
Understanding Pediatric HIV Care Management to Improve the
Quality of Care for Children Infected with HIV in Indonesia
Nuzul Qur’aniati
1
, Linda Sweet
2
, Dean Whitehead
2
, and Alison Hutton
2
1
Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia 60115
2
Flinders University, Adelaide, South Australia, Australia
Keywords: Care Management, Children, HIV.
Abstract: The number of children infected with the Human Immunodeficiency Virus (HIV) has cumulatively increased
by 68.5% during the period 2010 to 2015 in Indonesia. Due to the need for lifelong treatment to minimize its
impact, HIV is considered a chronic disease. With the change to living with a chronic condition, children with
HIV may need to receive coordinated care management across the spectrum of their disease from health
professionals, and, particularly, nurses. Studies from sub-Saharan countries have shown several programs that
have been implemented to manage childhood HIV epidemics. However, gaps in the implementation of
programs still exists, due to family contexts, disclosure of HIV status, stigma, discrimination, and health
professional capacities. This presentation will describe the programs for the provision of care for HIV infected
children in sub-Saharan Africa and their identified barriers and challenges. From the review findings, future
research will be proposed for which similar advances can be implemented in Indonesia as part of improving
the quality of care for HIV positive children.
1 BACKGROUND
The number of children living with the Human
Immunodeficiency Virus (HIV) is becoming more
prevalent. In 2013, almost 190,000 children and
adolescents, infected with HIV, lived in the Asia
region (Saad, Peck-LeongTan, & Subramaniam
2015). Globally, in 2015, the United Nations Program
on HIV/AIDS (UNAIDS) estimated 1.8 million
children aged under 15 years old were living with
HIV, 400 children become newly infected daily, and
110,000 children were died from Acquired Immune
Deficiency Syndrome (AIDS)-related diseases
(UNAIDS 2016a). The report from Global AIDS in
2014 stated that 4.9 million people were living with
HIV, with Indonesia ranked third highest (14%) after
India (43%), and China (17%) (WHO 2016). In
Indonesia, new infections of HIV among children
(10–14 years old) have increased by 63% since 2010
(UNAIDS 2016a). The report by the Ministry of
Health stated that the number of children infected
with HIV aged below 19 years had cumulatively
increased from 1,472 in 2011 to 2,252 in 2015 (MoH
2016).
For children living with HIV (CLWH), their lives
are negatively affected, so they may need to receive
coordinated care management across the spectrum of
their disease from health professionals, nurses, in
particular. Rochat, Mitchell and Richter (2008)
indicate that CLWH have complex problems related
to the biological, psychological, social, economic,
and environmental conditions in their lives and have
difficulty accessing healthcare services. For example,
hospitalized children with HIV are susceptible to
discomfort and stressful economic and social
circumstances with their disease, stigma regarding
HIV, over-burdened hospital facilities, and a lack of
specialized staff on the ward (Richter, Chandan &
Rochat 2009). On the other hand, numerous studies in
a sub-Saharan context have discussed how to manage
HIV epidemics for CLWH (Achema & Ncama, 2016;
Luyirika et al., 2013; Mbaye et al., 2009). Therefore,
this paper aims to describe the provision of care for
HIV-infected children and their identified barriers
and challenges. Furthermore, potential future
research in Indonesia will be outlined to improve the
life quality of children who are HIV positive.
Qur’aniati, N., Sweet, L., Whitehead, D. and Hutton, A.
Understanding Pediatric HIV Care Management to Improve the Quality of Care for Children Infected with HIV in Indonesia.
DOI: 10.5220/0008331507070711
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 707-711
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
707

2 METHODS
This study utilized an integrative review. This review
focused on the provision of care for CLWH
manuscripts published between 2009 and 2016.
Manuscripts were identified using the following
databases: Medline OVID, PsycInfo, Sage Informit,
Google Scholar, and Taylor & Francis online. The
search options used were Boolean/ phrase and smart
text searching with a combination of the following
key words: child or children or childhood or pediatric,
nurse or nurses or nursing, holistic or psychosocial or
social or patient-centered care, HIV, and hospital.
Narrower searches resulted in fewer reports. The
author then extended the key words: children, HIV,
comprehensive care. The author obtained 110
articles, and this was condensed to 11 primary
research manuscripts according to the inclusion
criteria: written in English and discussed the
provision of care for children with HIV. Most
manuscripts were found using Google Scholar and
Taylor & Francis online. Initially, the author wrote a
synopsis of each article onto a table containing the
author(s), year and location, research questions and
the aim of study, methodological design, and major
findings and then continued with the critical appraisal
process for quantitative and qualitative manuscripts.
3 RESULTS
Of the 11 included manuscripts, the results were
grouped into two over-arching themes: the provision
of care for HIV infected children and identified
barriers and facilitators to healthcare.
3.1 The Provision of Care for HIV-
Infected Children
Children infected with HIV require comprehensive
care, which does not only require access to
antiretroviral therapy (ART), but also to supportive
care to ensure they meet their optimal quality of life.
3.1.1 Access to Antiretroviral Therapy
(ART)
Access to ART crucially reduces children’s
morbidity and mortality. UNAIDS (2016) found that
access for children (aged 0–14) to ART increased
dramatically from 0% in 2000 to 50% in 2005.
However, according to the UNICEF (2016) report, of
1.8 million children under the age of 15 living with
HIV, only half were receiving treatment. A study
from the South Asia region comprising Afghanistan,
Bangladesh, Bhutan, India, Maldives, Nepal,
Pakistan, and Sri Lanka argues that the uses of text
messaging gateways for medical appointments and
ARV pick-ups are alternative strategies implemented
to support therapy adherence for CLWH.
3.1.2 Supportive Care
Children with HIV not only need ART, but also
require supportive care. This is an important finding
and according to Achema and Ncama (2016) holistic
supportive care, including nutritional, educational,
and psychosocial support given by families,
caregivers, and nurses is essential for CLWH to
support the achievement of a better quality life. As
well as nutritional, educational and psychosocial
support, sexual reproductive health and circumcision
positively prevent children from HIV transmission.
Children with HIV require education for
awareness and reproductive health to prevent
themselves from HIV or other sexually transmitted
infections (STs) before they become sexually active.
A qualitative study in South Africa found that young
children aged 10–14 years did not have adequate
knowledge about sexual and reproductive health
(Vujovic et al., 2014). Vujovic et al. (2014) state that
sexual and reproductive programs for adolescents are
rare. Within the same literature, children reported that
they needed separate clinics to adults, so they can ask
about physical development, condom use, pregnancy
and how to avoid pregnancy, menstruation, and
hygiene (Vujovic et al., 2014). Besides condom and
contraceptive injections being available from the
health service, children also said that they needed
friendly health providers with whom they could talk
comfortably (Vujovic et al., 2014).
Male circumcision is another cost-effective form
of supportive care, which effectively reduces the risk
of sexual transmission from males to females.
Modeling studies (2009–2011) from 14 countries:
Botswana, Ethiopia, Kenya, Lesoto, Malawi,
Mozambique, Namibia, Rwanda, South Africa,
Swaziland, Uganda, The United Republic of
Tanzania, Zambia, and Zimbabwe found that 80% of
males aged 15–49 were circumcised, which prevented
the occurrence of new HIV infections by 3.4 million
(Sgaier et al., 2014). Within 15 years, male
circumcision saved up to US$ 16.5 billion (Sgaier et
al., 2014). Therefore, the voluntary male
circumcision program can be part of the HIV
prevention strategy. To implement the program,
circumcision training for health professionals or
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
708
providing health education for families requires
management. For example, nurses in 15 priority
countries such as Sudan have been trained to provide
voluntary male circumcision services (UNAIDS
2016b).
3.2 Barriers and Facilitators to
Healthcare
As well as the provision of care, the implementation
of care for HIV positive children have barriers and
facilitators, including low socio-economic and
parental education, disclosure of HIV status, stigma
and discrimination, and health professional
capacities.
3.2.1 Low Socio-Economics and Lack of
Parental Education
Low socio-economics (LSEs) and lack of parental
education are barriers to healthcare seeking behavior.
McGrantham-Mc Gregor et al. (2007) cited in Rochat
et al. (2008) stated that poverty in sub-Saharan Africa
was a platform for HIV and AIDS, which were linked
to malnourishment, poorly developed health and
education, and a distressed care environment,
requiring attention. This information is consistent
with known facts from sub-Saharan Africa, where it
is reported that adolescent girls face higher risk of
HIV infection due to their life circumstances, i.e.
living in poverty, malnourishment, LSE problems,
and poor-quality education (UNICEF 2016b).
Moreover, poverty, economic problems, and large
family size contributed to dangerous survival
strategies such as transactional sex, and children’s
insecurities such as food, shelter, school fees, and
other school supplies (Betancourt et al., 2012).
Kidman and Heymann (2016) support that aspects of
vulnerability of HIV-experienced caregivers and
children infected with HIV are linked to poverty, food
insecurity, inability access to school, ill health, and
limited access to safety. Therefore, strengthening
economic problems and developing family health
education are important to ensure adequate care for
children with HIV. Betancourt et al. (2012) assert that
providing financial assistance positively supports
vulnerable children and their families.
3.2.2 Disclosure of HIV Status
Disclosure of HIV status is a big challenge and still
exists. In 2016, most people living with HIV
(PLWHA) did not know their status (UNAIDS
2016a). As stated in UNAIDS (2016b), 14.5 million
out of the 36.7 million people living with HIV do not
know their status. Parents or caregivers tend to silence
and protect their children from their status. This
mystifies their transition into adolescence (Bernays et
al., 2014). However, Bostwana has developed the
disclosure model as part of Botswana’s National HIV
care and treatment guidelines. The program provides
a friendly, supportive environment building on
positive living with HIV, based on a counseling
approach at regular clinic visits and adherence classes
(Lowenthal et al., 2014). The adherence classes are a
group learning session for children who initiate and
start taking antiretroviral drugs assisted by clinic
nurses (Lowenthal et al., 2014) so could enhance
adherence of therapy.
3.2.3 Stigma and Discrimination
Stigma and discrimination negatively impact
healthcare outcomes for CLWH. Stigma touches on
the loss of dignity leading to difficulties in epidemic
control (Indonesia, 2012). For example, the loss of
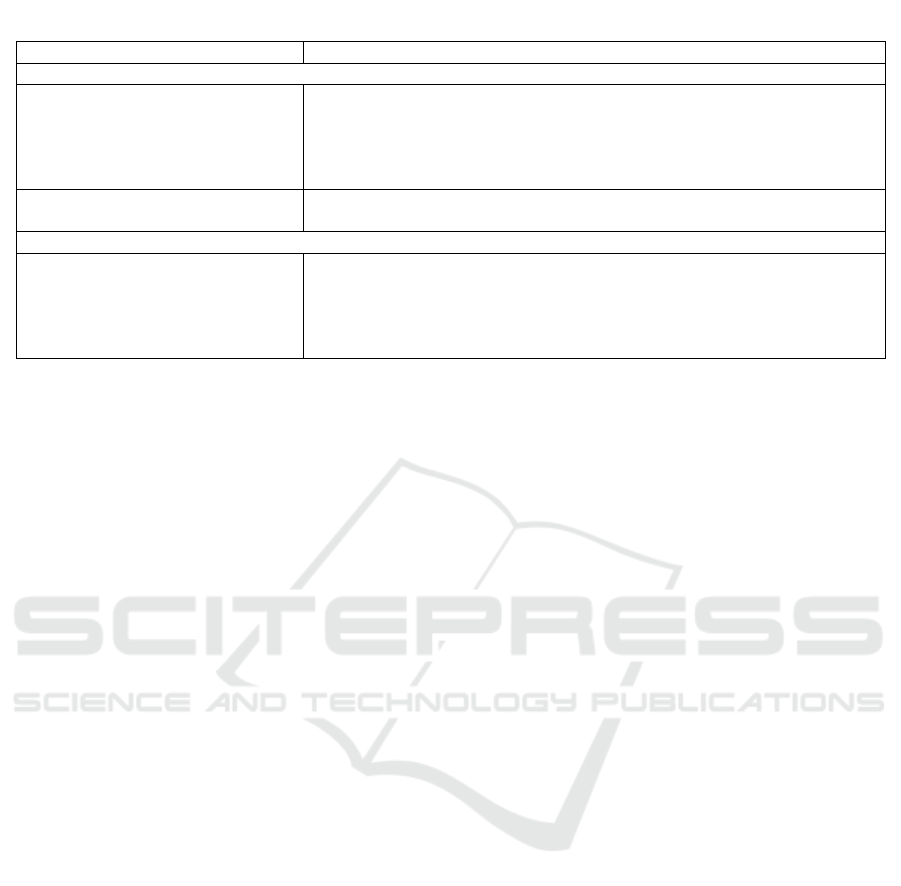
Table 1: The gaps for future implementation of research into the provision of care for CLWH in Indonesia.
Research Findings
Potential Research Topics in Indonesia
Key Performance: Access to ART: comprehensive sexual and reproductive health
Children have less knowledge on
sexual and reproductive health;
voluntary male circumcision is an
effective program for HIV
prevention.
Improving sexual and reproductive health for CLWH (practice, barriers and
challenges; strategies to enhance the practice; building knowledge of CLWH;
developing strategies to implement the practice for nurses); transition care for
young children.
Text messaging for ARV pick-up is
effective
How is adherence therapy conducted for CLWH? Strategies to engage
children and families to improve ARV.
Key Performance: Caregiving and HIV
Disclosure model with honest
communication from Botswana
improves the quality care of CLWH
Evaluate the implementation of disclosure status (e.g. barriers and
facilitators); assessing the knowledge and behaviour of health care towards
disclosure-status; strategy to improve the readiness of disclosure (e.g.
communication, model delivery of care); the role of the government in the
support of disclosure due to the implemented decentralization approach.
Understanding Pediatric HIV Care Management to Improve the Quality of Care for Children Infected with HIV in Indonesia
709

education opportunities, denying healthcare, taking
medication secretly, increasing psychological
problems, and less up-take on adherence therapy
(Bernays et al., 2014; Gokengin et al., 2016;
Indonesia, 2012; UN, 2015; Wei et al., 2016).
3.2.4 Health Professionals’ Capacities
The capacities of health professionals positively
support better quality of care for children with HIV.
However, two studies report that the implementation
of HIV care has challenges related to limited health
professional capacities, such as limited training,
providing poor counseling, a lack of referral system
management, faking information on medical records,
and poor logistic management (Adebimpe, 2013).
Furthermore, nurses are more likely to focus on
routines, rules, protocol, and become rigid to cope
with increasing burdens and limited resources
(Richter et al., 2012). Health professionals (nursing,
specialist pediatric training) are unwilling to work
with caregivers and children due to the stress of care
delivery in the wards (Richter et al., 2012). Hence,
hospital bureaucracy, resources, staff rotation, and
nursing shortages give caregivers an imperatively
pivotal role in their children’s care but participate
very little (Richter, Chandan, & Rochat, 2009).
4 DISCUSSIONS
Disseminating results from this review shows a that a
high burden on CLWH still exists. This review
identifies that family context, disclosure of HIV
status, stigma and discrimination, and health
professional practice negatively affect the care of
HIV positive children. CLWH depend on their
families. Since lack of parental education is one of the
barriers to care-seeking behavior, building the
knowledge of caregivers is operationally strategic to
support the quality of care for HIV positive children,
including providing treatment and medicine,
nutrition, and psychosocial care in the home.
Additionally, discussing disclosure of HIV status
within the family is an important factor to support the
effectiveness of treatment. UNICEF (2016c) stated
that disclosure of HIV status requires good and
accurate communication among children, caregivers,
and health providers (UNICEF 2016c). Furthermore,
UNICEF (2016c) stated that CLWH who experienced
stigma, discrimination, and other psychosocial
circumstances need to be empowered to improve HIV
outcomes and to enhance child protection. Lessons
learned from current practice in child protection
reported by UNICEF (2016a) determined that: (1) a
comprehensive framework integrating multi sector's
collaboration will enable positive outcomes on
infected CLWH protection; and (2) empowering
children in all programs will provide better
understanding on their barriers and challenges to
reduce stigma and discrimination. Key lessons from
UNICEF postulate future activities for increasing
girl’s access in secondary education besides
conveying proven programs, for example,
community empowerment, reducing stigma,
discrimination, and marginalization into healthcare
settings.
CLWH do not only require adherence of therapy but
also supportive intervention. However, it is evident in
this review that the capacities of health providers and
the healthcare system are still not optimal as limited
knowledge and skills are indicated along with limited
resources, shortages of nurses, and a poor healthcare
system. It is clear from this review that it is important
to build the capacity of health providers in terms of
providing adequate knowledge such as sexual and
reproduction health for young children and teenagers.
Therefore, this review provided lessons learned from
sub-Saharan experiences, which informed what is
known and what is not known about the provision of
care for CLWH as listed in Table 1. These gaps may
promote or generate a future research project in
Indonesia.
5 CONCLUSIONS
In summary, CLWH experienced barriers when
seeking healthcare. Firstly, CLWH were living in
poverty, which contributed to lack of nutrition,
minimal access to school, growth, and developmental
problems. Secondly, CLWH experience stigma,
discrimination, and disclosure problems, negatively
affecting their health outcomes. Due to existing
problems, CLWH do not only require ART but also
need supportive care. Moreover, health professionals
should have good capacities to support children with
HIV. Therefore, critical action is needed to ensure
that health providers provide good care, support, and
treatment for both children infected with HIV and
their caregivers.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
710

REFERENCES
Achema, G & Ncama, BP 2016, 'Analyzing Empathic-
Supportive Care Given to Children Living with HIV in
Nigeria', J Assoc Nurses AIDS Care.
Adebimpe, WO 2013, 'Challenge facing early infant
diagnosis of HIV among infants in resource poor
setting', African Journal of Reproductive Health, vol.
17, no. 1, pp. 122-9.
Bernays, S, Jarrett, P, Kranzer, K & Ferrand, RA 2014,
'Children growing up with HIV infection: the
responsibility of success', The Lancet, vol. 383, no.
9925, pp. 1355-7.
Betancourt, TS, Williams, TP, Kellner, SE, Gebre-Medhin,
J, Hann, K & Kayiteshonga, Y 2012, 'Interrelatedness
of child health, protection and well-being: an
application of the SAFE model in Rwanda', Soc Sci
Med, vol. 74, no. 10, pp. 1504-11.
Gokengin, D, Doroudi, F, Tohme, J, Collins, B & Madani,
N 2016, 'HIV/AIDS: trends in the Middle East and
North Africa region', Int J Infect Dis, vol. 44, pp. 66-73.
Indonesia, U 2012, Ringkasan kajian respon terhadap HIV
& AIDS.
Kidman, R & Heymann, J 2016, 'Caregiver supportive
policies to improve child outcomes in the wake of the
HIV/AIDS epidemic: an analysis of the gap between
what is needed and what is available in 25 high
prevalence countries', AIDS Care, vol. 28 Suppl 2, pp.
142-52.
Lowenthal, ED, Jibril, HB, Sechele, ML, Mathuba, K,
Tshume, O & Anabwani, GM 2014, 'Disclosure of HIV
status to HIV-infected children in a large African
treatment center: Lessons learned in Botswana',
Children and Youth Services Review, vol. 45, pp. 143-
9.
Luyirika, E, Towle, MS, Achan, J, Muhangi, J, Senyimba,
C, Lule, F & Muh, L 2013, 'Scaling up paediatric HIV
care with an integrated, family-centred approach: an
observational case study from Uganda', PLoS One, vol.
8, no. 8, p. e69548.
Mbaye, N, Rosenberg, A, Diouf, S, Diouf, M,
Ntumbanzondo, M, Ndiour, A, Diouf, O, Ouattara, AK,
Ouattara, Y, Boussari, L & Hartwig, KA 2009,
'Providing comprehensive care to children living with
human immunodeficiency virus in Senegal', Vulnerable
Child Youth Stud, vol. 4, no. 4, pp. 353-60.
MoH 2016, Laporan Perkembangan HIV Triwulan IV
Tahun 2015, by MoH, Direktorat Jenderal Pencegahan
dan Pengendalian Penyakit Kementerian Kesehatan.
Richter, L, Chandan, U & Rochat, T 2009, 'Improving
hospital care for young children in the context of
HIV/AIDS and poverty', J Child Health Care, vol. 13,
no. 3, pp. 198-211.
Richter, LM, Rochat, TJ, Hsiao, C & Zuma, TH 2012,
'Evaluation of a Brief Intervention to Improve the
Nursing Care of Young Children in a High HIV and
AIDS Setting', Nurs Res Pract, vol. 2012, p. 647182.
Do Health 2008, The psychological,social and development
needs of babies and young children and their caregivers
living with hiv and aids, by Rochat, T, Mitchell, C &
Richter, L.
Saad, BM, Peck-LeongTan & Subramaniam, G 2015,
'ASLI QoL2014 (Annual Serial Landmark International
Conference on Quality of Life) / AQoL 2014 Istanbul
(ABRA International Conference on Quality of Life),
Istanbul Technical University, Istanbul, Turkey, 26 - 28
December 2014Implication of HIV/AIDS Knowledge
on Quality of Life of Young Women in Malaysia',
Procedia - Social and Behavioral Sciences, vol. 202, pp.
218-26.
Sgaier, SK, Reed, JB, Thomas, A & Njeuhmeli, E 2014,
'Achieving the HIV Prevention Impact of Voluntary
Medical Male Circumcision: Lessons and Challenges
for Managing Programs', PLOS Medicine, vol. 11, no.
5, pp. 1-9.
UN 2015, Future of the AIDS response: building on past
achievements and accelerating progress to end the
AIDS epidemic by 2030, by UN, United Nations.
UNAIDS 2016a, Children and HIV Fact Sheet, by
UNAIDS.
UNAIDS 2016b, Prevention gap report UNAIDS.
UNICEF 2016a, Building HIV sensitive social protection
systems through the Cash Plus Care model: findings
from east and sothern Africa.
UNICEF 2016b, Children AIDS.
UNICEF 2016c, 'Protection and Resilience: A simple
checklist for why, where and how to coordinate HIV
and child protection policy and programming', pp. 1-12.
Vujovic, M, HelenStruthers, Meyersfeld, S, Dlamini, K &
Mabizela, N 2014, 'Addressing the sexual and
reproductive health needs of young adolescents living
with HIV in South Africa', Children and Youth Services
Review, vol. 45, pp. 122-8.
Wei, W, Li, X, Harrison, S, Zhao, J & Zhao, G 2016, 'The
relationships between HIV stigma, emotional status,
and emotional regulation among HIV-affected children
in rural China', AIDS Care, vol. 28 Suppl 2, pp. 161-7.
WHO 2016, Biregional Expert Consultation on Advancing
Implementation Research on HIV/AIDS in Asia,
Regional Office For The Western Pacific World Health
Organization, Manila, Philippines.
Understanding Pediatric HIV Care Management to Improve the Quality of Care for Children Infected with HIV in Indonesia
711
