
Supportive-Educative Nutrition Increases Family Support, Adequate
Nutrition, and Decrease Diabetic Gastroparesis
Siti Nur Qomariah
1
, I Ketut Sudiana
2
, Harmayetty
3
and Abu Bakar
3
1
Faculty of Health Science, Gresik University, Gresik, Indonesia
2
Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia
3
Faculty of Nursing Universitas Airlangga, Kampus C Mulyorejo, Surabaya, Indonesia
Keywords: Supportive-Educative, Nutrition, Diabetic Gastroparesis
Abstract: Chronic complications are common in the gastrointestinal tract of diabetes mellitus patients called diabetic
gastroparesis. Supportive-educative nutrition will help patients and families to achieve adaptive behavior
and nutrition self-sufficiency. The purpose of this study was to analyze the influence of supportive-
educative nutrition on family support, nutritional intake, and decreased gastroparesis of patients with
diabetes mellitus. This study used quasi experimental, with pre-posttest design. The sample of 24 patients
and the patient's family was taken by purposive sampling technique. Independent variable was supportive-
educative nutrition and dependent variables were family support, nutritional intake, clinical sign of
gastroparesis, and blood glucose levels. Family support data, nutritional intake, clinical sign of gastroparesis
were measured by questionnaire and blood glucose levels by intake of venous blood samples. The
inferential analysis used was Wilcoxon Signed Rank, Mann-Whitney U test, paired T-test, Independent T-
test with significant level α=0.05. The result showed that there were significant differences in family
support (p = 0.005), nutritional intake (p = 0.015), and clinical sign of gastroparesis (p = 0.000). There was
no difference in post-prandial blood glucose levels (p = 0.229). Supportive-educative nutrition of diabetic
gastroparesis can improve the knowledge and acceptance of patients and families about the patient's
condition so that family support will increase and achieve adequate nutritional intake and decreased clinical
sign of gastroparesis.
1 BACKGROUND
The number of Diabetes Mellitus sufferers
worldwide and in Indonesia is increasing year by
year, the incidence of complications of the disease
also increases. Complications of DM disease of all
organs of the body and cause various complaints
(Ernawati, Suharto and Dewi, 2015). Diabetic
patients have diabetic gastroparesis after > five years
of onset and prevalence of diabetic gastroparesis or
dyspepsia occurring around 33.7% in DM patients
(Sfarti et al., 2010). Symptoms of diabetic
gastroparesis include: full satiety, after eating full
stomach, nausea, vomiting, abdominal pain and
abdominal distension. Patients with diabetic
gastroparesis experience symptoms as they eat,
resulting in inadequate oral intake and patients
experiencing calorie deficiency, some vitamins and
minerals (Koch and Calles-Escandón, 2015).
Supportive-educative is a nursing assistance
system that is given to patients with chronic diseases
and families who need support and education in the
hope that patients and families are able to do the
treatment independently (Tomey and Alligood,
2014). Supportive-educative nutrition to patients and
families becomes very important in the management
of DM disease because it helps increase the
participation of families in an effort to improve the
management of DM disease. Management of
diabetic gastroparesis patients with pharmacological
therapy has not given optimal results. Supportive-
educative nursing actions in diabetic gastroparesis
patients and families on nutritional intake in diabetic
gastroparesis patients will help patients and families
achieve adaptive behavior and self-sufficiency in
nutrition fulfillment. Recommended diet
modification based on an understanding of the
physiology of gastric emptying of food according to
the physical state and nutritional classification.
200
Qomariah, S., Sudiana, I., Harmayetty, . and Bakar, A.
Supportive-Educative Nutrition Increases Family Support, Adequate Nutrition, and Decrease Diabetic Gastroparesis.
DOI: 10.5220/0008322702000205
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 200-205
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Research purposes was to analyzed the effects of
supportive- educative nutritional support to family
support, nutritional intake, decreased gastroparesis,
and measure blood glucose level in patients with
diabetes mellitus.
2 METHODS
2.1 Study Design
Type and design of this research using Quasi
Experiment, with pre-posttest design. The study was
conducted at the Hospital in Gresik on April, 11st to
May, 30th 2014.
2.2 Study Population, Sampling,
Variables
The affordable populations in this study were all
patients with Type 1 and Type 2 DM who had
dyspepsia and came to internal medicine. The
sampling process using purposive sampling
technique. Samples were taken based on the patient's
inclusion criteria: age 30-60 years, DM 5 years or
more, received the same hypoglycemic treatment:
oral/ insulin/ combination or the same
gastrointestinal medication. Family inclusion
criteria: age 25-60 years old, living at home with
patients and more intensively caring for patients,
able to read and write. Sample size in each group
was 12 patients and family.
Independent variable in this research was
supportive-educative nutrition using booklet
combination with guidance and teaching. Dependent
variables include: family support, patient behavior in
nutritional intake, clinical symptoms and blood
glucose levels 2 hours pp series diabetic
gastroparesis patients.
2.3 Measure
The instrument of data collection using observation
sheet of Diabetes Social Support Questionnaire-
Family, Block Food Frequency Questionnaire,
Gastroparesis Cardinal Symptom Index, and
examination of blood glucose level 2 hours pp in
cooperation with the Laboratory Hospital in Gresik.
2.4 Intervention
The patient's initial procedure measured family
support, last week's nutritional intake, clinical sign
diabetic gastroparesis, and 1st blood glucose level.
Then, the patient treatment group was given
supportive-educative nutrition for 4 times (every
meeting 30-60 minutes) in 4 weeks, before starting
the patient's action checked blood glucose 2nd, 3rd,
4th. The control group performed conventional
intervention in accordance with the Standard
Operating Procedures (SPO) of the hospital. The
final stage of patient and family is reassessed family
support, last week's nutritional intake, clinical
picture, and 5th blood glucose level.
2.5 Data Analysis
The collected data were analyzed descriptively and
analytically by Wilcoxon Signed Rank Test, Mann-
Whitney U test, Paired T-Test, Independent T-Test,
ANOVA Same Subject and ANOVA Interaction 2
Factor with significance level α=0.05.
2.6 Ethical Clearance
Ethical permission was obtained from the Ethical
approval No: 75-KEPK, April 7th 2014 from the
Ethics Committee of the Faculty of Public Health
Universitas Airlangga. At the beginning of this
study, participants fulfilled informed consent and
demographic data. The researchers keep secret data
of each participants by using code.
3 RESULTS
Participants between treatment group and control
group had a similar characteristic in gender, age, and
length suffer of DM, which is most of the patients
Table 1: Characteristic of Patients Diabetic
Gastroparesis
Variable
Treatment Group
Control Group
n
%
n
%
Gender
Male
Female
2
10
16.6
83.4
3
9
25
75
Age (M ± SD)
51.58 ± 5.9
52.42 ± 3.6
Education
Elementary
Junior
Senior
Higher Ed.
3
3
3
3
25
25
25
25
-
1
11
-
-
8.3
91.7
-
Length of DM
5-10 years
11-15 years
16-20 years
9
2
1
75
16.7
8.3
11
1
-
91.7
8.3
-
Supportive-Educative Nutrition Increases Family Support, Adequate Nutrition, and Decrease Diabetic Gastroparesis
201
were female and length of DM 5-10 years. The
average age treatment group was 51.58 years old, as
much as 75% patients had a length of DM 5-10
years (Table 1). Characteristic of patients in control
group shows that the average age was 52.42 years
old, as much as 91.7% patients had a length of DM
5-10 years.
The results of data collection were obtained in
the treatment group from the total of 12 participants
before the supportive-educative action of low family
support nutrition as much as 9 people (75%) and
high family support of 3 people (25%). After high
family support action as many as 10 people
(83.33%) and low family support as much as 2
people (16.67%). In the control group of total
participants 12 people before the action of low
family support nutrition counseling as much as 9
people (75%) and high family support as much as 3
people (25%). After given supportive-educative
nutrition, high family support as much as 8 people
(66.67%) and low family support counted 4 person
(33.33%).
Wilcoxon Test Signed Rank Test got p value =
0.005. The p <0.05 results mean that there is a
supportive-educative effect of nutrition on family
support in DM patients with gastroparesis. While
Mann-Whitney test obtained p value = 0.106. The
p> 0.05 results mean that there is no difference in
family support between the treatment group and the
control group.
Data of nutrient intake in treatment group from
total of 12 participants before supportive-educative
action of nutrition of nutritional intake of patient
was nutritional deficiency as much as 5 people
(41.67%), nutrition more than 3 people (25%) and
nutrition fulfilled as many as 4 people (33.33%).
After given supportive-educative, nutrition intake of
patient is enough nutrition as many as 10 people
(83.33%) and nutrition more as much as 2 person
(16.67%). In the control group of total participants
12 people before nutritional counseling treatment of
nutritional intake of patients was nutritional
deficiency as much as 5 people (41.67%), more
nutrition as many as 3 people (25%), nutrient
fulfilled by 4 people (33.33%). After standard
procedure from hospital, nutrition intake of patient is
enough nutrition as many as 11 people (91.67%) and
more nutrition as much as 1 person (8.33%).
Wilcoxon Test Signed Rank Test got p value =
0.015. Result p count <0.05 meaning that there is
influence of supportive-educative nutrition to
nutrition intake of DM patient with gastroparesis.
While Mann-Whitney test obtained p value = 0.001
count. The p <0.05 results mean that there is a
significant difference in the patient's nutritional
intake between the treatment group and the control
group.
Clinical overview data on treatment group of
total participant 12 people before supportive-
educative nutrition of participant experience clinical
sign gastroparesis very severe as much as 1 person
(8.33%), severe clinical sign of gastroparesis
counted 4 person (33.33%), medium clinical sign as
many as 3 people (25%), mild clinical sign as much
as 1 person (8.33%), and very light clinical sign of 3
people (25%). After given supportive-educative
nutrition, most of participant feel clinical sign
gastroparesis very light as much as 7 people
(58.3%). In the control group of total participants 12
persons before the participant's nutritional
counseling experience clinical sign of gastroparesis
very severe as much as 2 people (16.7%), severe
clinical sign counted 6 people (50%), medium
clinical sign as many as 3 people (25%), and very
light clinical sign of 1 person (8.33%). After the
action, most of the clinical experience gastroparesis
very light as much as 7 people (58.3%).
Paired T-Test test obtained p value = 0,000.
Results p <0.05 which means that there is influence
support-educative nutrition to the clinical sign of
DM patients with gastroparesis. While the
independent test T-Test obtained p value = 0.994.
The p> 0.05 results mean that there is no difference
in the clinical sign of the patient between the
treatment group and the control group.
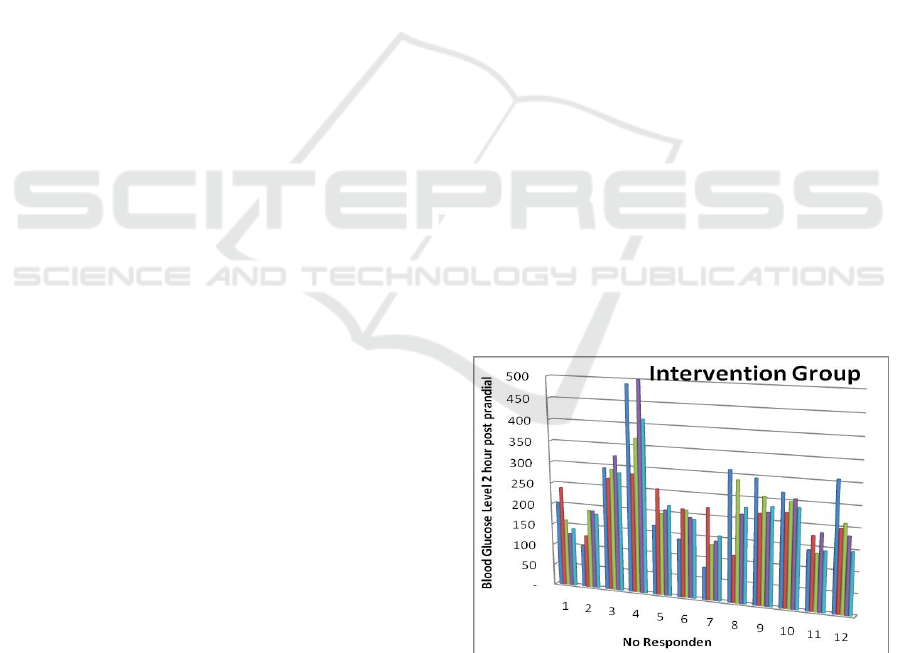
Most of the participants in the treatment group
showed an abnormal 2 hour pp blood glucose test of
200 mg / dL can be seen picture below.
Figure 1: Blood Glucose Test 2 hour pp series(1-5) on
intervention group.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
202

Figure 2: Blood Glucose Test 2 hour pp series on control
group.
ANOVA Same Subject test obtained p value =
0.229. Results p> 0.05 which means that there is no
influence supportive-educative nutrition to blood
glucose patient examination DM with gastroparesis.
While the test ANOVA Interaction Two Factors
obtained p value = 0.772. Results p> 0.05 which
means that there is no significant difference in blood
glucose levels of DM patients with gastroparesis
between the treatment group and the control group.
4 DISCUSSION
Family support is verbal information, real assistance
or behavior provided by the family with the subject
in his or her social environment or in the form of
attendance and things that can provide an emotional
advantage or influence on the behavior of the
recipient. People who get emotional support feel
relieved to be noticed, get advice or a pleasant
impression on him (Almutairi, 2015). Most
participants experienced increased family support
from low support to high support. There were 2
participants of the treatment group families who did
not experience a significant increase in family
support after the supportive-educative nutritional
action was performed because 2 intensive families
treated the patients to work in the civil service,
rarely at home and provide support and attention to
DM patients with gastroparesis. Factors that affect
family support one of them is intimacy. The more
intimate a person then the support obtained will be
greater. The family is the main group that has the
greatest emotional bond and the closest to the
sufferer, any grievances that are felt are usually
expressed on family members. Besides, families
relieve the burden of suffering during illness.
The results showed that most participants
experienced calorie deficiency before giving
supportive-educative nutrition. It says deficiency
when <60% of nutrient intake is needed (Keld and
Lal, 2014). The results of this study in line with
research in America showed that many patients with
DM gastroparesis deficiency energy, vitamins and
minerals by 194 patients from 305 patients. Caloric
deficiency of DM patients by <60% of estimated
total calorie requirement and deficiency of vitamin
C, D, E, K, folate, calcium, iron, magnesium and
potassium (Parkman, 2015). However, the study
participants showed no deficiency of certain
vitamins and minerals because most participants
received vitamin and mineral supplements to
provide less intake.
The results also showed 2 treatment group
participants with more nutritional intake. Patients
with chronic disease are sometimes saturated and
bored with existing dietary rules so that patients are
not adherent in the management of DM disease.
Giving supportive-educative nutrition in this study
not only touches the physical aspect but also the
psychological aspects so that patients are able to
adapt and independently in meeting and controlling
food intake.
DM patients with gastroparesis obtained data
before the nutritional supportive-educative measures
mostly had clinical sign of severe gastroparesis and
after most of have clinical sign of gastroparesis were
very light. Provision of nutritional supportive-
educative approaches known as Guidance (Booklet)
and Teaching by discussion method, where
participants and families are given the freedom to
express experience during illness, if any gaps are
corrected and guided by researchers and discussions
with patients and families to make decisions. This
method provides an opportunity for patients and
families to receive and respond to received guidance
and instruction (Notoatmodjo, 2010). This method
becomes very important because it emphasizes the
involvement of patients and families directly and
will more easily accept the various input given.
There were 1 treatment group participants who
still experienced severe gastroparesis sign after
providing supportive-educative nutrition. This is
because the participant does not carry out any
activity. This situation is in accordance with
previous research which shows that patient
perception can influence the success of action
(Homko, Siraj and Parkman, 2016). Symptoms and
signs of gastroparesis in DM patients due to slowing
Supportive-Educative Nutrition Increases Family Support, Adequate Nutrition, and Decrease Diabetic Gastroparesis
203

of emptying of the stomach without any organic
obstruction either in the stomach or small intestine
proximal part (Camiller et al., 2013). Light activity
such as walking casually half an hour after eating
will help empty the food in the stomach because the
food is quickly digested (Hasler, 2011).
Treatment group and control group participants
used gastrointestinal drugs. Symptoms associated
with gastroparesis in DM patients can be treated
using prokinetic drugs such as: metoclopramide,
cisapride and domperidone. These drugs can
penetrate the blood brain barrier causing side effects
drowsiness, anxiety, anxiety and fatigue. There is an
effect of gastrointestinal drug use on the decrease in
clinical sign of gastroparesis in DM patients. The
use of prokinetic drugs is not recommended in the
long term because it will lead to Parkinson's
syndrome and can occur seizures (Camilleri,
Bharucha and Farrugia, 2011). Between treatment
and control group also used same medication for
hipoglikemik and gastrointestinal drug, however
intervention group have more decrease in clinical
sign of gastroparesis than control group.
Most of the participants in the treatment group
showed an abnormal 2 hour blood glucose level that
is ≥200 mg/ dL. Adaptive behavior of individuals
and families, can not change the condition of
recombinant organ or cell DM patients that have
been damaged. This is in accordance with previous
research which states that the effects of gastroparesis
can damage the absorption of drugs so that blood
glucose levels become difficult to control (Oh and
Pasricha, 2013).
This study used diabetic gastroparesis patients
with the use of DM drugs and varying doses; oral,
insulin or a combination of oral-insulin. Incoming
foods will be absorbed in the small intestine that
activates insulin and glucagon. Insulin will cause
increased glycogenesis and inhibit glycogenolysis
(Guyton and Hall, 2014). Glucagon increases
glycogenesis by activating adenyl cyclase and
increasing intracellular cyclic adenosine
monophosphate (cAMP) in the liver. This will
activate phosphorylase through protein kinase
resulting in the breakdown of glycogen. With
glucagon then gluconeogenesis will also increase so
that the patient's blood glucose level is controlled
(Guyton and Hall, 2014).
The study participants who showed normal blood
glucose levels were some of the treatment group
participants and the control group who used
combination therapy of oral hypoglycemic drugs and
insulin. But the control group, although most use
oral hypoglycemic drugs can normalize blood
glucose levels. This is because most of the control
group participants with less duration of DM sickness
than the treatment group. Long suffer of DM
demonstrates the longer duration of DM disease that
is felt, the patient will feel bored and bored to
control the disease and obey the rules of the existing
diet. In addition to long-term DM pain associated
with damage to organs that produce insulin or cell
receptors (Camiller et al., 2013).
5 CONCLUSIONS
Supportive-educative nutrition can improve
understanding and acceptance of the family about
the patient's condition, related to increase family
support for the patient and changes in adaptive
nutritional intake behavior and decreased clinical
picture of gastroparesis. However, there was no
effect of supportive-educative nutrition on blood
glucose levels of 2 hp pp series of DM patients with
gastroparesis. The patient's blood glucose levels still
show abnormal blood glucose levels. Subsequent
studies may use gastric or endoscopic scintigraphic
diagnostic tests to confirm diabetic gastroparesis.
ACKNOWLEDGEMENT
We would like to acknowledge all of the
participants, nurse, and other hospital staff who
cooperated in the present study.
REFERENCES
American Diabetes Association, 2012. Standards of
Medical Care in Diabetes--2012. Diabetes Care,
35(Supplement_1), pp.S11–S63. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/22187469
[Accessed June 1, 2018].
American Diabetes Association, A.D., 2010. Standards of
medical care in diabetes--2010. Diabetes care, 33
Suppl 1(Supplement 1), pp.S11-61. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/20042772
[Accessed June 1, 2018].
Levine, M.E., 1966. Adaptation and Assessment: A
Rationale for Nursing Intervention. The American
Journal of Nursing, 66(11), p.2450. Available at:
https://www.jstor.org/stable/3420045?origin=crossref
[Accessed June 1, 2018].
Mystakidou, K. et al., 2010. Self-efficacy beliefs and
levels of anxiety in advanced cancer patients.
European Journal of Cancer Care, 19(2), pp.205–211.
Available at:
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
204

http://www.ncbi.nlm.nih.gov/pubmed/19659666
[Accessed June 1, 2018].
PERKENI, 2011. Konsensus Pengelolaan dan Pencegahan
Diabetes Melitus Tipe 2 di Indonesia 2011
Perkumpulan Endokrinologi Indonesia, Jakarta:
PERKENI. Available at:
https://s3.amazonaws.com/academia.edu.documents/3
6426530/Konsensus_DM_Tipe_2_Indonesia_2011_so
ft_launching_1.pdf?AWSAccessKeyId=AKIAIWOW
YYGZ2Y53UL3A&Expires=1527836083&Signature
=9U4%252F6%252FHVCmkxY%252Fp5WNLjdcMf
qwY%253D&response-content-
disposition=inline%253B%252 [Accessed January 2,
2015]. Almutairi, A. F. (2015) ‘Fostering a supportive
moral climate for health care providers: Toward
cultural safety and equity’, NursingPlus Open, pp. 1–
4. doi: 10.1016/j.npls.2015.02.001.
Camiller, M. et al. (2013) ‘Clinical Guideline:
Management of Gastroparesis’, The American Journal
of Gastroenterology, 108(1), pp. 18–37. doi:
10.1038/ajg.2012.373.Clinical.
Camilleri, M., Bharucha, A. E. and Farrugia, G. (2011)
‘Epidemiology, mechanisms, and management of
diabetic gastroparesis.’, Clinical gastroenterology and
hepatology : the official clinical practice journal of the
American Gastroenterological Association, 9(1), pp.
5–12. doi: 10.1016/j.cgh.2010.09.022.
Ernawati, N., Suharto and Dewi, Y. S. (2015)
‘Pemberdayaan Pasien berbasis Experiential Learning
terhadap Perilaku Pencegahan Komplikasi Akut dan
Kadar Glukosa Darah Pasien DM’, Jurnal Ners, 10(2),
pp. 256–264.
Guyton, A. C. and Hall, J. E. (2014) Buku ajar fisiologi
kedokteran. XII. Singapore: Elsevier.
Hasler, W. L. (2011) ‘Gastroparesis: pathogenesis,
diagnosis and management.’, Nature reviews.
Gastroenterology & hepatology, 8(8), pp. 438–53. doi:
10.1038/nrgastro.2011.116.
Homko, C., Siraj, E. S. and Parkman, H. P. (2016) ‘The
impact of gastroparesis on diabetes control: Patient
perceptions’, Journal of Diabetes and its
Complications, 30(5), pp. 826–829. doi:
10.1016/j.jdiacomp.2016.03.025.
Keld, R. and Lal, S. (2014) ‘Gastroparesis and nutrition’,
in Advanced Nutrition and Dietetics in
Gastroenterology, pp. 127–131. doi:
10.1002/9781118872796.ch3.6.
Koch, K. L. and Calles-Escandón, J. (2015) ‘Diabetic
gastroparesis’, Gastroenterology Clinics of North
America, pp. 39–57. doi: 10.1016/j.gtc.2014.11.005.
Notoatmodjo, S. (2010) Metodologi penelitian kesehatan.
Revisi. Jakarta: Rineka Cipta.
Oh, J. H. and Pasricha, P. J. (2013) ‘Recent advances in
the pathophysiology and treatment of gastroparesis’,
Journal of Neurogastroenterology and Motility, pp.
18–24. doi: 10.5056/jnm.2013.19.1.18.
Parkman, H. P. (2015) ‘Idiopathic gastroparesis’,
Gastroenterology Clinics of North America, pp. 59–
68. doi: 10.1016/j.gtc.2014.11.015.
Sfarti, C. et al. (2010) ‘Prevalence of gastroparesis in type
1 diabetes mellitus and its relationship to dyspeptic
symptoms’, Journal of Gastrointestinal and Liver
Diseases, 19(3), pp. 279–284.
Tomey, A. M. and Alligood, M. R. (2014) Nursing
Theorists and their work. 8th edn. Edited by A. M.
Tomey and M. R. Alligood. Philadelphia: Elsevier.
Supportive-Educative Nutrition Increases Family Support, Adequate Nutrition, and Decrease Diabetic Gastroparesis
205
