
Predicting Functional Recovery of Stroke Patients using Age Dependent
Model
Aleksandar Jeremic
1
, Milan Savic
2
, Ljubica Nikcevic
2
, Dejan Nikolic
3
and Natasa Kovacevic-Kostic
4
1
Department of Electrical and Computer Engineering McMaster University, Hamilton, ON, Canada
2
Special Hospital for Cerebrovascular Diseases, ”Sveti Sava”, Belgrade, Serbia
3
Physical Medicine and Rehabilitation, University Childrens Hospital, Faculty of Medicine, University of Belgrade,
Belgrade, Serbia
4
Clinical Centre of Serbia, Faculty of Medicine, University of Belgrade, Belgrade, Serbia
Keywords:
Functional Recovery, Stroke, Recovery Prediction.
Abstract:
Predicting functional recovery of stroke patients is important from both clinical and academic points of view.
From the clinical point of view it is important to patients, families and clinical workers. Most importantly, an
accurate prediction enables us to provide more accurate prognoses, set goals, manage therapies and improve
management of healthcare resources through optimal discharge procedures. For example, being able to predict
recovery of particular limbs we could potentially improve advanced planning of safe transfer in an optimally
determined time frame. Functional recovery is usually evaluated using various functional indices that evaluate
patients’ ability to perform daily living tasks. In this paper we propose to predict functional recovery using
two well established functional indices: functional independence measure and Barthels index. We model
those indices as a age dependent polynomial functions with unknown coefficients and estimate the unknown
parameters. In order to demonstrate applicability of the propose technique we compare the performance of
our non-linear polynomial model with the performance on linear MANOVA model.
1 INTRODUCTION
Stroke is a leading cause of a long-term disability and
consequently can significantly deteriorate quality of
life of the recovery patients. According to The Heart
and Stroke foundation report half of the patients re-
covering from stroke need help with daily activities.
Accordingly it would be beneficial to predict func-
tional recovery as it would allow health professionals
to provide patients with prognoses, set goals, select
therapies and plan discharge. Achieving these goals
would make possible to optimize utilization of health
care resources in order to reach maximum attainable
recovery level.
In recent years there has been considerable re-
search interest in predicting stroke recovery of par-
ticular limbs (arms, legs) (Houwink et al., 2013),
(Craig et al., 2011) or functional independence re-
covery i.e. patient ability to perform particular tasks
(Veerbeek et al., 2011). Due to inherent patient-to-
patient variability most of the proposed models (tech-
niques) require certain experiment based adjustments
in order to account for that variability. In (Brown
et al., 2015), (Kimura et al., 2017) the authors demon-
strated that functional independence measure (FIM)
can be potentially used to predict functional recov-
ery of the stroke patients. In addition to FIM, an-
other generic disability measure Barthel index (BI),
has been widely used in order to evaluate patients
ability to perform daily tasks. In recent reviews multi-
ple authors identified that different variables can work
as somewhat successful predictors of various indi-
cators (ability to walk, arm recovery, etc.) (Chum-
ney et al., 2010), (Putten et al., 1999), (Govan et al.,
2009). As we have stated earlier in addition to pre-
dicting limb recovery it may be equally important to
predict patients’ functional recovery as it can poten-
tially be used for efficient healthcare management.
In this paper we propose to predict functional in-
dependence recoveryusing coupled parametric model
based on functional independence measure (FIM)
and Barthel index (BI) measurements. As a pre-
liminary approach we evaluate applicability of the
growth curve model (generalized multivariate analy-
sis of variance model) in which the weighting coeffi-
cients are calculated optimally based on patient age.
Jeremic, A., Savic, M., Nikcevic, L., Nikolic, D. and Kovacevic-Kostic, N.
Predicting Functional Recovery of Stroke Patients using Age Dependent Model.
DOI: 10.5220/0007577702410245
In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2019), pages 241-245
ISBN: 978-989-758-353-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
241

We first propose parametric model in which the age is
accounted for by using parametric exponential func-
tions (known up to a parameter). We then estimate
the unknown parameters using part of the data set as
training set. We then evaluate the performance of the
proposed model by comparing it to the MANOVA
model and apply both models to the remaining pa-
tients. In future work we expect to include multivari-
ate dependence based on additional parameters such
as height, weight, body mass index, habits before the
stroke, etc.
The paper is organized as follows. In Section II we
describe the data set and the proposed estimation al-
gorithms. In Section III we evaluate the applicability
of the proposed algorithm using a real data set. Fi-
nally, in Section IV we discuss the results and future
work.
2 SIGNAL PROCESSING
MODELS
2.1 Data Set
We have evaluated 187 eligible participants that were
referred to the rehabilitation facility after stroke for
inclusion into rehabilitation program and follow-up.
To assess eligibility for the inclusion in the study the
patients were evaluated by board certified physiatrist
and specialist of internal medicine. Prior to the in-
clusion, all the participants were informed about the
study protocol and informed consent was obtained.
The study was approved by the Institutional Review
Board and was carried out according to the principles
of good clinical practice. The eventual onset of early
complications was indication for the termination of
the rehabilitation program for defined period of time.
The exclusion criteria for the study were recurrent hip
fractures and inability to completely finish the reha-
bilitation program or follow-up that was defined by
the study. Therefore, the initial group on admission
consisted of 217 patients, where 11 did not complete
rehabilitation program due to the worsening of health
condition and thus transferred to specialized referring
hospitals, while 19 subjects dropped out from dis-
charge period to the planned follow-up after 3 months
post-discharge.
Functional Independence Measure (FIM) was
used to evaluate patient’s functional status on 3 occa-
sions: at admission (Admission), on discharge from
the rehabilitation facility (Discharge) and 1 and 3
months after discharge (Follow-ups). After discharge,
patients were not included into any kind of rehabil-
itation program and were referred to home of resi-
dence. FIM presents valid and reliable test in the
estimation of aggregated changes in functional status
that appears in the defined period of the study eval-
uation (Young et al., 2009)-(Dodds et al., 1993). It
is composed of 18 categories that are scaled from 1-7
each (Young et al., 2009) We organize the data set in a
database consisting of 187 rows corresponding to the
patients and 9 columns of (age, FIM at the admission,
FIM at the discharge, FIM after 1 month, FIM after 3
months, BI at the admission, etc.)
2.2 Parameter Estimation
In order to be able to predict the functional recov-
ery we first propose standardized MANOVA model
in which the data is modelled as
Y = AX + E
where X is n × 5 matrix consisting of age and FIM
and Barthel indices at the admission and discharge,
A is a matrix of unknown parameters, and Y is an
n × 4 matrix consisting of FIM and Barthel indices
at 1 and 3 months after discharge respectively, and
E is the matrix of residual errors. This technique is
commonly used as a preliminary approach in order to
obtain goodness-of-fit assuming that the data can be
modelled using linear model.
In the second approach we propose to model the
the indices values after the discharge using a new non-
linear polynomial approach in which the indices val-
ues are modelled as polynomial functions of the input
parameters. Note that originally this approach was
used to model time dependent growth change and is
commonly used technique if prior knowledge is not
available. In this paper we propose to use hierarchical
polynomials in order to account for patient-to-patient
variability. In this paper we use polynomial model
given by
Y
i, j
=
q
∑
k=1
(a
k
∗ age
k−1
i
)+αFIM
admission
i
+βBI
admisson
i
+e
i,1
where q is the polynomial order, a are unknown pa-
rameters modelling age dependence, α and β are un-
known linear index parameters, and e
i, j
are residual
error (modelling noise).
To evaluate the applicability of the proposed algo-
rithms we find the normalized mean-square error and
likelihood ratio test. Note that the above models can
be easily extended to include larger number of param-
eters and this will be discussed further in Section 3.
BIOSIGNALS 2019 - 12th International Conference on Bio-inspired Systems and Signal Processing
242
3 RESULTS
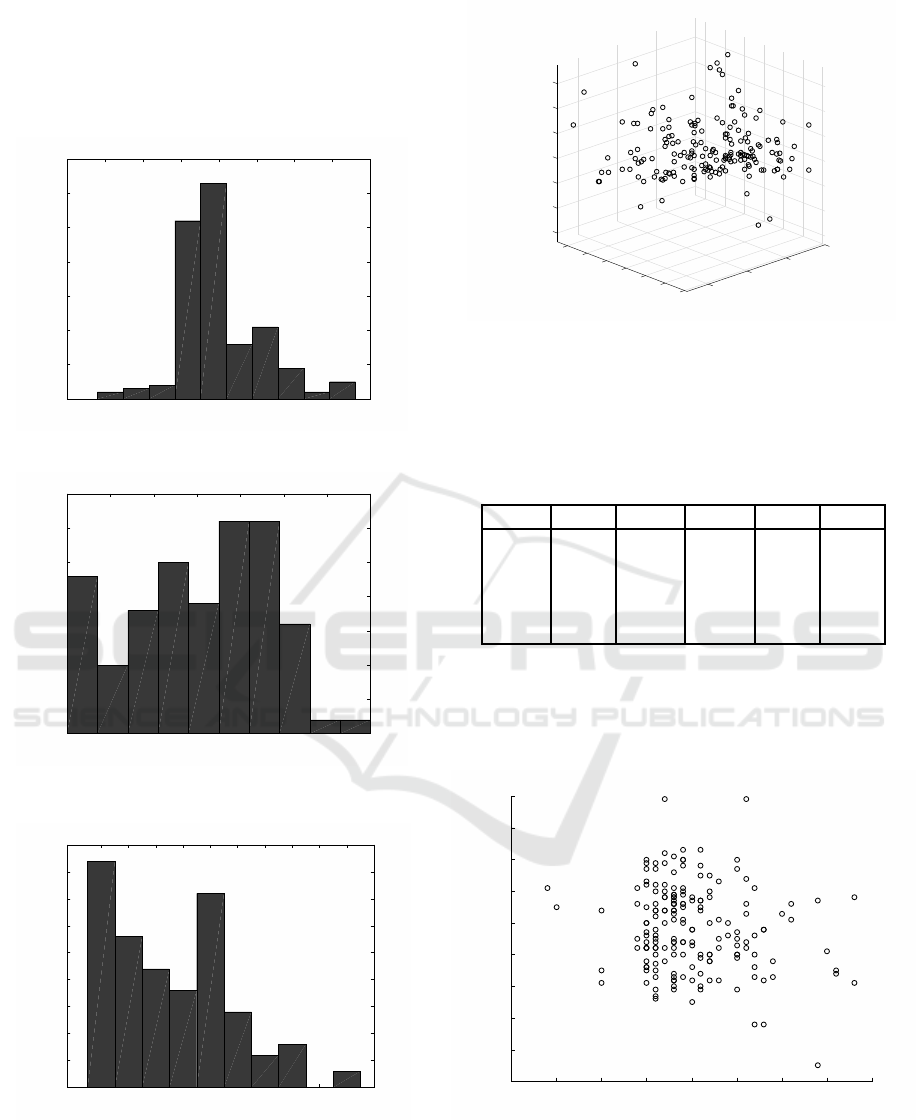
The total number of patients admitted was 187 with
age and indices characteristics being given in Figures
1-4.
50 55 60 65 70 75 80 85 90
Age
0
10
20
30
40
50
60
70
Figure 1: Histogram of patients’ age at the admission.
0 10 20 30 40 50 60 70
Barthel - admission
0
5
10
15
20
25
30
35
Figure 2: Histogram of Barthel index distribution at the ad-
mission.
20 24 28 32 36 40 44 48 52 56
FIM - admission
0
5
10
15
20
25
30
35
40
45
Figure 3: Histogram of FIM index distribution at the admis-
sion.
Additionally in Table 1 we show the correlation
coefficient of all the FIM and BI with respect to the
age. Due to existing inverse correlation relationship
the age dependent model can improve our ability to
55
60
100
65
20
70
Age
75
40
80
80
85
60
FIM 3mths
Barthel 3mths
80
60
100
120
40
140
Figure 4: 3D scatter plot of age, FIM and Barthel indices.
predict recovery. In addition the increase in corre-
lation between indices at the discharge indicate that
their values at the admission should be used simulta-
neously in order to improve the performance.
Table 1: Correlation coefficients.
Age FIMa FIM3 BIa BI3
Age 1.00 -0.05 -0.15 -0.17 -0.13
FIMa -0.05 1.000 0.69 0.87 0.64
FIM3 -0.15 0.69 1.00 0.66 0.92
BIa -0.17 0.87 0.66 1.00 0.59
BI3 -0.13 0.64 0.92 0.59 1.00
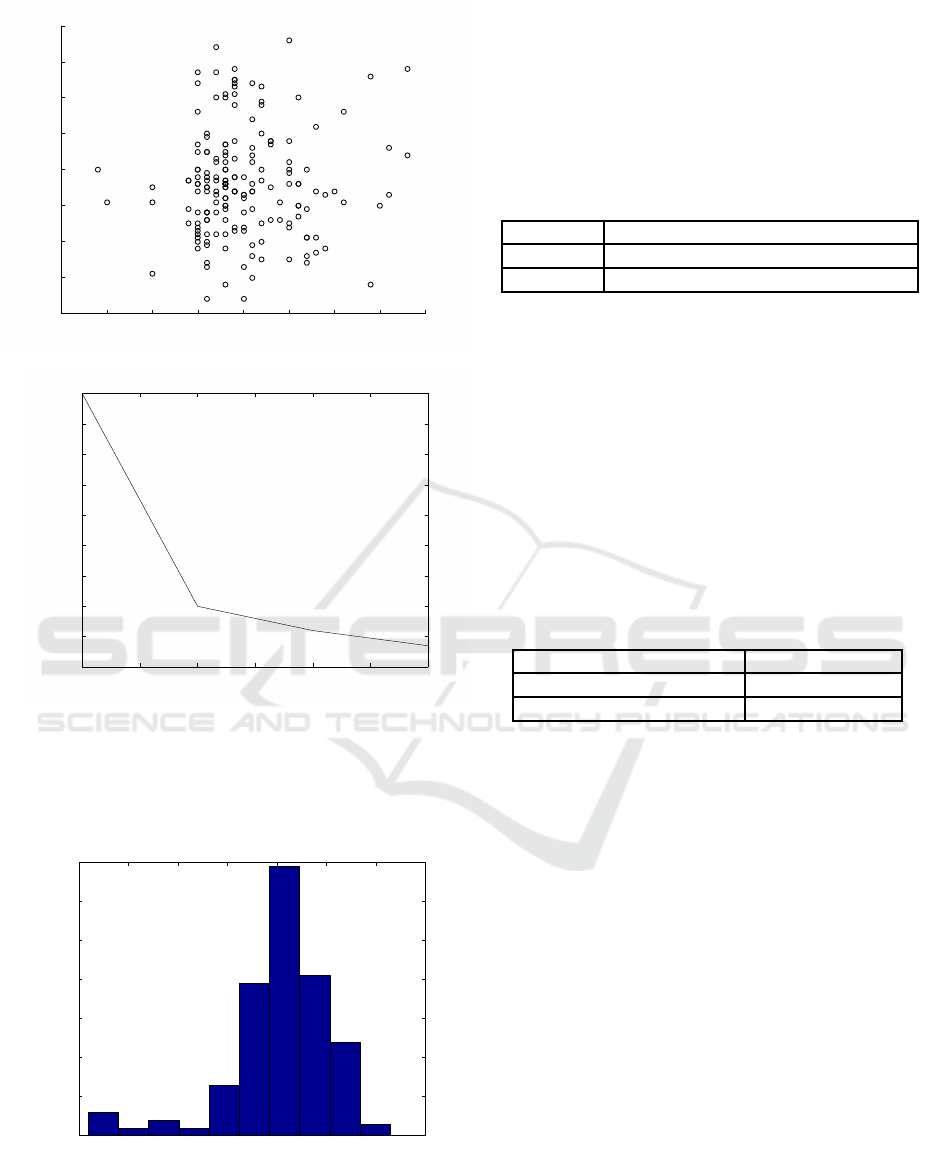
To illustrate the statistical properties of the data
sample we present two scatter plots. In Figure 5
we present the FIM change between admission and
3 months after discharge and in Figure 6 we present
similar results for BI.
50 55 60 65 70 75 80 85 90
FIM change
-10
0
10
20
30
40
50
60
70
80
Figure 5: Two-dimensional scatter of age and FIM change.
In Figure 7 we present the prediction result in
terms of mean-square error (MSE) for nonlinear
model as a function of number of parameters i.e poly-
nomial order. As expected after initial decay the MSE
slope decreases significantly which means that the
Predicting Functional Recovery of Stroke Patients using Age Dependent Model
243
50 55 60 65 70 75 80 85 90
BI change
10
20
30
40
50
60
70
80
90
Figure 6: Two-dimensional scatter of age and BI change.
1 1.5 2 2.5 3 3.5 4
Polynomial order
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
0.11
0.12
MSE
Figure 7: MSE of nonlinear model.
benefits of introducing additional parameters should
be examined in more details as they may lead to in-
crease in the computational complexity as well as
Cramer-Rao bound.
−4 −3 −2 −1 0 1 2 3
x 10
−3
0
10
20
30
40
50
60
70
MSE
Count
Figure 8: Two group clustering.
The likelihood ratio for two parameters models is
given in Table 2. From the results it seems that the
nonlinear model provides better fit in terms of the
likelihood function for the older patients. However
it should be noted that the sample size for the older
patients is slightly larger. In addition the nonlinear-
ity may play more important role at younger due to
more complex recovery processes and hence may not
be captured well by the proposed nonlinear model.
Table 2: Likelihood-ratio.
Likelihood-ratio nonlinear vs. linear
Age ≥ 65 0.35
Age ≤ 65 0.64
Finally in order to evaluate applicability of our al-
gorithm from the clinical point of view we classify
patients based on joint FIM and BI measurements in
the following way: if either FIM is larger than 36 or
BI is larger than 4 the recovery is labelled as suffi-
cient otherwise the recovery of a particular patient is
labelled as insufficient. We estimate the unknown pa-
rameters using half of the data set and evaluate its per-
formance using the other half. We repeat selection of
the training data set randomly 1000 times. The results
of the classification using predicted values are given
in Table 3.
Table 3: Classification error.
Error percentage
Insufficient recovery error 2%
Sufficient recovery error 1%
4 CONCLUSIONS
The importance of early inclusion in rehabilitation
program and exercise of older people after the stroke
could be explained by the fact that physical activity
influences the muscle strength and neural function re-
covery (Sipila et al., 2011). Such determinants are
very important particularly for individual’s quality of
life. It has been often hypothesized that the success
of recovery is extremely dependent on the timeliness
and adequacy of the treatment. While it is desirable to
provide the best possible care as soon as possible the
actual limitations that may exist in health-care sys-
tems due to a limited number of medical staff as well
as limited capacity in rehabilitation programs may
create need for appropriate planning and/or schedul-
ing.
To this purpose in this paper we proposed an al-
gorithm which can potentially be used to predict the
functional recovery which is one of the most impor-
tant factors that indicate ability for self-functioning of
BIOSIGNALS 2019 - 12th International Conference on Bio-inspired Systems and Signal Processing
244

the patients and return to daily activities. As a pre-
liminary approach we proposed and compared two
parameters linear and nonlinear models using mean
square error and likelihood-ratio. In addition the
residual vector may not be Gaussian distributed es-
pecially in which case an effort should be made to
investigate different estimation techniques that may
be more suitable for non-Gaussian models. Finally, a
clinically study with a larger number of patients and
additional types of observation should be performed
is it may provide better insight and improve quality of
the prediction models.
REFERENCES
Brown, A., Therneau, T., Schultz, B., Niewczyk, P., and
Granger, C. (2015). Measure of functional indepen-
dence dominates discharge outcome prediction after
inpatient rehabilitation for stroke. Stroke, 46(4):1038–
1044.
Chumney, D., Nollinger, K., Shesko, K., Skop, K., Spencer,
M., and Newton, R. (2010). Ability of functional in-
dependence measure to accurately predict functional
outcome of stroke-specific population: Systematic re-
view. J Rehabil Res Dev, 47(1):17–29.
Craig, L., Wu, O., Bernhardt, J., and Langhorne, P. (2011).
Predictors of poststroke mobility: Systematic review.
Int. J. Stroke, 6:321–327.
Dodds, T., Martin, D., Stolov, W., and R, D. (1993). A val-
idation of the functional independence measurement
and its performance among rehabilitation inpatients.
Arch Phys Med Rehabil, 74:531–536.
Govan, L., Langhorne, P., and Weir, C. (2009). Categorizing
stroke prognosis using different stroke scales. Stroke,
40(10):3396–3399.
Houwink, A., Nijland, R., Geurts, A., and Kwakkel, G.
(2013). Functional recovery of the paretic upper limb
after stroke: Who regains hand capacity? Arch. Phys.
Med. Rehabil., 94(94):839–844.
Kimura, Y., Yamada, M., Hamanaka, K., Tanaka, N.,
and Muroh, Y. (2017). Usefulness of the prediction
method based on a logarithmic model for functional
recovery in stroke patients: in case of using the motor-
functional independence measure score. Int. J Rehabil
Res, 40(2):134–137.
Putten, J., Hobart, J., Freeman, J., and Thompson, A.
(1999). Measuring change in disability after inpa-
tient rehabilitation: comparison of the responsiveness
of the barthel index and the functional independence
measure. J Neurol Neurosurg Psychiatry, 66(4):480–
484.
Sipila, S., Salpakoski, A., Edgren, J., Heinonen, A., Kaup-
pinen, M., and M, A.-K. (2011). Promoting mobility
after hip fracture (promo): study protocol and selected
baseline results of a year-long randomized controlled
trial among community-dwelling older people. BMC
Musculoskelet Disord, 27:277.
Veerbeek, J., Kwakkel, G., van Wegen, E., Ket, J., and Hey-
mans, M. (2011). Early prediction of outcome of ac-
tivities of daily living after stroke: A systematic re-
view. Stroke, 42:1482–1488.
Young, Y., Fan, M., Hebel, J., and Boult, C. (2009). Con-
current validity of administering the functional inde-
pendence measure (fim) instrument by interview. Am
J Phys Med Rehabil, 88:766–770.
Predicting Functional Recovery of Stroke Patients using Age Dependent Model
245
