
Optimising the Services Capacity Operation with Service Supply
Chain and Option Theories for Elderly Healthcare Systems in China
Jun Zhao and L. K. Chu
Department of Industrial and Manufacturing Systems Engineering, The University of Hong Kong, Hong Kong, China
Keywords: Elderly Healthcare Services, Service Supply Chain, Community Governance, Government Purchase of
Services, Option Contract.
Abstract: Traditional elderly healthcare service modes already can hardly meet the rapidly growing demand and high
customer expectations. The community-based elderly service mode (CESM), as a new mode merging with
the advantages of home-based and institution-based elderly service modes, is not yet widely applied in China.
We first analyse the problems of CESM in terms of the government purchase of services (GPS) policy,
governance theories and community elderly services coordination management. Then, we conclude the
research in the fields of the GPS, community governance and service supply chain coordination, and study
the experience of Hong Kong’s community care services system. On the basis, we propose an innovative
structure of community-based elderly healthcare service supply chain (EHSSC), and define the connotation
of EHSSC and its operational processes. Further, we optimise the operational mode for the EHSSC by using
the option contract and service voucher scheme, define the roles and functions of government, community
elderly service integrators, community elderly service providers and the elderly in EHSSC. The operation
processes of community elderly services capacity are illustrated to systematically address the issues of ‘who
participates in’ and ‘how to operate’ in CESM and coordinate the services capacity between the upstream and
downstream. Finally, we put forward some constructive suggestions for the implementation of EHSSC with
the option contract and service vouchers.
1 INTRODUCTION
Aggravated by the increasing demand and higher
customer expectations in China, the community-
based elderly service mode (CESM) has become
popular in China, providing new ideas to meet the
elderly service needs (Lin, 2014). The CESM
originated from the community care mode in the
United Kingdom. As one part of the community
works, the community care mode refers that
professional community workers mobilise
community resources and use formal and informal
support networks to cooperate with governmental and
non-governmental institutions, to help the needy in
the community (Zhang, 2002, Akjiratikarl et al.,
2007). In view of elderly healthcare service systems
in developed countries, China puts forward a brand
new CESM based on the government dominance,
social organizations participation and market
operation, to gradually establish a family-centred and
community-based professional services system to
provide life care, physical care, spiritual consolation,
culture and entertainment for the elderly in the
community. The CESM can not only meet the
elderly’s emotional demand of family attachment
living in their own familiar environment, but also let
them enjoy specialised services in the community,
which effectively integrates the family and society
resources. However, the CESM in China has not
taken satisfactory effects, there are still some issues
needed to be overcome and improved in terms of the
government purchase of services policy, governance
theories and community elderly services coordination
management.
To our knowledge, there is still not a unified
definition of ‘Government Purchase of Services
(GPS)’ in China and abroad (Song, 2013, Petersen et
al., 2015). The means of GPS in China and abroad
mainly include direct procurement, authority to
purchase, contracting out, vouchers, government
subsidies; and different countries may have different
means because of different national circumstances.
Some scholars reviewed the experience of GPS in
China and summarised the main obstacles to the
Zhao, J. and Chu, L.
Optimising the Services Capacity Operation with Service Supply Chain and Option Theories for Elderly Healthcare Systems in China.
DOI: 10.5220/0007249802130220
In Proceedings of the 8th International Conference on Operations Research and Enterprise Systems (ICORES 2019), pages 213-220
ISBN: 978-989-758-352-0
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
213

development of GPS including the poor construction
and organization ability, low efficiency, over-
administration and undeveloped supervision (Nai,
2014). Others put forward different measures to
improve the performance of GPS, such as the
extension of services scope, consideration of service
satisfaction, the elderly’s economic levels, third-party
assessment, trust-building, and independence of
social service organizations (Wen, 2017). Currently,
the implementation of CESM in China is mainly
through direct government purchase of services
(GPS) by which the government pays for some basic
elderly services to meet the community elderly
service demand. Services due to GPS mainly come
from grass-root elderly service organisations, which
are responsible for the final implementation and
delivery. However, the CESM in China has not
achieved the desired effects, major failings, amongst
others, are summarised as follows: (i) Various
government sectors/departments may not (or
incapable of) reach any consensus on the elderly
service demand and functions of community elderly
service organisations; thus resulting in confusion in
policy (Li and Dahl, 2015); (ii) There is not any
specialised and standard legal basis for making GPS,
thus leading to poor GPS decisions or even corruption
(Ramesh et al., 2014, Nai, 2014); and (iii) Those
grass-root service providers often pay lip service to
relevant management advice from government as
formality, and most elderly in communities can
hardly enjoy the benefits from the policy of GPS (Xu,
Wu, and Zeng, 2014). To improve the status quo in
China, we study the case of Hong Kong community
care service system, and analyse the advantages and
disadvantages between the China and Hong Kong
community elderly service systems.
In making GPS by the Chinese government, the
control is mostly responsible by the authority and
authorisations are given to departments
hierarchically. The grass-root community elderly
service institutions or providers are only responsible
for implementation. Such over-administration by the
government undermines the autonomy of community
elderly service institutions (Liu et al., 2008, Wang
and Salamon, 2010). Over time, this results in the
complacency of the service providers, loss of
enthusiasm of the stakeholders (especially the end
users), and the generally low regard and approval
rating of the CESM (Liu, 2006). Therefore, it is
desired that some form of intermediate entity in the
CESM, which can not only share the management
responsibilities with the government, but can also
enhance proactive management awareness and the
efficient use of government resources for elderly
services. We consider the transformation of the
government’s role in the CESM by introducing the
concepts polycentric governance and meta-
governance. Briefly, the proponents of the former
opine that the centre of power to manage the society
is diverse, putting the government, the market and the
society on the same position rather than that
prescribed by the state-centred theory (McKieran et
al, 2000). Polycentric uses cooperation and
consultations to resolve disagreements and conflicts
in the diverse and decentralised social environment.
On the other hand, meta-governance pays more
attention to the role of government in public service
administration (Jessop, 2015). The government still
plays the main role in the case of meta-governance,
and it is regarded as ‘the senior’ in the social
management network. However, the government
does not assume the highest authority but bears the
responsibilities of establishing common guidelines to
govern social organisations and stabilising the
general direction of the main players. For CESM, the
designed way of a governance framework is mainly
based on environmental factors, not least the specific
social and political environments in which it operates
(Meuleman, 2011).
With demand uncertainties due to market
fluctuations or operation changes, the government is
unable to adjust and update the purchasing decisions
in time, resulting in the supply-demand information
asymmetry and waste of community elderly services
capacity (Guo et al., 2013, Nelson and Sen, 2014). In
practice, this operational mechanism is lack of
centralised management as well as the coordination
between the demand and services capacity supply.
The community elderly service institutions have no
rights to supervise the elderly service providers
(ESPs) who cooperate with the government by
contracts, so they cannot directly coordinate price,
costs, service capacity ordering quantity and
relationships. Also, the performance evaluation made
by the elderly for the ESP is not paid attention, so that
the elderly services market is a lack of appropriate
incentives and competition (Yang and Hwang, 2006).
Gradually, the government-led community elderly
institutions lose the risk aversion consciousness.
The tremendous development of the service
industry has motivated the research in service supply
chain (SSC); and the resulting SSC concepts and
theories have been successfully applied to the fields
of logistics, tourism, finance, healthcare (Akkermans
and Vos, 2003; Hong et al, 2011; Huemer, 2012),
amongst others. A more comprehensive definition of
SSC is given by Song and Chen (2009), who describe
SSC as a form of service-oriented integration supply
ICORES 2019 - 8th International Conference on Operations Research and Enterprise Systems
214

chain that, once the downstream customer has
decided on the service demand, the service integrator,
as the core manager, will devise a solution to satisfy
the demand requirements. However, the study in SSC
is still evolving. Few studies have so far sufficiently
elaborated the features of services when developing
the understanding of SSC. Furthermore, the study in
the elderly service supply chain is still nascent. To
address China’s problems of its under-developed
CESM and supply-demand mismatch, there exist
enormous opportunities for exploring the
organisational structure of CESM from the
perspective of SSC. With regard to the coordination
and optimization for the SSC, most scholars have
proved the essence of SSC coordination was the
complementation and cooperation of services
capacity (Anderson and Morrice, 2000). And the
supply contracts are effective tools in SSC, mainly
including the quantity discounts and rebates, option
contract, flexible quantity contract, buyback contract,
compensation contract and so on. Many studies have
illustrated that the option contract could effectively
address the investment and risk-sharing issues on
production capacity as well as the purchase of
services capacity for the service integrator and the
subcontractor. Therefore, this study identifies this
research opportunity and aims at developing a CESM
to address China’s case. The proposed CESM will
embody modern SSC concepts and its coordination
mechanism will base on a set of option contracts.
Based on this research, a set of new methods can be
developed to obtain optimal solutions for elderly
service capacity coordination for the CESM.
2 CASE STUDY OF HONG
KONG’S COMMUNITY CARE
SERVICES SYSTEM
The CESM in Hong Kong is called the ‘community
care services’ (CCS), which is one important part of
Hong Kong’s developed elderly healthcare services
system with outstanding performance. The CCS
system in Hong Kong is more similar to the CESM
promoted in mainland China. Thus, the experience of
Hong Kong’s CCS is more valuable for us to learn.
2.1 Diversified and Integrated
Community Care Services for the
Elderly
The CCS in Hong Kong is mainly classified into two
categories based on the elderly’s physical and mental
status, including the ‘Day Care services for the
Elderly’ and ‘Enhanced Home and Community Care
Services’. The two types of CCS are designed
according to the elderly’s demand with a series of all-
round surveys. And the CCS centre, as the service
manager and implementer, carries out the case
management to track and update the elderly’s
healthcare information. Generally, all the care
services are provided by the third party that are the
non-governmental institutions and non-profit
institutions.
2.2 The Tripartite Cooperation of
Services Supply with Contracts
The supply of community care services capacity has
formed a tripartite cooperation mechanism among the
government, the business and the third party
institutions with contracts. The government refers to
the Hong Kong social welfare department and related
welfare sectors, the business includes the private
service institutions and philanthropists, and the third
party institutions involve the non-governmental
institutions and non-profit institutions.
The government plays the purchase of services,
fund-supporting, policy-making, supervision and
guidance roles in the services capacity supply. The
business works as an indispensable contributor to
make up for the capacity limitations of the
government and non-profit institutions and bring a
huge boost in sponsoring different charity
organizations. The third party institutions are the
executor of policies and services, to some extent
sharing the burden of the government and private
institutions.
2.3 The Pilot Scheme on Community
Care Service Voucher for the
Elderly in Hong Kong
Recently, the mode of community care service
voucher (CCSV) in Hong Kong has aroused
widespread concern (Social Welfare Department of
Hong Kong SAR, 2016b). The pilot scheme on CCSV
for the elderly launched by the Hong Kong Social
Welfare Department in 2013 aimed to provide service
vouchers of about six thousand and five hundred-
dollar monthly value for each elderly with moderately
impaired physical status to subsidise them to freely
select and use suitable care services or service
portfolios. Moreover, the pilot scheme employs the
‘money-follows-the-user’ means, whereby the
government provides subsidy directly to the elderly
(instead of service providers) in the form of service
Optimising the Services Capacity Operation with Service Supply Chain and Option Theories for Elderly Healthcare Systems in China
215
vouchers. Monthly, the government would pay the
ESP for voucher amounts which the ESP receives
from the elderly. During the implementation of the
first-phase CCSV scheme, the performance resulted
well, and now the second phase is in progress.
The CCSV mode is designed to change the
traditional care services capacity operational mode of
‘Government—Care Service Institutions’ into the
customer-centred resource flowing mode of
‘Government—the Elderly—Care Service
Institutions’. It is helpful to promote the public-
private partnership by offering the elderly more
choices of selecting private care services to relieve
pressure on the public care system. Thus, the CCSV
scheme can not only enable the elderly to become
sovereign consumers with government subsidies and
choose care services with freedom, but also stimulate
care institutions to improve their service levels for
competition, contributing to strengthening the
contacts among the elderly and social service
institutions.
2.4 Comparisons and Implications
based on the Practices in China and
Hong Kong
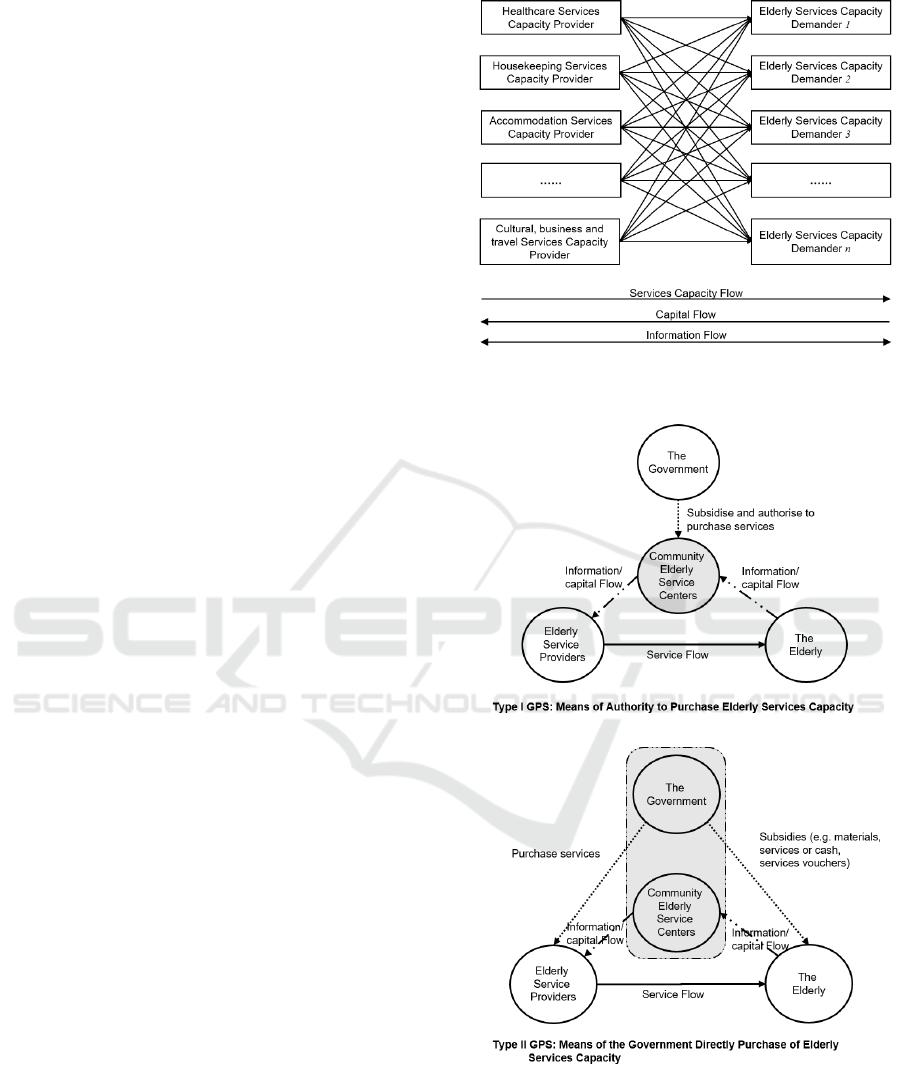
In China, the current services capacity supply and
demand model in the CESM works under an
uncoordinated circumstance without core operators,
where the services capacity flow, information flow
and capital flow can hardly be controlled centrally.
The government works as the policy-maker, capital-
supporter and services buyer, while the community
service institutions mainly serve as the subsidiary of
our government actually without autonomous
operation. Thus, the elderly services capacity
providers work independently for their own profits.
See Figure 1.
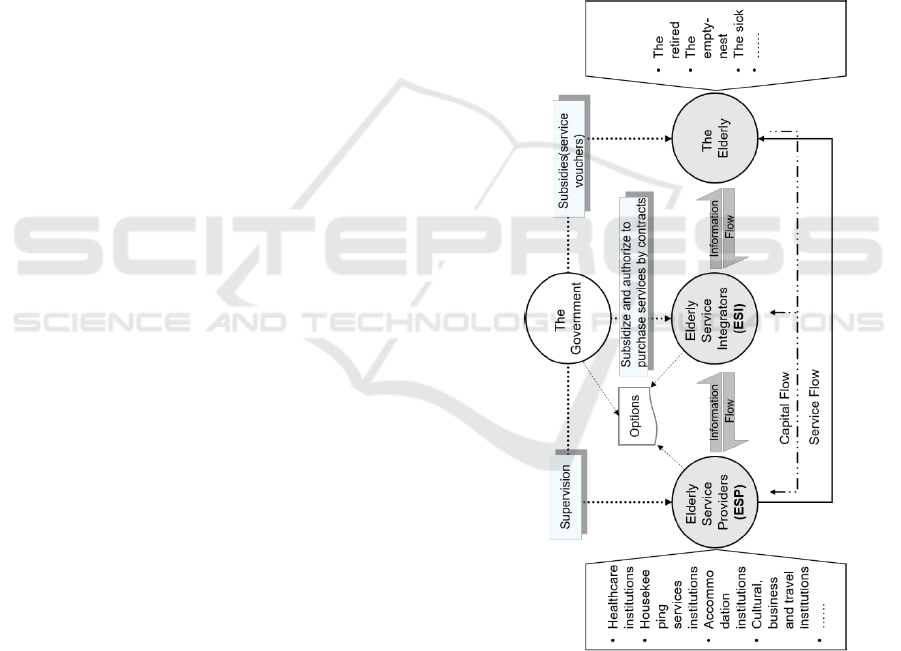
However, considering the typical cases of CESM
in China and Hong Kong, we can find that even
though the CESM may be different externally due to
the local governance, they can be mainly classified
into two types based on the means of GPS, in which
one type (Type I) is that the government authorises
the community centres to purchase elderly services
capacity, such as the Beijing Xuanwu District mode,
Nanjing Gulou District mode and Guangzhou Feng
Yuan Street mode (Lin, 2016); the other type (Type
II) is the government directly purchases elderly
services capacity from the ESP, such as the Hefei
mode (Zhao, 2016) and Hong Kong mode (Social
Welfare Department of Hong Kong SAR, 2016a). See
Figure 2.
Figure 1: The current services capacity supply and demand
in China’s CESM.
Figure 2: Two types of CESM based on the GPS modes in
China and Hong Kong.
Hong Kong’s CCS system has taken significant
effect on the social welfare (Social Welfare
Department of Hong Kong SAR, 2016a), which is
extremely instructive for the development of CESM
that we are currently implementing in mainland
ICORES 2019 - 8th International Conference on Operations Research and Enterprise Systems
216
China. First, the responsibilities of the core manager
(e.g. the community elderly services centres) in
elderly services should be highlighted with a
dominant role in the execution and coordination of
care services capacity, helping alleviate the
government’s burden. Second, the cooperation
among the government, the community service centre
(i.e. the elderly service integrator, namely ESI) and
the ESP can be reinforced by contracts and
supervision mechanisms. Also, we should encourage
the qualified ESP to participate in community-based
elderly services supply scheme, and introduce
competition mechanism to stimulate the ESP to
improve their service quality and efficiency. Third,
the role of government in elderly services cannot be
ignored, furthermore, we should improve the
government’s abilities on fund-supporting, planning,
supervision and guidance in the whole social elderly
services market, and advocate the government to
purchase elderly services. Finally, it is a creative
measure to offer more rights for the elderly to select
services and to make the elderly as the third party to
help regulate the service provides. However, the
CCSV is now limited to the specific group of aged
people in Hong Kong, and cannot be distributed to all
the elderly as a general welfare. Therefore, it is also
the starting point of this paper to explore how to
overcome the drawbacks of the CCSV mode, perform
the service voucher’s effect of promoting
competition, optimise service capacity allocation and
render the elderly the right to vote for suitable
providers in China.
3 THE OPERATION
MECHANISM OF CESM WITH
THE OPTION CONTRACT
BASED ON THE SSC
3.1 The Innovative Mode of
Community-based Elderly
Healthcare Service Supply Chain
Based on the above theoretical and practical analysis,
we propose a brand new system for the CESM based
on the SSC and governance theories. Zhang et al.
(2011) first studied the elderly service supply chain
(ESSC), and defined it as a type of functional chain
structure, which was oriented towards the
requirements of the elderly. Based on the study,
Zhang et al. (2013) completed a survey and
evaluation about the ESSC’s performance by
applying the ESSC mode into the Guangzhou Feng
Yuan Street community, and they demonstrated its
remarkable effect on improving the CESM. However,
they did not uncover the specific structure of ESSC
and studied further its operation. Considering their
research, we focus on the elderly services in
communities, propose and define that the community-
based elderly healthcare service supply chain
(EHSSC) is a community-centred ESSC in which the
government, the ESP and the elderly service
integrator (the ESI) work collaboratively and
interdependently by a series of contracts to provide
diversified elderly services including physical care,
housekeeping, accommodation, culture, business,
travel, finance and so on, to realize the centralised
management of service flow, capital flow and
information flow.
Figure 3: The mode of community-based EHSSC.
Specifically, the ESI serves as the core institution
in the EHSSC, such as the community elderly service
centre and the community information service centre,
to purchasing the elderly services capacity,
coordinate the supply-demand between the upstream
and the downstream and control the service quality
and risks. The ESPs, including the healthcare
Optimising the Services Capacity Operation with Service Supply Chain and Option Theories for Elderly Healthcare Systems in China
217
institutions, housekeeping services institutions,
accommodation and culture institutions and so on,
directly provide services to the elderly based on the
service solutions made by the ESI. The government
plays an indispensably important role in funding,
supervising the supply chain contracts, promoting
efficient operation and providing related supports.
See Figure 3.
3.2 The Operation Mechanism of
EHSSC with the Option Contract
and Service Vouchers
Considering the drawbacks of CCSV mode, we
design a kind of universal service voucher for all the
elderly in communities, and propose the contract
governance mode aiming to unify the four parties
including the government, the community ESI, the
ESP and the elderly.
Combing the advantages of CESM in China and
Hong Kong, we design a community-based elderly
services capacity operation framework with the
option contract and service vouchers, in which the
option contract is the agreement between the ESI and
the ESP, and the service vouchers are also one kind
of contract between the government and the elderly.
The service vouchers are designed with the
consideration of the elderly’s physical and economic
conditions, and the elderly may afford part of the
services fee by themselves. Thus, the service
vouchers can not only stimulate the elderly to use the
community care services, but also introduce the
competition and voting mechanism.
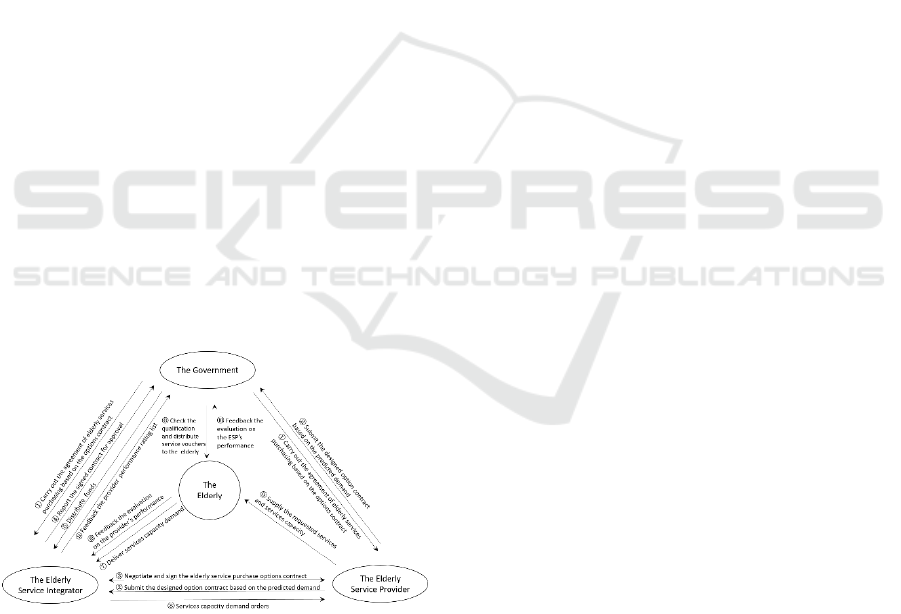
Figure 4: The operational mode of community-based
elderly services capacity supply-demand.
Specifically, the new mode works as follows (see
Figure 4). The government is responsible for
organizing the community ESI and the ESP, and
enacts the negotiation framework of elderly service
capacity option contracts and service voucher
scheme. Then, the ESP submits their service capacity
option contracts to the government and community
ESI. After the first examination and approval by the
government, the community ESI begins to evaluate
the potential ESPs and sign the community-based
elderly service capacity option contracts with the
candidate ESPs. Once the ESP accepts the service
option premium, they should provide requested
elderly services and services capacity with the agreed
price. When the option contract takes effect, the
community ESI would feedback the services capacity
pricing to the government. Then, the government
takes charge of approving and archiving the contracts,
subsequently authorises and funds the ESI to
purchase services capacity and pay related
expenditure. After launching the service voucher
scheme, the government will deliver different valued
service vouchers to the elderly based on the service
capacity pricing and the elderly’s conditions. The
elderly can use the service vouchers to buy favourite
services. Those ESPs, who receive the vouchers, can
redeem equal-valued cash from the government. In
summary, the four parties in the contract governance
mode have the independent operating autonomy,
which means they are interdependent with each other
and share a common interest. All of them have the
resources which are necessary for others to achieve
mutual benefits, but they are also independent to
control the resources, that is, the government holds
the capital, the elderly have the vouchers, the ESPs
have the services capacity, and the ESI has the
responsibilities to coordinate the demand and service
capacity. The participation of four governance parties
in the operational mode promotes the coordination
and cooperation among all stakeholders.
4 SUGGESTIONS ON THE
IMPLEMENTATION OF EHSSC
WITH THE OPTION
CONTRACT AND SERVICE
VOUCHER SCHEME
Thus, it should be a forward-looking method to build
up the CESM with option contract and SSC under the
policy of GPS. There are some suggestions needed to
be adopted to further improve the implementation of
EHSSC with the option contract and service voucher
scheme in practice.
First, it is a must for the government and the ESI
to change their behaviour means in order to
implement the EHSSC with the option contract. With
the transformation of government functions, the
relationships among the government, market and
ICORES 2019 - 8th International Conference on Operations Research and Enterprise Systems
218

society should be reframed objectively. Specifically,
the responsibilities undertaken by the government are
turned over to the community ESI and the ESP in
form of contracts, building up a three-level
cooperation framework within an option contract
system.
Second, it is a need to further improve the
construction of related regulations for the
implementation of EHSSC with the option contract
and service vouchers. The EHSSC with option
contract is a new governance mode to purchase
community-based elderly services capacity and
collaborate the upstream and downstream of SSC,
which is completely different from the traditional
government-led CESM. A new set of regulations and
corresponding measures, undoubtedly are need to be
worked out, such as the specification of funding and
policy support, standards of GPS and rules of
community ESP introduction.
Finally, it is significant to strengthen supervision
for EHSSC. As the executive of the community
elderly services capacity option contract and the core
enterprise in SSC, the community ESI needs to accept
the supervision from the government and the elderly,
in order to ensure the elderly services quality and the
overall interests of the EHSSC. The community ESP,
as the key carrier of the option contract, needs to be
supervised by ESI and the elderly, to unify the overall
goal of EHSSC and facilitate the standard and
sustainable operation.
5 CONCLUSIONS
Based on the current situation and problems on the
CESM, we optimise the CESM systematically from
the perspective of community governance theories,
SSC and option contracts. First, we introduce the
polymeric governance and Meta governance to
reframe and define the relationships and functions
among the government, community ESI and the
elderly. Second, we apply the concept of SSC to put
forward an innovative community elderly services
operation structure——EHSSC, and define the
connotation of EHSSC and its operational processes.
The new mode highlights the core role of ESI, who
strengthens the coordination between the upstream
and downstream, integrates services capacity from
various ESPs, and provides personalized and diverse
service solutions for the elderly. Furthermore, we use
the option contracts and service voucher scheme to
build up the four-dimensional supervision and
cooperation mechanism framework among the
government, the ESI, the ESP and the elderly, and
further propose the operational mode of EHSSC with the
option contract. Finally, we propose some suggestions for
the implementation of EHSSC with the option contract and
service vouchers in terms of the behavioural changes of the
government and ESI, regulations for the EHSSC and its
supervision system, to provide guidance for the
development of EHSSC.
REFERENCES
Akjiratikarl, C., Yenradee, P. and Drake, P. R., 2007. PSO-
based algorithm for home care worker scheduling in the
UK. Computers and Industrial Engineering, 53, 559-
583.
Akkermans, H. and Vos, B., 2003. Amplification in SSCs:
An Exploratory Case Study from the Telecom Industry.
Production and Operations Management, 12, 204-223.
Anderson, E. G. and Morrice, D. J., 2000. A simulation
came for teaching service-oriented supply chain
management: Does information sharing help managers
with service capacity decisions? Production and
Operations Management, 9, 40-55.
Bowles, S. and Gintis, H., 2002. Social Capital and
Community Governance. The Economic Journal, 112,
419-436.
Cai, E., Liu, Y., Jing, Y., Zhang, L., Li, J. and Yin, C., 2017.
Assessing Spatial Accessibility of Public and Private
Residential Aged Care Facilities: A Case Study in
Wuhan, Central China. ISPRS International Journal of
Geo-Information, 6, 304.
Guo, M., Li, B., Zhang, Z., Wu, S. and Song, J., 2013.
Efficiency evaluation for allocating community-based
health services. Computers & Industrial Engineering,
65, 395-401.
Hong, T. K., Zailani S., 2011. SSC Practices from the
Perspective of Malaysian Tourism Industry. In IEEE
International Conference on Industrial Engineering
and Engineering Management (IEEM), 539-543.
Singapore, SINGAPORE: IEEE.
Huemer, L., 2012. Unchained From the Chain: Supply
Management From A Logistics Service Provider
Perspective. Journal of Business Research, 65, 258-
264.
Jessop, B., 2000. The rise of governance and the risk of
failure: A Case Study of economic development, Social
Sciences Academic Press.
Jessop, B., 2015. Governance and Meta Governance: On
Reflexivity, Requisite Variety and Requisite Irony.
Foreign Theoretical Trends, 5, 14-22.
Li, S. and Dahl, J., 2015. Are Chinese Seniors Ready for
Nursing Home Care? [Online]. BEUJING REVIEW.
Available:
http://www.bjreview.com/Nation/201511/t20151102_
800041721.html [Accessed 26 Sep 2018].
Lin, W., 2014. Community service contracting for the
elderly in urban China. Doctor of Philosophy PhD
thesis, City University of Hong Kong.
Lin, W., 2016. Community service contracting for older
Optimising the Services Capacity Operation with Service Supply Chain and Option Theories for Elderly Healthcare Systems in China
219

people in urban China: a case study in Guangdong
Province. Australian Journal of Primary Health, 22,
55-62.
Liu, X., Hotchkiss, D. R. and Bose, S., 2008. The
effectiveness of contracting-out primary health care
services in developing countries: a review of the
evidence. Health Policy and Planning, 23, 1-13.
Liu X. J., 2006. Comparison and Choices of Urban
Community Governance Modes in China. Socialism
Studies, 2, 59-61.
Mckieran, L., Kim, S. and Lasker, R., 2000. Collaboration:
Learning the Basics of Community Governance.
Community, 23-30.
Meuleman, L., 2011. Metagoverning Governance Styles-
Broading Public managers Action Perspective, Jacob
Torfingand Peter Triantafillou. Interactive policy
making Metagovernance and Democracy. Colehester:
ECPR Press, 101-106.
Nai, Y. W., 2014. Several Important Problems of
Government Purchase of Public Services. China
Institutional Reform and Management, 38-41.
Nelson, M. L. and Sen, R., 2014. Business rules
management in healthcare: A lifecycle approach.
Decision Support Systems, 57, 387-394.
Petersen, O. H., Houlberg, K. and Christensen, L. R., 2015.
Contracting Out Local Services: A Tale of Technical
and Social Services. Public Administration Review, 75,
560-570.
Ramesh, M., Wu, X. and He, A. J., 2014. Health
governance and healthcare reforms in China. Health
Policy and Planning, 29, 663-672.
Social Welfare Department of Hong Kong SAR, 2016a.
2016-17 Estimates of Expenditure [Online]. [Accessed
7 Nov. 2016].
Social Welfare Department of Hong Kong SAR, 2016b.
Pilot Scheme on Community Care Service Voucher for
the Elderly [Online]. Hong Kong: Social Welfare
Department of Hong Kong SAR. Available:
http://www.swd.gov.hk/tc/index/site_pubsvc/page_eld
erly/sub_csselderly/id_firstphase/ [Accessed 05
December 2016].
Song, G., 2013. Government Purchase Services:
Mechanism Innovation of the Social Governance.
Journal of Beijing Polytechnic University(Social
Sciences Edition), 10-16.
Song, H. and Chen, J. L., 2009. The Impact of Strategic
Interaction and Value Co-creation to Legitimacy in
SSC. Management Sciences in China, 2-11.
Wang, P. and Salamon, L. M., 2010. Study on government
purchase of public services from social organizations:
lessons from China and abroad, Beijing, Peking
University Press.
Wen, Z., 2017. Government purchase of services in china:
Similar intentions, different policy designs. Public
Administration and Development, 37, 65-78.
Xu S. M., Zhang, J. P., 2014. The Logic and Path of Hub--
type Social Organizations’ Participation in Government
Purchase of Services Contracting --Taking the
Communist Youth League as an Example. Chinese
Public Administration, 9, 41-44.
Yang, W.-S. and Hwang, S.-Y., 2006. A process-mining
framework for the detection of healthcare fraud and
abuse. Expert Systems with Applications, 31, 56-68.
Zhang, X., 2002. Community-based care for the frail
elderly in urban China. Doctor of Philosophy PhD, The
University of Hong Kong.
Zhang, Z. Y., Shi, Y. Q. and Zhao, J. Analysis of the Elderly
Service Supply Chain Management Strategy based on
Service Quality Control and Cooperative Relationship.
COINFO '11, 2011 Hangzhou, China.
Zhang, Z. Y., Zhao, J. and Shi, Y. Q., 2013. Innovation
mode of elderly service supply chain: Performance
evaluation and optimization strategy: An investigation
on liwan district guangzhou city. Commercial Research
(Chinese), 55, 107-115.
Zhao, X. F., 2016. Study on the government purchase of
public service from the social organizations in China
[Online]. Institute of Economic System and
Management National Development and Reform
Commission. Available: http://www.china-
reform.org/?content_501.html [Accessed 05 December
2016].
ICORES 2019 - 8th International Conference on Operations Research and Enterprise Systems
220
