
How Anthropomorphism Affects User Acceptance of a Robot Trainer
in Physical Rehabilitation
Baisong Liu, Panos Markopoulos and Daniel Tetteroo
Department of Industrial Design, Eindhoven University of Technology, De Zaale, Eindhoven, The Netherlands
Keywords: Socially Assistive Robot, Anthropomorphism, Rehabilitation, User-centred Design, Acceptance.
Abstract: Developments in social robotics raise the prospect of robots coaching and interacting with patient during
rehabilitation training assuming a role of a trainer. This raises questions regarding the acceptance of robots in
this role and more specifically, to what extent the robot should be anthropomorphic. This paper presents the
results of an online experiment designed to evaluate the user acceptance of Socially Assistive Robots (SARs)
as rehabilitation trainers, and the effect of anthropomorphism on this matter. User attitudes were surveyed
with regards to three variations of a scenario where the robot with varying levels of anthropomorphism acts
as a trainer. The results show that 1) participants are accepting towards SAR-assisted rehabilitation therapies,
2) anthropomorphism influences patient’s perceived self-efficacy and attitude towards the system. A second
survey studied inventoried issues regarding patients’ acceptance of such systems, pertaining to technology
acceptance, patient needs for rehabilitation training and the effect of anthropomorphism. Based on the above
findings we propose user-informed design implications for improving user acceptance is rehabilitation
settings.
1 INTRODUCTION
The application of robotic technology in the domain
of physical rehabilitation is an area of ongoing
research (Laut et al., 2016). Projects have developed
robotic technology to support physically impaired
patients, such as mobility aids for aging and motor
function impaired users, assisting users in loaded
walking (Ding et al., 2017) and supporting
rehabilitation training exercises (Feys et al., 2015;
Popescu et al., 2016). Such projects have shown that
robots can help to improve the quality and quantity of
rehabilitation training. However, the current trend
mostly concerns with physically supporting (parts of)
the body (Cardona et al., 2017; Vitiello et al., 2017).
Socially Assistive Robotics (SAR) provides
assistance to users through social interaction (Feil-
Seifer and Mataric, 2005). The use of SAR in
rehabilitation training has been considered and
demonstrated as promising (Eriksson et al., 2005).
Taxonomies of components concerning socially
interactive robots have been proposed (Fong et al.,
2003; Feil-Seifer and Mataric, 2005), suggesting
human-oriented perception is an important part of
SAR interaction design. Thus far, this aspect is yet to
be explored in the context of rehabilitation training.
We have taken a user-centered approach to this
issue, exploring patients’ acceptance towards the
concept of a robot trainer for rehabilitation, and the
effect anthropomorphism has on its acceptance. This
paper provides insights for further design of utilizing
SAR in the context of rehabilitation training.
2 RELATED WORK
2.1 Social Robot Acceptance
General robot acceptance studies have investigated
the effects on acceptance of specific robotic traits,
such as gender of the voice (Eyssel et al., 2012), facial
expressions (Moosaei et al., 2017) and gestures (Zaga
et al., 2017). Regarding SAR, (Fong et al., 2003) have
identified the following factors to be of influence on
acceptance: 1) the user’s attitude towards the robot,
2) the robot’s field performance, 3) robot-displayed
emotions, 4) appearance and dialog, and 5)
personality. These studies explore robot acceptance
regardless of a specific context, and thus provide
general conclusions and directions for further
research.
30
Liu, B., Markopoulos, P. and Tetteroo, D.
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation.
DOI: 10.5220/0007343600300040
In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2019), pages 30-40
ISBN: 978-989-758-353-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Another branch of social robot acceptance study
focuses on specific contexts and user groups,
typically children, elderly and autism patients. For
example, the Almere Model has been proposed for
testing and predicting elderly users’ acceptance of
assistive social agent technologies, suggesting 12
factors to be of influence (Heerink et al., 2010).
Another study employed a zoomorphic companion
robot (Nabaztag) into an elderly user’s home to gain
insights on social robot acceptance, focusing on users
building a long-term relationship with a social robot
in domestic settings (Klamer and Allouch, 2010). The
acceptance of SAR in the specific context of
rehabilitation has not yet been investigated.
2.2 Anthropomorphism
Anthropomorphism of social robots is a powerful
factor influencing the user’s experience, including
empathy (Moosaei et al., 2017), enjoyment, and other
social emotions (Bartneck et al., 2010).
Anthropomorphism is proposed to be expressed in
appearance and behavior (Choi and Kim, 2008). So
far studies have explored different factors of
anthropomorphic appearance embodied in the design
of robots, for example through facial expressions
(Moosaei et al., 2017), voice (Siegel et al., 2009) and
gesture (Salem et al., 2013). As it has been suggested
that user responses to anthropomorphic robotics are
context based (Epley et al., 2007), it is important to
explore the effects of anthropomorphism for specific
contexts and use cases, such as that of physical
rehabilitation.
2.3 Social Robots for Rehabilitation
SAR has been proposed as an alternative to the
therapist for rehabilitation exercises, due to its
potential benefits of cost reduction, privacy,
improving engagement, and open up possibilities for
home training scenarios (Winkle et al., 2018). A
feasibility study has proven the potential of such
application (Kyong Il Kang et al., 2005). A further
study has suggested that even very simple robot
behavior might benefit compliance in stroke
rehabilitation exercises (Gockley and Mataric, 2006).
A more recent study underlined the link between
personalized robot behavior and user task
performance in rehabilitation training (Tapus and
Mataric, 2008.).
3 RESEARCH QUESTIONS
While the above-mentioned study by (Winkle et al.,
2018) examined the design of SAR from a therapist
perspective, this paper presents a study from the
perspective of the patient. The aim of this paper is to
explore patients’ attitude towards having a social
robot trainer to facilitate their rehabilitation training.
Specifically, we are interested in:
RQ1) What is the patient’ attitude towards having
a robot trainer as facilitator of their rehabilitation
training?
RQ2) How does the level of anthropomorphism in
SAR form-design influence the patients’ acceptance
in the context of rehabilitation training?
RQ3) What are patients’ preferences and
concerns regarding SAR within the context of
rehabilitation training?
4 METHOD
We conducted two studies to investigate our research
questions. In both studies, we used an illustration of a
fictional scenario with a patient performing her
rehabilitation exercise with the help of a robot trainer
(see figure 1), participants in the three conditions of
study one were shown with three different robot
trainer concepts presented in table 1.
In study one, aimed at answering RQ1 and RQ2,
we have used standard questionnaires and open
questions to collect the participants’ general attitude
towards social robotics, as well as their attitude
regarding the application of SAR to the scenario.
Study two was aimed at answering RQ3, and to
collect more in-depth information on some of the
answers obtained by study one. This study was
executed as a survey composed of mostly open
questions regarding RQ3.
4.1 Scenarios
Both studies utilized illustrated scenarios describing
a fictional interaction between a patient and a robot
trainer. To focus on only the social interaction
aspects, the robot in this scenario does not support or
enforce movements with the patient, as one might
expect in rehabilitation robotics, but takes only the
role of a coach who provides the patient with
information on the overall progress of the therapy,
instructions for the exercise and encouragement when
the patient is experiencing physical challenges. The
story of the scenario is based on observations of
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation
31

clinical treatment and was further improved by
consulting experienced physical therapists.
Figure 1: Scenario Used in the Survey.
The scenarios featured three versions of the robot
trainer, differing in their level of anthropomorphic
appearances. In the studies discussed above, robotic
anthropomorphism is expressed mainly through
facial expressions and gestures. Therefore, the three
versions of the robot trainer included one with
human-like body structure and expressions, one with
only expressions, and one with none of the two
factors, to represent high, medium and low levels of
anthropomorphism in robot form design (See Table
1). A small survey was conducted as a manipulation
check, to verify whether participants experienced the
three representations as differing. in terms of
anthropomorphism.
Table 1: Robot trainer designs.
Human-like
body
structure
x
x
Human-like
expression
x
Level of
anthropomo
rphism
High
Medium
Low
4.2 Study One Set-up
We first conducted a between subject study. Three
groups of participants were presented a survey
HEALTHINF 2019 - 12th International Conference on Health Informatics
32

containing the scenario on rehabilitation training,
each with a different form design for the robot trainer.
We used the Negative Attitude towards Robot
Scale (NARS) questionnaire (Nomura et al., 2004) at
the beginning of the survey to acquire participants’
general attitude towards social robots and to check
whether these were distributed equally over the three
groups. Then, the participants were presented the
scenario. After having experienced the scenario, we
took the Credibility/ Expectancy questionnaire
(Devilly and Borkovec, 2000) and the Technology
Acceptance Model (TAM) questionnaire to evaluate
the participants’ acceptance of the robot assisted
therapy and the robot trainer. At the end of the survey,
we asked the user to rate the look of the robot trainer
on a 10-point Machine-like to Human-like scale for a
manipulation check. The structure of the study is
presented in Table 2.
Table 2: Structure of Study One.
Screening questions
General attitude towards social robots
NARS questionnaire
Open question regarding attitude towards working
with social robots
Scenario “Lisa’s Rehabilitation Training Session with
Robot Trainer”
Attitude towards robot-assisted Rehabilitation
therapy
Credibility/Expectancy questionnaire
Open question regarding attitude towards
robot-assisted rehabilitation therapy
Attitude towards robot trainer in rehabilitation
therapy
TAM questionnaire
Open question regarding attitude towards robot
trainer in rehabilitation therapy
Manipulation check
Rate Robot Trainer’s look on a scale from Machine-like
to Human-like
Open question regarding attitude towards
robot-assisted rehabilitation therapy
4.3 Study Two Set-up
Study two was conducted with a within-subject
design. It presented the same scenario as study one,
but replaced the robot trainer with a blank box. After
participants read through the scenario, we presented
all three robot trainer concepts as available options
and ask them to pick the one they preferred, assuming
they were the patient in the scenario. We then
provided open questions for the participants to give
feedback on the reason of their choice and possible
improvements for the concept of their choice. Finally,
we asked participants to rate all three concepts of the
robot trainer on a ten-point rating scale from
“Machine-like” to “Human-like”. The detailed
structure is of study two is presented in Table 3.
Table 3: Structure of Study Two.
Screening Questions
Scenario “Lisa’s Rehabilitation Training Session with
Robot Trainer” with the trainer left blank
User preference for the given concept
Choose the desired robot trainer from the three given
concepts
Open questions regarding the choice
Open questions about further improvements for the
therapy and the robot trainer
Manipulation check
Rate three Robot Trainers’ look on a scale from
Machine-like to Human-like respectively
4.4 Participants
Participants were recruited through a crowdsourcing
platform for both studies. Participants were expected
to have been (formerly) involved in physical
rehabilitation training. The study involved four
groups of participants (total pool N = 103 after
screening, average age 37). Detailed numbers of
participants and group allocations are listed in Table
4. Study one and two were published on Amazon
Mechanical Turk on July 12, 2018 and lasted 14 days.
Each participant spent around 10 minutes on the
study. Based on the minimum hourly wage, the
reward was set at 1.5 USD.
To ensure the quality of the answers collected, we
set a three-step screening scheme. Firstly, workers on
Amazon Mechanical Turk had to answer three
questions, proving that they had experience in
physical rehabilitation, to access the survey.
Secondly, four reverse questions (changing positive
statements into negative ones, e.g. “I found the robot
trainer easy to interact with” into “I found the robot
trainer difficult to interact with”) were also planted
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation
33
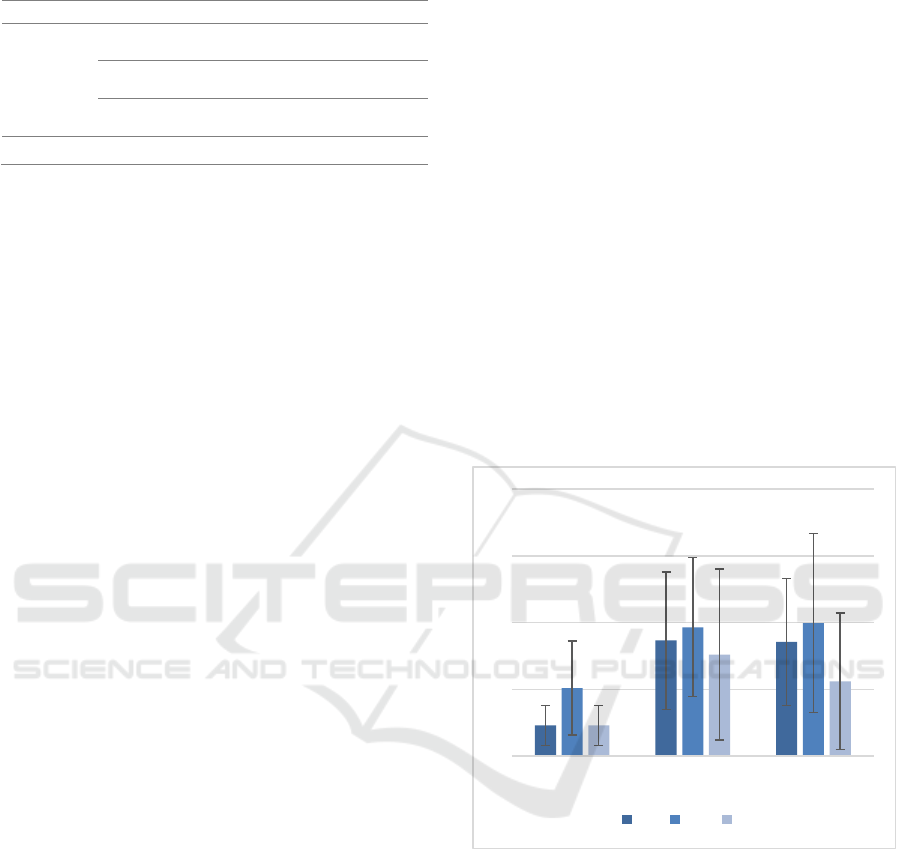
Table 4: Study participants.
Study
Conditions
Participants
Study One
HA (High
Anthropomorphism)
28 (HA1 - HA28)
MA (Medium
Anthropomorphism)
24 (MA1 - HA24)
LA (Low
Anthropomorphism)
20 (LA1 - LA20)
Study Two
-
31 (ST1 - ST31)
within the survey to check for satisficing behavior in
answering the survey. Lastly, we put an eight-digit
password at the end of the survey for claiming the
reward, only visible to participants who finished the
survey. We set the survey to be only available to
workers with approval rate higher than 97% percent
and job experience less than 5000 to further ensure
the quality of the answer.
4.5 Analysis
Quantitative data were analyzed through mean scores
for all conditions as an indicator of general
acceptance. Additionally, through one-way ANOVA
tests, we analyzed the effect of anthropomorphism on
the patient’s acceptance for SAR assisted
rehabilitation therapy and robot trainer technology.
We conducted a closed coding and an open coding
analysis on the qualitative data. The closed coding
scheme was applied to the data from Study One, and
consisted of the factors from the
Credibility/Expectancy and TAM questionnaires,
namely: Credibility, Expectancy, Perceived Ease of
Use (PEU), Perceived Usefulness (PU), Behavioral
Intention (BI), Attitude (A), Self-Efficacy (SE) and
Subjective Norm (SN).
Next, we combined the qualitative data from
Study One and Study Two and conducted an
inductive open coding analysis to generalize more
insights.
5 FINDINGS
We present our findings regarding three topics: 1)
general attitude towards SARs, 2) Acceptance of
SAR assisted rehabilitation therapy and robot trainer,
and 3) effects of anthropomorphism on the
acceptance of SAR assisted rehabilitation therapy and
robot trainer.
5.1 General Attitude towards Socially
Assistive Robots
With the NARS questionnaire, we tested Study One’s
participants’ negative attitude towards situations of
interaction with robots, social influence of robots and
emotional interaction with robots. One-way ANOVA
analysis showed that there are no significant
differences among the three groups for Factor 1
(Negative Attitude towards Situations of Interaction
with Robots) (F (2,68) = 2.83, ns), Factor 2 (Negative
Attitude towards Social Influence of Robots) (F
(2,68) = .69, ns), and Factor 3 (Negative Attitude
towards Emotions in Interaction with Robots) (F
(2,68) = 2.97, ns). This suggests that the three groups
have a similar attitude towards socially assistive
robots. The mean scores for the three groups and for
all three factors are under 3. Since NARS is a negative
attitude questionnaire, these lower scores suggest a
rather positive attitude towards the factors (see Figure
2).
Figure 2: Mean score of the three groups from Study One
for the three NARS factors.
Open coding analysis highlighted that robotic
technology is desired for its precision, being
objective, convenience, efficiency, opening up
possibilities for more privacy and eliminating
negative social encounters. Negative opinions
clustered around technological possibilities, and
cultural and ethical concerns. Below are the two
factors concerning acceptance for SARs.
5.1.1 Technological Status-quo
“I think it has the potential to be very interesting and
constructive, but hasn't been fully developed” (HA7)
1
2
3
4
5
Factor 1 Factor 2 Factor 3
HA MA LA
HEALTHINF 2019 - 12th International Conference on Health Informatics
34
“I might feel alone working with robot as robots don't
have cognitive behavior” (MA12)
7 quotes suggested robots are best suited for the
kind of jobs that are simple, repetitive and do not need
complicated judgment. In the participants’ opinions,
current robotic-related technologies still lack
flexibility to handle emergencies and lack proper
judgement for complex situations. Such technological
reality proposed a limitation for participants in terms
of the tasks assumed possible for robots to take on.
5.1.2 Issues of Technology-related Attitude
and Beliefs
“Not comfortable. Humans are losing the ability to
think and react without assistance.” (HA21)
“Not a fan, I can see the appeal, but I'm sure if
there is a living person who needs the money.” (LA6)
This refers to current cultural opinions about the
relationship between people and technology.
Participants regard certain human characteristics as
irreplaceable (e.g., empathy, social perception, etc.),
and worry that humans will be weakened and end up
in an inferior position compared to technology in the
future. The scenarios evoked a sense of anxiety about
human identity among respondents. A recent study
suggested that the anthropomorphic appearances of a
social robot can pose a threat to human
distinctiveness (Ferrari et al., 2016). In this sense,
anthropomorphism can trigger these negative
emotions, and should thus be considered in design
decisions.
Figure 3: Mean scores of three groups for Credibility and
Expectancy.
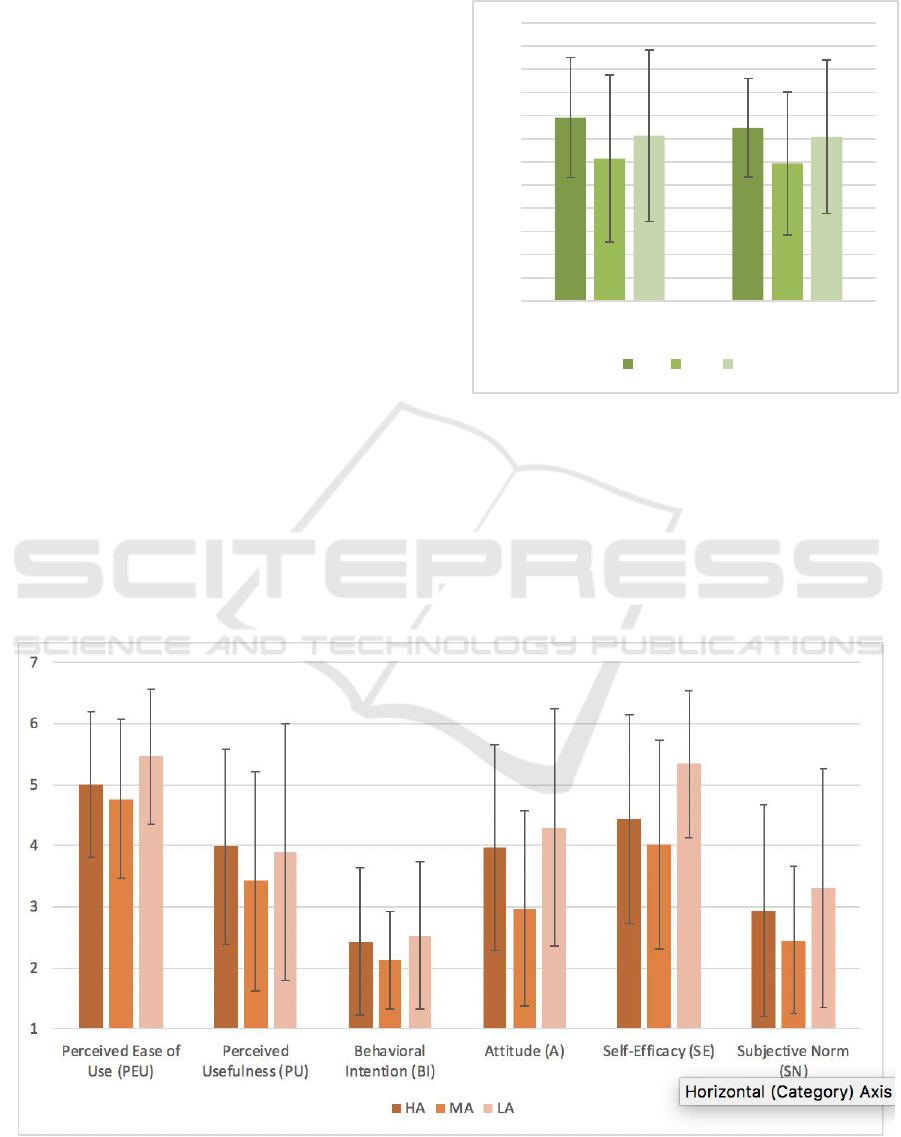
Figure 4: Means scores of TAM questionnaire.
3
5
7
9
11
13
15
17
19
21
23
25
27
Credibility Expectancy
HA MA LA
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation
35
5.2 Acceptance of SAR in
Rehabilitation Therapy and as
Robot Trainer
The Credibility/Expectancy questionnaire was used
in Study One to evaluate how much patients believe
and how much they feel that the social robot can be
an effective aid during rehabilitation training. This
questionnaire has a two-factored structure, three
items are used for each, two of them are nine-point
Likert scales, and the third is a scale from 0 to 100.
The latter is converted to a nine-point scale by
dividing by 12,5 and adding 1. The subscale items are
added resulting in two aggregate scores ranging
between from 3-27 for credibility and for expectancy
respectively, with 15 as the midpoint of the scale. The
mean scores for the three groups show that
participants for conditions HA and LA have positive
opinions on the credibility (HA: M=18.82, SD=5.18,
LA: M=17.26, SD=7.4) and expectancy (HA:
M=17.95, SD=4.26, LA: M=17.16, SD=6.64) of the
training, and participants for condition MA have
neutral scores for credibility (M=15.30, SD=7.21)
and expectancy (M=14.87, SD=6.18), as visible in
Figure 3.
The TAM questionnaire was used to measure the
acceptance of the robot trainer. The results suggest
that participants perceive the robot trainer as easy-to-
use (PEU & SE), have a neutral attitude towards the
concept (A) and are neutral with regards to its
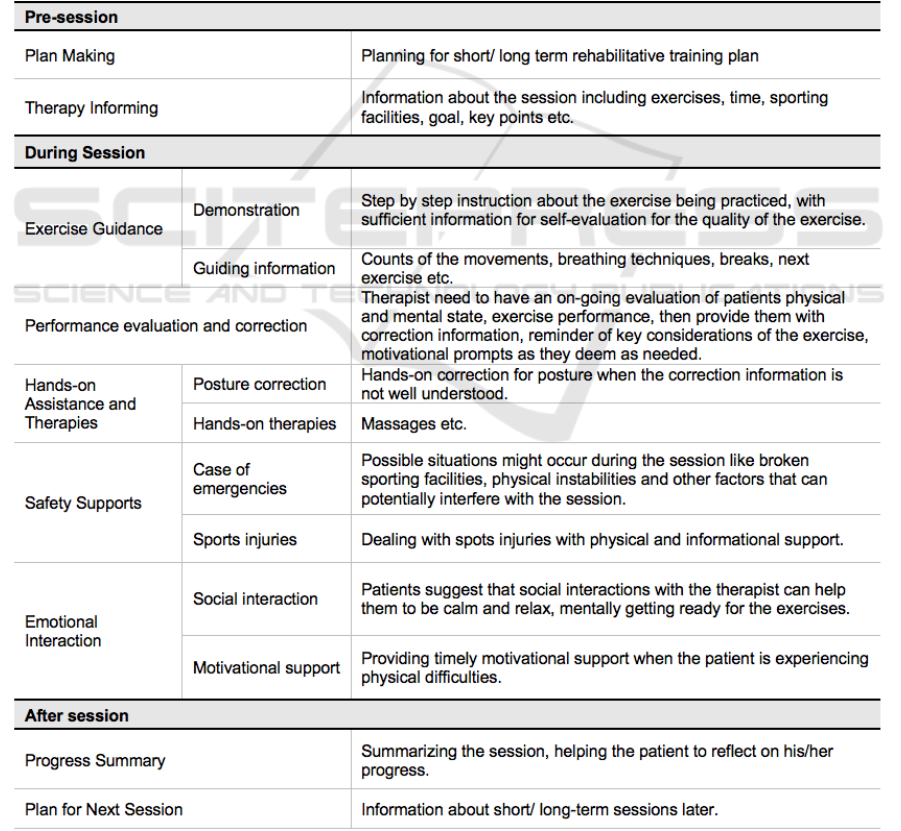
Table 5: Patient Needs for SAR-Assisted Rehabilitation Therapy.
HEALTHINF 2019 - 12th International Conference on Health Informatics
36

perceived usefulness (PU). Finally, participants have
a below average mean score for the factors
behavioural intention (BI) and subjective norm (SN)
(see Figure 4).
5.2.1 Patients’ Needs for SAR-assisted
Rehabilitation Training
From analyzing the qualitative data, a section labeled
“Patient Needs” emerged. Due to the limited contents
of the scenario provided, participants were left with
doubts about services they considered important in
their own rehabilitation therapies, but which were not
shown in the scenario. Over 100 quotes were
collected and summarized into 9 categories of needs
presented in Table 5.
5.2.2 Perceived Benefits of SAR-assisted
Rehabilitation Training
“My own rehabilitation therapy was with a human,
but it accomplished the same purpose.” (HA17)
Mean scores of Credibility/Expectancy
questionnaire show that participants have above
average expectations from the rehabilitation therapy
provided by a robot trainer.
Self-directed practice is considered to be an
important component in rehabilitation therapy
(Winkle et al., 2018). Quotes from the questionnaire
confirmed that the process is mostly done by the
patient him- or herself, and demands consistency and
certain quantity. To this end, participants have
confidence in having a robot trainer providing
guidance, feedback and motivational prompts.
Participants also mentioned the following additional
benefits a robot trainer could bring about:
1. Providing Stable and Basic Services and
Eliminating Human Errors and Interference.
“The facility I used insisted their doctor see me. He
(the therapist) ignored my doctor's orders. This
(robot trainer) would prevent that from happening.”
(MA19)
“I wouldn't feel judged while doing it. It seems
positive and reassuring.” (HA15)
Some participants mentioned their rehabilitation
experience, during which, there were moments that
they felt neglected, misdiagnosed or given the wrong
instructions and being interrupted by inappropriate
social interactions. These participants believed a
robot trainer to be more goal-oriented, therefore
enabling them to better focus on the training exercise
and eliminating possible human errors.
2. Financial Benefits and Cost Effectiveness.
“My experience was that they were interested in what
they could get from insurance, my needs were not.”
(HA18)
“Development of at-home exercises that can be
performed without purchasing expensive equipment
needed” (LA9)
Cost efficiency and flexibility brought by a robot
trainer were expected by the participants, suggesting
tele-rehabilitation is one of the most promising usage
cases that can be developed for robot trainer.
5.2.3 Concerns about SAR-assisted
Rehabilitation Therapy
Concerns primarily focused on 1) how the robot will
make up for the loss of human specific values in
rehabilitation therapy e.g. empathy, perceptions on
the patients and the overall rehabilitation training
based on experience and expertise, and capability of
dealing with emergencies, 2) the normally
included/expected therapies that are not shown in the
scenario, e.g. massages, hands-on corrections, real-
time demonstrations and exercise walk-through, and
3) the loss of social and emotional interactions. When
it comes to evaluating patients’ training performance,
providing emotional support and dealing with
emergencies and safety issues, participants remained
concerned. The concerns centered on the participants’
lack of trust in the robot trainer, since it does not have
empathy towards the patient. Furthermore, patients
doubted whether the motivational prompts would be
perceived as sincere, or just pre-programmed
prompts.
5.3 Anthropomorphism and
Acceptance
Participants were asked to rate the look of the robot
on a ten-point rating scale (0 = machine-like, 9 =
human-like), as a manipulation check to ensure the
independent variable — in this case the
anthropomorphism level of the robot trainer — was
perceived as intended. The scores in both studies
turned out to be as intended. For study one, a one-way
ANOVA analysis showed the perceived human-
likeliness of the high anthropomorphic concept
(M=4.28, SD=1.77), medium anthropomorphic
concept (M=2.96, SD=2.33) and low
anthropomorphic concept (M=.70, SD=1.03) were
significantly different, F (2-70) =22.79, p<.001. In
study two the three concepts were all shown to every
participant at the same time. Participants were asked
to rate all three concepts on anthropomorphism. One-
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation
37

way ANOVA analysis also shows a significant
difference between the ratings of human-likeliness (F
(2,89) = 121.34, p<.001) between the three versions
(HA:M=6.67, SD=1.79, MA:M=3.1, SD=1.4,
LA:M=.48, SD=1.46).
A one-way ANOVA analysis showed no
significant effect of anthropomorphism on the
credibility (F (2,68) = 1.89, ns) and expectancy (F
(2,68) = 2.02, ns) of the SAR-assisted rehabilitation
therapy.
A similar analysis on the outcomes of the TAM
questionnaire found a significant preference for the
low anthropomorphic concept (M = 5.34, SD = 1.2),
over the high anthropomorphic (M = 4.43, SD = 1.71)
and the medium anthropomorphic concept (M = 4.02,
SD = 1.7) on the factor Self-Efficacy (SE), F (2,68) =
3.8, p < .05. No significant effects of
anthropomorphism were found for the factors
Perceived Ease of Use (PEU, F (2,68) = 1.84, ns),
Perceived Usefulness (PU, F (2,68) = .7, ns),
Behavioural Intention (BI, F (2,68) = .27, ns),
Attitude (A, F (2,68) = 3.03, ns) and Subjective Norm
(SN, F (2,68) = 1.15, ns).
In Study Two, participants were asked to choose
their preferred version of the robot trainer.
Participants preferred the high anthropomorphic
concept (17 out of 31), followed by the medium
anthropomorphic concept (9/31) and low
anthropomorphic concept (5/31). 13 quotes indicated
that the human-likeliness was the reason for choosing
the high anthropomorphic concept, 7 quotes because
it looks warm and feels personal, and 6 quotes
because it seems most able to provide a better and
more varied service. Reason for participants who
chose one of the other two concepts were 1)
participants feel safe around them, 2) participants are
unfamiliar with the high anthropomorphic concept,
not knowing what to expect, and 3) a robot trainer
with high anthropomorphic appearance, but only
voice interaction, is considered unintelligent. A low
anthropomorphic robot trainer offering the same
interaction was deemed realistic within the current
situation. In line with this reasoning, a unique group
of quotes appeared for the high anthropomorphism
concept. These 15 quotes inquired whether the robot
would provide hands-on training assistance. This
highlights a potential link between the robot’s
appearance and users’ expectations about its
functionality.
All three concepts got quotes suggesting to make
the robot trainer more human-like rather than
machinelike, which indicates a preference for high
anthropomorphic SARs for rehabilitation training
(see Figure 5). Interestingly, most of these quotes
were proposed in relation to the most
anthropomorphic concept.
Figure 5: Number of Quotes for Desired
Anthropomorphism Level.
6 DESIGN IMPLICATIONS
6.1 Managing Form Factor and
Patient’s Expectations
Patient’s expectations are related to their impressions
of the robot trainer, and were found to affect patients
perceived self-efficacy toward the robot trainer. The
form design of the should fit the task that will be
performed, as the form factor of the trainer is
indicative for the patients to assume the service that
will be offered. Therefore, the form design of the
robot trainer should be referred to the task assigned to
it, and made easy for patients to have a realistic
expectation and a positive opinion.
6.2 Connecting to Wearable
Technologies
One of the participants’ major concerns is the quality
of the feedback given by the robot trainer. Also, trust
is a crucial issue in a medical context. The use of
wearable technologies has the potential for dealing
with both issues. Data like heart rate, perspiration,
body posture, speed, muscle tension and more can
provide a more comprehensive understanding of the
training condition of the patient (Beckerle et al.,
2017), giving a more accrete and timely
understanding of the situation in progress.
Furthermore, being able to see the instrument of
measuring would help in explaining and specifying
the process and content of user data collection,
27
6
17
2
10
0
0
10
20
30
40
50
60
Human-Like Machine-Like
HA MA LA
HEALTHINF 2019 - 12th International Conference on Health Informatics
38

therefore facilitating better trust in SAR-assisted
rehabilitation therapy.
6.3 Allowing Emotional Input for
Tailored Experience
A physiotherapist is always able to pick up emotional
conditions of the patient, therefore can select the
suitable motivational prompts accordingly. Being
able to acquire and respond appropriately to a
patient’s emotional condition can better help to tailor
the experience offered, and can help to fast-forward
the adaptation phase, where the robot trainer has to
learn about the patient.
7 LIMITATIONS OF CURRENT
STUDY
The main limitations pertain to the nature of the
materials presented to participants (sketches and
scenarios) and the sampling approach
(crowdsourcing). The attitudes expressed are based
on imagined experiences based on very limited
stimuli. More extensive and realistic exposure to a
robot acting as a coach in rehabilitation therapy
would provide higher confidence in the results found,
and further study will also shift focus to elder groups
which fits better with rehabilitation context. Second,
with crowdsourcing one is constrained to the
crowdsourcing platform as a sampling frame. This
allows surveys that cover different geographical
areas, but the sample may be skewed to people very
familiar with internet technology. Further, there could
be potential for more satisficing behaviors from
crowd workers interested to earn the reward rather
than provide good data. On the upside,
methodological research has shown that
crowdsourcing can be effective and valid approach
for accessing participants and that crowd workers can
actually be more motivated to provide good quality
answers(Stewart et al., 2017). Moreover, suitable
checks were made to check on the quality of the data
in accordance to the screening process and verifying
reversed questions.
8 CONCLUSION
This work explores of patients’ acceptance for
socially assistive robot in rehabilitation settings, and
the use anthropomorphic form factor in robotic design
in this context. We discovered that 1) participants
have a neutral to positive attitude towards SARs and
it’s use in rehabilitation therapy as trainer, 2) the SAR
technology in therapies is regarded easy to use but
participants generally lack intention for using the
system, which is possibly due to unfamiliarity with
SARs and lack of trust for them, 3) the level of
anthropomorphism has an effect on patients’ self-
efficacy and attitude for the robot trainer, a potential
link exists between SAR form factor and user
expectation for its service, 4) high anthropomorphic
concept is generally preferred. As we found out, to
bring SAR into rehabilitation therapies, much work is
yet to be done in solving patient concerns, improving
the quality of the therapy and developing detailed
personalized motivational strategies. Further studies
should replicate and elaborate these results while
exposing patients to more realistic experiences of
social-robot assisted rehabilitation therapy and
include proximal (non-crowdsourced) studies with
actual patients.
REFERENCES
Bartneck, C., Bleeker, T., Bun, J., Fens, P., Riet, L. (2010)
'The influence of robot anthropomorphism on the
feelings of embarrassment when interacting with
robots'. Paladyn, Journal of Behavioral Robotics, 1(2).
Beckerle, P., Salvietti, G., Unal, R., Prattichizzo, D., Rossi,
S., Castellini, C., Bianchi, M. (2017) ' A Human–Robot
Interaction Perspective on Assistive and Rehabilitation
Robotics', Frontiers in Neurorobotics, 11.
Cardona, M., Destarac, M. A., Garcia, C. E. (2017)
'Exoskeleton robots for rehabilitation: State of the art
and future trends In' 2017 IEEE 37th Central America
and Panama Convention (CONCAPAN XXXVII)
Managua: IEEE, pp. 1–6.
Choi, J., Kim, M. (2008) 'The Usage and Evaluation of
Anthropomorphic Form in Robot Design', 15.
Devilly, G. J., Borkovec, T. D. (2000) 'Psychometric
properties of the credibility/ expectancy questionnaire',
14.
Ding, Y., Galiana, I., Asbeck, A. T., De Rossi, S. M. M.,
Bae, J., Santos, T. R. T., … Walsh, C. (2017)
'Biomechanical and Physiological Evaluation of Multi-
Joint Assistance With Soft Exosuits' IEEE Transactions
on Neural Systems and Rehabilitation Engineering,
25(2), 119–130.
Epley, N., Waytz, A., Cacioppo, J. T. (2007) 'On seeing
human: A three-factor theory of anthropomorphism'
Psychological Review, 114(4), 864–886.
Eriksson, J., Mataric, M. J., Winstein, C. J. (2005) 'Hands-
Off Assistive Robotics for Post-Stroke Arm
Rehabilitation' In 9th International Conference on
Rehabilitation Robotics, 2005. ICORR 2005. Chicago,
IL, USA: IEEE, pp. 21–24.
How Anthropomorphism Affects User Acceptance of a Robot Trainer in Physical Rehabilitation
39

Eyssel, F., Kuchenbrandt, D., Bobinger, S. (2012) ‘If You
Sound Like Me, You Must Be More Human’: On the
Interplay of Robot and User Features on Human- Robot
Acceptance and Anthropomorphism, 2.
Feil-Seifer, D., Mataric, M. J. (2005) 'Socially Assistive
Robotics' In 9th International Conference on
Rehabilitation Robotics, 2005. ICORR 2005. Chicago,
IL, USA: IEEE, pp. 465–468.
Ferrari, F., Paladino, M. P., Jetten, J. (2016) 'Blurring
Human–Machine Distinctions: Anthropomorphic
Appearance in Social Robots as a Threat to Human
Distinctiveness' International Journal of Social
Robotics, 8(2), 287–302.
Feys, P., Coninx, K., Kerkhofs, L., De Weyer, T., Truyens,
V., Maris, A., Lamers, I. (2015) 'Robot-supported upper
limb training in a virtual learning environment: a pilot
randomized controlled trial in persons with MS' Journal
of NeuroEngineering and Rehabilitation, 12(1), 60.
Fong, T., Nourbakhsh, I., Dautenhahn, K. (2003) 'A survey
of socially interactive robots' Robotics and Autonomous
Systems, 42(3–4), 143–166.
Gockley, R., Mataric, M. J. (2006) 'Encouraging physical
therapy compliance with a hands-Off mobile robot' In
Proceeding of the 1st ACM SIGCHI/SIGART
conference on Human-robot interaction - HRI ’06 Salt
Lake City, Utah, USA: ACM Press, pp. 150.
Heerink, M., Kröse, B., Evers, V., Wielinga, B. (2010)
'Assessing Acceptance of Assistive Social Agent
Technology by Older Adults: the Almere Model'
International Journal of Social Robotics, 2(4), 361–
375.
Klamer, T., Allouch, S. B. (2010) 'Acceptance and use of a
social robot by elderly users in a domestic environment'
IEEE.
Kyong Il Kang, Freedman, S., Mataric, M. J., Cunningham,
M. J., Lopez, B. (2005) 'A Hands-Off Physical Therapy
Assistance Robot for Cardiac Patients' In 9th
International Conference on Rehabilitation Robotics,
2005. ICORR 2005. Chicago, IL, USA: IEEE, pp. 337–
340.
Laut, J., Porfiri, M., Raghavan, P. (2016) 'The Present and
Future of Robotic Technology in Rehabilitation'
Current Physical Medicine and Rehabilitation Reports,
4(4), 312–319.
Moosaei, M., Das, S. K., Popa, D. O., Riek, L. D. (2017)
'Using Facially Expressive Robots to Calibrate Clinical
Pain Perception' In Proceedings of the 2017 ACM/IEEE
International Conference on Human-Robot Interaction
- HRI ’17 Vienna, Austria: ACM Press, pp. 32–41.
Nomura, T., Kanda, T., Suzuki, T., Kato, K. (2004)
'Psychology in human-robot communication: an
attempt through investigation of negative attitudes and
anxiety toward robots' IEEE, pp. 35–40.
Popescu, N., Popescu, D., Ivănescu, M. (2016) 'Intelligent
Robotic Approach for After-stroke Hand
Rehabilitation' In Proceedings of the 9th International
Joint Conference on Biomedical Engineering Systems
and Technologies. Rome, Italy: SCITEPRESS -
Science and Technology Publications, pp. 49–57.
Salem, M., Eyssel, F., Rohlfing, K., Kopp, S., Joublin, F.
(2013) 'To Err is Human(-like): Effects of Robot
Gesture on Perceived Anthropomorphism and
Likability' International Journal of Social Robotics,
5(3), 313–323.
Siegel, M., Breazeal, C., Norton, M. I. (2009) 'Persuasive
Robotics: The influence of robot gender on human
behavior' In 2009 IEEE/RSJ International Conference
on Intelligent Robots and Systems. St. Louis, MO,
USA: IEEE, pp. 2563–2568.
Stewart, N., Chandler, J., Paolacci, G. (2017)
'Crowdsourcing Samples in Cognitive Science' Trends
in Cognitive Sciences, 21(10), 736–748.
Tapus, A., Mataric, M. J. (2008) 'Socially Assistive Robots:
The Link between Personality, Empathy, Physiological
Signals, and Task Performance' 9.
Vitiello, N., Mohammed, S., Moreno, J. C. (2017) 'Guest
Editorial Wearable Robotics for Motion Assistance and
Rehabilitation' IEEE Transactions on Neural Systems
and Rehabilitation Engineering, 25(2), 103–106.
Winkle, K., Caleb-Solly, P., Turton, A., Bremner, P. (2018)
'Social Robots for Engagement in Rehabilitative
Therapies: Design Implications from a Study with
Therapists' In Proceedings of the 2018 ACM/IEEE
International Conference on Human-Robot Interaction
- HRI ’18. Chicago, IL, USA: ACM Press, pp. 289–297.
Zaga, C., de Vries, R. A. J., Li, J., Truong, K. P., Evers, V.
(2017) 'A Simple Nod of the Head: The Effect of
Minimal Robot Movements on Children’s Perception
of a Low-Anthropomorphic Robot' In Proceedings of
the 2017 CHI Conference on Human Factors in
Computing Systems - CHI ’17, Denver, Colorado, USA:
ACM Press, pp. 336–341.
HEALTHINF 2019 - 12th International Conference on Health Informatics
40
