
Anthropomorphic Virtual Assistant to Support Self-care of Type 2
Diabetes in Older People: A Perspective on the Role of Artificial
Intelligence
Gergely Magyar
1
, João Balsa
2
, Ana Paula Cláudio
2
, Maria Beatriz Carmo
2
, Pedro Neves
2
,
Pedro Alves
2
, Isa Brito Félix
3
, Nuno Pimenta
4,5
and Mara Pereira Guerreiro
3,6
1
Department of Cybernetics and Artificial Intelligence, Technical University of Kosice, Letna 9, Kosice, Slovakia
2
Biosystems & Integrative Sciences Institute (BioISI), Faculdade de Ciências da Universidade de Lisboa, Lisboa, Portugal
3
Unidade de Investigação e Desenvolvimento em Enfermagem (ui&de),
Escola Superior de Enfermagem de Lisboa, Lisboa, Portugal
4
Sport Sciences School of Rio Maior – Polytechnic Institute of Santarém, Rio Maior, Portugal
5
Exercise and Health Laboratory, Interdisciplinary Centre for the Study of Human Performance, ULisboa,
Cruz-Quebrada, Portugal
6
Centro de Investigação Interdisciplinar Egas Moniz (CiiEM), Instituto Universitário Egas Moniz,
Monte de Caparica, Portugal
{fc51688, fc51686}@alunos.fc.ul.pt, npimenta@esdrm.ipsantarem.pt
Keywords: Virtual Humans, Relational Agents, Artificial Intelligence, Health Care, Behaviour Change, Type 2 Diabetes,
Older People.
Abstract: The global prevalence of diabetes is escalating. Attributable deaths and avoidable health costs related to dia-
betes represent a substantial burden and threaten the sustainability of contemporary healthcare systems. In-
formation technologies are an encouraging avenue to tackle the challenge of diabetes management. Anthro-
pomorphic virtual assistants designed as relational agents have demonstrated acceptability to older people and
may promote long-term engagement. The VASelfCare project aims to develop and test a virtual assistant
software prototype to facilitate the self-care of older adults with type 2 diabetes mellitus. The present position
paper describes key aspects of the VASelfCare prototype and discusses the potential use of artificial intelli-
gence. Machine learning techniques represent promising approaches to provide a more personalised user ex-
perience with the prototype, by means of behaviour adaptation of the virtual assistant to users’ preferences or
emotions or to develop chatbots. The effect of these sophisticated approaches on relevant endpoints, such as
users’ engagement and motivation, needs to be established in comparison to less responsive options.
1 INTRODUCTION
The global prevalence of diabetes is escalating
(Karuranga et al., 2017). Across the globe 90% of di-
abetic adults suffer from type 2 diabetes (T2D); the
disease or its complications are the 9
th
major cause of
death (Zheng, Ley and Hu, 2018). Recent Portuguese
data estimated a total diabetes prevalence of about
13%. In Portugal more than one out of four persons
aged between 60 and 79 years old have diabetes
(Sociedade Portuguesa de Diabetologia, 2016).
Hyperglycaemia control in T2D involves lifestyle
changes, including an adequate diet and physical ac-
tivity and, where needed, regular medication. Diffi-
culties in adhering to diabetes management, which re-
quires sustained behavioural change, is associated
with poor glycaemic control in more than half of the
patients (García-Pérez et al., 2013). Long term hyper-
glycaemia results in life-threatening complications,
including cardiovascular disease, neuropathy,
nephropathy and retinopathy. These complications
represent an economic burden to health care systems,
in addition to the clinical and humanistic burden
posed to diabetes sufferers and their families
(Karuranga et al., 2017). Improving adherence to
T2D management is therefore critical, as it will delay
or avoid diabetes complications whilst relieving the
Magyar, G., Balsa, J., Cláudio, A., Carmo, M., Neves, P., Alves, P., Félix, I., Pimenta, N. and Guerreiro, M.
Anthropomorphic Virtual Assistant to Support Self-care of Type 2 Diabetes in Older People: A Perspective on the Role of Artificial Intelligence.
DOI: 10.5220/0007572403230331
In Proceedings of the 14th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2019) - Volume 1: GRAPP, pages
323-331
ISBN: 978-989-758-354-4; ISSN: 2184-4321
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
323

financial pressure on healthcare systems over-
whelmed by the demands of an ageing population.
Information Technologies (IT) are a promising
avenue to help T2D patients self-managing their con-
dition sustainably and without time or place re-
strictions. Mobile applications are regarded as
cheaper, more convenient and more interactive than
other IT-based interventions, such as short message
services and computer-based interventions (Hou et
al., 2016). They have demonstrated a positive effect
in improving glycaemic control in T2D patients. For
example, Cui and co-workers (2016) conducted a sys-
tematic review of 13 randomised controlled trials on
the effect of mobile applications on the management
of T2D. Six studies provided data for meta-analysis,
with a total of 1022 patients (average age from 45.2
to 66.6 years). They found that mobile applications
were associated with a significant reduction in HbA1c
by -0.40% (Cui et al., 2016). One issue meriting de-
bate is whether older people with T2D will have a
benefit comparable to their younger counterparts, as
trials included mostly younger samples (Cui et al.,
2016; Hou et al., 2016). Mobile applications for older
adults should be designed considering the needs of
this population group.
Relational agents, which are virtual characters ca-
pable of establishing long-term relationships with us-
ers, emerge as an encouraging approach to engage
older people.
The VASelfCare project aims to develop and test
a prototype of a relational agent application to facili-
tate self-care of older people with T2D. In this paper
we discuss ideas on the role of artificial intelligence
to enhance functionalities of the VASelfCare proto-
type; this falls under one of the conference topic areas
(interactive environments). Our position paper builds
on an international collaboration between the
VASelfCare team and a researcher experienced in be-
haviour adaptation of social robots in cognitive stim-
ulation therapy for older people. The ideas put for-
ward are discussed in light of experimental and bibli-
ographic evidence.
The core of this paper is comprised by three key
sections. Firstly, section 2 provides a broad over-
view of published work on relational agents, includ-
ing a brief description on the use of artificial intelli-
gence. Section 3 describes our relational agent pro-
totype (VASelfCare). Together, these sections set
the scene for the proposed ideas about the role of
artificial intelligence to enhance functionalities of
our prototype.
2 RELATED WORK
Studies resorting to relational agents have been con-
ducted in several areas. The importance of incorpo-
rating an artificial intelligence component in these
agents has been recognized for some years now
(Cassell, 2001).
In the area related to our work, healthcare, sub-
stantial research has been conducted by Bickmore et
al., namely in approaches tackling mental condi-
tions. For instance, Bickmore et al. (2010) evaluated
how patients with a high-level of depressive symp-
toms responded to a computer animated conversa-
tional agent in a hospital environment. Another pub-
lication describes the use of relational agents in
health counselling and behaviour change interven-
tions in clinical psychiatry (Bickmore and Gruber,
no date). Ring et al. reported a pilot study based on
an affectively-aware virtual therapist for depression
counselling (Ring, Bickmore and Pedrelli, 2016).
Still in mental health, Provoost et al. (2017) re-
viewed the use of embodied conversational agents in
clinical psychology, mostly focusing on autism and
on social skills training. The benefit of relational
agents in patients with lower health literacy was
demonstrated (Bickmore et al., 2010). It has also
been showed that interventions based on relational
agents are well accepted by older people (Bickmore
et al. 2005; Bickmore et al. 2013).
Devault and co-workers developed a conversa-
tional agent deploying artificial intelligence tech-
niques for natural language understanding and dia-
logue management to establish an engaging face-to-
face interaction. The goal was creating interactional
situations favourable to the automatic assessment of
distress indicators (Devault et al., 2014).
The role of emotions and the importance of estab-
lishing rapport between a virtual agent and the human
user, coupled to the relevance of nonverbal behaviour
in affective interaction, have been studied, for in-
stance, by Gratch et al. (2007), Bickmore et al. (2005)
Bickmore, Gruber and Picard (2005), and Paiva et al.
(2017).
One of the more explored subareas of artificial in-
telligence in other fields of research on virtual assis-
tants is natural language processing, which intends to
achieve a more believable interaction. For example,
(Hoque et al., 2013) developed a virtual agent for so-
cial skills training that reads facial expressions and
uses natural language processing techniques to under-
stand speech and prosody, responding with verbal and
nonverbal behaviours in real time. Also, Rubin, Chen
and Thorimbert (2010), surveyed the use of language
GRAPP 2019 - 14th International Conference on Computer Graphics Theory and Applications
324

technologies in the development of intelligent assis-
tants in libraries.
The importance of virtual assistants in healthcare
as well as the relevance of incorporating machine
learning techniques is also reported in a work by
(Shaked, 2017), where the authors identify a set of
key features for the design of this kind of applications
when interacting with older people.
The use of relational agents in people with T2D
has been little explored. One exception is an Austral-
ian study, which described the development of an in-
telligent diabetes lifestyle coach for self-management
of diabetes patients (Monkaresi et al., 2013). How-
ever, this study lacks data on usability or the effect on
endpoints of interest. More recently, an on-going
study in the USA has used a relational agent as a
health coach for adolescents with type 1 diabetes and
their parents (Thompson et al., 2016).
3 VASELFCARE PROTOTYPE
Our application targets medication adherence and
lifestyle changes (physical activity and diet) in a step-
wise fashion by means of an anthropomorphic virtual
assistant, named Vitória. As previously mentioned,
the virtual assistant was designed as relational agent.
This is expected to increase engagement and long-
term use (Bickmore, 2010), and to facilitate the inter-
action with people with lower literacy. Development
of the application was guided by usability principles
for older people (Arnhold, Quade and Kirch, 2014).
3.1 Interaction with the Application
When opening the application Vitória is depicted in a
3D living room scenario. When clicking on the button
“Enter”, users with T2D are directed to a menu where
several choices are available, including talking to Vi-
tória (Dialogue view – Figure 1).
3.1.1 The Dialogue View
Vitória communicates with users both verbally, by
means of a synthetic voice, and non-verbally
through facial and body animations. The latter de-
pend on users’ responses. The 3D scenario in which
this virtual assistant is depicted changes according
to the dialogue context (e.g. the kitchen scenario is
presented when talking about the diet), the time of
day (i.e. the view from the window in the back-
ground) and the season (e.g. the window view with
sunshine or rain).
Figure 1: Dialogue view in the evaluation phase (version
1.00).
Another design option tailored for older people in-
cludes subtitles in Vitória’s speech, which may over-
come hearing difficulties.
Users communicate with Vitória using buttons or
recording values, such as the daily number of steps,
and medication taken. The latter data are plotted into
graphs or other visual representations (Figure 2), used
by Vitória to give feedback during the interaction.
Figure 2: Medication-taking feedback (scenario: one oral
antidiabetic, two daily doses; question mark means no self-
reported data) (version 1.0.5).
The first daily interactions for medication adher-
ence and lifestyle changes collect data on pertinent
variables, with the purpose of tailoring the interven-
tion to users’ characteristics. For example, behaviour
change on medication adherence considers users’
knowledge about antidiabetic agents, their usual be-
haviour and the perceived self-efficacy in managing
their medication. This phase is designated “evaluation
phase”. In the subsequent “follow-up phase”, the be-
haviour change intervention is informed by theory
and users’ characteristics.
Based on the literature (Bickmore, Schulman and
Sidner, 2011), each daily interaction is structured in
sequential steps. Interactions in the evaluation phase
have six steps: opening, social talk, assess, feedback,
Anthropomorphic Virtual Assistant to Support Self-care of Type 2 Diabetes in Older People: A Perspective on the Role of Artificial
Intelligence
325

pre-closing and closing. The “opening” step, which
consist in greeting the user, is followed by a social
dialogue, including inquiries about users’ general
emotional and physical state (“social talk”). Ques-
tions on a variable of interest, such as knowledge
about antidiabetic medication, are then posed (“as-
sess”), followed by feedback on the answers collected
previously. Finally, contents of the next interaction
are described (“pre-closing”) and a farewell is deliv-
ered (“closing”).
Daily interactions in the follow-up phase are also
structured in repeated sequential steps: opening, so-
cial talk, review tasks, assess, counselling, assign
tasks, pre-closing and closing. The first and last two
steps are similar to those described above. In the “re-
view tasks” step, information is collected about pre-
viously agreed tasks or behaviours. Then, information
is provided about the reported task or behaviour, in-
cluding reward talk or a discussion of behaviour(s)
determinants (“assess”). In the counselling step, users
receive information on strategies to achieve the desir-
able behaviour (if applicable) and on specific educa-
tional topics. After, users negotiate new behavioural
goals and tasks with Vitória (“assign tasks”).
A rule-based component has been implemented in
the application, to convey a more flexible dialogue
flow in the follow-up phase.
The Behaviour Change Wheel (BCW), a compre-
hensive and evidence-based theoretical framework of
behaviour change, was chosen to inform the interven-
tion design (Michie, Atkins and West, 2014). The
BWC is underpinned by the COM-B model. This
model posits that engagement in a behaviour (B) at a
given moment depends on capability (C) plus oppor-
tunity (O) and motivation (M). Analysis of a given
behaviour in relation to COM-B allows the identifi-
cation of determinants, which must be addressed to
achieve change. The BCW entails also the selection
of interventions functions (broad strategies for induc-
ing the target behaviour) and behaviour change tech-
niques (active replicable elements that promote
change).
Suitable and effective behaviour change tech-
niques (BCT) were incorporated in different steps of
the interactions, guiding the dialogue creation
(Michie et al., 2013). For example, “Self-monitoring
of behaviour” was applied in the “review tasks”; it
consists of recording medication taken or steps count.
In the “Assess” step, information on medication-tak-
ing is provided by means of a calendar, a technique
entitled “Feedback on behaviour”. In this step users
also identify potential determinants of non-adher-
ence, which allows the selection of ameliorating strat-
egies in the “counselling” step. This BCT is desig-
nated “problem solving”. Educational topics ad-
dressed during “counselling” encompass the “infor-
mation about health consequences” BCT.
Dialogue creation in the assessment and follow-
up phases employs a helpful-cooperative communi-
cation style (Niess and Diefenbach, 2016).
3.1.2 The Other Views
In its current version, the application has six views in
addition to the dialogue view (“Main menu”, “Re-
cording”, “My diary”, “My data”, “Information” and
“About the application”). The main menu offers sev-
eral sub-menus; each sub-menu, in turn, corresponds
to a view of the application.
In the “My diary” view, users can create a weekly
plan. The diary automatically proposes meal times
with recipe suggestions. Users can also add, remove
and edit activities.
“My Data” allows users to review information on
topics, such as their prescribed antidiabetic medica-
tion, anthropometric measurements (e.g. a visual rep-
resentation of body mass index) and their reported be-
haviour, by means of the same charts used by Vitória
in daily interactions.
The “Information” view consists of a glossary
plus educational content about diabetes, diet, physical
activity, antidiabetic medication.
“Recording” allows users to input data such as the
number of steps walked per day or blood glucose lev-
els. The application gives automatic feedback to en-
tered data, including messages in case of potentially
erroneous values. Another example of automatic
feedback is depicted in Figure 3; this feedback guides
the user on the treatment of a hypoglycaemic episode,
when the inputted blood glucose level is below 70
mg/dl.
Figure 3: Example of an instant response to the recording
of a low blood sugar level (version 1.0.5).
Finally, the “About the Application” view in-
cludes information about the application develop-
ment, security and privacy policy.
GRAPP 2019 - 14th International Conference on Computer Graphics Theory and Applications
326
While the dialogue view is restricted to one inter-
action per day, the aforementioned views can be
freely accessed.
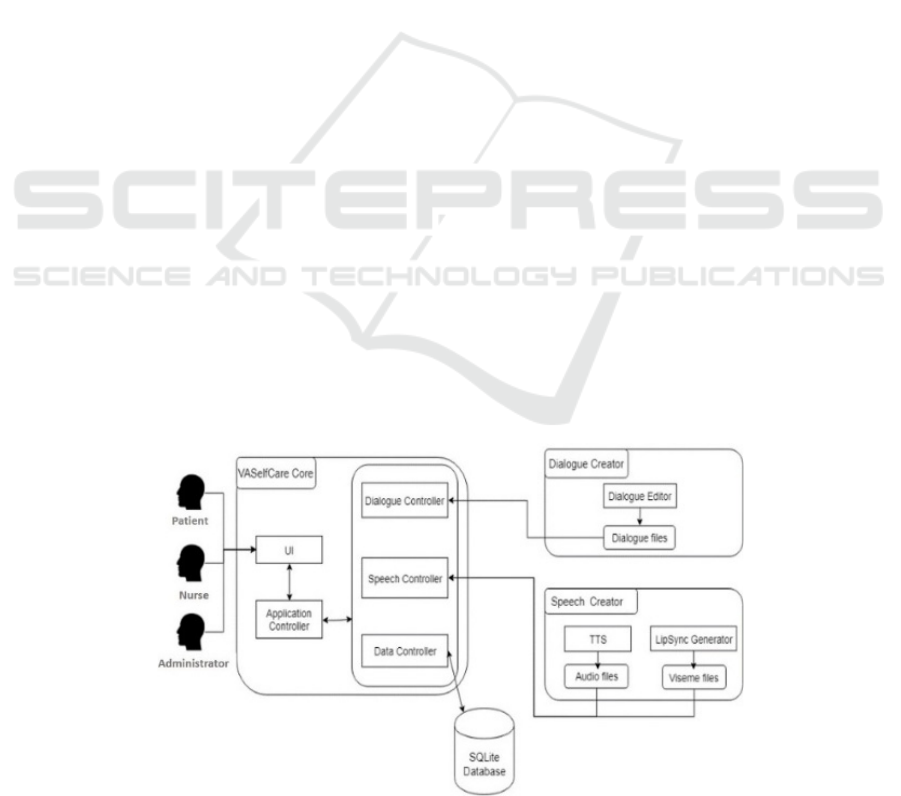
3.2 The Application Architecture
The components of our prototype are depicted in Fig-
ure 4. The VASelfCare Core comprises the scripts re-
sponsible for the user interface and the logic of the
application; it is implemented inUnity3D with C#
scripts. This core component resorts to services pro-
vided by two external elements: the Dialogue Crea-
tor and the Speech Generator.
VASelfCare Core comprises several modules with
distinct responsibilities: the Application Controller,
the Dialogue Controller, the Speech Controller,
and the Data Controller.
The Application Controller is responsible for the
logical sequence of the application and communicates
with the other modules of the VASelfCare Core.
The Dialogue Controller decides the correct order of
the dialogues, choosing the dialogue files that are
used in a specific moment of the interaction.
The Speech Controller is the module that allows Vi-
tória to speak, searching and activating the audio and
viseme files that correspond to the on-going dialogue.
Finally, the Data Controller module has the respon-
sibility of exchanging data with the embedded local
database. In this database the application stores clini-
cal information entered at the time of registration and
all the relevant data concerning the flow of interaction
with older patients.
The application runs in tablets with Android sys-
tem without Internet connection, which is intended to
facilitate access at users’ homes, where Internet is not
always available. When an Internet connection is de-
tected the application backs-up the database up onto
the project server.
4 THE ROLE OF ARTIFICIAL
INTELLIGENCE IN THE
VASELFCARE APPLICATION
The architecture of the VASelfCare prototype pre-
sented in section 3 offers multiple opportunities for
machine learning to further enhance the capabilities
of the virtual assistant. This section provides a brief
background on reinforcement learning and discusses
the potential use of artificial intelligence methods in
the VASelfCare application.
4.1 Reinforcement Learning
Generally, reinforcement learning is a learning
method which determines how to map situations to
actions and also tries to maximize a numerical reward
signal. The actions performed by the agent are not
identified explicitly, they have to be discovered
through exploration in order to get the most reward
(Sutton and Barto, 2018).
The agent can sense its environment and take ac-
tions which can change the state of the environment
to reach a given goal. The formulation of the task in-
cludes the following three aspects: sensation, action
and goal.
Figure 4: VASelfCare architecture.
Anthropomorphic Virtual Assistant to Support Self-care of Type 2 Diabetes in Older People: A Perspective on the Role of Artificial
Intelligence
327

In addition to the aforementioned concepts of re-
inforcement learning, there are three other key ele-
ments to correctly define a reinforcement learning
problem: policy, reward function and value function
and (Sutton and Barto, 2018).
Policy in general defines the agent’s way of be-
having in a given situation. More precisely it serves
for mapping from perceived states of the environment
to actions which must be executed when in those
states.
The reward function defines the goal of the rein-
forcement learning problem. It is responsible for
mapping the perceived state of the environment or
state-action pair to a number (reward) which defines
the desirability of the given state. The agent’s goal is
to maximize this reward during the learning process.
Contrarily to the reward function, which indicates
what is good or bad for the agent in the immediate
sense, the value function defines what is good for the
agent in the long run. In general, the value function is
the maximal value of reward which can be expected
by the agent during the learning process.
Traditional methods of machine learning, such as
reinforcement learning, were used successfully in
many areas. However, they were not primarily de-
signed for learning from real-time social interaction
with humans. This encompasses challenges, such as
dealing with limited human patience or ambiguous
human input. To address these challenges socially
guided machine learning was designed (Thomaz and
Breazeal, 2006).
In reinforcement learning the reward signal is rep-
resented by human feedback (e.g. facial emotion, ges-
ture, verbal expression). Such a system is designed to
efficiently learn from people with no experience in
reinforcement learning. This learning method can be
used to further enhance the cognitive capabilities of
Vitória, the VASelfCare virtual assistant.
4.2 Applying Reinforcement Learning
to the Prototype
4.2.1 Behaviour Adaptation based on Users’
Evaluation
One of the possibilities is changing Vitória’s facial
and body animations based on users’ preferences. The
task of the learning agent in this case is to find what
kind of pre-defined animations are desired by users
(e.g. fast or slower movements, more expressive ver-
sus more neutral facial animations). To increase the
learning speed animations can be labelled; the ones
which have the same label and are not accepted by the
user can be excluded from the learning right away.
Nonetheless, to ensure variability of the virtual assis-
tant behaviour these can show up with low probability
in future interactions. The reward for the agent could
be provided by users’ ratings of Vitória’s animations.
An additional possibility pertains to the fifth step
of the evaluation stage: counselling. As mentioned in
section 3.1, one of the goals of this step is to educate
users on different topics. Reinforcement learning can
help to create a personalised counselling step, which
builds on existing knowledge and provides new infor-
mation. The actions of the learning agent can be the
descriptions of the new concepts and the reward can
be provided by testing the newly acquired knowledge
of the user; this step is already included in the evalu-
ation stage.
For the sake of discussion, we can consider a sce-
nario in which Vitória does not have information
about the existing level of knowledge of a new user.
Firstly, this construct must be evaluated, to determine
what is already known about a topic (e.g. diabetes or
the prescribed medication). In the follow-up interac-
tions the virtual assistant can then address more often
topics where knowledge is absent or limited. Employ-
ing this mechanism provides a tailored approach
whilst ensuring that users will have comprehensive
knowledge about diabetes management.
4.2.2 Behaviour Adaptation based on the
Assessment of Users’ Facial Emotions
In recent years many emotion recognition services
were made publicly available. Due to the complexity
of facial emotion assessment, these cloud services fa-
cilitate the development of emotion recognition sys-
tems. In practice, users upload an image or provide an
URL address to the service, which returns infor-
mation about emotion assessment, usually in the form
of numerical data, representing the probability of the
presence of a given emotion in the image.
Selected examples of emotion recognition ser-
vices are Face++ Cognitive Services’ Emotion
Recognition which can detect anger, disgust, fear,
happiness, neutral, sadness, and surprise. Google Vi-
sion detects four emotional states on the face: anger,
joy, sorrow, and surprise. The Microsoft Face API an
detect eight emotions: anger, contempt, disgust, fear,
happiness, neutral, sadness, and surprise. The
Sighthound Cloud API can recognize anger, disgust,
fear, happiness, neutral, sadness, and surprise.
In a recent work we combined the above-men-
tioned services and trained a machine learning model
to increase the overall accuracy of face emotion as-
sessment (Magyar et al., 2018). The resulting system
was tested on different face emotion datasets and was
GRAPP 2019 - 14th International Conference on Computer Graphics Theory and Applications
328

able to increase accuracy from an average of 70 –
75% to approximately 95%. In the VASelfCare pro-
totype such an emotion recognition system can be
used to gather data about the overall emotional state
of users, therefore detecting and preventing unwanted
states (e.g. distress, pain). A pilot study for assessing
elderly patients’ emotions in a cognitive stimulation
therapy session with a robot already showed that such
information can be valuable when adapting the
agent’s behaviour (Takac et al., 2018).
As an example, we can consider the second step
of the daily interaction: social talk. In this step Vitória
initiates small talk with a user on various topics (e.g.
family, music, daily news, etc.). By combining rein-
forcement learning and emotion recognition, the vir-
tual assistant can explore topics associated with posi-
tive feelings (e.g. expressing happiness when talking
about grandchildren) and with negative feelings (e.g.
expressing sadness when talking about a late spouse).
Using this information and a history of previous con-
versations, the social interaction can be personalised,
to ensure a positive mood during the interaction.
Facial emotion recognition can also be used in re-
inforcement learning as a reward for the learning
agent. In this approach the behaviour of the virtual as-
sistant will be adapted based on the emotional re-
sponse of the user. This means that Vitória will likely
to prefer those actions which result in boosting the us-
ers’ mood and avoid those provoking sadness.
4.2.3 Chatbots
Another interesting possibility is applying artificial
intelligence to the VASelfCare prototype by means of
chatbots, which are increasingly getting more atten-
tion. As for facial emotion assessment, there are many
publicly available cloud services for building chat-
bots. Although these are mainly used for customer
support applications, they can be easily integrated in
the VASelfCare prototype.
For the sake of simplicity, we provide the descrip-
tion of Microsoft’s Q & A maker and how it can be
used in interactions with older people with T2D.
Nearly all cloud-based bot frameworks work on a
similar principle.
To create a chatbot from scratch it is firstly neces-
sary to gather data on relevant topics, such as medi-
cation, activities in the form of previous conversa-
tions, user manuals and product materials. Secondly
these documents are processed and used to train a ma-
chine learning model, which extracts information
from the documents and uses it to form answers to
questions on a given topic. The model trained initially
can be tested by experts to refine the system answers.
The model is then ready for use and can serve the var-
ious needs of the users.
In case of updates (e.g. a new marketed drug), the
model can be easily re-trained by feeding data about
the product to the system.
This feature holds great potential, since questions
about diabetes management can come up daily in the
interactions with Vitória. By constantly updating the
model with the newest information it is ensured that
the virtual assistant is providing accurate information,
previously checked by experts, to multiple users. This
system can also work with available text-to-speech
technologies, so users will not have to read the mes-
sages.
5 CONCLUSIONS
Artificial intelligence, and particularly machine
learning techniques, represent promising approaches
to provide a more personalised user experience with
the VASelfCare prototype. These approaches include
tailoring the virtual assistant behaviour based on us-
ers’ preferences or facial emotion assessment and the
use of chatbots.
Scholten et al. (2017) reviewed the capabilities of
relational agents to fulfil users’ needs in eHealth in-
terventions. They made a distinction between non-
responsive and responsive relational agents. The for-
mer are not designed to respond to emotionally ex-
pressed users’ needs in real time. Research shows that
non-responsive relational agents can engage users.
Although their development is simpler, there is a
higher risk of a worse user experience (Scholten,
Kelders and Van Gemert-Pijnen, 2017).
Responsive relational agents, designed to detect
frustration and to empathically respond to it, have
shown a positive effect on users’ attitudes. However,
this effect has not been demonstrated in clinical pop-
ulations (Scholten, Kelders and Van Gemert-Pijnen,
2017). Therefore, the benefits of facial emotion as-
sessment merit further research, particularly consid-
ering that both nonresponsive and responsive agents
can provide a positive experience.
Tailoring of health information has been defined
as “any combination of information and behaviour
change strategies intended to reach one specific per-
son based on characteristics that are unique to that
person related to the outcome of interest and derived
from an individual assessment” (Kreuter, M., Farrell,
D., Olevitch, L., & Brennan, 2000). This approach
demonstrated a positive effect in health behaviour
outcomes in web-delivered interventions (versus non-
Anthropomorphic Virtual Assistant to Support Self-care of Type 2 Diabetes in Older People: A Perspective on the Role of Artificial
Intelligence
329

tailored approaches) (Lustria et al., 2013). Our cur-
rent prototype tailors the counselling step, dealing
with diverse pre-existing levels of knowledge, by
means of an decision system. Nonetheless, due to the
nature of human-computer interaction it is nearly im-
possible to prepare the system for every situation us-
ing an explicit rule-based system. Reinforcement
learning enables a more flexible platform for the
agent to learn an appropriate behaviour based on us-
ers’ preferences. It can also be used as a complemen-
tary method to the existing decision system. In this
scenario the system would firstly determine what kind
of action should be executed by the agent. Then rein-
forcement learning would be applied to determine
how the action should be executed when dealing with
a concrete user. By applying such a combination of
machine learning methods, the application will offer
a more flexible and tailored behaviour of the agent.
An open dialogue (textual or verbal) between us-
ers and the relational agent, such as the one provided
by a chatbot, may support users’ needs, providing a
better experience and consequently improving adher-
ence to the intervention. Ultimately, this assumption
will have to be subjected to empirical trial.
We have pointed out several opportunities for re-
search. Such research will contribute to answer a crit-
ical question posed by Dehn & Mulken (2000) about
two decades ago.: “what kind of animated agent used
in what kind of domain influence what aspects of the
user’s attitudes or performance?.”
ACKNOWLEDGEMENTS
This project was supported by FCT, Compete 2020
(grant number LISBOA-01-0145-FEDER-024250,
02/SAICT/2016) and by FEDER Programa Opera-
cional do Alentejo 2020 (Grant number ALT20-03-
0145-FEDER-024250).
REFERENCES
Arnhold, M., Quade, M. and Kirch, W. (2014) ‘Mobile
Applications for Diabetics : A Systematic Review and
Expert-Based Usability Evaluation Considering the
Special Requirements of Diabetes Patients Age 50
Years or Older Corresponding Author ’:, Journal of
Medical Internet Research, 16(4), pp. 1–18. doi:
10.2196/jmir.2968.
Bickmore, T. (2010) ‘Relational Agents for Chronic
Disease Self-Management’, in Hayes, B. and Aspray,
W. (eds) Health Informatics: A Patient-Centered
Approach to Diabetes. Cambridge, MA: MIT Press, pp.
181–204.
Bickmore, T. and Gruber, A. (no date) ‘Relational agents in
clinical psychiatry.’, Harvard review of psychiatry,
18(2), pp. 119–30. doi: 10.3109/10673221003707538.
Bickmore, T., Gruber, A. and Picard, R. (2005)
‘Establishing the computer-patient working alliance in
automated health behavior change interventions’,
Patient Education and Counseling, 59(1), pp. 21–30.
doi: 10.1016/j.pec.2004.09.008.
Bickmore, T. W. et al. (2005) ‘“It’s just like you talk to a
friend” relational agents for older adults’, Interacting
with Computers, 17(6), pp. 711–735. doi: 10.1016/j.int
com.2005.09.002.
Bickmore, T. W. et al. (2010) ‘Response to a relational
agent by hospital patients with depressive symptoms’,
Interacting with Computers. Elsevier B.V., 22(4), pp.
289–298. doi: 10.1016/j.intcom.2009.12.001.
Bickmore, T. W. et al. (2013) ‘A randomized controlled
trial of an automated exercise coach for older adults’,
Journal of the American Geriatrics Society, 61(10), pp.
1676–1683. doi: 10.1111/jgs.12449.
Bickmore, T. W., Schulman, D. and Sidner, C. L. (2011) ‘A
reusable framework for health counseling dialogue
systems based on a behavioral medicine ontology’,
Journal of Biomedical Informatics. Elsevier Inc., 44(2),
pp. 183–197. doi: 10.1016/j.jbi.2010.12.006.
Cassell, J. (2001) ‘Conversational Agents Representation
and Intelligence in User Interfaces’, AI Magazine,
22(4), pp. 67–84. doi: 10.1609/aimag.v22i4.1593.
Cui, M. et al. (2016) ‘T2DM self-management via
smartphone applications: A systematic review and
meta-analysis’, PLoS ONE, 11(11), pp. 1–15. doi:
10.1371/journal.pone.0166718.
Dehn, D. M. and Mulken, S. van (2000) ‘The impact of
animated interface agents : a review of empirical
research’, International Journal of Human-Computer
Studies, 52, pp. 1–22.
Devault, D. et al. (2014) ‘SimSensei Kiosk: A Virtual
Human Interviewer for Healthcare Decision Support’,
in International conference on Autonomous Agents and
Multi-Agent Systems, AAMAS ’14, Paris, France, May
5-9, 2014. IFAAMAS/ACM, pp. 1061–1068.
García-Pérez, L.-E. et al. (2013) ‘Adherence to therapies in
patients with type 2 diabetes.’, Diabetes therapy, 4(2),
pp. 175–94. doi: 10.1007/s13300-013-0034-y.
Gratch, J. et al. (2007) ‘Creating Rapport with Virtual
Agents’, Intelligent Virtual Agents, pp. 125–138. doi:
10.1007/978-3-540-74997-4_12.
Hoque, M. (Ehsan) et al. (2013) ‘MACH: my automated
conversation coach’, in Proceedings of the 2013 {ACM}
international joint conference on {Pervasive} and
ubiquitous computing - {UbiComp} ’13. Zurich,
Switzerland: ACM Press, p. 697. doi: 10.1145/24934
32.2493502.
Hou, C. et al. (2016) ‘Do Mobile Phone Applications
Improve Glycemic Control (HbA1c) in the Self-
management of Diabetes? A Systematic Review, Meta-
analysis, and GRADE of 14 Randomized Trials’,
Diabetes Care, 39(11), pp. 2089–2095. doi: 10.2337/dc
16-0346.
GRAPP 2019 - 14th International Conference on Computer Graphics Theory and Applications
330

Karuranga, S. et al. (eds) (2017) IDF Diabetes Atlas. 8th
edn. Brussels, Belgium: International Diabetes
Federation. Available at: http://diabetesatlas.org/.
Kreuter, M., Farrell, D., Olevitch, L., & Brennan, L. (2000)
Tailoring health messages: customizing communica-
tion with computer technology. Mahwah New Jersey:
Lawrence Erlbaum Associates. Available at:
https://www.popline.org/node/174671 (Accessed: 4
December 2018).
Lustria, M. L. A. et al. (2013) ‘A meta-analysis of web-
delivered tailored health behavior change
interventions’, Journal of Health Communication,
18(9), pp. 1039–1069. doi: 10.1080/10810730.2013.
768727.
Magyar, J., Magyar, G., Sincak, P. 2018. A Cloud-Based
Voting System for Emotion Recognition in Human-
Computer Interaction. 2018 World Symposium on
Digital Intelligence for Systems and Machines, pp. 109-
114.
Michie, S. et al. (2013) ‘The behavior change technique
taxonomy (v1) of 93 hierarchically clustered
techniques: Building an international consensus for the
reporting of behavior change interventions’, Annals of
Behavioral Medicine, 46(1), pp. 81–95. doi:
10.1007/s12160-013-9486-6.
Michie, S., Atkins, L. and West, R. (2014) The Behaviour
Change Wheel.
Monkaresi, H. et al. (2013) ‘Intelligent Diabetes
Lifestyle Coach’, Fifth International Workshop on
Smart Healthcare and Wellness Applications
(SmartHealth’13) - Adelaide, Australia, p. s/p.
Niess, J. and Diefenbach, S. (2016) ‘Communication Styles
of Interactive Tools for Self-Improvement’, Psychology
of Well-Being. Springer Berlin Heidelberg, 6(1), p. 3.
doi: 10.1186/s13612-016-0040-8.
Paiva, A. et al. (2017) ‘Empathy in Virtual Agents and
Robots: A Survey’, ACM Trans. Interact. Intell. Syst.,
7(3), p. 11:1–11:40. doi: 10.1145/2912150.
Provoost, S. et al. (2017) ‘Embodied conversational agents
in clinical psychology: A scoping review’, Journal of
Medical Internet Research, 19(5). doi:
10.2196/jmir.6553.
Ring, L., Bickmore, T. and Pedrelli, P. (2016) ‘An
affectively aware virtual therapist for depression
counseling’, ACM SIGCHI Conference on Human
Factors in Computing Systems (CHI) workshop on
Computing and Mental Health. doi: 10.1128/JB.01951-
12.
Rubin, V. L., Chen, Y. and Thorimbert, L. M. (2010)
‘Artificially intelligent conversational agents in
libraries’, Library Hi Tech, 28(4), pp. 496–522. doi:
10.1108/07378831011096196.
Scholten, M. R., Kelders, S. M. and Van Gemert-Pijnen, J.
E. W. C. (2017) ‘Self-guided Web-based interventions:
Scoping review on user needs and the potential of
embodied conversational agents to address them’,
Journal of Medical Internet Research, 19(11). doi:
10.2196/jmir.7351.
Shaked, N. A. (2017) ‘Avatars and virtual agents –
relationship interfaces for the elderly’, Healthcare
Technology Letters, 4(3), pp. 83–87. doi: 10.1049/
htl.2017.0009.
Sociedade Portuguesa de Diabetologia (2016) Diabetes:
Factos e Números - o ano de 2015.
Sutton, R. S. and Barto, A. (2018) Reinforcement Learning:
An Introduction. MIT PRESS. Available at:
https://mitpress.mit.edu/books/reinforcement-learning-
second-edition (Accessed: 13 November 2018).
Takac, P. et al. (2018). Cloud Based Affective Loop for
Emotional State Assessment of Elderly. In: G
D'Onofrio, ed.. Active & Healthy Aging: Novel Robotic
Solutions and Internet of Things. Avid Science, ISBN
978-93-86337-71-9
Thomaz, A. L. and Breazeal, C. (2006) ‘Reinforcement
learning with human teachers: Evidence of feedback
and guidance with implications for learning
performance’, AAAI Conference on Artificial
Intelligence, 6, pp. 1000–1005. doi: 10.1039/C3EE
43707H.
Thompson, D. et al. (2016) ‘Use of Relational Agents to
Improve Family Communication in Type 1 Diabetes:
Methods’, JMIR Research Protocols, 5(3), p. e151. doi:
10.2196/resprot.5817.
Zheng, Y., Ley, S. H. and Hu, F. B. (2018) ‘Global
aetiology and epidemiology of type 2 diabetes mellitus
and its complications’, Nature Reviews Endocrinology.
Nature Publishing Group, 14(2), pp. 88–98. doi:
10.1038/nrendo.2017.151.
Anthropomorphic Virtual Assistant to Support Self-care of Type 2 Diabetes in Older People: A Perspective on the Role of Artificial
Intelligence
331
