determined
in advance, a cooling calculation for temperature is
used. Depending on a time gradient decreases from
time to time by a constant quantity.
4.3.4 Acceptance and Stop Criterion
Moves are accepted in every case if they improve the
solution. Moves leading to a worse solution the ac-
ceptance probability is determined by e
− f
temp
, where f
describes the cost function and temp the current tem-
perature. The whole procedure stops when the cal-
culation gains a final temperature or exceeds a given
amount of time due to the near real-time requirement
of the system.
5 EVALUATION
The evaluation of the solution approach and its im-
plementation in a case study in a real-world setting
is planned for advanced research. So far we used a
simulated environment of an operating room area rep-
resenting 10 operating rooms each with 10 hours of
operation/day and 4 starting time slots/hour. We used
a data set of 15 surgeries with real-world data that
produce a low-level events stream to simulate a surgi-
cal day and feed the SDS. The detected intra-surgical
phases trigger the calculation of remaining interven-
tion times and use this information afterward to start
rescheduling. In this stage the interventions can have
five different states:
• Planned: Are introduced to the system, but OR or
time slot are not assigned yet.
• Scheduled: OR or time slots are assigned, but in-
tervention didn’t start already.
• In progress: Intervention is running and changes
in running intervention time are likely but OR
isn’t moveable.
• Reassigned: Scheduled intervention is reassigned
to other OR or time slot.
• Canceled: Are delayed with higher priority for
next day.
Observations showed that each running intervention
updates its predicted remaining time on an average
of 20 times so the rescheduling is triggered the same
number. Further, the observations indicate that the
metaheuristic provides good solutions according to
tardiness and schedule stability. Few reassignments
or cancellations are done by the algorithm and non-
elective interventions, that are fed into system as well,
are assigned fast (see figure 3).
First implications of the proposed system for produc-
tive operations are that the notable number of updates
of the surgery schedule will increase. This is be-
cause that domain knowledge of the OR manager ,
e.g. for remaining intervention times, is now mod-
eled and leads to a higher degree of transparency,
since less information and thus decisions are based
on experience-based knowledge and human estima-
tions. For the main user of the system (the OR man-
ager) two major improvements can be noted. First,
the whole process for information collection in the
operating room area is simplified. Second, the cogni-
tive efforts for combining current states, estimations,
available resources and potential emergencies, which
is done without software support so far, is reduced
significantly. These performance aspects will later be
investigated in more detail by comparing it to deci-
sions made by the OR manager.
Compared to other approaches tackling the OSS our
work provides some benefits. (Li et al., 2016; Riise
et al., 2016; Dios et al., 2015) also address short-
term scheduling, but focus on optimization and man-
ual adjustments on the day before. Hence, intra-day
rescheduling is still unsupported and conducted by the
OR manager. (Bruni et al., 2015) and (Heydari and
Soudi, 2015) describe a similar problem of handling
emergencies and uncertainties in surgery reschedul-
ing and formulate new solution strategies from a algo-
Online Surgery Rescheduling - A Data-driven Approach for Real-time Decision Support
341
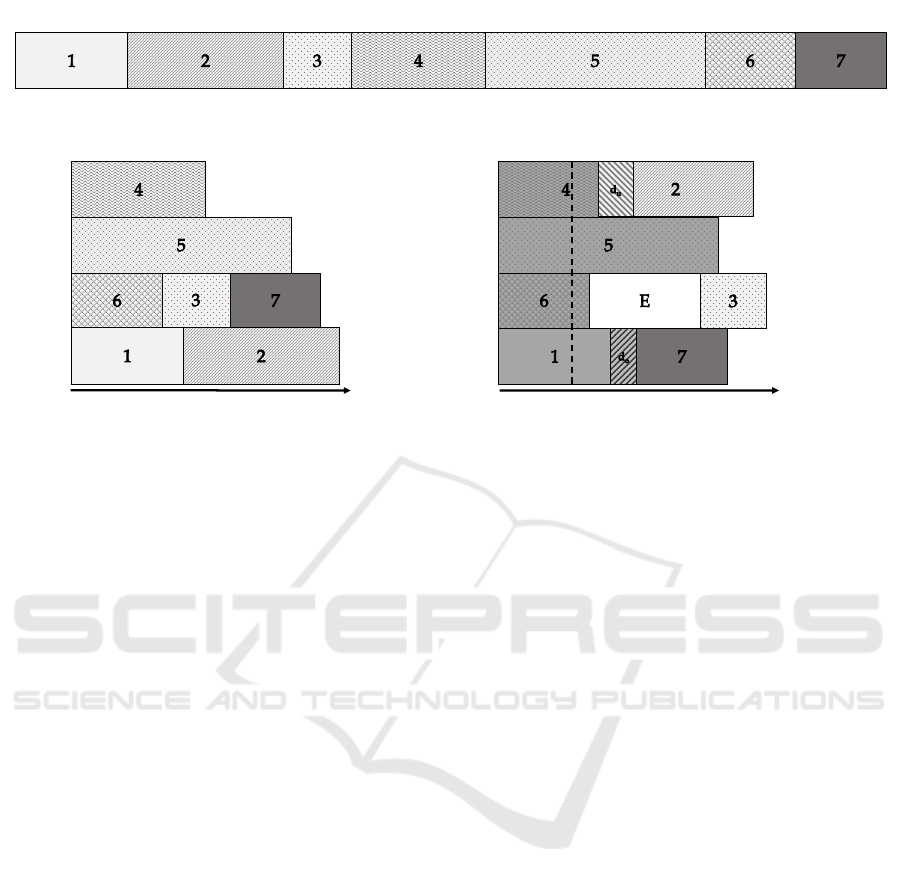
(0) Set of interventions I
(1) Initial schedule at time t
0
t
0
OR
1
OR
2
OR
3
OR
4
(2) Updated schedule at t
a
time with emergent case E
and predicted intervention duration changes d
u
and d
o
t
i
OR
1
OR
2
OR
3
OR
4
t
i
t
a
Figure 3: Components of the solution approach and their interactions.
rithmic point-of-view but lack with an integrated ar-
chitectural approach and implementation details that
would lead to simplifications for decision maker.
6 CONCLUSION
In this paper we presented a new solution approach
for supporting the OSS problem by a real-time deci-
sion support system for rescheduling. Based on intra-
surgical information about the current surgical phases
and predictions about remaining intervention times it
allows updating the surgery schedule and replanning
due to emergent or canceled patients. The proposed
approach denotes an innovative solution since most
of the current approaches operate on the tactical and
strategical planning and scheduling with longer time
horizons. We focused in this work on modeling OR-
related resources and constraints and for now omit
other related entities like intensive care (ICU) unit
or the like. But the approach can easily be extended
in this directions, e.g. by modeling other personnel
resources (nurses, porters, anesthetists) or facilities
(equipment, devices, ICU capacities). It was shown
that the benefits of our approach focus on the sup-
port of the OR manager and improve his daily tasks
twofold. First, the process for information collection
in the operating room area is simplified since it re-
duces communicative efforts, e.g. for monitoring cur-
rent system status the status of running interventions
in particular. Second, the cognitive efforts for com-
bining current states, estimations, available resources
and potential emergencies, is reduced significantly.
The prediction and the rescheduling subsystem pro-
vide an automatized solution for tasks which so far
are dispatched without software support.
In future work, we will focus on methodologies for
the appropriate delivery of information to the OR
manager. For instance a situation-aware user inter-
face would benefit our approach concerning for bet-
ter representation and prevention of information over-
load. Further, modeling more resources and con-
straints would lead to a more realistic Finally the eval-
uation of the integrated system in a real-world setting
in a operating room area will be done to compare the
performance of the system against human decision
makers.
ACKNOWLEDGMENTS
This paper was funded by the German Federal Min-
istry of Education and Research under the project
Competence Center for Scalable Data Services and
Solutions Dresden/Leipzig (BMBF 01IS14014B) and
by the German Federal Ministry of Economic Af-
fairs and Energy under the project InnOPlan (BMWI
01MD15002E).
REFERENCES
Atkin, J. A. D., Burke, E. K., Greenwood, J. S., and Ree-
son, D. (2008). On-line decision support for take-off
runway scheduling with uncertain taxi times at london
heathrow airport. Journal of Scheduling, 11(5):323–
346.
ICEIS 2018 - 20th International Conference on Enterprise Information Systems
342

Bruni, M. E., Beraldi, P., and Conforti, D. (2015). A
stochastic programming approach for operating the-
atre scheduling under uncertainty. IMA Journal of
Management Mathematics, 26(1):99–119.
Ceschia, S. and Schaerf, A. (2016). Dynamic patient admis-
sion scheduling with operating room constraints, flex-
ible horizons, and patient delays. Journal of Schedul-
ing, 19(4):377–389.
Demeulemeester, E., Beli
´
en, J., Cardoen, B., and Samudra,
M. (2013). Operating room planning & scheduling.
Handbook of Healthcare Operations Management.
Dergachyova, O., Bouget, D., Huaulme, A., Morandi, X.,
and Jannin, P. (2016). Automatic data-driven real-
time segmentation and recognition of surgical work-
flow. International Journal of Computer Assisted Ra-
diology and Surgery, 11(6):1081–1089.
Dios, M., Molina-Pariente, J. M., Fernandez-Viagas, V.,
Andrade-Pineda, J. L., and Framinan, J. M. (2015). A
decision support system for operating room schedul-
ing. Computers & Industrial Engineering, 88:430–
443.
Erdogan, S. A., Denton, B. T., Cochran, J. J., Cox, L. A.,
Keskinocak, P., Kharoufeh, J. P., and Smith, J. C.
(2010). Surgery planning and scheduling. In Wiley En-
cyclopedia of Operations Research and Management
Science. Wiley Online Library.
Erdogan, S. A., Gose, A., and Denton, B. T. (2015). Online
appointment sequencing and scheduling. IIE Transac-
tions, 47(11):1267–1286.
Guerriero, F. and Guido, R. (2011). Operational research
in the management of the operating theatre: a survey.
Health Care Management Science, 14(1):89–114.
Guo, Z. X., Ngai, E., Yang, C., and Liang, X. (2015). An
rfid-based intelligent decision support system archi-
tecture for production monitoring and scheduling in a
distributed manufacturing environment. International
Journal of Production Economics, 159:16–28.
Hans, E. W. and Vanberkel, P. T. (2012). Operating theatre
planning and scheduling. In Handbook of healthcare
system Scheduling, pages 105–130. Springer.
Heydari, M. and Soudi, A. (2015). Predictive / reactive
planning and scheduling of a surgical suite with emer-
gency patient arrival. Journal of Medical Systems,
40(1):30.
Kirkpatrick, S., Gelatt, C. D., and Vecchi, M. P. (1983).
Optimization by simulated annealing. science,
220(4598):671–680.
Lalys, F. and Jannin, P. (2014). Surgical process modelling:
a review. International Journal of Computer Assisted
Radiology and Surgery, 9(3):495–511.
Li, F., Gupta, D., and Potthoff, S. (2016). Improving oper-
ating room schedules. Health Care Management Sci-
ence, 19(3):261–278.
May, J. H., Spangler, W. E., Strum, D. P., and Vargas, L. G.
(2011). The surgical scheduling problem: Current re-
search and future opportunities. Production & Opera-
tions Management, 20(3):392–405.
Ngai, E., Leung, T., Wong, Y. H., Lee, M., Chai, P., and
Choi, Y. S. (2012). Design and development of a
context-aware decision support system for real-time
accident handling in logistics. Decision support sys-
tems, 52(4):816–827.
Padoy, N., Blum, T., Ahmadi, S.-A., Feussner, H., Berger,
M.-O., and Navab, N. (2012). Statistical modeling
and recognition of surgical workflow. Medical image
analysis, 16(3):632–641.
Riise, A., Mannino, C., and Burke, E. K. (2016). Modelling
and solving generalised operational surgery schedul-
ing problems. Computers & Operations Research,
66:1–11.
Samudra, M., Demeulemeester, E., Cardoen, B.,
Vansteenkiste, N., and Rademakers, F. E. (2016).
Due time driven surgery scheduling. Health Care
Management Science, pages 1–27.
Spangenberg, N., Augenstein, C., Franczyk, B., Wagner,
M., Apitz, M., and Kenngott, H. (2017). Method for
intra-surgical phase detection by using real-time med-
ical device data. 30th IEEE International Symposium
on Computer-Based Medical Systems 2017, 30:1–8.
van Essen, J. T., Hurink, J. L., Hartholt, W., and van den
Akker, Bernd J. (2012). Decision support system
for the operating room rescheduling problem. Health
Care Management Science, 15(4):355–372.
Vieira, G., Herrmann, J., and Lin, E. (2003). Reschedul-
ing manufacturing systems: A framework of strate-
gies, policies, and methods. Journal of Scheduling,
6:39–62.
Online Surgery Rescheduling - A Data-driven Approach for Real-time Decision Support
343
