
Comparison of Stress Level and Quality of Life in Elderly
Who are Living with Chronic Illness in Bangkok and Surabaya
Ni Putu Wulan Purnama Sari
1
and Jintana Artsanthia
2
1
Faculty of Nursing, Widya Mandala Catholic University Surabaya (WMCUS), Jl. Raya Kalisari Selatan 1, Pakuwon City,
Surabaya, Indonesia
2
Faculty of Nursing, Saint Louis College (SLC), 19 Sathorn Road, Yannawa, Bangkok, Thailand
Keywords: Chronic Illness, Elderly, Quality of Life, Stress Level.
Abstract: Elderly with chronic illness, such as hypertension (HT) and diabetes mellitus (DM), was prone to stress that
potentially decrease quality of life (QOL). This study aimed to compare and analyze the differences of stress
level and QOL in hypertensive and/or diabetic elderly between Bangkok and Surabaya. This cross-sectional
study involved 100 and 96 elderly with HT and/or DM in communities of Bangkok and Surabaya
respectively (n=196). There were 60 DM, 68 HT, and 68 DM&HT cases compiled from both sites.
Instrument used were SPST-20 and WHOQOL-BREF. Independent sample T test and Kolmogorov-
Smirnov Z test were used for data analysis (α=.05). There were 6% and 0% mild stress, 64% and 29.17%
moderate stress, 24% and 67.71% high stress, 6% and 3.13% severe stress were found in Bangkok and
Surabaya respectively. Stress level was differ significantly between Bangkok and Surabaya (p=.000).
Coping strategy tends to be more adaptive in Bangkok. There were 25% and 0% poor QOL, 52% and
91.67% moderate QOL, 23% and 8.33% good QOL were found in Bangkok and Surabaya respectively.
QOL was also differ significantly between Bangkok and Surabaya (p=.000). Elderly in Surabaya had higher
stress level, but elderly in Bangkok had lower QOL.
1 BACKGROUND
Non-communicable disease (NCD) or chronic
diseases are not passed from person to person. They
are of long duration and generally slow progression.
The four main types of NCD are cardiovascular
disease (e.g. hypertension/HT), cancer, chronic
respiratory disease, and diabetes mellitus (DM).
80% of all NCD deaths occur in low- and middle-
income countries. Almost three quarters of NCD
deaths - 28 million - occur in low- and middle-
income countries. 16 million NCD deaths occur
before the age of 70; 82% of these "premature"
deaths occurred in low- and middle-income
countries (WHO, 2015).
In Thailand, the burden of disease is gradually
shifting from communicable diseases to NCD,
injuries, and mental illness. Greatest public health
benefits are gained through prevention of NCD
(particularly cardiovascular disease, cancer, and
DM), injuries, and mental health disorder. These
benefits can be achieved if risk factors are identified
and mitigated through appropriate interventions. If
NCD and mental illnesses are detected at an early
stage and appropriate controls initiated, their
severity can be significantly reduced. The burden of
NCD usually falls disproportionately on the lower
socio-economic groups who often face higher
exposure to risk factors and have limited access to
health services. Diseases such as DM, cancer, and
cardio-vascular diseases are often not detected until
they reach advanced levels (WHO Thailand, 2014).
In response to the increasing impact of NCD, the
Royal Thai Government has increasingly directed its
attention on prevention and control initiatives. The
Bureau of Non-Communicable Diseases is
responsible for NCD, injury prevention, tobacco and
alcohol control programs. The Bureau has made
steady progress in monitoring the burden of NCD
and injuries in addition to identify major behavioural
risk factors classified by province. The Bureau also
plans to improve the collection and analysis of NCD
and injury mortality and morbidity data. This is
being done in efforts to monitor trends and evaluate
the success of interventions. The Bureau of Policy
and Strategy notes that due to the unreliability of
incidence data for selected NCD, injuries, and
Sari, N. and Artsanthia, J.
Comparison of Stress Level and Quality of Life in Elderly Who are Living with Chronic Illness in Bangkok and Surabaya.
DOI: 10.5220/0008321201010109
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 101-109
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
101
mental illnesses, cases of hospitalization with more
accurate diagnosis are needed to ascertain trends as
well as strengths/weaknesses of current programs.
In Indonesia, the burden of disease is gradually
shifting from communicable diseases to NCD also.
Over the past decades, Indonesia has made
phenomenal progress. Per capita income has been
increasing at a blistering pace, up to around $3,000
per capita in 2010. At the same time, fertility has
dropped dramatically, while life expectancy has
increased steadily. From an individual perspective,
these developments are clearly welcome. DM is of
particular concern ‒ by 2030, the number of people
with DM will nearly double, from 7.6 million in
2013 to 11.8 million. With an annual growth in DM
prevalence of 6%, this far exceeds the country’s
overall annual population growth rate (Blueprint for
Change Program, 2013). The costs associated with
NCD in Indonesia are substantial. According to our
calculations, the five domains of NCD
(cardiovascular disease, cancer, chronic obstructive
pulmonary disease, DM, and mental illness) will
cost Indonesia $4.47 trillion (or $17,863 per capita)
from 2012 to 2030 (data for total health expenditure
is obtained from the Global Health Expenditure
Database (GHED) of WHO, updated in 2014).
Not only because of adjustment to the new role
as an elderly in the family and age-related physical
changes, elderly with NCD are also get stressors
from the disease burden, such as disturbing signs and
symptoms, diet restriction, continuous physical
exercise requirement, etc. Chronic illnesses or NCD
can create stress in elders, both physically and
psychologically. Apart from impairing physical and
mental health, chronic illnesses may also have
negative impact on occupational and social
functioning and thus affecting the quality of life
(QOL). Positive thinking and an optimistic attitude
are needed to increase the compliance to treatment
regime and can motivate them to adjust their lifestyle
(e.g. quit smoking and alcohol use, giving up fatty
foods), thus help to promote healthy living
This study aimed to compare and analyze the
differences of stress level and QOL in elderly who
are living with chronic illness especially HT and/or
DM between Bangkok and Surabaya.
2 METHODS
This was a comparative study involving 196 elderly
with Diabetes Mellitus (DM) and/or Hypertension
(HT) in communities in Surabaya and Bangkok.
There were 96 and 100 cases compiled from
Surabaya and Bangkok respectively. Sample
distribution between 2 sites is presented in Table 1.
Sample was chose by criteria then totally
included in the study (total sampling). Inclusion
criteria consist of (1) elderly who are willing to
participate in the study, and (2) consume medication
from medical doctor to treat the disease. Exclusion
criteria were cannot communicate using Pasa Thai or
Bahasa Indonesia.
Instrument used were valid and reliable
questionnaire. SPST-20 was used to measure stress
level (IOC=.78; Cronbach's Alpha=.94). It consisted
of 20 items assessed in Likert scale format: 1 = no
stress, 2 = mild stress, 3 = moderate stress, 4 = high
stress and 5 = severe stress. The category of stress
level was 0-23 = mild stress, 24-41 = moderate
stress, 42-61 = high stress, and >62 = severe stress.
WHOQOL-BREF was used to measure QOL
(IOC=.83; Cronbach's Alpha=.84). It consisted of 26
items assessed in Likert scale format from 1 to 5,
various terminologies were used to define the score
of Likert in each item. Transformation score of 0-
100 was used in this study context. The category of
QOL is presented in Table 2.
Descriptive statistic, independent sample T test,
and Kolmogorov-Smirnov Z test were used for data
analysis (α = .05). Ethical clearance was issued by
Ethical Committee of Saint Louis College (SLC),
Bangkok, Thailand (November 17
th
, 2016), Number:
E. 038/2559.
Table 1: Sample distribution
Case Bangkok Surabaya Total
DM 30 30 60
HT 35 33 68
DM&HT 35 33 68
Total 100 96 196
Table 2: Category of QOL
Domain Poor Moderate Good
Physical 7-16 17-26 27-35
Psychological 6-14 15-22 23-30
Social 3-7 8-11 12-15
Environment 8-18 19-29 30-40
Overview 26-60 61-95 96-130
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
102
3 RESULTS
In total, the study respondents composed of 15.82%
male and 84.18% female. Age range was 60 – 78
years old. The educational background of sample in
Bangkok was mostly primary school (53%), while in
Surabaya was mostly secondary school (64.58%).
The income of sample in Bangkok was mostly 43%
at THB 2000-6000 per-month (43%), while in
Surabaya was mostly less than IDR 800 thousand
per month (53.13%). In Bangkok, most respondents
has relative who suffered from DM/HT (66%), while
in Surabaya no family background was reported
(69.79%). Table 3 will explain demography
characteristic of study respondents.
There were 6% and 0% mild stress, 64% and
29.17% moderate stress, 24% and 67.71% high
stress, 6% and 3.13% severe stress were found in
Bangkok and Surabaya respectively. Majority, we
found moderate stress in Bangkok and high stress in
Surabaya. 25% and 0% poor QOL, 52% and 91.67%
moderate QOL, 23% and 8.33% good QOL were
found in Bangkok and Surabaya respectively.
Majority, we found moderate QOL in both site.
Table 4 and 5 will explain the result of descriptive
statistical analysis of measured variables.
The value of stress level in Bangkok was more
various than Surabaya. The data of stress level was
not normally distributed and not homogenous (p<α).
Kolmogorov-Smirnov Z test showed that there was
significant difference of stress level between
Bangkok and Surabaya (p=.000). After deeper
analysis of each item in SPST-20 instrument, there
were 11 items determined this significant difference.
They were item 1, 2, 4, and 5 about anxiety, 6 about
finance, 7 about muscular pain, 10 about appetite, 11
about headache, 14 about anger, 18 about
concentration, and 19 about fatigue.
The value of overview QOL was also more
various in Bangkok. All data of QOL was normally
distributed and homogenous (p>α). Independent
sample T test showed that there was significant
difference of QOL between Bangkok and Surabaya
(p=.000). After deeper analysis of each item in
WHOQOL-BREF instrument, there were 14 items
determined this significant difference. They were Q1
about overview QOL, Q2 about health satisfaction,
Q5 about enjoyment of life, Q6 about life meaning,
Q7 about concentration, Q9 about living environ-
ment, Q18 about working satisfaction, Q19 about
Table 3: Demography characteristic
Characteristic Bangkok
(
100
)
Surabaya
(
96
)
n % n %
Sex
Male
Female
20
80
20
80
11
85
11.45
88.54
Age (years old)
60-69
>70
48
52
48
52
75
21
78.13
21.87
Education
Primary school
Secondary school
Bachelor degree
No stud
y
53
25
8
14
53
25
8
14
25
62
9
0
26.04
64.58
9.38
0
Occupation
Farmer
Businessman
Government officer
Other (retire,
housewife)
1
10
2
87
1
10
2
87
0
12
1
83
0
12.50
1.04
86.46
Monthly income
THB <2,000
(IDR <800,000)
THB 2,000-6,000
(IDR 800,000-2.4
million)
THB 6,000-10,000
(IDR 2.41-4 million)
THB >10,000
(IDR >4 million)
18
43
19
20
18
43
19
20
51
31
10
4
53.13
32.29
10.42
4.17
Family background
of HT/DM
Yes
No
66
34
66
34
29
67
30.21
69.79
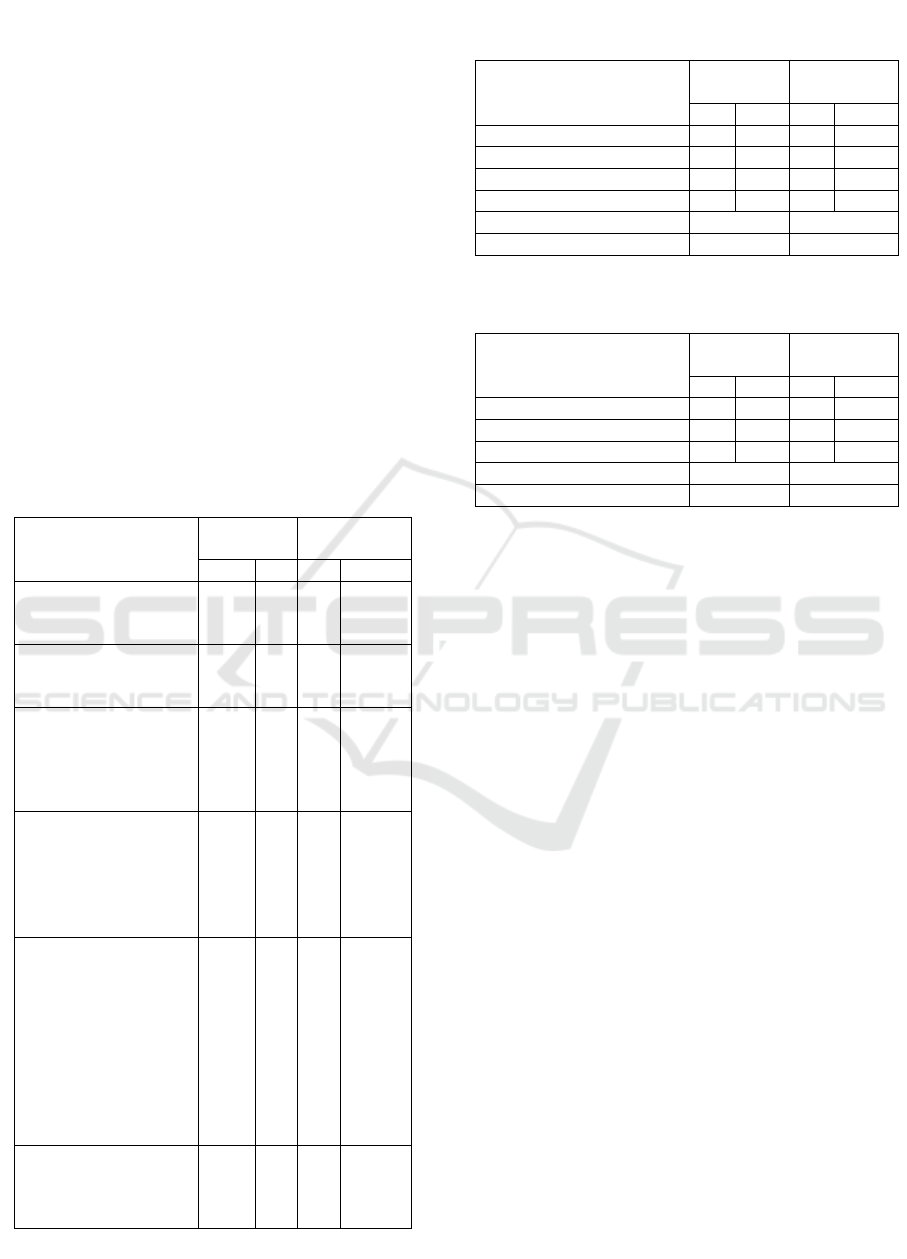
Table 4: Table of frequency and descriptive statistic of
Stress Level
Category Bangkok
(
100
)
Surabaya
(
96
)
n % n %
Mil
d
6 6 0 0
Moderate 64 64 28 29.17
High 24 24 65 67.71
Severe 6 6 3 3.13
Mean 36.82 48.42
Std. Deviation 13.29 8.89
Table 5: Table of frequency and descriptive statistic of
overview QOL
Category Bangkok
(100)
Surabaya
(96)
n % n %
Poo
r
25 25 0 0
Moderate 52 52 88 91.67
Goo
d
23 23 8 8.33
Mean 78.83 60.91
Std. Deviation 18.96 8.15
Comparison of Stress Level and Quality of Life in Elderly Who are Living with Chronic Illness in Bangkok and Surabaya
103

self-satisfaction, Q20 about personal/social relation-
ship, Q21 about sexual life, Q22 about social
support, Q24 about access to health care facility,
Q25 about transportation, and Q26 about negative
feeling. All domains was affected by the difference,
especially social domain in which all items were
affected (Q20, Q21, Q22), and psychological
domain (Q5, Q6, Q7, Q19, Q26).
4 DISCUSSION
4.1 Stress Level Differences
Results showed that there was significant difference
of stress level in elderly who are living with chronic
illness between Bangkok and Surabaya. This
difference was influenced by physical, psychology-
cal/emotional, and financial aspect. Physical aspect
relates to muscular pain, headache, appetite loss, and
fatigue. Psychological aspect relates to anxiety,
anger, and decreased concentration. Financial aspect
relates to low monthly income.
Muscular pain is frequently found in elderly.
Muscular pain in elderly usually happens because of
osteoporosis and osteoarthritis (Urban et al., 2010;
Camacho-Soto et al., 2011). An exploratory study in
Ghana showed that musculo-skeletal pain in elderly
is psychological, will worsen when they think too
much because of retirement, especially without a
house or enough money; also when the elderly left
alone at home and not doing anything, at times they
feel so bored (Aziato et al., 2016). The elderly
experience mild, moderate or severe pain and the
severity of pain increases with advancing age (Herr
et al., 2010). Pain also impairs sleep among the
elderly (Jacobson et al., 2009). Lack of sleep could
induce headache, along with hunger because of low
appetite. Chronic pain leads to a high incidence of
depression and anxiety among the elderly (Cino,
2014). Pain and aches were frequent stressors found
in elderly; therefore pain in various area of the body
could increase their stress level.
Appetite loss and the lack of hunger related to
aging have been termed as the anorexia of aging.
The etiology is multi-factorial and includes a
combination of physiological changes associated
with aging (decline in smell and taste, reduced
central and peripheral drive to eat, delayed gastric
emptying), pathological conditions (depression,
dementia, somatic diseases, medications and
iatrogenic interventions, oral-health status), and
social factors (poverty, loneliness). The anorexia of
aging is associated with protein-energy malnutrition,
sarcopenia, frailty, functional deterioration,
morbidity, and mortality. Loss of appetite may lead
to protein-energy malnutrition and weight loss
(Wysokinski et al., 2015). Appetite loss with weight
loss becomes a stressor for elderly because of its bad
consequences for health.
Fatigue is one of the most common symptoms
experienced by older people, both with and without
chronic disease. It is unpleasant and distressing and
can affect functioning and QOL (Egerton, 2013).
Fatigue can be an overwhelming and distressing
experience that constrains capacity for physical
functioning and social participation as well as
worsens morbidity and mortality outcomes (Yu et
al., 2010). A prospective study results focused on the
correlation between subjective fatigue, cognitive
function, and everyday functioning in elderly
showed that all domains of cognitive function and
everyday functioning declined significantly over
five years; and the decline rates differed by the latent
class of subjective fatigue. Except for the decreased
fatigue class, there were different degrees of
significant associations between the decline rates of
subjective fatigue and all domains of cognitive
function and everyday functioning in other classes of
subjective fatigue (Lin et al., 2013). Fatigue could be
a serious stressor for elderly because of its
consequences for everyday functioning impacted on
QOL.
The anxiety disorders are a prevalent mental
health problem in older age; it has a particular co-
morbidity and risk factor profile (Sami &
Nilforooshan, 2014). Anxiety disorders in the
elderly have been associated with neurotic
personality trait, cognitive decline, and increased
burden on physical health including frailty,
worsening physical functioning, increased disability
and increased taking of medications (Gale et al.,
2011; Ní Mhaoláin et al., 2012). Physical activity is
associated with lower levels of depression and
anxiety in elderly; female gender and lower
educational background had higher values of anxiety
and depression (Teixeira et al., 2013). Anxiety could
influence stress level in elderly because of its effect
on physical function in everyday life.
Anger could be an ordinary reaction to life
situations or indicative of emotional illness. Anger
can be healthy, and this should be recognized. For
some elders, anger correlates with good mental
health. Depression is regarded as an alternative to
anger – anger turned inward. Anger in elderly
correlates with the quality of their past relationships
with parents, siblings, children, and friends; conflict
management, coping strategy, work history, sexual
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
104

history, and life view. The elder’s anger response
has become conditioned over time. The elder could
be trying to gain attention or to distance himself
from others through the use of anger. The
rechanneling of anger in elderly can be promoted
through the use of physical activity, resident
councils, recreation activities, and other socially
acceptable means (McKinnon, 1998). By using these
means, coping strategy could be influenced.
Concentration is the ability to maintain attention
in a longer period. One of acute stress reaction is
concentration disorder (Idrus, 2016). A study
towards 74 elderly concluded that chronic stress and
coping strategies may be modulated by the presence
or absence of cognitive impairment, where memory
deficit awareness constitutes an additional potential
factor involved in high stress severity (Souza-
Talarico et al., 2009). Concentration disorder may
affect stress level in elderly because of its effect on
cognitive function impairment.
Financial problem is one of great stressor for
elderly, especially for those who had permanent job
previously. Study results showed that some elderly
already retire, and respondents in Surabaya had
lower monthly income than Bangkok. Financial
stress or strain which is presumably frequently
experienced by elderly in low socioeconomic status
or low income resulted in lower personal control
associated with distress (Caplan & Schooler, 2007).
Although financial strain is associated with actual
income and poverty, it is also associted with
cognitive capacity, depression, and self-esteem in
elderly, resulted in adverse effects on subjective
health (Angel et al., 2003). Economic security is the
key element that in a straightforward manner affects
people’s quality of life (Drobnic et al., 2010).
Financial problem in elderly needs to be addressed
by the family in which the elders live; therefore
stress level and subjective health status could be
perceived better.
During the aging process, there is evidence that
global perceived stress is associated with greater
reported exposure to daily stressor in older adults
(Stawski et al., 2008). These experiences of aging
and chronic illness symptoms may lead to
continuous anticipation of negative consequences,
triggering high levels of perceived stress symptoms
and cortisol levels. Stress symptomps are dependent
to coping strategy (Souza-Talarico et al., 2009). The
more adaptive coping strategy implemented, the
lower stress level perceived. Lower stress level
found in study respondents in Bangkok showed that
the elders there implemented more adaptive coping
strategy than the study respondents in Surabaya.
4.2 QoL Differences
Results showed that there was significant difference
of QOL in elderly who are living with chronic
illness between Bangkok and Surabaya. This
difference was mostly existed in psychological and
social domain of QOL. The difference was
influenced by working satisfaction (physical
domain); enjoyment of life, life meaning,
concentration, self-satisfaction, and negative feeling
(psychological domain); personal/social relationship,
sexual life, and social support (social domain);
living environment, access to health care facility,
and transportation (environmental domain).
Working satisfaction in elderly relates to physical
capacity needed for performing daily live activities
or household works; most study respondents already
retire, or being a housewife for now. Work is an
important economic, social, and psychological
ingredient of human life. Higher work intensity may
lead to deterioration of health and simultaneously
less likely to be able to afford the time needed for
health care due to work obligation (Zajc & Kohont,
2017). Time of health care in elderly with chronic
illness needs to be sufficient for monitoring their
health status and providing long-term vare needed
based on current health conditions. Less amount of
free time also affects life satisfaction, happiness,
depressed feeling, problem solving capacity, and
self-confidence of individual (Zajc & Kohont,
2017). Elderly needs sufficient free time and leisure
aktivities to increase their life satisfaction and QOL.
Enjoyment of life were found to be lesser in
individual with limiting and long standing illness,
such as DM and HT resulted in stroke, smoking,
physical inactivity, and alcoholic. Enjoyment of life
could predict a reduced risk of functional
impairment at older ages impacting QOL.
Independent predictors of functional impairment are
greater age, less wealth, having limiting – long
standing illness; baseline diabetes, arthritis, and
stroke; having a single impaired activity of daily
living at baseline, and physical inactivity (Steptoe et
al., 2014). Enjoyment in later life may also affect
cognitive health in elderly. Lack of cognitive health
in elderly results in decreased independence and
well-being, increrased health care costs, and
wellbeing, increased healthcare costs,
institutionalization and high levels of caregiver
burden (Hughes & Ganguli, 2009). Enjoymeny of
life needs to be adressed by elderly and the people
around them, along with adaptive coping strategy
implemented, so that better QOL could be achieved.
Comparison of Stress Level and Quality of Life in Elderly Who are Living with Chronic Illness in Bangkok and Surabaya
105

Life meaning, together with hope, have
significant correlation with positive mental health.
Life meaning explained 8% of variance of life
satisfaction. Life meaning is an independent
predictor of life satisfaction and self-esteem
(Halama & Dedova, 2007). For a single living older
woman, low living standard assessed by economic
and housing conditions seems to be a more serious
obstacle than poor health, making it difficult to
obtain a reasonable life satisfaction (Horstmann et
al., 2012). Generally, QOL is influenced by living
standard. Reasonable standard of living has changed
with time and cultural settings. In a society with
inequalities in living standard, there is elevated
stress level, especially in the lowest socio-economic
status, leading to poorer health and even lower life
satisfaction (Marmot, 2005). Poor QOL found in
Bangkok and lower QOL found in Surabaya
potentially because of inequalities in living standard
in the society, or unmatched status between
expectations and ambitions of respondents and the
possibility to reach their goals in life.
Self-satisfaction was associated with self-image.
Negative self-image is associated with various
psychological problems such as psychiatric
disturbance, low self-esteem, depression, and
behaviour problems. Self-image could predict
mental health in adulthood. The chronological age
influences the self-perception about self image. The
level of satisfaction indicates the assessment of the
quality of the resources that individuals hold in order
to face the challenges of age. Interpersonal
relationships and the reference cultural system,
where the individual acts, significantly contribute to
the definition of the idea of self (Diana et al., 2014).
Self-image in elderly is influenced by the construct
of self developed by values and culture in the family
and community. Better understanding of physical
changes and self-realization related to age could
promote positive self-image and psychological well-
being in elderly.
Negative feeling sometimes experienced by
elderly, such as loneliness and feeling abandon.
Loneliness was widespread among elderly widows.
Many felt isolated, dislocated from former social
circulation and missed being relevant (Nyanzi,
2011). A study conducted in rural Thailand towards
212 elderly showed that 9% were found to live
alone, 20% stated that they felt abandoned to some
degree. Feelings of abandonment do appear to result
in lower QOL in terms of psychological factors,
including one’s overall enjoyment of life, having a
meaningful life, and feelings of despair, anxiety or
depression (Sudnongbua et al., 2010). Abandonment
or loneliness of elderly, especially in rural area,
usually is a result of children emigration to other
area/city because of work and job obligations. But,
in city like Bangkok and Surabaya this condition
also exists, also mainly because of job obligations.
Adult children these days should pay more attention
to their elderly parents to promote better QOL.
Sexual life for elderly is difficult matter,
especially related to widower, negative body image,
depression, and erectile dysfunction due to chronic
illness. Sexuality impacts elderly’s QOL by
mechanism of spouse/family support, life
enjoyment, and secure feeling. Most study
respondents were women elderly, marital status and
widower were not identified. Post-menopausal
widows have less sexual appeal than younger
widows for whom reproduction is a viable outcome
of sexuality. Adult children usually control the
sexuality of their elderly parents often by
discouraging sexual liaisons. Adult children may
also arrange for new spouses with utilitarian value,
such as providing healthcare for ill elders (Nyanzi,
2011). QOL showed significant positive correlations
with body image and sexuality, but a significantly
negative correlation with depression. Body image,
depression, education level, sexuality, and stressor
were significant predictors influencing QOL in
middle-aged adults in the community (Kim & Kang,
2015). Erectile dysfunction was associated with
higher level of diabetes-specific health distress and
worse psychological adaptation to DM, related to
worse metabolic control. Erectile problem was also
associated with a dramatic increase in the prevalence
of severe depressive symptoms, less satisfactory in
sexual life, lower scores in the mental component of
QOL assessed by SF-36 (Berardis et al., 2002).
Social support gained from the family or
neighborhood is important to increase the value of
social domain of QOL in elderly because
communication with other person could add life
experiences that are stress relieving and cognitively
stimulating. A study in Turkey towards 108 older
adults concluded that QOL correlated with social
support from subgroups of family (spouse and
childrern), friends, and special friend (Unsar et al.,
2016). Social environment comprised of social
relationships and interpersonal interaction. Social
relationships can provide protection to life stresses
depression, loneliness, cognitive decline, risk of
institutionalization. Interpersonal interactions
promote psychological well-being and decreased
rates of morbidity and mortality (Smith &
Christakis, 2008). Socially active older adults tend to
have better cognition. Maintaining social networks
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
106

in later life may be beneficial as it provides several
social opportunities (Flatt & Hughes, 2013). Social
support gained from several social activities in later
life could promote cognitive health, life enjoyment,
adaptive coping strategy, and QOL.
Environmental factors also affect QOL. The
factors which are important in maintaining a good
QOL are being safe, overall living conditions,
having sufficient money, access to health services,
access to information for everyday living, leisure
activities, physical environment, and transport
(Sudnongbua et al., 2010). Living arrangement was
associated with health among older adults. Living
arrangement concordance increases the likelihood of
rating self-rated health as good, with concordance
having a greater impact for institutionalized elders
than for communityresiding elders (Sereny & Gu,
2011). Both living arrangement and home
modifications are important for promoting better
QOL in elderly who are having physical limitations.
Living environment is essential for elderly; it is
important to assure their safety, comfort, life
enjoyment, and condusive interpersonal relationship
with all family member.
Access to health care facility is essential for
elderly who are living with chronic illnesses,
sufficient time and proper health care service are
needed to promote routine check up of elderly’s
health condition. A poor, aging service design exerts
a negative effect on the QOL of elderly people. This
usually happens because government agencies have
limited resources, so that improvement items cannot
be implemented simultaneously. A comprehensive
aging place policy and increases effective use of
resources are needed to meet elderly people
demands, provide a clear design, and improve
service quality to match the demands and
expectations of elderly people (Chen, 2016).
Transportation is also important for promoting
better QOL in elderly. Currently, there are about 8.4
million senior citizens who depend on others for
their transportation. Shortly, the number of older
drivers will be more than double, making the issue
of senior transportation even more critical. In fact,
according to the Administration on Aging, by the
year 2030 the number of drivers over age 85 will be
4–5 times what it is today. The use of private vehicle
is not easy in older age, because of eye problems,
musculo-skeletal pain, tremor, and family
restriction; and because the skills and abilities
associated with driving tend to diminish with age—
viable alternate forms of transportation for the
elderly will continue to be an important issue for
years to come (FamilyCare America, 2018).
Therefore, elderly really need an easily accessible
public transportation developed by government or
private agencies to promote the use of medical care,
especially in urban life presented in Bangkok and
Surabaya.
5 CONCLUSIONS
There was significant difference of stress level in
elderly who are living with chronic illness between
Bangkok and Surabaya. This difference was
influenced by physical, psychological/emotional,
and financial aspect. Physical aspect relates to
muscular pain, headache, appetite loss, and fatigue.
Psychological aspect relates to anxiety, anger, and
decreased concentration. Financial aspect relates to
low monthly income. Coping strategy tends to be
more adaptive in Bangkok.
There was significant difference of QOL in
elderly who are living with chronic illness between
Bangkok and Surabaya. This difference was mostly
existed in psychological and social domain of QOL.
The difference was influenced by working
satisfaction (physical domain); enjoyment of life,
life meaning, concentration, self-satisfaction, and
negative feeling (psychological domain); personal/
social relationship, sexual life, and social support
(social domain); living environment, access to health
care facility, and transportation (environmental
domain). Inequalities in living standard tends to
happen in Surabaya’s society.
ACKNOWLEDGEMENTS
This study was funded by Saint Louis College (SLC)
and Widya Mandala Catholic University Surabaya
(WMCUS). This publication was supported by
Faculty of Nursing, WMCUS. We thanked all
respondents for participating in this study.
REFERENCES
Angel, R.J., Frisco, M., Anghel, J.L., Chiriboga,
D.A. 2003. Financial strain and health among
elderly Mexican-origin individuals. Journal of
Health and Social Behavior, 44: 536-551.
Aziato, L., Ohene, L.A., Norman, L. Antwi, H.O.
2016. Ageing with aches and pains’: lived
experiences of the elderly in Ghana.
Comparison of Stress Level and Quality of Life in Elderly Who are Living with Chronic Illness in Bangkok and Surabaya
107

International Journal of Caring Sciences, 9(2):
551-560.
Berardis, G.D., Franciosi, M., Belfiglio, M., Nardo,
B.D., Greenfield, S., Kaplan, S.H., Pellegrini, F.,
Sacco, M., Tognoni, G., Valentini, M.,
Nicolucci, A. Erectile dysfunction and quality of
life in type 2 diabetes patients. Diabetes Care,
25(2): 84-291.
Camacho-Soto, A., Sowa, G. & Weiner, D. K. 2011.
Chapter 58 - Geriatric pain. In: Candido, K et al.,
(ed.) Essentials of Pain Medicine (Third
Edition). Saint Louis: W.B. Saunders.
Caplan, L.J., Schooler, C. 2007. Socioeconomic
status and financial coping strategies: the
mediating role of perceived control. Social
Psychology Quarterly, 70(1): 43-58.
Cino, K. 2014. Aromatherapy hand massage for
older adults with chronic pain living in long term
care. Journal of Holistic Nursing, 32: 304-313.
Chen, S-H. 2016. Determining the service demands
of an aging population by integrating QFD and
FMEA method. Qual Quant., 50: 283–298.
Diana, P., Bottoni, G., Ferrari, G. 2014. Self-image
and self-satisfaction: a research among southern
Italian students using a battery of OSIQ items.
Italian Sociological Review, 2014, 4, 1, pp. 51-
70.
Drobnic, S., Beham, B., Prag, P. 2010. Good job,
Good life? Working conditions and quality of
life in Europe. Soc Indic Res., 99: 205–225.
Egerton, T. 2013. Self-reported aging-related
fatigue: a concept description and its relevance to
physical therapist practice. Physical Therapy,
93(10): 1403-1413.
Family Care America. (2018). Transportation and
The Elderly. Retrieved from:
http://www.caregiverslibrary.org/caregivers-
resources/grp-transportation/transportation-and-
the-elderly-article.aspx
Flatt, J.D., Hughes, T.F. 2013. Participation in social
activities in later life: does enjoyment have
important
implications for cognitive health?. Aging Health,
9(2): 149–158.
Gale, C.R. et al. 2011. Factors associated with
symptoms of anxiety and depression in five
cohorts of community-based older people: the
HALCyon (healthy ageing across the life course)
programme. Psychological Medicine, 41: 2057–
2073.
Halama, P., Dedova, M. 2007. Meaning in life and
hope as predictors of positive mental health: do
they explain residual variance not predicted by
personality traits. Studia Psychologica, 49(3):
191-200.
Herr, K., Titler, M., Fine, P., Sanders, S.,
Cavanaugh, J., Swegle, J., Forcucci, C. & Tang,
X. 2010. Assessing and treating pain in hospices:
current state of evidence-based practices. J Pain
Symptom Manage, 39: 803-19.
Horstmann, V., Haak, M., Tomsone, S., Iwarsson,
S., Gräsbeck, A. 2012. Life satisfaction in older
women in Latvia and Sweden—relations to
standard of living, aspects of health and coping
behaviour. J Cross Cult Gerontol., 27: 391–407.
Hughes, T.F., Ganguli, M. 2009. Modifiable midlife
risk factors for latelife cognitive impairment and
dementia. Curr. Psychiatry Rev., 5(2): 73–92.
Idrus, M.F. 2016. Stress-related disorder (in Bahasa
Indonesia). Retrieved from:
http://med.unhas.ac.id/kedokteran/wp-
content/uploads/2016/10/Gangguan-Terkait-
dengan-Stres.pdf
Jacobson, B. H., Boolani, A. & Smith, D. B. 2009.
Changes in back pain, sleep quality, and
perceived stress after introduction of new
bedding systems(). Journal of Chiropractic
Medicine, 8: 1-8.
Kim, J.S., Kang, S. 2015. A study on body image,
sexual quality of life, depression, and quality of
life in middle-aged adults. Asian Nursing
Research, 9, 96-103.
Lin, F., Chen, D-G., Vance, D.E., Ball, K.K.,
Mapstone, M. 2013. Longitudinal relationships
between subjective fatigue, cognitive function,
and everyday functioning in old age.
International Psychogeriatrics, 25(2): 275-285.
Marmot, M. 2005. Social determinants of health
inequalities. Lancet, 365: 1099–1104.
McKinnon, N. 1998. Caring for angry elders: what
makes them that way, and what you can do about
it. Nursing Homes, 47(11): 51-54.
Ní Mhaoláin, A.M. et al. 2012. Frailty, depression,
and anxiety in later life. International
Psychogeriatrics, 24: 1265–1274.
Nyanzi, S. 2011. Ambivalence surrounding elderly
widows’ sexuality in urban Uganda. Ageing Int.,
36: 378–400.
Sami, M.B., Nilforooshan, R. 2015. The natural
course of anxiety disorders in the elderly:a
systematic review of longitudinal trials.
International Psychogeriatrics, 27(7): 1061–
1069.
Sereny, M.D., Gu, D. 2011. Living arrangement
concordance and its association with self-rated
health among institutionalized and community-
residing older adults in China. J Cross Cult
Gerontol., 26: 239–259.
Smith, K.P., Christakis, N.A. 2008. Social networks
and health. Annu. Rev. Sociol., 34: 405–429.
Souza-Talaricoa, J.N., Chaves, E.C., Nitrini, R.,
Caramellic, P. 2009. Chronic stress is associated
with high cortisol levels and emotional coping
mechanisms in amnestic mild cognitive
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
108

impairment. Dement Geriatr Cogn Disord, 28: 465–
470.
Stawski, R.S., Sliwinski, M.J., Almeida, D.M.,
Smyth, J.M. 2008. Reported exposure and
emotional reactivity to daily stressors: the roles
of adult-age and global perceived stress. Psychol
Aging, 23(1): 52–61.
Steptoe, A., de Oliveira, C., Demakakos, P.,
Zaninotto, P. 2014. Enjoyment of life and
declining physical function at older ages: a
longitudinal cohort study. CMAJ, 186(4): 150-
156.
Sudnongbua, S., LaGrow, S., Boddy, J. 2010.
Feelings of Abandonment and Quality of Life
Among Older Persons in Rural Northeast
Thailand. J Cross Cult Gerontol., 25: 257–269.
Teixeira, C.M., Vasconcelos-Raposo, J.,
Fernandes, H.M., Brustad, R.J. 2013. Physical
activity, depression and anxiety among the
elderly. Soc Indic Res, 113: 307–318.
Unsar, S., Erol, O., Sut, N. 2016. Social support and
quality of life among older adults. International
Journal of Caring Sciences, 9(1): 249-257.
Urban, D., Cherny, N. & Catane, R. 2010. The
management of cancer pain in the elderly.
Critical Reviews in Oncology/Hematology, 73,
176-183.
World Health Organization (WHO). 2015. Non-
communicable Diseases Progress Monitor 2015
(September 2015). ISBN: 978 92 4 150945 9
WHO Thailand. 2014. Noncommunicable Diseases
(NCD) Country Profiles. Retrieved from:
www.who.int/nmh/countries/tha_en.pdf
WHO. 2014. WHO Global Health Expenditures
Atlas (September 2014). Retrieved from:
www.who.int/health-accounts/atlas2014.pdf
Wysokiński, A., Sobów, T., Kłoszewska, I., Kostka,
T., 2015. Mechanisms of the anorexia of aging—
a review. Age, 37:81.
Yu, D.S., Lee, D.T., Man, N.W. 2010. Fatigue
among older people: a review of the research
literature. Int J Nurs Stud., 47:216 –228.
Zajc, JC., Kohont, A. 2017. Impats of work intensity
on employees’ quality of work, life and health.
Teorija in Praksa, 54(2): 209-223.
Comparison of Stress Level and Quality of Life in Elderly Who are Living with Chronic Illness in Bangkok and Surabaya
109
