
The Influence of Cognitive Therapy on Quality of Life of
People with Diabetes Melitus
Dwi Heppy Rochmawati
Faculty of Nursing, Sultan Agung Islamic University, Semarang, Central Java, Indonesia
Keywords: Cognitive Therapy, Diabetes Mellitus, Quality of Life.
Abstract: People with diabetes mellitus usually experienced disappointment and anxiety about the disease, causing the
quality of life to decline. The purpose of this study is to describe the results of cognitive therapy on the
quality of life of diabetes mellitus clients. Cognitive Therapy is a form of therapy that can train clients to
change negative ways of thinking due to disappointment and failure so that clients can be better and can be
productive again. Cognitive Therapy is carried out in the form of counseling and is oriented towards
changing negative thoughts into positive ones. This research uses quasi experiment with pre and post test
without control group method, it means that data collection is done before and after intervention with
cognitive therapy. Most of the aged 48-51 years (76%), education (44%) were junior high, female gender
was 13 respondents (52%) and duration> 3 years 10 respondents (40%). Quality of life before therapy
average score 103.96 with positive life quality of 17 respondents (68%). Quality of life after therapy
average score of 111.60 with positive life quality of 22 respondents (88%). There is influence of cognitive
therapy on improving quality of life of people with diabetes mellitus (p-value 0.035).
1 BACKGROUND
Diabetes Mellitus (DM) is one of the non-
communicable diseases whose prevalence is
increasing from year to year. DM is often referred to
as the great imitator, because this disease can affect
all the organs of the body and cause various
complaints. Symptoms vary greatly and can arise
slowly, so patients are not aware of any changes.
Results of basic health research (Riskesdas) in
2013 prevalence of diabetes mellitus in Indonesia
based on interview who was diagnosed with a doctor
by 1.5 percent. Diabetes Mellitus is diagnosed by a
doctor or a symptom of 2.1 percent. The highest
prevalence of diabetes diagnosed by doctors is in DI
Yogyakarta (2.6%), DKI Jakarta (2.5%), North
Sulawesi (2.4%) and East Kalimantan (2.3%). The
prevalence of diabetes diagnosed by doctors or
symptoms is highest in Central Sulawesi (3.7%),
North Sulawesi (3.6%), South Sulawesi (3.4%) and
Nusa Tenggara Timur 3.3%.
Diabetes Mellitus as a chronic illness has
psychological effects such as decreased quality of
life. Psychological conditions are negative if not
done because the treatment will aggravate the
condition of the illness and increase the risk of
death, it can be formulated research problem is to
develop Cognitive Therapy (CT) to improve the
quality of life of Diabetes Mellitus clients.
Cognitive Therapy (CT) is basically used to
change a person's thinking about a problem and this
helps people see the problem in a different and
positive perspective. CT is very popular and is
considered one of the best therapies for many mental
disorders such as obsessive compulsive disorder,
OCD, anxiety, phobia, depression, post traumatic
stress disorder, bulimia and schizophrenia. The
results of Gonzales (2010) study on DM patients
who received CT after treatment showed decreased
severity of depression and increased glycemic
control. Research on the effects of CBT on
depression: the role of problem-solving assessment
conducted by Chen, Jordan, and Thompson (2006)
suggests that CBT improves the ability to solve
problems and reduce depression levels.
2 METHODS
This research uses quasi-experiment with pre-test
and post-test one group method. Population and
648
Rochmawati, D.
The Influence of Cognitive Therapy on Quality of Life of People with Diabetes Melitus.
DOI: 10.5220/0008330306480652
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 648-652
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
samples in this study were all patients with Diabetes
Mellitus which amounted to 54 people. Sampling
using total sampling method. Data collection using
questionnaires and giving intervention in the form of
cognitive therapy, which is a therapy to change the
negative auto mind into positive. The analysis using
a test dependent sample t-test
3 RESULTS
3.1 Respondents’ Characteristics
Based on Table 1, the largest age of respondents in
this study was age 48-51 years, amounting to 29
respondents (53.7%). While at least 40-43 years age
amounted to 10 respondents (18.5%). The most
respondents’ education in this study was graduated
from junior high school as many as 21 respondents
(38.9%) and not school or drop out as much as 6
respondents (11.1%). The most sex group is women
that is 34 respondents (63%). Meanwhile, the male
gender was 20 respondents (37%). Regarding the
duration of the disease, the most respondents
suffered more than 3 years of illness as many as 32
respondents (59.3%) and at least 1 to 2 years of
illness as many as 10 respondents (18.5%).
3.2 Univariate Analysis
3.2.1 Quality of Life
Table 2 shows that respondents who have positive
life quality are 29 respondents (53.7%) and negative
life quality of 25 respondents (46.3%). The table
also shows that respondents who have a positive
quality of life as much as 43 respondents (79.6%)
and negative life quality of 11 respondents (20.4%).
Based on Table 3, it can be concluded that
quality of life pre intervention average score is
103.96 with standard deviation 15.001. The lowest
score was 76 and the highest score was 134. With
95% confidence level, the mean pre life quality
score of pre intervention was between 97.77 and
110.15. While the concept of self-post intervention
average score was 111.60 with a standard deviation
of 12.196. The lowest score was 80 and the highest
score was 132. With a 95% confidence level, the
mean post intervention quality score was 106.57-
116.63.
3.3 Bivariate Analysis
Bivariate analysis will describe whether there is a
difference in quality of life before and after therapy
using a test dependent sample t-test. This bivariate
analysis is performed to prove the hypothesis that
has been formulated.
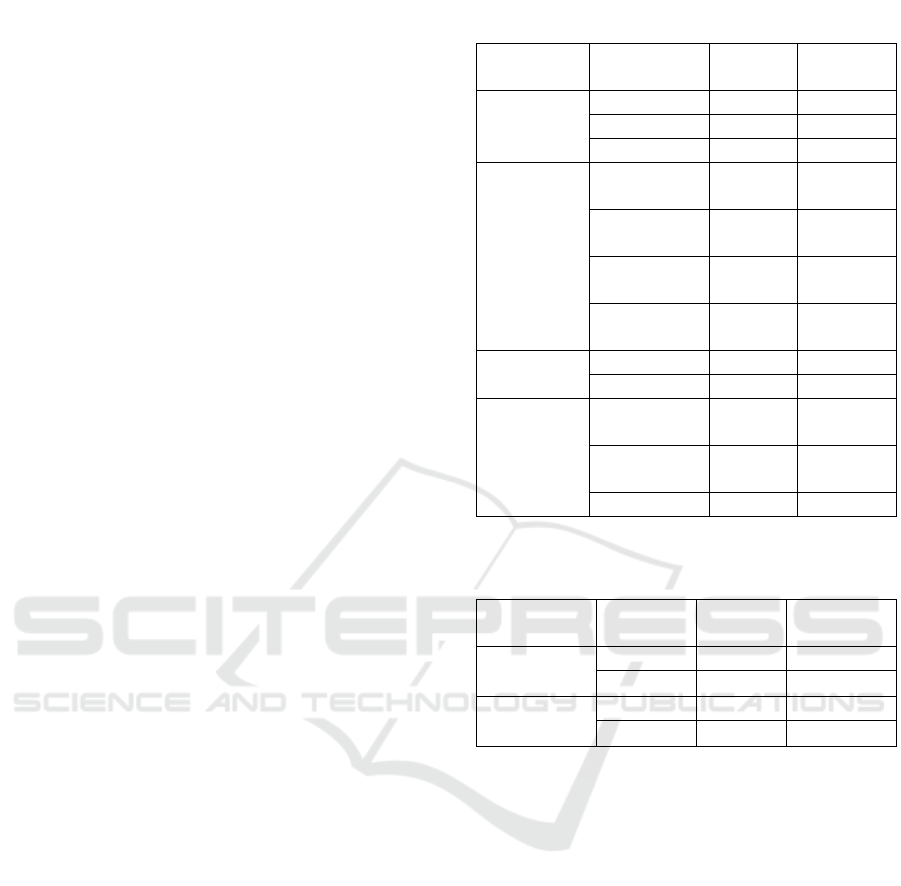
Table 1: Demographic Characteristics (n = 54).
Characteristic
Category
Frequency
Percentage
(%)
Age
40-43
10
18.5
44-47
15
27.8
48-51
29
53.7
Education
No school/
dropout
6
11.1
Elementary
School
13
24.1
Junior High
School
21
38.9
Senior High
School
14
25.9
Sex
Male
20
37.0
Female
34
63.0
Illness
Duration
1 year-2
years
10
18.5
> 2 years-3
years
12
22.2
> 3 years
32
59.3
Table 2: Quality of life data pre and post-test
(n = 54).
Characteristic
Category
Frequency
Percentage
(%)
Pre-Test
Positive
29
53.7
Negative
25
46.3
Post-Test
Positive
43
79.6
Negative
11
20.4
The Influence of Cognitive Therapy on Quality of Life of People with Diabetes Melitus
649
From the results of the analysis using dependent
sample t-test showed that the average score of
quality of life before following the therapy was
103.96 and after following the therapy of 111.60
with a difference of -7.64 means that there is an
increase in quality of life after following therapy
with an average increase of 7.64. The result of
calculating the value of “t” is 2.231 with p-value
0.035 (2-way test) smaller than alpha (0.05) meaning
that there is statistically significant difference
between mean of quality of life score before and
after therapy (Table 4).
4 DISCUSSION
4.1 Age
The results showed that the largest age of
respondents in this study was age 48-51 years,
amounting to 29 respondents (53.7%). While at least
40-43 years age amounted to 10 respondents
(18.5%). Life expectancy from year to year has
increased, in 2010 life expectancy is 67.4 years and
2020 is estimated to be 70.2 years. Based on the
existing results that the increasing age has nothing to
do with quality of life. Negative quality of life that
existed in the respondents due to several factors that
did not participate researched in this study.
4.2 Education
The result of the research shows that most of
respondent's education in this study is graduated
from junior high school as much 21 respondents
(38.9%) and no school / drop out as much as 6
respondents (11.1%). The highest education of
diabetes mellitus is graduated from junior high
school. Patients with diabetes mellitus who
graduated from junior high school experience
confusion in assessing the ability that is in him
because of the limited knowledge received so that
the effect on taking action in the face of illness and
quality of life is also influenced by the ability of his
judgment.
4.3 Sex
The results showed that the largest proportion of
respondents were women. This is in line with the
prevalence that women are twice as likely to have
diabetes mellitus. While the sex does not have a
significant relationship to the quality of life.
4.4 Duration of Illness
The results showed that most respondents suffered
more than 3 years of pain as many as 32 respondents
(59.3%) and at least 1 to 2 years of illness as many
as 10 respondents (18.5%). Long suffering pain
affects the ability of self in determining attitude
when facing suffering (Bastaman, 2007). A positive
quality of life is formed in the sufferer with the
longest illness through self-view and positive
experience. Thus, respondents can define attitudes
and change the idea that there is a wisdom behind
suffering.
4.5 Quality of Life
The results can be seen that most people with
diabetes mellitus have a positive quality of life.
Data obtained from 54 respondents, on the
measurement before the cognitive therapy
intervention, the result of positive quality of life was
29 respondents (53.7%) and the measurement after
the cognitive therapy intervention was found the
result of the positive life quality was 43 respondents
(79.6%).
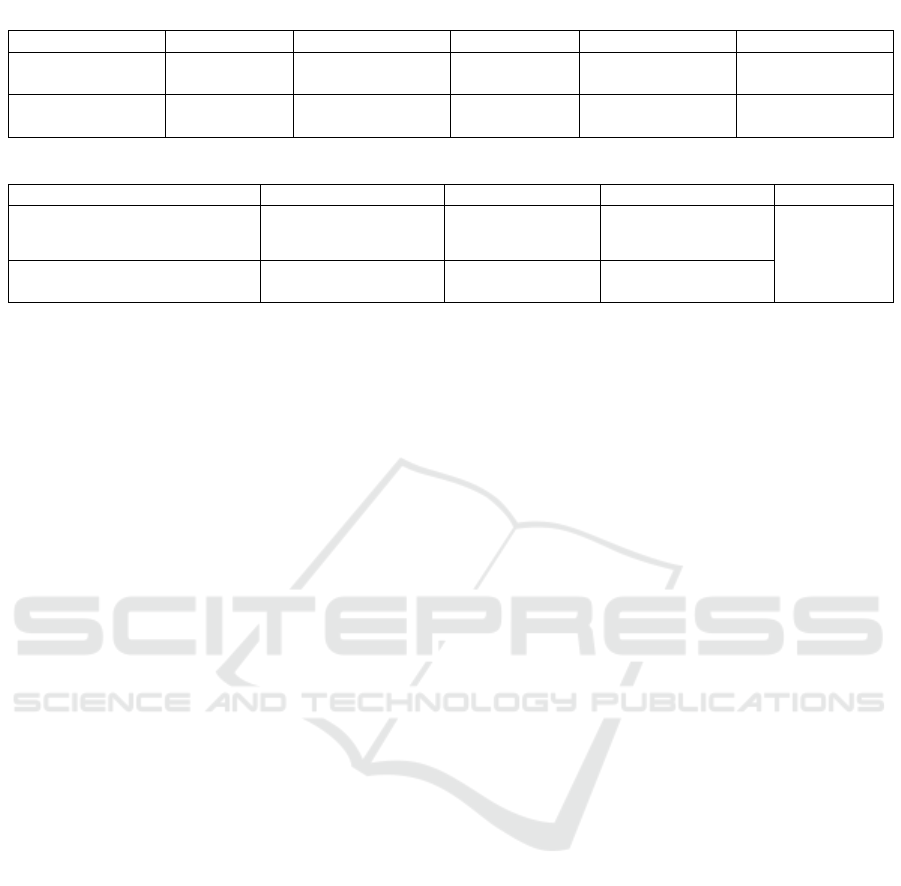
Table 3: Results of quality analysis of pre life and post intervention (n = 54).
Variable
Mean
Median
SD
Min-Max
95 % CI
Quality
of Life
103.96
105.00
15.001
76 – 134
97.77 – 110.15
Quality
of Life
111.60
111.00
12.196
80 – 132
106.57 – 116.63
Table 4: Average quality score distribution before and after following therapy.
Variable
N
Mean
SD
p-value
Quality of Life
Pre Intervention
54
103.96
15.001
0.035
Quality of Life
Post Intervention
54
111.60
12.193
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
650

Respondents who have a positive quality of life
can master new experiences and previous
experiences. Past experiences can affect a person's
quality of life. New experiences are gained when
individuals interact with their new surroundings
(Perry & Potter, 2009 and Alimul, 2006). Quality of
life is formed because there is a feeling of being
able to do something, personal and interpersonal
relationships, personal characteristics that affect
self-expectations and a stable self-realization can
lead to the purpose of adult development (Perry &
Potter, 2009).
4.6 Effect of Cognitive Therapy on the
Quality of Life of Diabetes Mellitus
Based on the results of the study, the analysis using
the dependent sample test showed that the average
self-concept score before following the therapy was
103.96 and after following the therapy of 111.60
with a difference of -7.64 means that there is
improvement of quality of life after following
therapy with average increase of 7.64. The result of
calculating the value of "t" is 2.231 with p-value
0.035 (2-way test) smaller than alpha (0.05)
meaning that there is statistically significant
difference between mean of quality of life score
before and after therapy.
According to the above calculation results,
statistically giving intervention has an effect on
quality of life. There is improved quality of life
before and after therapy. Quality of positive life
indicates the existence of self-acceptance where
individuals with a positive quality of life know
themselves well. Individuals who have a positive
quality of life can understand and accept a number
of facts about him so that the evaluation of yourself
to be positive and can accept themselves as they are.
Individuals who have a positive quality of life will
design goals that are in accordance with reality, that
is, goals that are likely to be achieved, able to face
the future life and assume that life is a process of
discovery.
5 CONCLUSIONS
This study concludes that cognitive therapy has
effect to the quality of life of people with diabetes
mellitus.
Regarding the recommendation, professional
nurse who has a particular scientific specialization
should be able to apply the knowledge and ability to
utilize the knowledge held in order to support the
successful development of the profession. The
giving of soul-nursing specialist therapies to be
more activated both in the area of healthy mental
nursing, nursing risk of mental problems and mental
nursing care area. The results of this study can be
used as basic data for researchers and further
research. For further research can develop some
methods and types of research on cognitive therapy
with different areas and respondents. For
educational institutions to provide more
opportunities to researchers in order to develop
science. Families and communities should be aware
that their role in assisting and caring for clients is
necessary. Continuous psychic and moral support
greatly determines the client's health and compliance
in medication and diet.
ACKNOWLEDGEMENTS
Rector of Sultan Agung Islamic University of
Semarang. Research Institute and Community
Service Islamic University of Sultan Agung
Semarang. Dean of the Faculty of Nursing
Universitas Islam Sultan Agung Semarang. All
Fellow Lecturers and Employees in S1 Nursing
Study Program Faculty of Nursing University of
Islamic University of Sultan Agung Semarang. The
whole family is especially parents, husband and
beloved children, who have provided motivation and
support throughout the process. All respondents,
families of respondents and related parties in taking
this research data. All parties involved in the
preparation of this research proposal, which cannot
authors mention one by one.
REFERENCES
Agustiani, D. H. (2009). Psikologi Perkembangan.
Bandung: Refika Aditama.
Badan Pusat Statistik. (2010). Profil Kriminalitas
Remaja.http://www.bps.go.id/hasil_publikasi/flip_201
1/4401003/files/search/searchtext.xml. dperoleh 14
Januari 2013.
Bastaman, H. D. (2007). Logoterapi : Psikologi untuk
Menemukan Makna Hidup dan Meraih Hidup
Bermakna. Jakarta: PT. Grafindo Persada.
Dahlan, M. S. (2011). Statistik untuk Kedokteran dan
Kesehatan : Deskriptif, Bivariat, dan Multivariat
dilengkapi Aplikasi dengan Menggunakan SPSS.
Jakarta: Salemba Medika.
Frankl, V. E. (1963). Man's Search for Meaning: An
Introduction to Logotherapy. New York: Washington
The Influence of Cognitive Therapy on Quality of Life of People with Diabetes Melitus
651

Square Press. (Earlier title, 1959: From Death-Camp
to Existentialism. Originally published in 1946 as Ein
Psycholog erlebt das Konzentrationslager), diperoleh
tanggal 8 Februari 2013.
Kartono, D. K. (2011). Patologi Sosial 2 : Kenakalan
Remaja. Jakarta: PT. Raja Grafindo Persada.
Keliat, B.A., & Yosep. (2010). Keperawatan Jiwa.
Bandung: Refika Aditama.
Kemenkes RI. (2010). Pedoman Umum Perlindungan
Kesehatan Anak Berkebutuhan Khusus.
http://kemenkes.go.id/2010/Pedoman-Umum-
Perlindungan-Kesehatan-Anak-Berkebutuhan-
Khusus/. Diperoleh 19 Januari 2013.
Mazaya, K.N. & Supradewi, R. (2011). Konsep Diri dan
Kebermaknaan Hidup Pada Remaja di Panti Asuhan.
Proyeksi, Vol. 6, 103-112
Ndoen, L.F. (2010). Jurnal Pengungkapan Pada Mantan
Narapidana. Fakultas Psikologi Universitas
Gunadarma.
Nisfulaili, Y. (2010). Hubungan Antara Konsep Diri dan
Kebermaknaan Hidup Kaum Waria di IWAMA (Ikatan
Waria Malang). http://lib.uin-
malang.ac.id/thesis/fullchapter/05410021-yulia-
nisfulaili.ps. Diperoleh 12 Februari 2013.
Sitohang, N. W. (2009). Makna Hidup Pada Remaja Putri
Pengguna NAPZA di Lembaga Pemasyarakatan II A
Palembang. Palembang : Fakultas Psikologi
Universitas Gunadarma
Tridhonanto, A. &. (2010). Meraih Sukses dengan
Kecerdasan Emosional. Jakarta: Elex Media
Komputindo.
Wong, D. L., & et.all. (2009). Buku Ajar Keperawatan
Pediatrik edisi 6 volume 1. Jakarta: EGC Penerbit
Buku Kedokteran.
Widianita, P. L., Mikarsa, L. H. & Hartiani, F. (2009).
Gambaran Makna Hidup Remaja Penderita Leukimia.
Indonesian Journal of Cancer. Jakarta : Fakultas
Psikologi Universitas Indonesia
Yulianti, S. A., & Widiasih, R. (2009). Gambaran
Orientasi Masa Depan Narapidana Remaja Sebelum
dan Setelah Pelatihan di Rumah Tahanan Negara
Kelas I Bandung. Volume 10, Nomor XXI, halaman
103. Diunduh 19 November 2012.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
652
