
Family Support and Coping Mechanisms in Patients with Pulmonary
Tuberculosis
Makhfudli, Alfan Fachrul Rozi, Tintin Sukartini, Candra Panji Asmoro
Faculty of Nursing, Universitas Airlangga, Kampus C Mulyorejo, Surabaya, Indonesia
Keywords: Family Support, Coping Mechanisms, Pulmonary Tuberculosis.
Abstract: Pulmonary tuberculosis is a stressor for patients, which shows coping mechanism that are adaptive or
maladaptive. One of the sources of coping mechanisms is social support, including instrumental,
informational, and emotional support. This study aims to analyze the correlation between family support and
coping mechanisms of patients with pulmonary tuberculosis. This study used a cross-sectional design. The
population comprised of patients with pulmonary tuberculosis in intensive phase treatment and continuous
phase treatment categories one and two at the TB Polyclinic. The sample comprised of 110 respondents based
on the inclusion criteria. The independent variable was family support and the dependent variable was the
coping mechanism. Data were collected through questionnaires and analyzed using the Spearman Rho
statistical test. There is a correlation between family support and pulmonary tuberculosis patients’ coping
mechanisms. The Spearman Rho test results were obtained at p = 0.000 and the correlation coefficient r =
0.377. This means there was positive correlation between family support and coping mechanisms, but the
power of correlation was weak. Patients with pulmonary tuberculosis are dominated by good family support.
The coping mechanisms of respondents is adaptive. Health institutions and health workers should optimize
family support to increase patients’ coping mechanisms.
1 BACKGROUND
Pulmonary tuberculosis is a disease that requires
serious treatment. Tuberculosis is still a health
problem for people in the world, although many
countries have made efforts to overcome this since
1995 (Regulation of the Minister of Health of the
Republic of Indonesia No. 67 of 2016 on
Tuberculosis Control). Pulmonary tuberculosis is a
chronic disease and patients with chronic illnesses
feel a loss of health, independence, productivity, and
self-fulfillment (Yusuf et al., 2015). Patients
diagnosed with pulmonary tuberculosis often
experience stigma from the community, even from
their family who are a source of coping, thus affecting
the patient's coping mechanisms (Azizah et al., 2016).
There is a relationship between family support and
stress (Nursalam, 2009) and poor family support
increases stress. Stigma in patients with pulmonary
tuberculosis is an important social determinant of
health (Craig et al., 2017). In addition to the stigma of
the community, many people with pulmonary
tuberculosis experience stress, depression, and
anxiety problems. This is caused by many factors felt
by people with pulmonary tuberculosis. One of these
is a poor coping mechanism in response to the
stressors they are faced with. Poor coping
mechanisms can be caused by poor family support in
patients with pulmonary tuberculosis.
Coping is a psychological adaptation to stress and
serious life events (Scheenen et al., 2017). The better
the coping strategies that are used to respond to
stressors, the smaller the risk of stress, conversely
when coping mechanisms used are maladaptive, the
risk of stress is higher. Maladaptive coping is
associated with increased stress (Deshmukh et al.,
2017). Psychological disorders of stress, depression,
and anxiety experienced by tuberculosis patients are
a manifestation of the maladaptive coping
mechanisms, impacting on their physical health.
Based on the results of interviews with patients
with pulmonary tuberculosis in the government
pulmonary hospital, it can be concluded that patients
feel burdened and anxious because of pulmonary
tuberculosis. Family support varies; some have good
family support, and some have poor family support.
The patients’ adaptation responses to their
tuberculosis disease varies.
642
Makhfudli, ., Rozi, A., Sukartini, T. and Asmoro, C.
Family Support and Coping Mechanisms in Patients with Pulmonary Tuberculosis.
DOI: 10.5220/0008330206420647
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 642-647
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Pulmonary tuberculosis sufferers have various
health problems, not only physical but also
psychological. Problems in the psychological aspect
are the emergence of stress, depression, and anxiety
because of poor coping mechanisms in patients with
pulmonary tuberculosis. Based on research conducted
by Muhammad Anugrah and Mokhammad Arifin
(2016), who conducted research on anxiety in patients
with pulmonary tuberculosis in Kedungwuni
Regency Pekalongan, 34 samples were obtained, and
the results indicated that 18 people (52.9%)
experiencing mild anxiety, 11 people (32.4%)
experienced moderate anxiety, and the remaining five
people (14.7%) experienced severe anxiety. The
results of the study by Atif et al. (2014) indicated that
67.1% of 336 respondents were at risk of depression
at the beginning of tuberculosis treatment. The data
of stress, depression, and anxiety events in patients
with pulmonary tuberculosis were also obtained by
stress measurement, depression, and anxiety.
Research intervention by Suryani et al. (2011)
indicated that 64.9% people experienced stress,
anxiety, and mild depression, while 35.1% suffered
from moderate depression.
Increased pulmonary tuberculosis in patients is a
challenge, not only for health workers in health
agencies, but also for the community. Appropriate
management will reduce the risk of the transmission
of pulmonary tuberculosis and will certainly improve
the quality of life for patients with pulmonary
tuberculosis. Having pulmonary tuberculosis causes a
loss of health and as a predisposing factor in the
biology of the emergence of stress in the individual,
will result in the formation of coping mechanisms.
For individuals experiencing stress, coping
mechanisms that emerge can come from various
sources of coping, including social support (Yusuf et
al., 2015). One form of social support is the support
of families. Each family has resources to look after
family members faced with health problems
(Friedman et al., 2010). In addition, family and
community members' support, including peers, is an
important factor influencing treatment compliance
positively, as a form of positive coping mechanisms
in patients with pulmonary tuberculosis (Deshmukh
et al., 2017).
2 METHODS
2.1 Design
This study was conducted using a cross-sectional
approach. The research aimed to analyze the
relationship between independent and dependent
variables. The independent variable in this study is
family support. The dependent variable in this
research is the coping mechanism.
2.2 Sample
The population in this study were pulmonary
tuberculosis patients in the government pulmonary
hospital intensive and advanced treatment phase,
categories 1 and 2. The sampling technique used was
consecutive sampling, which was conducted by
criticizing the sample using inclusion and exclusion
criteria. The sample size in this study comprised of
110 pulmonary tuberculosis patients at the
government pulmonary hospital in the intensive and
advanced treatment phase of category 1 and 2,
according to the inclusion criteria.
2.3 Data Collection
Data were collected using an instrument in the form
of a questionnaire that had been tested for validity and
reliability by previous researchers; hence, it was not
necessary to test validity and reliability in this study.
The questionnaire related to family support and
included emotional, instrumental and informational
supports, measuring respondents’ coping
mechanisms using a Brief Cope scale. Data were
analyzed using the Spearman Rho statistical test to
determine the correlation between variables.
2.4 Ethical Clearance
This study received a certificate of ethical clearance
from the Faculty of Nursing Universitas Airlangga
No. 572/KEPK.
3 RESULTS
Based on Table 1, the number of respondents was 110
people with a majority of 59 (53.6%) females. The
largest number of respondents were aged 21–30
years, comprising of 30 people (27.3%); only one
respondent was aged 71–80 years. The level of the
education of respondents was dominated by
elementary school graduates (SD)/equivalent and
senior high school (SMA)/equivalent with the same
number of 35 people or 31.8% in each group. Most
respondents were married (79 people or 71.8%), 37
respondents (33.6%) were housewives, and just three
respondents worked as Civil Servants (PNS). There
Family Support and Coping Mechanisms in Patients with Pulmonary Tuberculosis
643
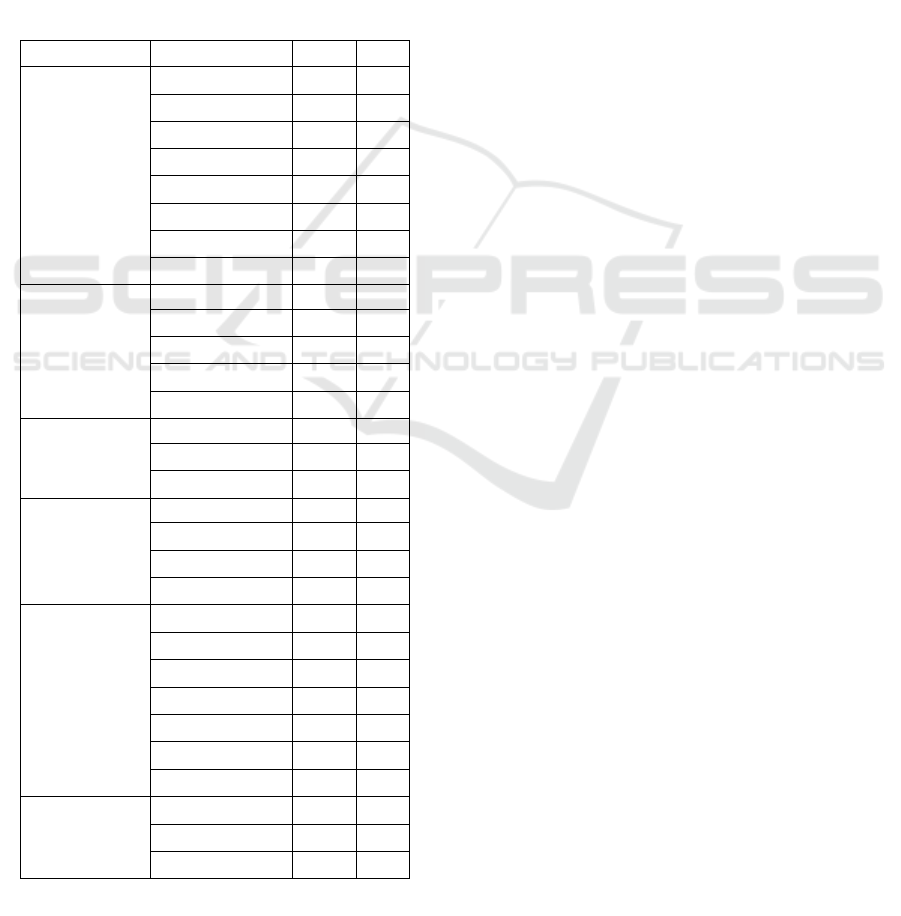
were just two religions followed by the respondents,
and Islam is the religion most widely embraced by the
respondents with 107 respondents (97.3%).
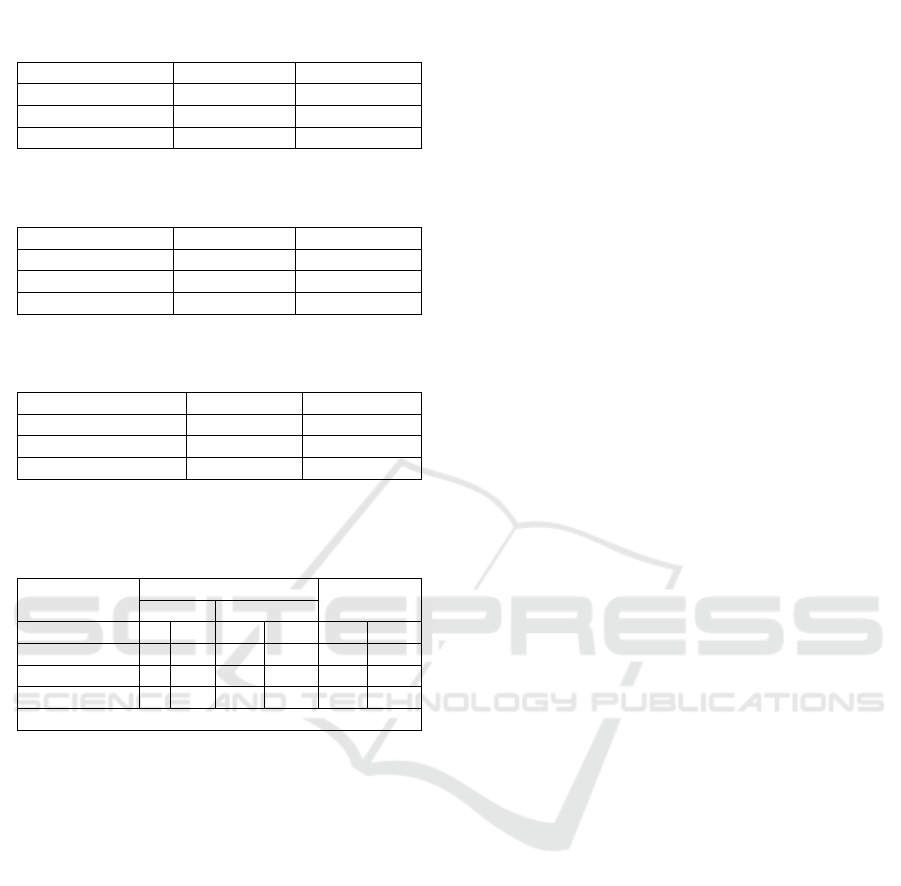
Table 2 shows the frequency of respondents in the
treatment phases of pulmonary tuberculosis. Table 2
indicates that the number of respondents who are in
the intensive phase of treatments is lower than those
respondents who are in the phase of follow-up
treatment at 49 respondents or 44.5%.
Table 3 indicates that good family support is
obtained by most research respondents with 109
respondents or 99.1% of the 110. Table 4 indicates
that adaptive coping mechanisms are widely used by
the respondents with 94 respondents or 85.5%.
Table 5 indicates that one respondent has less
family support and adaptive coping mechanisms and
there are 16 respondents with good family support,
but maladaptive coping mechanisms. Data were
analyzed using the Spearman Rho test, in relation to
family support relationships with coping mechanisms
of pulmonary tuberculosis patients at the Government
Pulmonary Hospital, with the result p = 0.000. The p-
value is below the p-value of 0.05 meaning H0 is
rejected and H1 is accepted; this means there is a
relationship between family support and coping
mechanisms with a weak strength of 0.377.
4 DISCUSSION
Family support is divided into instrumental support,
informational support, and emotional support
(Friedman et al., 2010). The support received by the
study respondents generally indicates good family
support from all three aspects. This is due to the
implementation of family duties in the field of health,
providing care to members of the family who are sick.
Setiadi (2008) suggests that families can take care
measures as well as make efforts to obtain follow-up
actions to prevent worsening health problems. Family
support given directly to the respondents has a
positive impact. This is in line with work by Sabine
Trepte et al. (2015) who state that emotional,
instrumental, and informational support given offline
is better than support given online.
Family support received by respondents comes
from the support of nuclear families who live in one
house, who understand the healthy development of
respondents and generally provide support in the
forms of informational support, instrumental and
emotional support. Informational support from the
family will increase the respondents knowledge of
pulmonary tuberculosis. Good knowledge will
improve the coping mechanisms of respondents. This
is in line with research conducted by Indah Ramadhan
et al. (2013) who suggest that there is a significant
relationship between the level of knowledge and
coping mechanisms.
The emotional support that is part of the support
of the family, includes loving support, understanding,
and attention and will create calm in the
psychological aspect of the respondent directly
related to coping mechanisms. A person who gets
good emotional support will reduce the stigma of self
and increase self-esteem. The research by Peng Wei
et al. (2016) shows that family support has a moderate
effect on the respondents’ self-esteem, while Mega
Arianti et al. (2016) mentions that high self-stigma is
Table 1: Demographic characteristics of respondents.
Characteristic Indicators f
(
x
)
%
Age
(years old)
18
–
20 13 11.8
21
–
30 30 27.3
31
–
40 21 19.1
41
–
50 27 24.5
51
–
60 13 11.8
61
–
70 5 4.5
71
–
80 1 0.1
Total
110 100
Education
Not
p
asse
d
6 5.5
Elementary 53 48.2
Junior hi
g
h 35 31.8
Senior high 16 14.5
Total
110 100
Gender
Male 51 46.4
Female 59 53.6
Total 110 100
Marital status
Marrie
d
79 71.8
Single 20 18.2
Widow/e
r
11 10
Total
110 100
Occupation
Gov. staff 3 2.7
Private staff 26 23.6
Housewife 37 33.6
Labore
r
18 16.4
Unem
p
lo
y
ment 18 16.4
Others 8 7.3
Total
110 100
Religion
Moslem 107 97.3
Christian 3 2.7
Total
110 100
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
644
due to a lack of knowledge and support from the
family. Erin K. Truong et al. (2015) mentions that the
quality of life of respondents, who are not stressed by
the stigma, showed better results because the
mechanism of the coping formed is positive.
Increased self-esteem and decreased self-stigma due
to positive family support will make a person feel
confident and able to use adaptive coping
mechanisms, broadly influencing the quality of life.
Family support is very important for supporting
respondents in adapting to stressors, as patients with
pulmonary tuberculosis. Good family support will
elicit a positive response from the responder so they
are calmer and able to adapt well. Eventually, they
will have an impact on improving pulmonary
tuberculosis patients’ quality of life. This is in
accordance with research by Deshmukh et al. 2017
who suggest that family support affects the resilience
of individuals who experience anxiety due to
stressors. Family support also deals with self-esteem
and quality of life. Chia-Chun Li et al. (2015) state
that respondents with low self-esteem and low family
support tend to have a lower quality of life compared
to respondents with low self-esteem but high social
support.
Most respondents use an adaptive coping
mechanism but there are some respondent who have
a maladaptive coping mechanism. The adaptive
coping mechanisms that most respondents use in
facing their stressors are activities such as praying or
meditating when experiencing problems; respondents
take action or steps to try to make the problem better
and are looking for good or wisdom in the problem.
The respondents with adaptive coping mechanisms
are natural and learn to live with problems they are
experiencing as well as accepting the problem they
face.
The coping mechanism used by the research
respondents showed different results; most
respondents used adaptive coping mechanisms and a
small percentage of respondents used maladaptive
coping mechanisms. Different coping responses in
each individual are influenced by how individuals
perceive stressful events; coping does not necessarily
lead to solving problems faced by individuals
(Azizah, et al., 2016). Coping mechanisms are
dynamic, so, according to various factors influencing
the selected coping mechanisms, human behavior is
always dynamic (Yusuf et al., 2015).
Pulmonary tuberculosis and its impact on life
aspects is a stressor that affects respondents’, their
family, and other aspects of their lives. The coping
mechanism used by respondents clearly differs
because it depends on how individuals perceive the
stressors they are facing; they are influenced by
various factors, so even if the same stressors and its
impact on the aspects of life apply, the perceptions
and the supporting factors of the emergence of coping
mechanisms on each respondent vary, which means
that the coping mechanisms used in adapting to
stressors also vary.
A coping mechanism that is widely used by the
respondents in this study is the adaptive coping
mechanism. The results of this study indicates that
most research respondents can adapt to the stressors
they face. Good adaptation to stressors will affect the
respondents’ psychological responses as well as
emotional disturbances; individuals with good coping
mechanisms will calmly respond to stressors and
improve their resilience. This is in line with research
by Okafor et al. (2016) who suggest that active coping
behavior is associated with increased resilience.
The results of the data analysis indicate that there
is a relationship between family support and coping
mechanisms in patients with pulmonary tuberculosis.
Some respondents have less family support but have
Table 2: Frequency of respondents in the phase of
treatment of pulmonary tuberculosis.
Phase f %
Intensive 49 44.5
Continue
d
61 55.5
Total 110 100
Table 3: Family support and coping mechanisms of
patients with pulmonary tuberculosis.
Family support f %
High 109 99.1
Less 1 0.9
Total 110 100
Table 4. Coping mechanisms of patients with
pulmonary tuberculosis.
Co
p
in
g
mechanism f %
Ada
p
tive 94 85.5
Maladaptive 16 14.5
Total 110 100
Table 5. The relationship of family support with the
coping mechanisms of patients with pulmonary
tuberculosis.
Variable Famil
y
su
pp
ort Total
Less Hi
g
h
Coping Mec f % f % f %
Maladaptive 0 0 16 14.5 16 16.5
Adaptive 1 0.9 93 84.5 94 85.5
Total 1 0.9 109 99.1 110 100
(p)
0.000
(
r
)
0.377
Family Support and Coping Mechanisms in Patients with Pulmonary Tuberculosis
645

adaptive coping mechanisms. Some respondents have
good family support but use a maladaptive coping
mechanism. Facing stressors, such as suffering from
pulmonary tuberculosis and its effects, will certainly
cause psychological disturbances, especially for the
sufferer. Individuals who deal with stressors are
perceived to suppress their desire to seek the
resources they need, such as economy, time, family
social support, and other resources to help them deal
with it (Azizah et al., 2016).
Family support is required by the patient to help
them deal with problems well. Family support is a
social support experienced by family members who
are ready to provide help and assistance whenever it
is needed (Friedman et al., 2010). Family support is
comprised of three forms of support, helping the
patient with pulmonary tuberculosis in adapting to the
problem. This appropriates facilities, information,
and attention of the family, to elicit good coping
mechanisms or adaptive coping mechanisms in
response to the stressors.
Family support is a resource that can generate
physical and psychological comfort for an individual.
Family support provides a positive aspect for family
members who receive support (Azizah et al., 2016).
Family is a source of coping mechanism for
individuals in the face of stressors or problems they
face (Azizah et al., 2016). Good family support to
family members who are experiencing health
problems in this study has a positive impact in the
form of positive or adaptive coping mechanisms of
patients in response to stressors.
Family support is not the only source of coping
mechanisms. There are many other factors that
influence and become a source of coping mechanism.
The results of a study showing a family support
relationship with coping mechanisms indicates that
family support influences an individual to choose the
coping mechanism they use to respond to stressors,
whether adaptive or maladaptive coping mechanisms
are emerging. Individuals can adapt well to problems
they face with the family support they receive from
family members.
The existence of family support relationships with
coping mechanisms in patients with pulmonary
tuberculosis is in line with the study of Das et al.
(2017) who believe that individuals who receive
family and friends’ support show good coping
mechanisms that are adaptive and resilient. Nursalam
et al. (2009) state that family support can reduce
stress. The better the support given to family
members who are experiencing psychological
disorders, such as stress, the more the stress is
reduced. Research conducted by Tintin et al. (2016)
indicates that family support can improve
psychological responses to individuals when facing
problems. Psychological disorders including stress,
anxiety, and depression are closely related to coping
mechanisms. The maladaptive coping mechanism
leads to psychological disorders; an adaptive coping
mechanism will prompt an individual to respond to
the stressor positive. One source of individual coping
mechanisms, whether adaptive or maladaptive, is the
social support they receive from their family.
5 CONCLUSIONS
Family support is related to coping mechanisms.
Patients with pulmonary tuberculosis are dominated
by good family support. The coping mechanisms of
respondents is adaptive. Health institutions and health
workers should optimize family support to increase
patients’ coping mechanisms.
REFERENCES
Andarmoyo, S. (2012) Keperawatan Keluarga Konsep
Teori, Proses dan Praktik Keperawatan. I. Yogyakarta:
Graha Ilmu.
Atif, M. et al. (2014) ‘Impact of tuberculosis treatment on
health-related quality of life of pulmonary tuberculosis
patients: a follow-up study’, pp. 1–11.
Azizah, L. M., Zainuri, I. and Akbar, A. (2016) Buku Ajar
Keperawatan Kesehatan Jiwa-Teori dan Aplikasi
Praktik Klinik. 1st edn. Yogyakarta: Indomedia
Pustaka.
Azwar (2016) Sikap Manusia (Teori dan Pengukurannya).
Yogyakarta: Pustaka Pelajar.
Caesarena Rianko Putri, M. (2012) ‘Hubungan Antara
Coping Dan Psychological Distress Pada Istri Yang
Mengalami Kekerasan Dalam Rumah Tangga’.
Craig, G. M. et al. (2017) ‘International Journal of
Infectious Diseases Tuberculosis stigma as a social
determinant of health : a systematic mapping review of
research in low incidence countries’, International
Journal of Infectious Diseases. International Society for
Infectious Diseases, 56, pp. 90–100. doi:
10.1016/j.ijid.2016.10.011.
Cremers, A. L. et al. (2015) ‘Assessing the Consequences
of Stigma for Tuberculosis Patients in Urban Zambia’,
113, pp. 1–17. doi: 10.1371/journal.pone.0119861.
Das, S. et al. (2017) ‘Impact of stress, coping , social
support , and resilience of families having children with
autism : A North East India-based study’, Asian Journal
of Psychiatry. Elsevier B.V., 28, pp. 133–139. doi:
10.1016/j.ajp.2017.03.040.
Deshmukh, R. D. et al. (2017) ‘Ac ce cr t’, Indian Journal
of Rheumatology. Tuberculosis Association of India.
doi: 10.1016/j.ijtb.2017.05.003
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
646

Li, C. et al. (2015) ‘European Journal of Oncology Nursing
Social support buffers the effect of self-esteem on
quality of life of early-stage cervical cancer survivors
in Taiwan’, European Journal of Oncology Nursing.
Elsevier Ltd, 19(5), pp. 486–494. doi:
10.1016/j.ejon.2015.02.008.
Monzani, D. et al. (2015) ‘The Situational Version of the
Brief COPE: Dimensionality and Relationships With
Goal-Related Variables The Situational Version of The
Brief COPE’. PsychOpen, a publishing service by
Leibniz Institute for Psychology Information (ZPID),
Trier, Germany (www.zpid.de)., 11(2), pp. 295–310.
doi: 10.5964/ejop. v11i2.935.
Narasimhan, P. et al. (2013) ‘Risk Factors for
Tuberculosis’, p. 11. doi:10.1155/2013/828939
Family Support and Coping Mechanisms in Patients with Pulmonary Tuberculosis
647
