
Early Breastfeeding in Post-Section Birth
Sestu Retno D.A
1
, Niken Grah Prihartanti
2
and Musafa’ah
1
1
Bachelor Nursing Departement of STIKES Pemkab Jombang
2
Midwifery Departement of STIKES Pemkab Jombang
Keywords: Early Breastfeeding, Cesarean Section, Infant, Health Provider.
Abstract: Early Initiation of Breastfeeding process on cesarean section (c-section) laboring are rarely implemented. The
purpose of study was to know the factors that influence the implementation of early breastfeed of post c-
section. This study was an analytical research with cross sectional design. The sample as many as 32 collected
by consecutive sampling technique. The research variables were the factor of mother, father, infant, provider
and the implementation of early breatfeed factor. Data were collected by questionnaires and observation sheets
and analyzed by logistic regression. There were two variables (the factor of infant and provider) which gained
value of λ = > 1.96. the c-sectionore of p value < 0.05. It means, the factor of infant and provider were
significant influence to the implementation of early breastfeed. From both factors, the most influence factor
was provider which is the most expected c-sectionore (B) as many as 54,273. Research conclude that there
are two factors that contribute post c-section breastfeeding, infant factor and provider factor (nurses and
midwives). Provider factor is the most dominant factor that influence to the implementation of early
breastfeed. Guiding and counseling is needed for mother who had c-section in order to complete the
implementation of early breastfeed.
1 BACKGROUND
The implementation of early breastfeed was
influenced by the labouring method. The cesarean
section (c-section) needs a long recovering that the
normal labroing. Baby who was born by c-section
will different stayed with her mother, because her
mother still in recovery room after the anasthetic
process.
A preliminary study conducted at RSUD Jombang
during the year 2012 at RSUD Jombang there were
317 spontaneous childbirth and 3,566 abnormal
laboring, between abnormal labor is delivery with c-
section, with amount 971 (27%). All patients post
sectio secaria do not do IMD. This causes delays in
bonding, mother skin contact with infants (McLeroy,
Bibeau, Steckler, & Glanz, 1988).
On the theory, factor which influence post c-
section early breastfeeding is pain condition of the
post c-section mother (Padmavathi, Jayadeepa, &
Babu, 2014). But actually, pain condition of the
mother has been eliminated by anesthesia effect.
Based on the above background, the researcher is
interested in conducting research on an analysis factor
which influence early breastfeed to post c-section
mother. This study examined the effect of micro
systems that include: mother, father (husband), infant
and provider to the implementation of early
breastfeed.
2 METHODS
This study was an analytical research with cross
sectional design, in which the variable of cause and
effect which was measured in the same time
(Supriyanto & Djohan, 2011). The type of study with
observational explanative approach in order to collect
data of respondent to answer the strategic issues that
were happening, which caused post c-section mothers
that did not implement of early breastfeed. The
population of this study was all post-c-section
patients treated in the Jombang Junior Hospital in
February-May 2017. The number of patients in
February - May 2017 who got c-section at Jombang
General Hospital was 119 mothers.
The samples in this study were patients who got
inclusion and exclusion criteria. Inclusion criteria
were gestational age >37 weeks, mother with sub-
arachnoid block anesthesia, the nipple protrudes, c-
712
D.A., S., Prihartanti, N. and Musafa’ah, .
Early Breastfeeding in Post-Section Birth.
DOI: 10.5220/0008331607120716
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 712-716
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
section indications were not due to pre-eclampsia/
Eclampsia, cardiac abnormalities, asthma, or infants
in secondary arrest. Exclusion criteria were infants
with congenital abnormalities, infants was born
unstable, mother with complications c-section.
From the result of calculation formula, it was
found that 24 respondents, with calculated the drop
out case as many as 20%, it was determined the
number of samples for this study were 32
respondents. Sampling was used by simple random
sampling. Instruments used to collect data in this
study were questionnaires and observation sheets.
Questionnaires distributed personally to each post c-
section mother.
The data were presented in the form of
distribution tables and their intrepretations. Structural
model analysis aimed to examine the effect of the
correlation between exogenous factors on
endogenous factors. The influence of the correlation
had a coefficient value; because it was structural then
the coefficient value was then known as path
coefficient. The path coefficient in the structural
model was called Inner Weigth which was shown
from the coefficient of structural path. The first step
of structural model analysis used to examine the
correlation between exogenous factors to endogenous
factors.
The hypothesis assumption was proved by testing
the significance of the path (path significance).
Pathway significance test aimed to examine the
significance of exogenous factors which influence
endogenous factors. The formed value of the test used
the t-test, comparing the t statistics of the inner model
with t table. If the value of t statistics > t table then
concluded there was a significant influence of
exogenous factors on endogenous factors. With two-
tailed test and using the fault tolerance level α = 2.5%,
the value of t table = 1.96.
Multivariate analysis test used in this study was
logistic regeresi test. Logistic regression aimed to
obtain the best model in determining the determinants
of factors that affect the implementation of early
breastfeed in post c-section mothers in RSUD
Jombang. In this modeling all candidate variables
were tested together. Model selection was done
hierarchically by means of all independent variables
incorporated into the model, and then the non-
significant variable was removed from the model in a
sequence starting from its largest p-wald value.
3 RESULTS
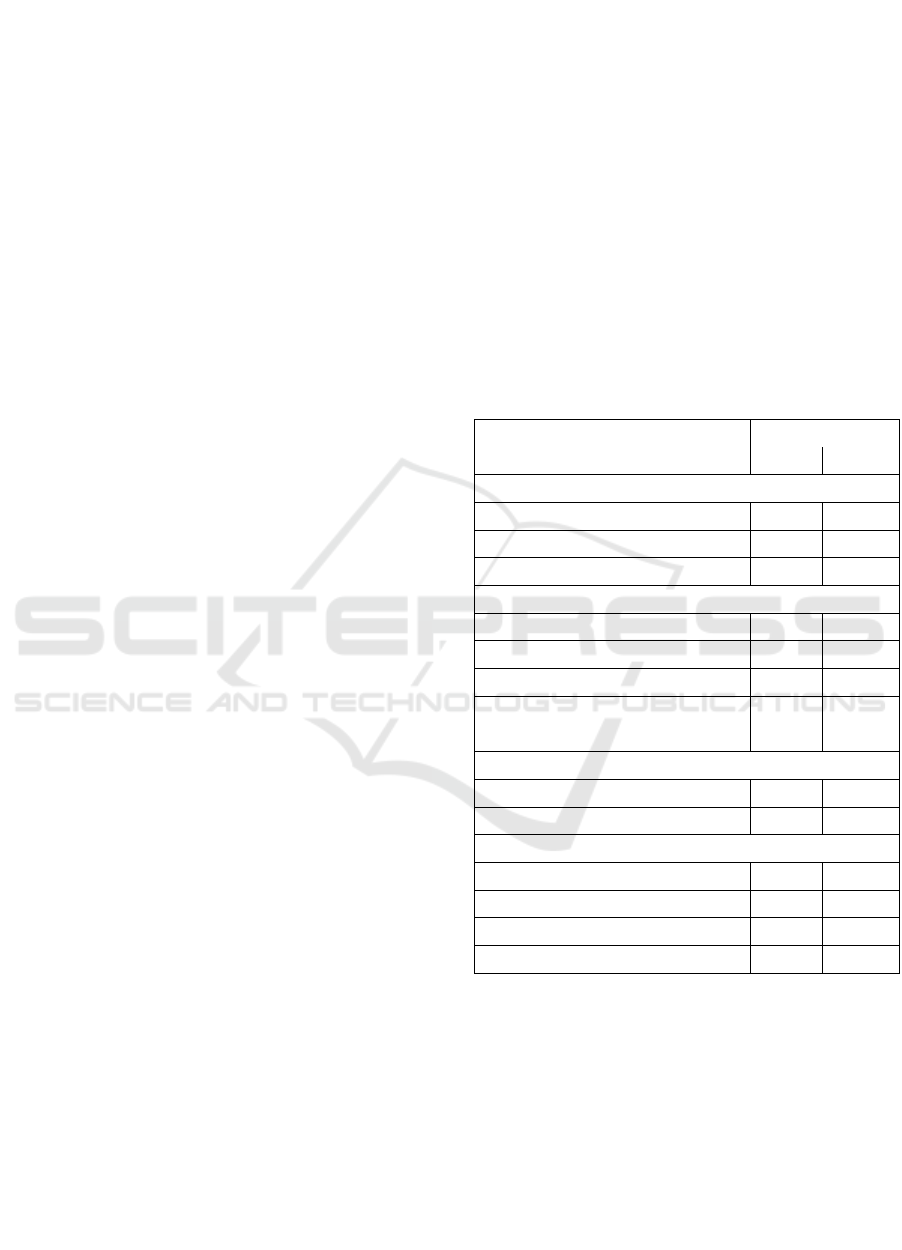
Table 1 describe the characteristics of respondents:
education, the majority of respondents education was
senior high school with a percentage of 59.6%. Most
of respondents work as housewives with percentage
of 57.9%. Then, private employments as many as
28.1% and least 3.1% as farmers. Information about
c-section delivery based on the above table, it was
known that the majority of respondents have received
information about the birth of the c-section as many
as 71.8%. While those who had never received
information about c-section delivery as many as
28.1%. Majority of respondents had received
information about c-section delivery from health
personnel that was equal to 65.6%.
Table 1: The characteristic of respondents.
Category
Frequency
Σ
%
Education
Elementary and junior high school
8
24.1
Senior high school
19
59.6
Vocasional and bachelor
5
16.3
Job
Farmer
1
3.1
Private
9
28.1
Enterpreneur
2
7.2
Civil Servant
1
3.1
Housewives
19
57.9
Information of c-section
Yes
23
71.8
No
9
28.1
The source of information of c-section
Health Workers
21
65.6
Mass Media
1
3.1
Electronic Media
2
6.2
Neighboor/ Friend/ Family
8
25
Table 2 describe the maternal factors, the majority
of post c-section mothers aged between 20-35 years
as much as 71.8%. The number of live births
experienced by post c-section mothers was multipara
of 62.5%. The ability of post c-section mother to feel
the emotional state of newborns was in the category
of being as many as 71.8%. Mother's attitude to the
baby was almost the same between positive attitudes
and negative attitudes. Post c-section mother's
anxiety toward psychosocial post reaction c-section,
it was known that majority of post c-section mother
Early Breastfeeding in Post-Section Birth
713
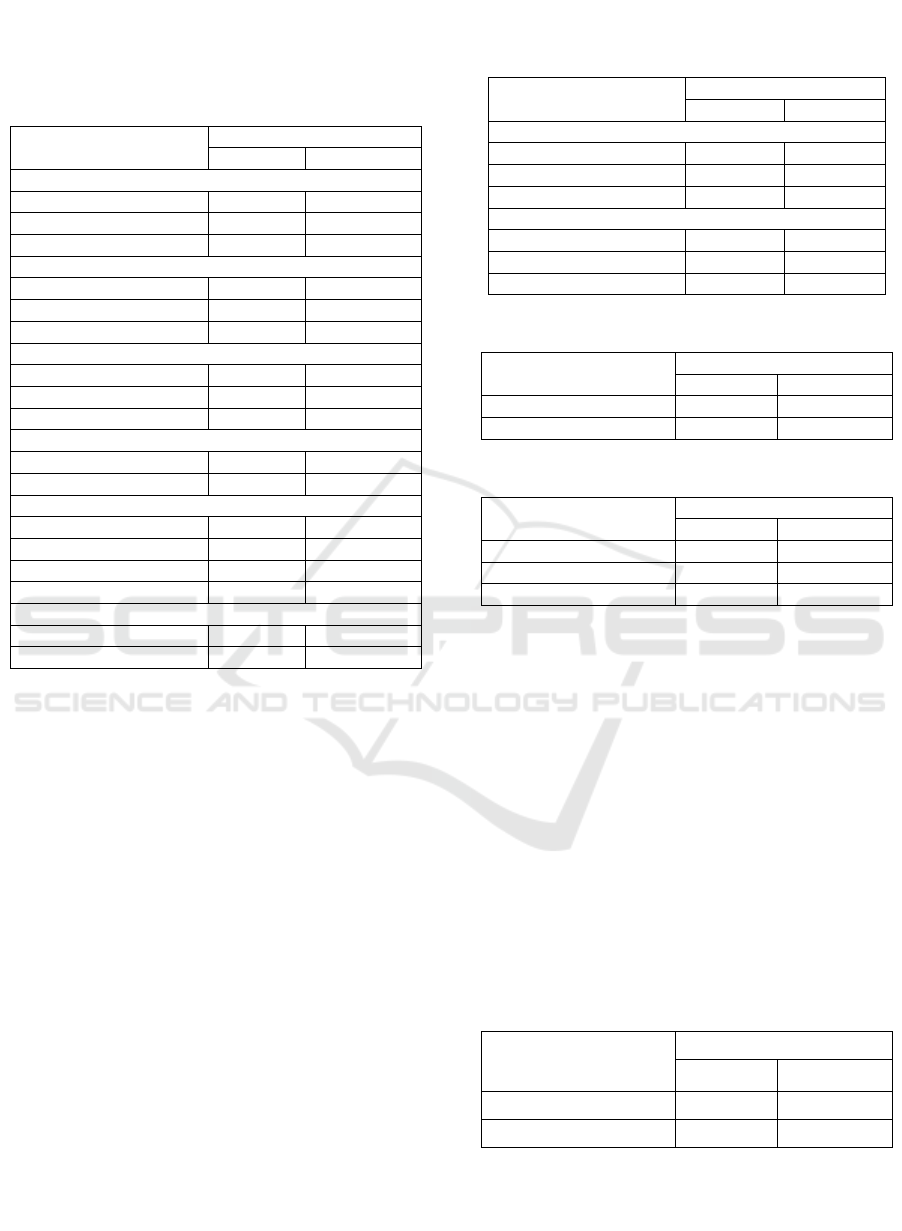
had mild anxiety about 75%. All mothers (100%) who
gave birth with c-section had high self-esteem
regarding the implementation of early breastfeed.
Table 2: Mother’s factors.
Category
Frequency
Σ
%
Age
< 20 years old
2
6.2
20 - 35 years old
23
71.8
> 35 years old
7
21.8
Parity
Nulipara
11
34.3
Multipara
20
62.5
Grande Multipara
1
3.1
Empaty
Low
4
12.5
Intermediate
23
71.8
High
5
15.6
Attitude
Negative
18
56.2
Positive
14
43.8
Anxiety
Not Anxiety
6
18.7
Mild
24
75.0
Intermediate
2
6.2
Big
0
0
Self-esteem
Low
0
0
High
32
100.0
Husband's support based on Table 3 below was
known that the majority of husbands gave enough
support to his wife who gave birth with Sectio
Caesaria, as many as 93,8%, and all had interaction in
good category, that is 100%.
Table 4 explained that almost all infants were able
to suck strongly when meeting with the nipple of the
mother, which was 96.9%. Based on table 5 below
was known that the factor of service category enough
and less was almost the same, that is for service was
quite equal to 46.8% and service less 40.6%.
Implementation of early breastfeed in infants from
post c-section mothers, based on table 6 below was
known the majority who did not do early breastfeed
that was equal to 96.9%. In contrast, only a small
portion (3.1%) performs an early breastfeed.
The factors which influenced the implementation of
early breastfeed can be seen in Table 7.
In this study there were 4 variables that were
suspected related to the implementation of early
breastfeed in RSUD Jombang. Based on the results of
the analysis shown in table 7 obtained t value
statistics> t table (1.96) that is on the variable factor
of the infant and provider service factor.
Table 3: Father’s factors.
Category
Frequency
Σ
%
Support
Less
1
3.1
Enough
30
93.8
Good
1
3.1
Interaction
Less
0
0
Enough
0
0
Good
32
100
Table 4: Responsive reflects of infant.
Category
Frequency
Σ
%
Weak
1
3.1
Strong
31
96.9
Table 5: Provider’s service.
Category
Frequency
Σ
%
Less
13
40.6
Enough
15
46.8
Good
4
12.5
The result of mutivariate analysis in Table 8
below showed that 2 model variables had p value
<0.05. It means that baby factor variable and provider
service factor significantly influence of early
breastfeed implementation and was the final model of
determinant factor of early breastfeed
implementation. From this analysis it could be
concluded that the two variables that enter into
multivariate, the most dominant variable related to
the implementation of early breastfeed was provider
service factor where the value of Expected (B) was
greatest (54.273), second was baby factor (22.750).
So the path of influence of exogenous factors on
endogenous factors could be concluded as in table 9
below.
Table 6: Implementation of early breasfeed.
Category
Frequency
Σ
%
Did dot do
31
96.9
Do
1
3.1
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
714
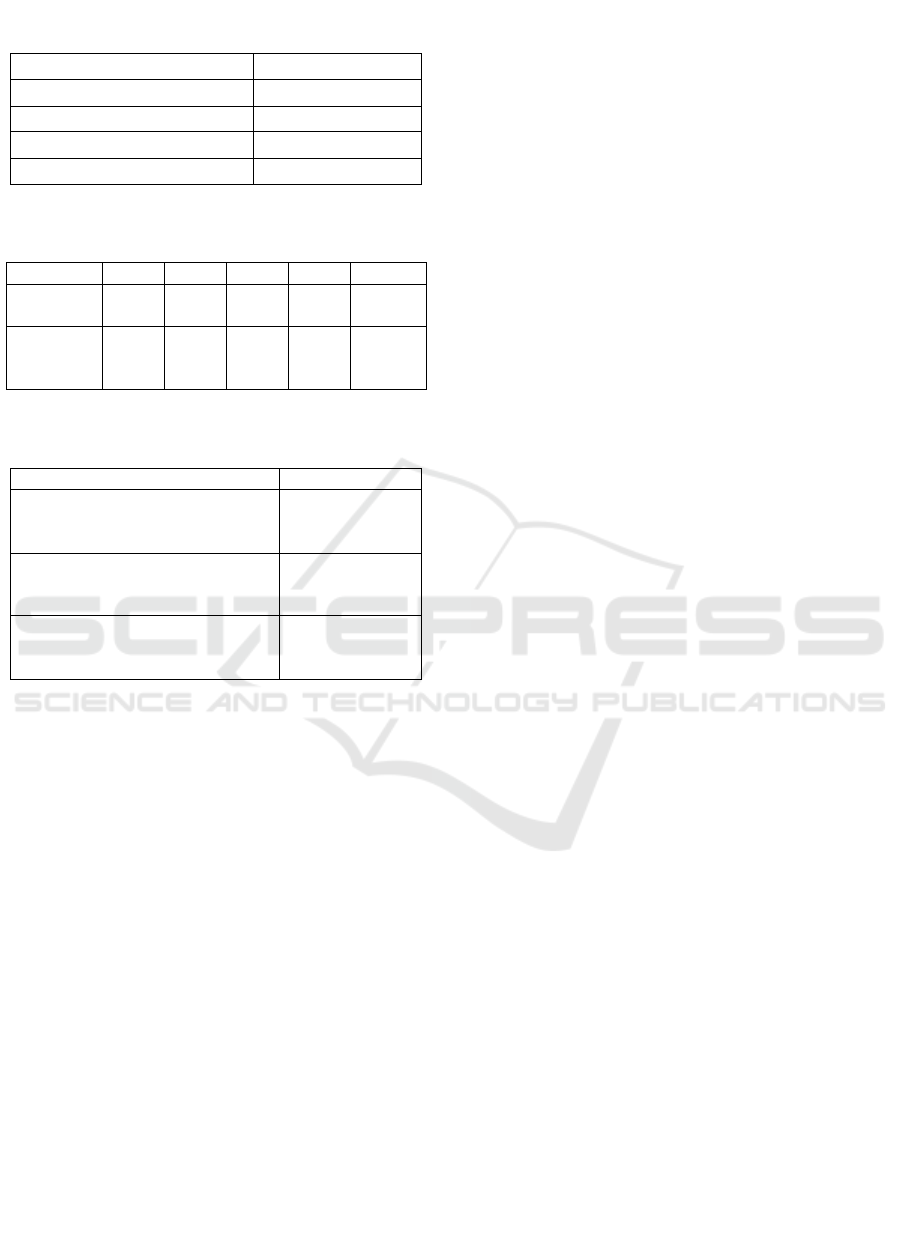
Table 7: Bivariate analysis of factor which correlate to the
implementation of early breast feed.
Category
t-statistic
Mother factor
0.07
Father factor
0.04
Infant factor
2.35
Provider factor
2.77
Table 8: Multivariate analysis of factor which correlate to
the implementation of early breasfeed.
Variable
B
SE
Wald
Sig.
Exp(B)
Baby’s
factor
3.107
1.332
5.674
0.013
22.750
Provider
Services
factor
3.883
1.431
8.854
0.002
54.273
Table 9: Influence line of exogenous factors to the
implementation of early breatfeed.
The influence line
Effect
Mother factors to
implementation of early
breastfeed
No
Father factors to
implementation of early
breastfeed
No
Infant factors to
implementation of early
breastfeed
Yes
Based on table 9, it could be concluded if wanted
the implementation of early breastfeed running with
the maximum then need to note the factors of
influence it, the baby and provider factors.
4 DISCUSSION
Mercer & Walker (2006) say that the contribute factor
for woman to be a mother are mother factor, infant
factor, father factor, provider service. Mother’s age
can affect physical and cognitive maturity. Maturity
can develop by learning from oneself or experience
of others (Perry & Potter, 2005).
The results showed that maternal age was
included in a good age for reproduction. So, the
mother was physically mature enough to give birth,
so also psychologically mother was also very ready to
play the role of mother. The condition of surgery
experienced by the mother currently causes
disruption in the role of mother. Finally, the age of
mothers who should be able to make mothers more
mature to be meaningless, this happens because the
mother underwent surgery that can cause the mother
to experience stress. Under conditions of stress the
mother needs the help of health services to meet her
needs.
The results showed the implementation of early
breasfeeding is very low although most of the
mothers empathize with the baby. Based on Mercer
(1990) empathize is one of the factors that influence
role of mother. This was because empathy was only
limited to understand and felt the feelings of others,
while the condition of the mother when helpless of
the early breastfeed could not be done without the role
of nurses and midwives, so it was necessary of
nursing interventions to facilitate early breastfeed
implementation. It was closely related to the
bounding attachment which was a relationship of
affection with the inner attachment between mother
and baby naturally. This was a process as a result of
an interaction between mother and baby who loved
each other, provided both emotional and needy
fulfillment. With bounding attachment between
mother and baby it would be very helpful in the needs
of health services.
The results of this study also showed that most of
the respondents entered the multiparity category.
Mother multiparous, there should be experience for
breastfeeding (Pernasia, 2004). But in this study the
state of multiparous mothers did not support the
mother's role in the early breastfeed.
The anxiety experienced by the mother during c-
section was the majority in the light category. So the
anxiety indicator could not explain the mother factor
in the implementation of early breastfeed. Everyone
must have experienced anxiety at certain moments
and with different levels. This might happen because
the individual felt that he did not have the ability to
deal with what might happen to him in the future
(Bellack & Hersen, 1988; Wangmuba, 2009).
Mother self-esteem in this study all had high self
esteem, therefore self-esteem indicator able to explain
mother factor in nursing service requirement. The
involvement of a husband in the implementation of
the early breastfeed would motivate the mother and
determine the emotional stability of the mother. A
stable emotional state determined the positive attitude
of the mother (Pérez-Ríos, Ramos-valencia, & Ortiz,
2008). Stability could be achieved if the husband or
family provided support or motivation to the
maximum. On the other hand, this was appropriate
because the husband was not allowed to accompany
his wife in the operating room, especially when in the
operating room, so that the support provided by the
husband was not maximal. The support of husband in
the operating room was needed to improve mother's
Early Breastfeeding in Post-Section Birth
715

confidence in implemention of early breastfeed
(Kolcaba & Dimarco, 2005). So it can be concluded
that although the wife got husband’s support, but the
husband was not on the side of the mother when the
surgery caused increased health care need post sectio
caesaria mother.
Infant factor (reflex suck), in this study showed
almost all babies had good sucking ability. Sucking
reflex indicator was able to explain baby factor. Infant
factors were not correlated with health care needs, but
had a direct relationship to the implementation of the
early breastfeed.
The role of the provider was crucial to the success
of the early breastfeed. Seeing the results of this
study, early breastfeed would not be implemented if
the provider did not facilitate the mother to do early
breastfeed (Padmavathi et al., 2014) standart care
refinement was required for early breastfeed
implementation of post c-section mothers who would
provide guidance to the provider in performing
nursing actions (relaxation and distraction) to
improve comfort in post c-section mothers.
5 CONCLUSIONS
Research conclude that there are two factors that
contribute post c-section breastfeeding factor. Two
factors that influence successful implementation of
the early breastfeed is infant factor and provider
factor (nurses and midwives). However provider
factor is the dominant factor in the successful
implementation of early breastfeed in post-sectio
caesaria mother which includes facilitation and
facilitation. For nursing education institutions, the
results of this study can be used as the development
of maternity courses, so as to broaden the insight of
students in implementing nursing care, especially
nursing maternity.
REFERENCES
Bellack, A. S., & Hersen, M. E. (1988). Behavioral
assessment : A practical handbook. Pergamon press.
Kolcaba, K., & Dimarco, M. A. (2005). Comfort theory and
its application in pediatric nursing. Pediatric Nursing,
31(3), 187-194.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K.
(1988). An ecological perspective on health promotion
program. Health Education & Behavior, 15(4), 351-
377.
Mercer, R. T., & Walker, L. O. (2006). A review of nursing
interventions to foster becoming a mother. Journal of
Obstetric, Gynecologic, & Neonatal Nursing, 35(5).
Padmavathi, P., Jayadeepa, T., & Babu, A. A. (2014).
Iniiation of breast feeding after caesarian delivery.
Asian Journal of Nursing Education, 4(1).
Pérez-Ríos, N., Ramos-valencia, G., & Ortiz, A. P. (2008).
Cesarean delivery as a barrier for breastfeeding
initiation: the Puerto Rican experience. Journal of
Human Lactation, 24(3), 293-302.
Pernasia. (2004). Manajemen laktasi : Menuju persalinan
aman dan bayi baru lahir sehat (2 ed.). Jakarta: EGC.
Perry, A. G., & Potter, P. A. (2005). Fundamental
keperawatan: Konsep, proses, dan praktek. Jakarta:
EGC.
Supriyanto, S., & Djohan, A. J. (2011). Metodologi riset
bisnis dan kesehatan. Kalimantan: Grafika Wangi.
Wangmuba. (2009). Fakor-faktor penyebab kecemasan.
Retrieved from http://wangmuba.com/
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
716
