
Surgical Phase Recognition of Short Video Shots based on Temporal
Modeling of Deep Features
Constantinos Loukas
Medical Physics Lab, Medical School, National and Kapodistrian University of Athens,
Mikras Asias 75 str., Athens, Greece
Keywords: Surgery, Video, Classification, CNN, LSTM, Deep Learning.
Abstract: Recognizing the phases of a laparoscopic surgery (LS) operation form its video constitutes a fundamental
step for efficient content representation, indexing and retrieval in surgical video databases. In the literature,
most techniques focus on phase segmentation of the entire LS video using hand-crafted visual features,
instrument usage signals, and recently convolutional neural networks (CNNs). In this paper we address the
problem of phase recognition of short video shots (10s) of the operation, without utilizing information about
the preceding/forthcoming video frames, their phase labels or the instruments used. We investigate four
state-of-the-art CNN architectures (Alexnet, VGG19, GoogleNet, and ResNet101), for feature extraction via
transfer learning. Visual saliency was employed for selecting the most informative region of the image as
input to the CNN. Video shot representation was based on two temporal pooling mechanisms. Most
importantly, we investigate the role of ‘elapsed time’ (from the beginning of the operation), and we show
that inclusion of this feature can increase performance dramatically (69% vs. 75% mean accuracy). Finally,
a long short-term memory (LSTM) network was trained for video shot classification, based on the fusion of
CNN features and ‘elapsed time’, increasing the accuracy to 86%. Our results highlight the prominent role
of visual saliency, long-range temporal recursion and ‘elapsed time’ (a feature ignored so far), for surgical
phase recognition.
1 INTRODUCTION
Laparoscopic surgery (LS), a common type of
minimally invasive surgery (MIS), provides not only
substantial therapeutic benefits for the patient, but
also the opportunity to record the video of the
operation for reasons such as documentation,
technique evaluation, skills assessment, and
cognitive training of junior surgeons (Loukas et al.
2011),(Lahanas et al. 2011). However, a major
technological challenge is the effective content
management of the recorded videos, given that an
operation may last for more than an hour, whereas
the duration of yearly operations per surgeon may
exceed 1000 hours (Petscharnig and Schöffmann
2018).
The traditional way of classifying/retrieving
videos relevant to a particular feature of the
operation is via text mining from manual
annotations. Apart from the operation type, the
annotation may include keywords such as a special
technique performed, anatomic characteristics, or
instruments utilized. However, this type of labelling
has some limitations, preventing the effective
management, representation and indexing of the
recorded videos. First, manual annotation is tedious
and time-consuming. Second, semantic
characteristics that are discovered to be of the
surgeon’s interest at a later stage, are excluded from
future searches. Third, global annotation of terms
provides limited information about their time-stamp,
unless this is manually inserted. In most cases, the
surgeon performs manual skimming of the video to
locate the object/event of interest, which is
inefficient. In order to provide surgeons with
additional tools for video content management, an
effective way for video content representation is
essential.
Automated surgical phase recognition from the
LS video is an important topic of research, usually
defined as ‘surgical workflow analysis’ (SWA). The
phases of a surgical operation constitute its
fundamental temporal units, where the surgeon
attempts to complete an overall task before
Loukas, C.
Surgical Phase Recognition of Short Video Shots based on Temporal Modeling of Deep Features.
DOI: 10.5220/0007352000210029
In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2019), pages 21-29
ISBN: 978-989-758-353-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
21

Figure 1: An overview of the 8 surgical phases (P1-P8). The frames were extracted from the annotations of a single LC
operation.
advancing to the next phase. During the phase, the
surgeon manipulates certain anatomic tissues with
the surgical instruments, some of which may be
specific to its label. Surgical phases are of crucial
importance for the structure of the operation as they
correspond to the top hierarchy level according to
the ‘operation decomposition’ model: phases, steps,
tasks/events, and gestures, as described in a recent
review (Loukas 2018). Hence, a method able to
recognize the phase of a surgical operation would
offer solutions to various challenges encountered in
surgical video content management systems. Other
applications include phase-based skills assessment,
automatic selection of didactic content, and
improved OR scheduling (if phase recognition is
performed online).
Initial SWA works employed tool usage signals
from RFID and electromagnetic (EM) sensors as
well as manual annotations, based on the hypothesis
that a surgical phase is characterized by a certain
hand gesture or/and tool usage pattern (Loukas and
Georgiou 2013),(Bouarfa et al. 2011),(Padoy et al.
2012). However, employment of additional sensors
may interfere with the operational workflow and
there are concerns whether these data can be
automatically acquired in the operating room.
Visual features extracted from the recorded video
of the operation seem a more straightforward option
due to the endoscopic camera employed. Compared
to endoscopic examinations, surgical videos present
significant challenges such as presence of smoke
(coagulation), heavy interaction with the operated
organs (dissection/clipping/cutting), and frequent
camera motion as well as tool insertion/removal.
Prior works on vision-based phase recognition
included hand-engineered features based on color,
texture, intensity gradients, or combinations of them
(Lalys et al. 2012). In (Blum et al. 2010), gradient
magnitudes, histograms and color values were
employed. After dimensionality reduction based on
tool usage signal data, laparoscopic cholecystectomy
(LC) operations were segmented into 14 phases with
accuracy close to 77%. The combination of visual
features with tool usage signals was also employed
in (Dergachyova et al. 2016). In another study,
phase border detection of LC videos was performed
via image-based instrument recognition (Primus et
al. 2016).
The aforementioned works employ handcrafted
features, which are specifically designed to capture
certain type of information ignoring other image
characteristics. Recently, deep learning approaches
(e.g. Convolutional Neural networks-CNNs) have
shown promising results for phase recognition. For
example, Twinanda et al. proposed the EndoNet
architecture, a CNN based on the AlexNet
architecture, which was fine-tuned on a dataset of 40
LC operations for the task of tool and phase
recognition (Twinanda et al. 2017). The precision of
offline and online phase recognition was close to
85% and 74% respectively. In the recent M2CAI
2016 challenge for online phase recognition of LC
operations, Jin et al. achieved a mean jaccard score
of 78.2% (the challenge allowed a 10s margin in the
predictions). Their method combined feature vectors
extracted from a fine-tuned ResNet50 CNN
architecture combined with a long-short term
memory (LSTM) network to encode temporal
information (Jin et al. 2018). These works focus on
the online segmentation of the entire operation based
on fully supervised training and using visual
information from the preceding video frames as well
as their inferred phase labels. Recently, a CNN-
based method for video shot classification of
laparoscopic gynecologic actions was proposed in
(Petscharnig and Schöffmann 2017). Video shots of
BIOIMAGING 2019 - 6th International Conference on Bioimaging
22
the entire course of each surgical action were
employed for training and testing.
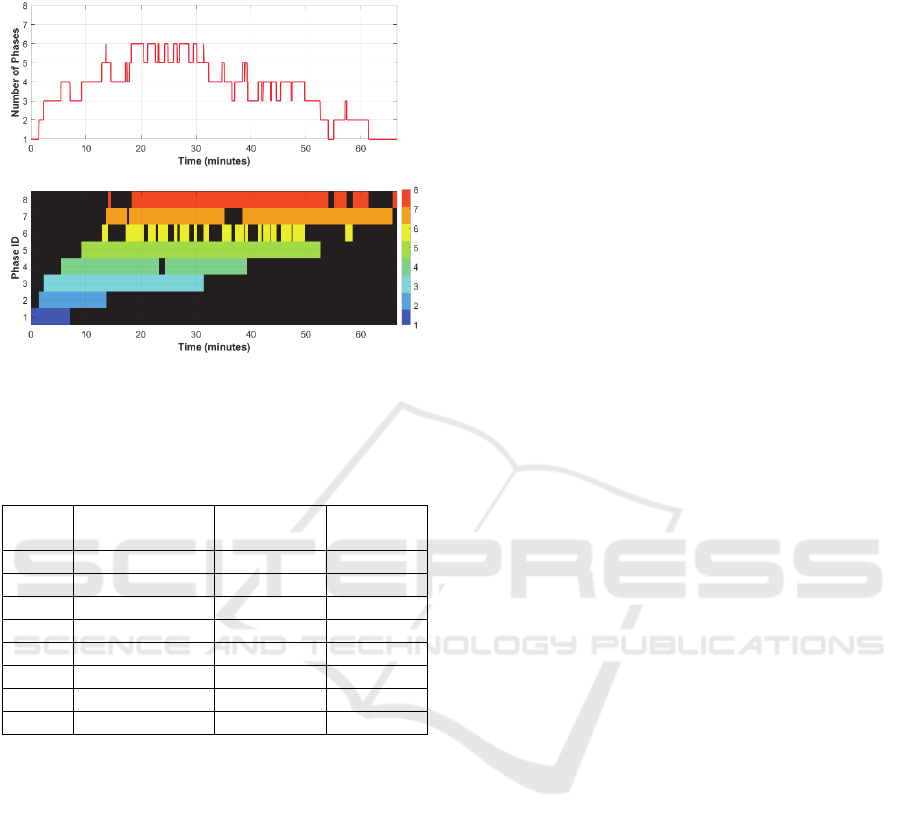
Figure 2: Graphical overview of the number of
simultaneously occurring phases (top) and the temporal
span of each phase (bottom), across the dataset of 27
surgical operations.
Table 1: Statistical overview of the phases.
Phase
ID
mean ± std
(minutes)
min
(minutes)
max
(minutes)
P1 3.04 ± 1.70 1.42 7.08
P2 1.71 ± 2.06 0.35 11.03
P3 10.53 ± 7.97 1.95 26.82
P4 4.70 ± 2.87 0.94 12.39
P5 10.40 ± 6.30 1.68 24.11
P6 1.14 ± 0.59 0.28 3.03
P7 5.68 ± 2.80 1.01 15.97
P8 4.93 ± 5.61 0.66 22.26
In this paper we present a method for phase
recognition from short video shots (10s) of surgical
operations, without any prior knowledge about the
preceding/forthcoming video frames, phase labels or
instruments used. We concentrated on LC which is a
fundamental operation for junior surgeons. Each
video shot essentially represented only a small
fraction of the entire phase. Prompted by the
advances in image classification based on deep
learning approaches, we investigated four state-of-
the-art CNN architectures (Alexnet, VGG19,
GoogleNet, and ResNet101), for feature extraction
via transfer learning. Features were extracted from
two different types of receptive fields: one based on
traditional frame resize to match the CNN’s input
size and another one based on the most salient
region of the input image. Video shot representation
was performed via two temporal pooling
mechanisms. Initially, video shot classification was
based on the 1
st
nearest-neighbour (NN) using two
different distance metrics. Most importantly, we
investigated the role of absolute ‘elapsed time’ (from
the beginning of the operation), in video shot
classification and we present results that show that
the inclusion of this feature can increase
performance dramatically. Finally, we fused the
CNN features with ‘elapsed time’ and applied long-
range temporal recursion to estimate the probability
of each surgical phase for a video shot, which
improved even further the classification
performance.
2 METHODOLOGY
2.1 Video Shot Dataset
In this work we employed surgical videos from the
M2CAI 2016 Challenge Dataset, which includes
video recordings of complete LC operations
(Twinanda et al. 2017),(Stauder et al. 2016). In
particular, we analyzed 27 video recordings (about
19 hours total duration), from the ‘workflow-train’
sub-dataset. The videos are recorded at 25 frames
per second (25 fps), with full HD resolution
1920×1080. Each video includes frame-by-frame
annotations of the 8 surgical phases of LC: P1)
Trocar Placement, P2) Preparation, P3) Calot
Triangle Dissection, P4) Clipping & Cutting, P5)
Gallbladder Dissection, P6) Gallbladder Packaging,
P7) Cleaning & Coagulation, and P8) Gallbladder
Retraction. Sample frames of the surgical phases are
presented in Figure 1. It may be seen that some
phases may present distinct image characteristics
(e.g. P1, P8), whereas others (e.g. P5-P7) are quite
challenging for visual recognition due to their
similarity or/and presence of smoke (e.g. see P5, P6,
P7).
It should be emphasized that not all operational
phases are sequential and they are governed by some
temporal constraints: P6, P7, P8 are not always
sequential (P6 may occur after P7, or/and P7 after
P8), P7 may occur 2 times, and P7 may not be
present at all. However, phases P1-P5 are always
present in an operation and occur sequentially. A
statistical overview of the phases is presented in
Table 1. It may be seen that P2 and P6 have the
shortest duration whereas P3 and P5 have the
longest one.
Figure 2 shows the number of simultaneously
occurring phases as well as the timings of each
phase, across all 27 video recordings, in the same
diagram. From the top diagram it may be seen that
Surgical Phase Recognition of Short Video Shots based on Temporal Modeling of Deep Features
23

up to the first 10 minutes, about 1-3 phases may
occur (from P1-P4), and the same is valid after the
50th min (from P5-P8). From the bottom diagram it
may be seen that the order of the phases is relatively
fixed and their duration is limited (e.g. P1-P5).
Furthermore, some phases present almost no
temporal overlap (e.g. P1 vs. P4-P8 and P2 vs. P6-
P8), whereas some others present moderate overlap
(e.g. P1 vs. P3 and P2 vs. P5). From this analysis it
is evident that the absolute temporal position of a
video frame (with regard to the beginning of the
operation), is a crucial factor that should be
considered in phase recognition.
Based on the aforementioned dataset, we
extracted the video shot dataset which was employed
for classification. In particular, for each video and
for each of the 8 phases, we extracted 2 non-
overlapping shots of 10s duration (i.e. 250 frames).
The video shots were extracted from random
temporal positions of each phase, ensuring that the
first/last frame of each shot was within the temporal
limits of each phase. In two videos, P7 was absent so
in order to have an equal number of shots per phase,
we randomly selected 50 (out of 54) shots for each
of the P1-P6 and P8 phases, leading to a total
number of 400 video shots, equally distributed
across the 8 phases.
2.2 CNN Feature Extraction
Feature extraction was based on transfer learning
using ‘off-the-shelf’ features extracted from four
state-of-the-art CNNs: Alexnet, VGG19, GoogleNet,
and Resnet101. These network architectures were
chosen as they are known to perform well on
surgical endoscopy images (Petscharnig and
Schöffmann 2018). Transfer learning implies that
the CNNs were pretrained, in this case on the
Imagenet database which contains millions of
natural images distributed in 1000 classes. Although
surgical images are substantially different, given the
powerful architecture of the CNNs and the huge
volume of Imagenet, transfer learning has been
proved a simple, yet good-working approach for
content-based description of surgical images
(Petscharnig and Schöffmann 2017). Moreover, our
dataset is considerably small to train these CNNs
from scratch. However, as will be discussed later,
we perform training to model the temporal variation
of the extracted CNN features.
Alexnet consists of eight layers: 5 convolutional
layers followed by 3 fully-connected (FC) layers.
For each frame in a video shot, we extracted features
from layer fc7, which is the before-final-fc (BFFC)
layer with length n1=4096. VGG19 is much deeper,
consisting of 16 convolutional layers followed by 3
fully connected layers. We again extracted features
from the BFFC layer (fc7, n2=4096). GoogleNet is
different to Alexnet and VGG19, including various
Inception modules with dimensionality reduction
and only one fully connected layer combined with a
softmax layer (22 layers in total). For each frame we
used the features extracted from the BFFC layer:
pool5-7x7_s1 (n3=1024). Finally, the Resnet101
model is the deepest of the four (101 layers); it
stacks several residual blocks in-between the
convolutional blocks aiming to alleviate the
vanishing gradient problem, usually encountered
when stacking several convolutional layers together.
For the ResNet101 model we used the bottleneck
features extracted from the BFFC layer: pool5
(n4=2048).
Based on the aforementioned approach we
extracted feature descriptors from each video frame.
In order to achieve a compact feature representation
of the video shot, we concatenate the descriptors
along the temporal dimension and apply two
temporal pooling mechanisms: max-pooling and
average-pooling. The former extracts the maximum
value from each dimension of the BFFC layer,
whereas the second one outputs the average from
each dimension of the BFFC layer. For each CNN
architecture employed, both approaches result in a
single feature descriptor for each shot, equal to the
size of the corresponding BFFC layer.
2.3 CNN Input and Saliency Maps
The size of the input layer of the aforementioned
CNNs is: 227×227 (Alexnet) and 224×224 (VGG19,
GoogleNet, and ResNet101). In previous works, the
original image is resized either to match the CNN’s
input, or so that the smaller side matches one side of
the CNN input layer and then the center crop is used
as input to the CNN (Petscharnig and Schöffmann
2017),(Varytimidis et al. 2016). However, both
approaches have some limitations. Considering that
the original video resolution is 16/9, the former case
leads to a spatial degradation of the original image,
as the aspect ratio is forced to be 1 (see Figure 3). In
the latter case, image resizing does not affect the
aspect ratio, but extracting features from the center
crop may lead to an efficient representation of the
original frame since the structures of interest are not
always in the center (w.r.t. Figure 1, in P1 the trocar
is located towards the upper-right corner whereas in
P4 the clips/tool-tip are in the bottom).
BIOIMAGING 2019 - 6th International Conference on Bioimaging
24
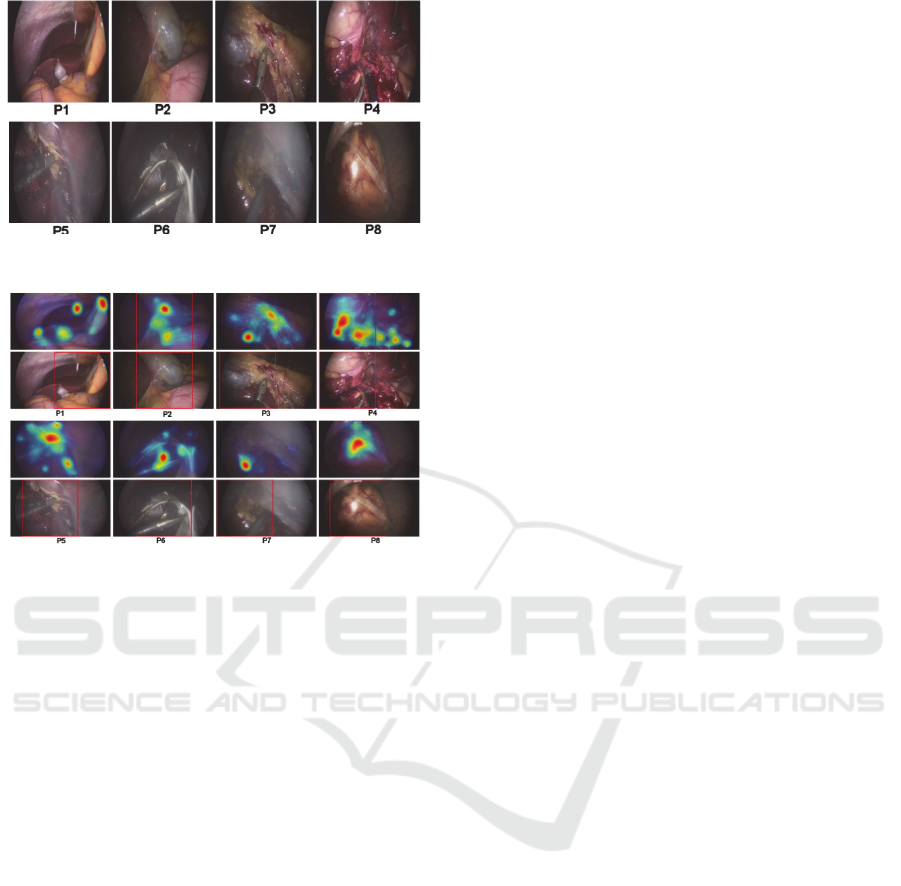
Figure 3: The images shown in Fig. 1, resized to 224×224.
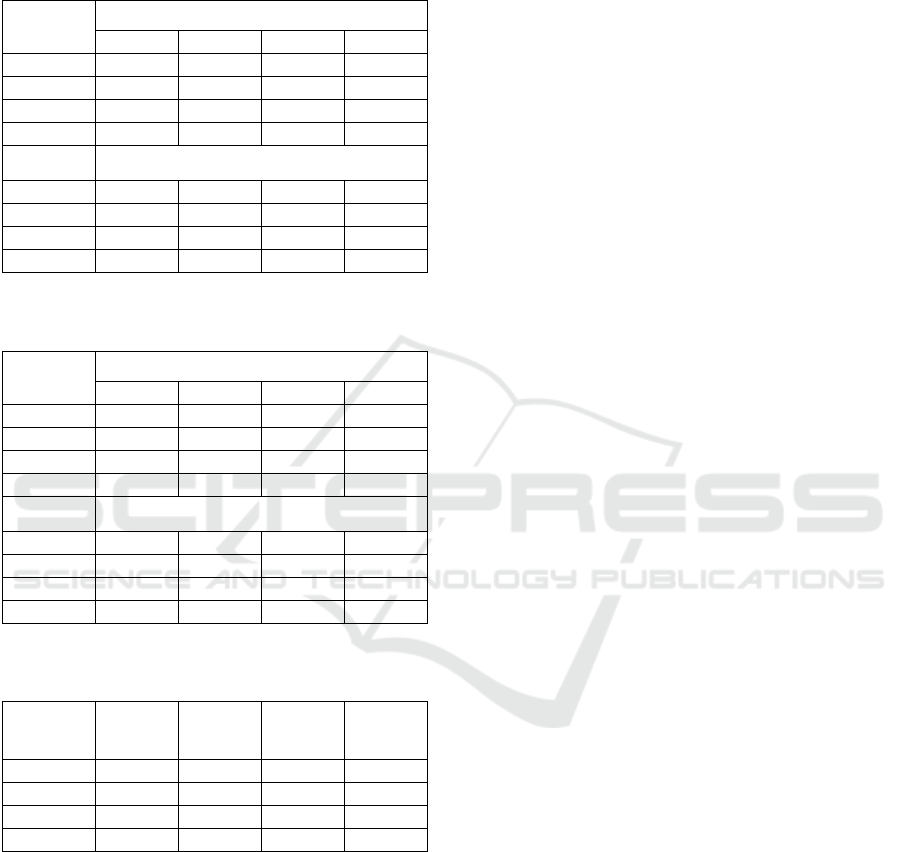
Figure 4: The saliency maps overlaid on the images shown
in Fig. 1 (top) and the rectangular patches which were
used as input to the CNN (bottom).
In this work, we propose an alternative
mechanism for region selection based on visual
saliency. Integration of visual saliency in CNN-
based content-based image representation is a major
trend nowadays. The main idea is to generate a
saliency map that represents the most salient regions
of the input image, without any prior assumption,
based on various criteria such as color- and texture-
contrast (Leboran et al. 2017),(Cheng et al. 2015).
Recent works have shown that using as input to the
CNN a salient, instead of a center/resized crop,
image provides better classification results (Obeso et
al. 2017). In this work we have employed the static
version of the adaptive whitening saliency (AWS)
methodology, which has shown superior
performance in predicting human attention (Leboran
et al. 2017). Recently, this method was applied for
keyframe extraction from video shots of LC
operations (Loukas et al. 2018). In brief, the model
employs a bank of 2D LogGabor filters, generating a
series of filter response maps, which are then
accumulated to generate the final saliency map of
the image.
For the purpose of this work, first we resized the
original full HD frame of the video shot so that the
smaller side (height) matched one side of the CNN
input layer (i.e. 224 or 227). Second, we computed
the saliency map of the resized frame based on the
AWS model. Third, we computed the 5 strongest
local maxima of the saliency map using a
neighborhood size 9×9. Fourth, the spatial
coordinates of these maxima were averaged
providing the center location of an image patch that
was used as input to the CNN. In case the center
location was so that the patch lied outside the resized
frame, the patch was shifted to lie within the frame
window. Finally, a feature descriptor was extracted
from the BFFC layer of the CNN, as described
previously.
Figure 4 provides the saliency maps overlaid on
the corresponding resized frames shown in Figure 1.
Below are the rectangular patches (in this case
224×224), which were used as input to the CNN. It
may be seen that most of the structures of interest lie
within the image patch, such as the trocar in P1, the
gallbladder in P2, the tools in P3-P7, and the
retrieval bag in P8.
2.4 Video Shot Classification based on
Temporal Pooling
Video shot classification was based on the 1st NN
using two different distance metrics: Euclidean and
cosine. For both metrics we used the compact
feature representation of each shot based on the
max- and average-pooling mechanisms, described
before. The Euclidean metric simply takes the L2
norm of the compact feature descriptors whereas the
cosine distance is defined as one minus the cosine of
the included angle between the descriptors. Each of
the 400 compact feature descriptors of the
corresponding video shots was treated as a candidate
descriptor, for which the class is predicted based on
its nearest distance among all other descriptors
(treated as training descriptors). The results were
obtained separately for each combination of pooling
mechanism and distance metric.
As described in Section 2.1, the time-stamp of
the video frames seem to play an important role in
the prediction of the surgical phase. Hence, we also
investigated the effect of adding the time-stamp of
the video shot as an additional dimension to the
CNN features (n+1). Consequently, each video shot
was represented by the pooled CNN descriptor
concatenated by the time stamp of the shot (taken as
the elapsed time, T
elapsed
, of the 1
st
frame of the shot
from the beginning of the operation).
Surgical Phase Recognition of Short Video Shots based on Temporal Modeling of Deep Features
25

2.5 Video Shot Classification based on
Temporal Modeling
A significant limitation of the aforementioned
pooling mechanisms for the video shot
representation, is that the resulting descriptor does
not take into account the temporal order of the
individual frames. In other words, if one shuffles the
frames of a video shot, then each of these
mechanisms will lead to the same feature descriptor.
However, the order of the frames (and so the
extracted CNN descriptors) is an important piece of
information that should be utilized in the
classification task. A recurrent neural network
(RNN) exhibits dynamic temporal behaviour for a
time sequence, as the connections between nodes
form a directed graph along the sequence. Moreover,
RNNs use their internal state to process input
sequences and they are able to connect previous
information to the present task, such as using
previous video frames for the understanding of the
present frame and eventually the class of the entire
video shot.
In this work, the CNN feature extraction process
was applied at each time point of the shot, leading to
a temporal order of feature descriptors. Then, we
employed the LSTM network, a special kind of
RNNs, composed of a series LSTM units (as many
as the number of shot’s descriptors), and a FC layer
with softmax at the end to perform classification into
the eight phases. To training parameters of the
LSTM network were similar to those proposed
recently in (Li et al. 2018): batch size=16, training
epochs=80, hidden units=200, learning rate=0.001,
the Adam method for optimization and cross-
entropy as loss function.
Similarly to the aforementioned idea of
concatenating the compact CNN shot descriptor with
the time-stamp of the video shot, here we employed
as input to the LSTM network the CNN features
(extracted from each frame of the shot),
concatenated with the time-stamp of the
corresponding video frame (dimensionality: n+1).
The model was run on every 25th frame (i.e. 1 fps)
to reduce the computational cost. During
training/testing the temporal order of the feature
descriptors was preserved. The LSTM network was
trained on 50% of the video shot dataset (i.e. 200
video shots) and the remaining 50% served as the
test set. We performed 5 random cycles of training,
making sure that a video shot was included at least
once in a training cycle, and then we averaged the
evaluation metrics (see next section).
3 EXPERIMENTAL RESULTS
The performance of the aforementioned approaches
was evaluated in terms of the following metrics:
Acc = (TP + TN)/(P + N) (1)
Pre = TP/(TP + FP) (2)
Rec = TP/(TP + FN) (3)
F1 = 2 × Pre × Rec/(Pre + Rec) (4)
where: Acc, Pre, Rec, F1 denote Accuracy,
Precision, Recall, and F1-score, respectively; TP,
TN, FP, FN, P, N denote: true positives, true
negatives, false positives, false negatives, positives
and negatives, respectively.
Table 2 shows average classification results
using CNN features extracted from the resized raw
images, for the two temporal pooling mechanisms
and the two distance metrics. It is worth noting that
for a particular CNN and pooling mechanism, the
distance metrics are similar, except for ResNet101
where Euclidean leads to worse results for average
pooling. With regard to the two pooling
mechanisms, max pooling seems to yield better
performance, especially when used with cosine, for
all CNNs. The best performance was achieved by
Table 2: Classification results based on resized raw images (Features: CNN).
CNN
type
Pooling: Max
Distance: Cosine
Pooling: Average
Distance: Cosine
Pooling: Max
Distance: Euclidean
Pooling: Average
Distance: Euclidean
Acc Pre Rec F1 Acc Pre Rec F1 Acc Pre Rec F1 Acc Pre Rec F1
alex
net
.60 .60 .61 .61 .59 .60 .59 .60 .59 .60 .60 .60 .56 .58 .57 .57
google
net
.60 .61 .62 .61 .55 .55 .56 .55 .60 .60 .61 .61 .53 .53 .54 .53
vgg19 .60 .61 .61 .61 .57 .56 .57 .57 .60 .61 .60 .60 .56 .57 .57 .57
resnet
101
.64 .65 .64 .64
.61 .64 .61 .62
.65 .66 .65 .65
.57 .59 .58 .58
BIOIMAGING 2019 - 6th International Conference on Bioimaging
26
ResNet101 (~65%) using max-pooling with either
distance metric.
Table 3: Classification results based on salient maps
(Features: CNN).
CNN
type
Pooling: Max, Distance: Cosine
Acc Pre Rec
F1
alexnet
0.62 0.61 0.62 0.61
googlenet
0.63 0.65 0.64 0.64
vgg19
0.61 0.61 0.62 0.62
resnet101
0.69 0.70 0.70 0.70
Pooling: Max, Distance: Euclidean
alexnet
0.57 0.57 0.57 0.57
googlenet
0.60 0.61 0.61 0.61
vgg19
0.60 0.60 0.61 0.60
resnet101
0.68 0.68 0.68 0.68
Table 4: Classification results based on salient maps
(Features: CNN and T
elapsed
).
CNN
type
Pooling: Max, Distance: Cosine
Acc Pre Rec
F1
alexnet
0.71 0.73 0.71 0.71
googlenet
0.70 0.72 0.70 0.70
vgg19
0.71 0.72 0.71 0.71
resnet101
0.75 0.76 0.75 0.75
Pooling: Max, Distance: Euclidean
alexnet
0.68 0.68 0.68 0.68
googlenet
0.61 0.61 0.61 0.61
vgg19
0.65 0.65 0.66 0.65
resnet101
0.68 0.68 0.68 0.68
Table 5: Classification results based on salient maps and
LSTM (Features: CNN and T
elapsed
).
CNN
type
Acc Pre Rec
F1
alexnet
0.73 0.74 0.73 0.72
googlenet
0.81 0.82 0.81 0.81
vgg19
0.78 0.77 0.78 0.77
resnet101
0.86 0.88 0.86 0.86
Table 3 summarizes the classification results
using features extracted from the most salient region
of the image, as described in Section 2.3. Average-
pooling is omitted as it was proved to yield worse
results. Compared to Table 2 it is clear that
extracting features from the most salient image patch
leads to 2-5% improvement for both distance metrics
and for all CNNs. The cosine distance produced
better results (by 3-5%), for all CNNs. The best
performance was achieved again by ResNet101
(~70%), whereas the other three CNNs had similar
performance (61-65%) although higher than that
shown in Table 2.
Table 4 presents the results using the CNN
features extracted from the salient patch,
concatenated with the ‘elapsed time’ feature.
Compared to Table 3, there is a notable
improvement by ~5-10% for all metrics, CNN
architectures, and distance metrics (except for
GoogleNet/ResNet101 with Euclidean, which is the
same). Note that the difference in this experiment
was that the feature vector was increased by 1, the
elapsed time of the 1st frame of the shot from the
operation start. Again, the cosine distance produces
better results than Euclidean, for all CNNs (~3-9%
improvement). The best performance was achieved
again by ResNet101, about 5% higher than that
using only the CNN features (75% vs. 70%).
Table 5 provides the results based on LSTM
model training. Similarly to Table 4, the input to the
network was the CNN feature vector extracted from
the most salient region of the video frame,
concatenated with its time-stamp (i.e. elapsed time
from operation start). Clearly the LSTM model
yields superior performance across all metrics,
compared to the naive NN cosine distance with max-
pooling (compare to Table 4). Specifically, the
improvement was about: 2%, 10%, 7% and 11% for
Alexnet, GoogleNet, VGG19, and ResNet101,
respectively. The best performance was achieved
again by ResNet101 (86-88%), whereas the second
best model was GoogleNet (~81%).
Table 6 illustrates the performance of the LSTM
model for the individual classes, using a confusion
matrix. Columns denote the predicted class while
rows indicate the true class. The numbers denote the
prediction percentage with respect to the samples
from a particular class (positives). For phases P1-P4,
the model yields almost perfect predictions, higher
than 94%, and with very low or no confusion among
the other classes. For P7 and P8 the results are also
remarkable: 79% and 87% respectively. The model
seems to slightly confuse P7 with P5 (9%), and
much less with P4 and P8 (~5%). Phase P8 is
slightly confused with P5 and P7 (5% and 8%
respectively). For P5 and P6 the performance is
similar (~72%). P5 is mostly confused with P7
(26%), whereas P6 with P7 (19%) and P4 (10%).
The lower results for P5, P6 may be due to the visual
similarity with P7 as a result of smoke, as depicted
in Figure 1.
Surgical Phase Recognition of Short Video Shots based on Temporal Modeling of Deep Features
27

Table 6: Confusion matrix based on salient maps and
LSTM (Features: CNN and T
elapsed
).
True/
Pred.
P1 P2 P3 P4 P5 P6 P7 P8
P1
1
P2
.94
.06
P3 .05
.94
.01
P4
.93
.01 .01 .01 .04
P5
.72
.26 .02
P6 .10
.71
.19
P7 .04 .09 .02
.79
.06
P8 .05 .08
.87
4 CONCLUSIONS
In this paper we propose a method for video shot
classification into surgical phases based on deep
features and temporal information modeling. Our
results lead to the following conclusions. First,
extracting CNN features from the most salient
regions of the image allows to achieve better results
(up to 5%). Second, when using a NN approach for
classification, the cosine distance provides better
results (up to 5%). Third, video shot representation
based on max-pooling of CNN image features is
better than average pooling (up to 6%). Fourth,
deeper CNNs provide more robust features for
classification (up to 10% improvement). Fifth,
‘elapsed time’ (a feature ignored so far), can
increase performance dramatically (up to 10% and
6% for shallower and deeper architectures,
respectively). Finally, employing an LSTM model
for temporal modeling of the CNN features fused
with ‘elapsed time’ provides significant performance
improvement: 86% accuracy and 88% precision
(compared to 75% and 76% when max-pooling is
employed, respectively). The investigation of a
visual saliency model specialized to surgical videos,
fine tuning of a ResNet model in which ‘elapsed
time’ is embedded, and other temporal information
modeling architectures, are major topics of interest
for future research work.
ACKNOWLEDGEMENTS
The author thanks Special Account for Research
Grants and National and Kapodistrian University of
Athens for funding to attend the meeting.
REFERENCES
Blum, T. et al., 2010. Modeling and segmentation of
surgical workflow from laparoscopic video. In
Medical Image Computing and Computer-Assisted
Intervention (MICCAI). Lecture Notes in Computer
Science. pp. 400–7.
Bouarfa, L. et al., 2011. Discovery of high-level tasks in
the operating room. Journal of Biomedical
Informatics, 44(3), pp.455–462.
Cheng, M.-M. et al., 2015. Global contrast based salient
region detection. IEEE Transactions on Pattern
Analysis and Machine Intelligence, 37(3), pp.569–582.
Dergachyova, O. et al., 2016. Automatic data-driven real-
time segmentation and recognition of surgical
workflow. International Journal of Computer Assisted
Radiology and Surgery, 11(6), pp.1081–9.
Jin, Y. et al., 2018. SV-RCNet: Workflow recognition
from surgical videos using recurrent convolutional
network. IEEE Transactions on Medical Imaging,
37(5), pp.1114–1126.
Lahanas, V. et al., 2011. Psychomotor skills assessment in
laparoscopic surgery using augmented reality
scenarios. In 17th International Conference on Digital
Signal Processing (DSP). Corfu, Greece: IEEE, pp. 1–
6.
Lalys, F. et al., 2012. A framework for the recognition of
high-level surgical tasks from video images for
cataract surgeries. IEEE Transactions on Biomedical
Engineering, 59(4), pp.966–976.
Leboran, V. et al., 2017. Dynamic whitening saliency.
IEEE Transactions on Pattern Analysis and Machine
Intelligence, 39(5), pp.893–907.
Li, Y. et al., 2018. Context aware decision support in
neurosurgical oncology based on an efficient
classification of endomicroscopic data. International
Journal of Computer Assisted Radiology and Surgery,
13(8), pp.1187–1199.
Loukas, C. et al., 2018. Keyframe extraction from
laparoscopic videos based on visual saliency detection.
Computer Methods and Programs in Biomedicine,
165, pp.13–23.
Loukas, C. et al., 2011. The contribution of simulation
training in enhancing key components of laparoscopic
competence. The American Surgeon, 77(6), pp.708–
715.
Loukas, C., 2018. Video content analysis of surgical
procedures. Surgical Endoscopy, 32(2), pp.553–568.
Loukas, C. and Georgiou, E., 2013. Surgical workflow
analysis with Gaussian mixture multivariate
autoregressive (GMMAR) models: a simulation study.
Computer Aided Surgery, 18(3–4), pp.47–62.
Obeso, A.M. et al., 2017. Connoisseur: classification of
styles of Mexican architectural heritage with deep
learning and visual attention prediction. In 15th
International Workshop on Content-Based Multimedia
Indexing (CBMI). Florence, Italy, pp. 1–7.
Padoy, N. et al., 2012. Statistical modeling and
recognition of surgical workflow. Medical Image
Analysis, 16(3), pp.632–41.
BIOIMAGING 2019 - 6th International Conference on Bioimaging
28

Petscharnig, S. and Schöffmann, K., 2018. Binary
convolutional neural network features off-the-shelf for
image to video linking in endoscopic multimedia
databases. Multimedia Tools and Applications, pp.1–
26.
Petscharnig, S. and Schöffmann, K., 2017. Learning
laparoscopic video shot classification for
gynecological surgery. Multimedia Tools and
Applications, 77(7), pp.8061–79.
Primus, M.J. et al., 2016. Temporal segmentation of
laparoscopic videos into surgical phases. In 14th
International Workshop on Content-Based Multimedia
Indexing (CBMI). Bucharest, Romania: IEEE, pp. 1–6.
Stauder, R. et al., 2016. The TUM LapChole dataset for
the M2CAI 2016 workflow challenge. ArXiv,
1610.09278.
Twinanda, A.P. et al., 2017. EndoNet: A deep architecture
for recognition tasks on laparoscopic videos. IEEE
Transactions on Medical Imaging, 36(1), pp.86–97.
Varytimidis, C. et al., 2016. Surgical video retrieval using
deep neural networks. In Medical Image Computing
and Computer-Assisted Intervention (MICCAI)-
M2CAI Workshop. Athens, Greece, pp. 4–14.
Surgical Phase Recognition of Short Video Shots based on Temporal Modeling of Deep Features
29
