
Why My Grandfather Finds Difficulty in using Ehealth: Differences
in Usability Evaluations between Older Age Groups
Marijke Broekhuis
1,2
, Lex van Velsen
1,2
, Silke ter Stal
1,2,
,
Jordi Weldink
1
and Monique Tabak
1,2
1
Roessingh Research and Development, Roessinghsbleekweg 33B, Enschede, The Netherlands
2
Faculty of Electrical Engineering, Mathematics and Computer Science, University of Twente, Enschede, The Netherlands
Keywords: eHealth, Older Adults, Usability Evaluations, SUS, Thematic Analysis.
Abstract: Many studies emphasize the need for more in-depth analysis of how age-related barriers influence the user
acceptance of eHealth. In this study, we elaborate on existing work in this field by identifying how age
differences affect usability evaluations in eHealth. We examined how older adults between 55-64 years
(n=10) evaluated the usability of a game-based eHealth application in comparison to adults of 65 years and
older (n=19). A concurrent think aloud protocol and the System Usability Scale (SUS) were administered to
29 participants. Usability issues were elicited from the think aloud transcripts and benchmark scores were
obtained from the SUS. We conducted both: (1) a statistical analysis on the amount of usability issues and
SUS score; and (2) a thematic analysis of the usability issues. Our study found that the 55-64 age group
encountered significantly fewer usability issues compared to the 65+ age group. Furthermore, the thematic
analysis revealed that while both groups had similar problems regarding the ‘Navigation & Structure’ category
of the game-based eHealth application, there was much variation in the other usability categories of ‘Content
& Information’, ‘Design & Presentation’ and ‘Other’. Our results can improve the development of eHealth
that support healthy ageing.
1 INTRODUCTION
Many new eHealth systems focus on supporting
healthy ageing. A major health risk facing older
adults is frailty: The decline in cognitive and physical
functions that can lead to recurrent falls, hospital
visits and even death (Fried et al., 2001). Multiple
studies have found that the symptoms of frailty can be
slowed down by staying physically active (Liu and
Fielding, 2011; Theou et al., 2011) and engaging in
cognitive training (Ng et al., 2015). The group of
older adults continues to rise – since 1990 there has
been an increase of 62% of people aged 65 years or
older (CBS, 2018) – and consequently the risks of
frailty increases. This can impose a heavy load on
health care systems. EHealth can support and relieve
health care systems by motiving older adults to stay
active by providing online physical or cognitive
training. Furthermore, whereas a health professional
can only treat a limited number of patients, eHealth
can be implemented to reach for larger groups of
older adults.
However, a recurring problem in eHealth is the
successful implementation of eHealth in the daily
lives and routines of people and health care processes.
eHealth systems should be tailored to the specific
environments and skills of the intended end-user
groups to maximize the probability of successful
implementation (Broens et al., 2007). One important
pre-requisite for the acceptance and eventual
implementation of eHealth is good usability (Broens
et al., 2007; Narasimha et al., 2017). To measure
usability of systems and to identify usability
problems, it is important to conduct usability
evaluation tests involving potential end-users. In
many studies, eHealth systems are evaluated on their
usability among the target end-user group. However,
for systems to be truly effective, they must be user-
friendly for various groups of people and be able to
compensate for variability in, for example, socio-
economic status, health literacy, technology literacy
and chronic care needs (Kreps and Neuhauser, 2010;
Lyles and Sarkar, 2015).
Several factors affect any usability evaluation.
First, adults of 65 years or older have fewer computer
skills than younger generations (Chen and Persson,
2002; Gatto and Tak, 2008). However, eHealth
systems that take into account lower computer
48
Broekhuis, M., van Velsen, L., ter Stal, S., Weldink, J. and Tabak, M.
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups.
DOI: 10.5220/0007680800480057
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 48-57
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

literacy could be perceived as cumbersome or even
unusable by the younger generation who are more
experienced with computers, tablets, and
smartphones. Second, with higher age the risk of
multimorbidity, defined as the prevalence of two or
more chronic conditions, increases (Salive, 2013).
Living with a chronic illness can induce higher levels
of stress (McEwen, 2008), that can affect how easily
users can perform tasks within a system or the types
of health information they need. Third, the study of
Wildenbos et al. (2018) identified cognitive (e.g.
working memory, spatial cognition), physical (e.g.
flexibility of joints, speed of performance),
perception (e.g. visual accommodation, colour
vision), and motivational (e.g. trust in own abilities,
efficiency in benefits) barriers that older adults often
experience when using a system. The first three are
the result of high age and can affect user interaction.
For example, people who have limited fine motor
skills could find difficulty in clicking on small
elements in a graphical user interface (GUI). Also,
motivational barriers can be different for the older
and younger generations (Wildenbos et al., 2018).
The study of Morey et al. (2017) describes how
younger participants saw more benefits in an app
intended for heart failure patients than older adults.
This can affect how users perceive the effectiveness
and usefulness of a system. Last, although older
adults often perceive how technology could benefit
them in healthy ageing, the technology should not be
unacceptably intrusive in either their homes and lives
(Jacelon and Hanson, 2013; Peek et al., 2016).
Younger generations are far more familiar with
technology and are likely to have a more positive
view on how technology can be integrated in their
daily routines.
In this study, we aimed to discover if and how
usability evaluations differ between age cohorts. We
conducted a usability evaluation of an eHealth
system, a game-based eHealth application called
‘Stranded’, between two groups: (1) adults of 55-64
years, and (2) adults of 65 years or older. The goal
was to examine if there are differences in the usability
perceptions between the two age groups in the types
and severity of usability issues.
2 METHODS AND MATERIALS
2.1 Case
In eHealth interventions, the challenge is to establish
and maintain engagement of the user for long-term
use of the technology, which is needed to establish the
targeted health goals of the older adult. ‘Stranded’ is
a game-based eHealth application that aims to engage
the older adult on the long term by using gaming
technologies. To the user, this game-based
application can be seen as an alternative interface for
the original eHealth application (called tele-
rehabilitation). The intended target group for the
application is aged 65-75 years, with sufficient
computer literacy to independently use a mobile
device or pc and with an interest in digital games. In
the design process, game design and the selection of
game elements were fitted to the specific preferences
and characteristics of the intended target group. This
resulted in a set of game design guidelines (as
described in de Vette et al., submitted) for older
adults, with the following characteristics: moderate—
to-high novelty (e.g. story line, enabling exploration),
moderate-to-high dedication (e.g. enabling
achievement, learning and mastery), low Discord and
Threat (e.g. relaxed atmosphere, not triggering
negative emotions) and low Social (i.e. solo player).
Figure 1: Screenshot of the Stranded home screen. By
clicking on one of the cabins, the user goes to the tele-
rehabilitation portal.
When Stranded is started for the first time, an opening
animation introduces the backstory. Every session
starts with the choice for the original or game-based
eHealth application. In the game, the main character
– a female explorer – is stranded on a deserted island
after her ship was caught in a storm. From the beach,
the player can explore the island and access huts.
These huts are connected to the training modules and
linked to the original tele-rehabilitation. In addition,
the player can go to a virtual crop field, visit the rest
of the island and play mini-games there, or find out
about a wooden quay where a boat it built. Items wash
up on the beach in bottles, which contents are adapted
based on the outcomes in the training module. For
example, the bottles can contain items that can be
stored in a trophy hut or seeds that can be planted in
the crop field. The locations on the island map show
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups
49

levels that can be played, which can be opened by
completing a training schedule in the huts. In these
locations, several mini-games can be played. After
finishing a level, the player receives a part of a boat.
After finishing all levels (corresponding to the
finishing of the 12 week rehabilitation programme),
your boat is built and you can leave the island.
2.2 Participants
Participants were eligible for participation in this
study if they fitted within one of the two age groups
and if they had basic computer skills, such as sending
an e-mail. We recruited participants through a Dutch
panel for adults aged between 55 and 64 and we
collaborated with local geriatric physiotherapy
practices to recruit participants aged 65 or older.
2.3 Study Procedure
Before participation, all respondents completed and
signed an informed consent form. First, participants
were asked about their demographics after which they
were given five tasks to complete within the game-
based eHealth application. The participant had five
minutes to fulfil each task. During these tasks, they
had to verbalize their thoughts. After completing
these tasks, they filled out the System Usability Scale
(SUS) (Brooke, 1996).
2.4 Data Analysis
Audio recordings and screen-capture recordings were
made during the usability evaluation sessions and
transcribed. Usability issues were identified from the
Table 1: Overview of the critical issues and corresponding usability category.
ID
Age groups
Usability issues
N&S
C&I
D&P
Other
1.1
55-64 / 65+
The user does not know the purpose of the cabins in the
home-screen.
X
1.2
55-64 / 65+
The user cannot find the entrance to the kitchen.
X
1.3
55-64 / 65+
The user has difficulty distinguishing clickable and non-
clickable elements in the interface.
X
1.4
55-64 / 65+
The user cannot find the ingredient list in the kitchen
X
1.5
55-64 / 65+
The user does not understand that in the island overview
interface, each circle represents a mini game.
X
1.6
55-64 / 65+
The user cannot find the direction sign to the island
overview in the home-screen
X
1.7
55-64 / 65+
The system does not offer the user any support for entering
special characters while logging in
X
1.8
55-64 / 65+
The user believes the introduction of a physical exercise is
the actual explanation of the exercise.
X
1.9
55-64 / 65+
The interface does not show where the physical exercises
can be found (e.g. through the physical exercise cabin)
X
2.1
65+
The user wants to leave the game because he or she cannot
find the elements he or she is looking for (e.g. exercise, e-
mail, mini game)
X
2.2
65+
The user has difficulty understanding the connection
between the various gaming elements
X
2.3
65+
The system does not provide an option to erase incorrect
text from the entry boxes in the login screen without using
the keyboard
X
2.4
65+
The user does not understand the connection between the
gaming interface and the tele-rehabilitation portal
X
2.5
65+
The user does not understand the purpose of the play button
in the exercise video. He or she believes this button is used
to go to the next exercise.
X
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
50

transcripts and classified as a minor, serious, or
critical, following the procedure by Van Velsen et al.
(2011). The following definitions of Duh et al. (2006)
were used for the severity classification:
Minor issue: Occurred infrequently among the
participants and/or the problem only increased
task completion time slightly;
Serious issue: Occurred frequently among the
participants and/or the problem severely
increased task completion time;
Critical issue: Occurred when all participants
had the same problem and/or the problem
prevented participants from completing tasks.
The identification of the usability issues and
determination of the severity of each issue, was first
performed by one coder (MB). A second coder (LvV)
independently analysed a subset of the data.
Discrepancies between de codebooks were discussed
and overcome, after which the first coder (MB) again
coded the whole codebook, and finally the second
coder (LvV) reviewed the codebook.
Next, based on the framework proposed Van der
Geest (2004), each usability issue was grouped into
one of the following four categories: (1) Navigation
& Structure; (2) Content & Information; (3) Design
& Presentation; and (4) Other. This categorization
was performed by a pair of two researchers (MB &
StS). A third researcher (LvV) checked the final
categorization. After discussions between the
researchers about disparities, final alterations to the
categorization of the usability issues were made.
Table 1 shows a subset of the codebook, the critical
issues per age group with corresponding usability
category.
2.5 Statistical Analysis
Tests for normality indicated that normal
distributions could not be assumed. Therefore, the
data was analysed by applying non-parametric
methods. Mann-Whitney U tests were calculated to
measure: (1) if there was a significant difference
between the average SUS scores of the two age
groups; (2) if there were significant differences
between the number of minor, serious, and critical
issues between the two age groups; and (3) if there
were significant differences between unique minor,
serious, and critical issues between the two age
groups.
3 RESULTS
3.1 Demographics
In total, 29 older adults participated. Table 2 gives a
complete overview of the demographics of both age
groups. Ten respondents aged 55-64 participated in
the study. Six of them (60%) were male, and four
(40%) were female. The average age was 59 years.
Their educational background included lower
vocational education (20%), vocational education
(40%), and higher vocational education (40%).
A total of 22 older adults of 65+ years agreed to
participate, of which 19 completed the study. Twelve
of them were male (63.2%) and seven were female
(36.8%). Their mean age was 74 years and their level
of education consisted of elementary education
(5.3%), lower vocational education (42.1%),
vocational education (26.3%), and higher vocational
education (21.1 %). However, one participant did not
mention her educational background.
3.2 SUS Scores
With an average SUS score of 42.0, the usability of
Stranded was found to be just below the acceptability
threshold of the SUS scoring scale for 55-64 age
group. The participants of the 65+ age group gave the
game-based eHealth application ‘Stranded’ a SUS
score of 26.7, which means that the usability of
Stranded is unacceptably poor.
3.3 Usability Issues
There were in total 398 usability issues found across
all participants: 111 usability issues in the 55-64 age
group and 287 usability issues in the 65+ age group.
We deduplicated usability issues across participants
per age group, which resulted in 105 unique usability
issues. Finally, we examined which usability issues
were being present for both age groups and again
removed duplicates. This resulted in 26 unique
usability issues that were found among participants in
both age groups; 44 issues that were only found in the
65+ age group, and nine issues that were only found
in the 55-64 age group. Table 3 shows the number of
minor, serious, and critical usability issues for each
age group.
The 55-64 age group yielded a total of 12 (34.2%)
minor, 14 (40%) serious, and 9 (25.7%) critical
unique usability issues. Examples of minor issues are
‘Not sure how to use the button game modus’, and
‘Restart-button is mistaken for a start-button’.
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups
51

Examples of serious issues are ‘Physical exercises do
not provide information about the length of each
exercise’, and ‘Difference between gaming elements
and computer icons (e.g. game buttons and windows-
icons) is unclear’. Examples of critical issues are
‘Direction signs to the crop field cannot be found in
the home page of the game-based eHealth
application’, and ‘The purpose of the cabins in the
home-screen is unclear for the user’.
The think aloud protocol elicited 32 (45.7%)
minor, 24 (34.3%) serious, and 14 (20%) critical
usability issues for the 65+ age group. Minor issues
included ‘Avatar looks like a male rather than a
female character’, and ‘Dislikes the music’. Serious
issues were problems such as ‘The help-page
provides insufficient information to support the
playing of the game’, and ‘The application does not
explain how to build the boat’ (e.g. through
performing the physical exercises). Issues such as
‘Connection between the tele-rehabilitation portal
and the gaming interface is unclear’, and ‘The gaming
interface provides insufficient information for the
user about where the physical exercises can be
found’, were classified as critical issues.
Table 2: Demographics (age, education, technology usage) of the 55-64 age group and the 65+ age group.
Age group
ID
Sex
Age
Education
Technology usage
55-64
01
M
60
Vocational
PC/Laptop, Smartphone, Tablet
02
M
55
Higher vocational
PC/Laptop, Smartphone
03
M
63
Vocational
PC/Laptop, Smartphone, Tablet
04
M
57
Vocational
PC/Laptop, Smartphone, Tablet
05
F
58
Higher vocational
PC/Laptop, Smartphone, Tablet
06
F
63
Higher vocational
PC/Laptop, Smartphone, Tablet
07
M
59
Lower vocational
PC/Laptop, Smartphone, Tablet
08
F
57
Lower vocational
PC/Laptop, Smartphone
09
M
56
Higher vocational
PC/Laptop, Smartphone
10
F
59
Vocational
PC/Laptop, Smartphone
65+
11
F
68
Lower vocational
PC/Laptop, Smartphone, Tablet
12
M
79
Vocational
PC/Laptop
13
M
78
Higher vocational
PC/Laptop, Smartphone, Tablet
14
M
67
Lower vocational
Smartphone
15
M
87
Lower vocational
PC/Laptop, Smartphone
16
M
65
Vocational
PC/Laptop, Smartphone
17
M
72
Higher vocational
PC/Laptop, Smartphone, Tablet
18
M
69
Vocational
PC/Laptop, Smartphone
19
M
80
Higher vocational
PC/Laptop
20
M
77
Lower vocational
PC/Laptop, Smartphone, Tablet
21
M
69
Elementary education
PC/Laptop, Smartphone, Tablet
22
F
74
Higher vocational
PC/Laptop, Smartphone
23
M
74
Lower vocational
Smartphone, Tablet
24
F
82
Lower vocational
PC/Laptop, Smartphone
25
F
72
n.a.
PC/Laptop
26
F
77
Lower vocational
Smartphone, Tablet
27
F
77
Vocational
PC/Laptop, Smartphone, Tablet
28
M
65
Vocational
PC/Laptop, Smartphone
29
F
79
Lower vocational
PC/Laptop, Tablet
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
52

3.4 Statistical Differences between Age
Groups
Mann-Whitney U-test scores were computed between
the mean scores of the SUS and the numbers of minor,
serious, and critical usability issues. When
considering the SUS scores between the two age
groups, the 65+ age group (Mdn = 27.5, IQR = 10-
42.5), significantly differed from the 55-64 age group
(Mdn = 38.8, IQR = 30.6-48.8), U = 52, p = .05. Also,
the number of serious issues in the 65+ age group
(Mdn = 8, IQR = 6-9), significantly differed from that
in the 55-64 age group (Mdn = 4.5, IQR = 3-6.3), U
= 33, p = .004. Finally, the number of critical issues
in the 65+ age group (Mdn = 4, IQR = 3-5) showed a
significant difference with that in the 55-64 age group
(Mdn = 1, IQR = 0-3), U = 14, p = .001. The
difference in the number of minor issues was not
significant between the 55-64 age group (Mdn = 5,
IQR = 2-7.5) and the 65+ age group (Mdn = 3, IQR =
2-5), U = 118.5, p = .28. Figure 2 illustrates the
differences of the medians between age groups for the
usability issues using box plots.
3.5 Thematic Analysis of Usability
Issues
The usability issues were grouped into one of the
following four categories: (1) Navigation &
Structure; (2) Content & Information; (3) Design &
Presentation; and (4) Other. The first category
included 11 usability issues, of which six issues were
present for both age groups. The second category
contained 19 usability issues, of which six issues were
present for both age groups. In the third category,
there were 29 usability issues, of which ten issues
were present for both age groups. The final category
included 20 usability issues, of which four were
present for both age groups. Figure 3 shows the
number of minor, serious and critical usability issues
per category for each age group.
Table 3: Usability issues (minor, serious, critical) per age
group.
55-64
65+
Both
Minor
7
27
4
Serious
2
12
13
Critical
-
5
9
Total
9
44
26
3.5.1 Navigation & Structure
Participants in both age groups had difficulty
controlling game elements, such as moving the avatar
in the GUI and objects in the mini games. Also,
navigation to different locations (the tele-
rehabilitation portal and the mini games) caused
problems because the system gives little information
to users about where various elements can be found.
When a user by accident found the mini games by
chance, he or she had difficulty rediscovering those
locations in a subsequent task. Most participants
preferred the use of the browser navigation elements
to the navigation elements in the GUI. The main
difference between the age groups was that
participants in the 65+ age group sometimes decided
to quit the game because they thought they had to go
somewhere else to locate the physical exercises,
whereas the younger age group continued their search
in the GUI.
3.5.2 Content & Information
The information available in the game-based eHealth
application did not provide sufficient information for
users to feel in control of the game. For both age
groups, participants puzzled over the use and purpose
of various GUI elements, namely: (1) the cabins in the
home-screen, which are the link to the tele-
rehabilitation portal; (2) the buttons ‘game modus’ (to
switch off the gamified interface) and ‘basic modus’
(for people with color sensitivity or contrast
difficulties); (3) the functionalities in the mail inbox;
(4) the login entry fields, and (5) the use of the
vegetable garden. Furthermore, in both age groups
there was ambiguity about the overall goal, namely to
build a boat to escape the island. In the 65+ group,
participants mentioned that they did not understand
how they can build a boat, and in the 55-64 age group
they did not understand the purpose of the docks (in
which the boat will be shown). The difference is that
this was a minor issue for the 55-64 age group, but a
serious issue for the 65+ group.
The participants in the age group 55-64 required
additional information on various elements of the
game-based eHealth application and the connecting
tele-rehabilitation portal. For example, when
following the physical exercises, they needed more
explanation on the length and frequency of these
exercises. The participants in the 65+ age group
experienced more difficulty understanding the
available information. The information provided in
the help video on how to use the mail inbox runs too
quickly, and participants did not understand the
information provided in the GUI.
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups
53
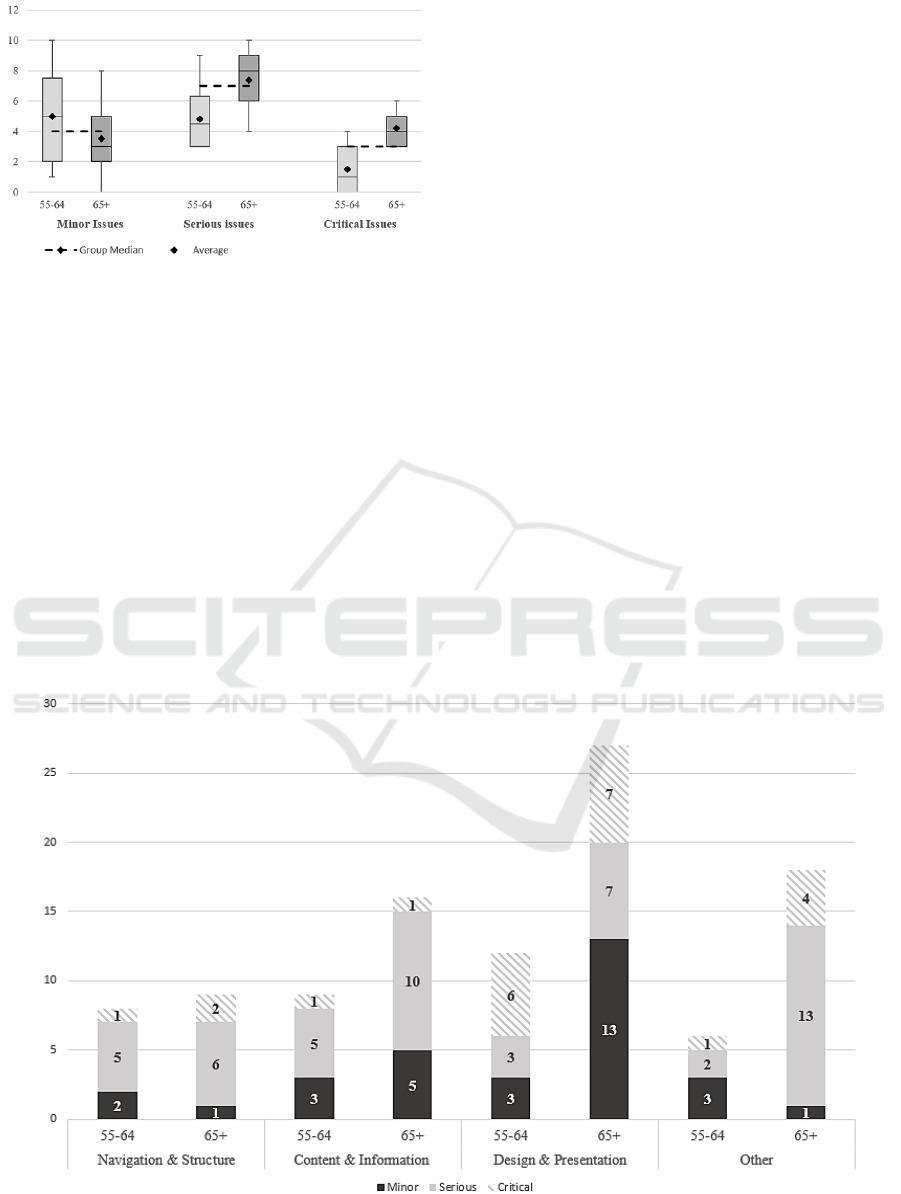
Figure 2: Box plots of the number of minor, serious and
critical issues per age group.
3.5.3 Design & Presentation
Similar usability issues regarding the aesthetics and
design for both age groups were mostly critical and
serious issues. Participants had problems discovering
the direction signs in the home screen of the GUI,
which prevented or slowed down task completions.
Furthermore, the design of buttons in the GUI led to
confusion. For example, every time a user went back
to the home screen the information button lighted up.
This led users to believe that there was new or
additional information available for them to read,
which was not necessarily the case. Also, every
participant sometimes had trouble discriminating
between clickable and non-clickable GUI elements.
Looking at the unique issues for each age group,
there were many additional usability issues in the 65+
age group, while just two minor issues were unique
for the 55-64 age group. In the 65+ group, there were
several issues regarding the aesthetics. Participants
did not like the music and the objects in the GUI were
displayed in too small a size for them to identify.
Also, participants ran into problems because of the
layout of GUI elements. Since some elements are
placed closely together, users often clicked on the
wrong element without noticing. Moreover, one
respondent who was color blind could not understand
the color codes in the tele-rehabilitation portal.
Finally, some participants reported usability issues
regarding the design but these problems were are
actually due to their unfamiliarity with standard
design principles of computer interfaces.
3.5.4 Other
In both age groups difficulties were reported
regarding the accessibility of the system. Users had
trouble creating special characters to log on and the
game-based eHealth application is not adaptive for
people living with dyslexia or other reading
problems. There were just two minor usability issues
that were only present in the 55-64 age group. One of
these is that participants had no problems locating the
direction sign to the garden, but difficulty pressing
this sign because the clicking area only partly
Figure 3: Minor, serious and critical usability issues per usability category for both age groups (55-64 and 65+).
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
54

technical aspects, such as the page load time. For
example, when participants clicked on a direction
sign, the loading of the next interface screen holds of
loading the next page until the avatar has walked to
the direction sign. Issues that were considered critical
were issues where participants had difficulty grasping
the game story and the overall goal of the game-based
eHealth application. The connection between the
game-based eHealth application and the tele-
rehabilitation portal often remained unclear and
participants did not understand the game story. These
were critical issues that prevented users from
completing the given tasks.
4 DISCUSSION
This study examined how age-related barriers affect
the usability evaluations of an eHealth system. There
were four main results. First, participants of the 55-
64 age group rated the overall system usability
significantly higher than participants of the 65+ age
group. Second, participants of the 55-64 age group
had significantly fewer usability issues than
participants for the 65+ age group. Third, the
identified usability issues reported by the 55-64 age
group were less severe than in the 65+ age group.
Last, there are differences in the types of usability
issues found by the two age groups, except for
navigation within the game-based eHealth
application. Navigation & Structure issues were quite
similar for both groups. In contrast, Design &
Presentation and Content & Information, and Other
issues had more variation in severity and content
between the two age groups.
The statistical differences between the age groups
can be explained via the groups’ digital skills. Van
Deursen et al. (2009) found that a higher age
especially affects operational and formal internet
skills, such as operating an internet browser and
maintaining sense of orientation. In this study, we
found similar results. Although in both groups
participants had orientation problems in the system,
we found differences regarding operational skills
between the age groups. The participants in the 65+
age group had difficulty with understanding technical
features and functionalities of the game-based
eHealth application. These issues were not present for
the 55-64 age group. Also, the 65+ age group had
more serious issues related to understanding the
content and the purposes of GUI elements, like
buttons, than did the older adults aged 55-64, in the
game-based eHealth application. In addition, for the
65+ age group, these issues were often more severe,
serious or critical, than for the 55-64 age group.
However, these statistical differences do not yet
explain the low SUS scores for both age groups.
Typically, a SUS score does not drop below the
threshold of 50 (Bangor, Kortum and Miller, 2008).
For older adults to use technology, it is important that
they perceive some benefits and relevance in using
the technology (Melenhorst and Bouwhuis, 2004).
However, from the usability test, it became clear that
many participants had difficulty grasping the purpose
of the cabins in the home–screen (i.e. to access the
tele-rehabilitation portal). Also, they did not
understand the connection between the gamified
interface and the portal. It could be that the gamified
interface slightly blurs the underlying goal of
improving one’s physical condition and making
progress in the game by performing physical
exercises.
The thematic analysis also revealed differences
between the age groups, in the type of usability
categories. These differences can be explained
because the categories refer to various factors of how
a user interacts with a system. Navigation & Structure
issues result from goal-driven strategies. A user must
understand and predict consequences by clicking on
a GUI element (Kitajima, Blackmon and Polson,
2000). This requires the system to have an intuitive
and logical structure. In contrast, the categories of
Content & Information and Design & Presentation
refer to functionalities of the system that support a
user in his or her quest. Users may need varying levels
of detailed information and support. For eHealth,
information needs to be tailored to users’ levels of
health literacy (Chew, Bradley and Boyko, 2004),
motivation to adopt a healthy lifestyle (Harjumaa and
Oinas-Kukkonen, 2009) and both physical and
cognitive functioning (Flores et al., 2008; Gerling et
al., 2012; Hoogendam et al., 2014). In the category
‘Other’ there were several issues related to the
accessibility of the system. The study of Huber and
Vitouch (2008) found that the accessibility of the
system can significantly affect the usability ratings.
The current usability evaluation methods do not
take these additional factors into account to
compensate for its potential effect on the perceived
usability. Usability experts and researchers working
in the field of healthy ageing could use these results
to optimize and standardize usability evaluations and
benchmarks of eHealth systems. As we found in the
thematic analysis, within each category there is a
large variance in the type of usability issues. For
example, in the Design & Presentation category the
issues varied from disliking music to problems with
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups
55

graphics resulting from color blindness. Also, the
Other category is as an undefined category
comprising a group of leftover usability issues, such
as technical and accessibility issues, that could not be
placed in the other three categories. We need more
information on factors that affect usability in the
eHealth domain and which aspects of the system
affect the user-friendliness of eHealth.
4.1 Study Limitations
This study applied fixed age boundaries in the
evaluation of usability. Of course, in real-life there
will be less distinctive age boundaries for users of
eHealth systems. Also, in the literature, there is a
growing body of research on how age, especially
older age, affects usability, user acceptance and
perceived intention-to-use of eHealth systems in daily
life. However, in our study we wanted to know in
more detail which aspects of a system’s usability are
affected by age-related barriers. We did this by
examining differences in the types and severity scores
of usability issues. Finally, this study used a
qualitative approach to examine how age differences
affected usability. To generalize the results to the
elderly population, we need to conduct larger studies
on representative cross sections of the ageing
population.
5 CONCLUSIONS
Current usability evaluations in eHealth do not take
into account variations in end-user populations and
their effects on the perceived usability of a system.
This study found that the perceptions of usability
differ between two consecutive age groups. Not only
were there differences in the type of usability issues
between the age groups, but also statistically
significant differences were found in the number of
serious and critical usability issues that each age
group encountered. This study has established that
variations in end-user populations affect usability
evaluations in eHealth. The next step is to examine
which factors we need to take into account to measure
effectively the user-friendliness of eHealth
applications.
ACKNOWLEDGEMENTS
This work is conducted within the context of the IMI
SPRINTT (IMI-JU 115621) project.
REFERENCES
Bakkes, S., Tan, C. T. and Pisan, Y. (2012) ‘Personalised
Gaming:A Motivation and Overview of Literature’, in
Proceedings of The 8th Australasian Conference on
Interactive Entertainment: Playing the System-IE ’12.
doi: 10.1145/2336727.2336731.
Bangor, A., Kortum, P. T., & Miller, J. T. (2008). An
empirical evaluation of the system usability scale.
International Journal of Human-Computer
Interaction, 24(6), 574–594. https://doi.org/10.1080/
10447310802205776
Broens, T., Huis in‘t Veld, R., Vollenbroek-Hutten, M.M.R.,
Hermens, H.J., van Halteren, A.T. and Nieuwenhuis,
L.J.M. (2007) ‘Original article " Determinants of
successful telemedicine implementations : a literature
study’, Journal of Telemedicine and Telecare, 13(6), pp.
303–309.
Brooke, J. (1996) ‘SUS - A quick and dirty usability scale’,
Usability evaluation in industry. doi: 10.1002/
hbm.20701.
Central Bureau for Statistics (CBS) (2018, October 31).
Statistics Netherlands: Population: key figures [Dataset].
Retrieved from: https://opendata.cbs.nl/statline/#/CBS/
nl/dataset/37296ned/table?ts=1537956882273
Chen, Y. and Persson, A. (2002) ‘Internet use among young
and older adults: Relation to psychological well-being’,
Educational Gerontology, 28(9), pp. 731–744. doi:
10.1080/03601270290099921.
Chew LD, Bradley KA, B. E. (2004) ‘Brief questions to
identify patients with\rinadequate health literacy’,
Family Medicine, 36(8), pp. 585–594. doi: 10.1186/
1471-2458-12-80.
van Deursen, A. J. A. M. and van Dijk, J. A. G. M. (2009)
‘Using the Internet: Skill related problems in users’
online behavior’, Interacting with Computers. Elsevier
B.V., 21(5–6), pp. 393–402. doi: 10.1016/j.intcom.
2009.06.005.
Duh, H. B.-L., Tan, G. C. B. and Chen, V. H. (2006)
‘Usability evaluation for mobile device: a comparison
of laboratory and field tests’, Proceedings of the 8th
conference on Human-computer interaction with
mobile devices and services, pp. 181–186.
Flores, E., Tobon, G., Cavallaro, E., Cavallaro, F.I., Perry,
J.C. and Keller, T. (2008) ‘Improving patient
motivation in game development for motor deficit
rehabilitation’, in Proceedings of the 2008
International Conference in Advances on Computer
Entertainment Technology - ACE ’08, p. 381. doi:
10.1145/1501750.1501839.
Fried, L. P., Tangen, C.M., Walston, J., Newman, A.B.,
Hirsch, C., Gottdiener, J., Seeman, T. Tracy, R., Kop,
W.J., Burke, G., McBurnie, M.A. (2001) ‘Frailty in
Older Adults: Evidence for a Phenotype’, The Journals
of Gerontology Series A: Biological Sciences and
Medical Sciences. doi: 10.1093/gerona/56.3.M146.
Gatto, S. L. and Tak, S. H. (2008) ‘Computer, Internet, and
e-mail use among older adults: Benefits and barriers’,
Educational Gerontology, 34(9), pp. 800–811. doi:
10.1080/03601270802243697.
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
56

van der Geest, T. (2004) ‘Beyond accessibility: Comparing
three website usability test methods for people with
impairments’, in Proceedings of the HCI 2004, pp.
129–132.
Gerling, K. M., Schulte, F.P., Smeddinck, J. and Masuch,
M. (2012) ‘Game design for older adults: Effects of
age-related changes on structural elements of digital
games’, in Lecture Notes in Computer Science
(including subseries Lecture Notes in Artificial
Intelligence and Lecture Notes in Bioinformatics). doi:
10.1007/978-3-642-33542-6_20.
Harjumaa, M. and Oinas-Kukkonen, H. (2009) ‘Persuasive
Systems Design: Key Issues, Process Model, and
System Features’, Communications of the Association
for Information Systems, 24(28), pp. 485–500. doi:
10.17705/1CAIS.02428.
Hoogendam, Y. Y., van der Lijn, F., Vernooij, M.W.,
Hofman, A., Niessen, W.J., van der Lugt, A., Ikram,
M.A., van der Geest, J.N. (2014) ‘Older Age Relates to
Worsening of Fine Motor Skills: A Population-Based
Study of Middle-Aged and Elderly Persons’, Frontiers
in Aging Neuroscience. 2014/10/14, 6, p. 259. doi:
10.3389/fnagi.2014.00259.
Huber, W. and Vitouch, P. (2008) ‘Usability and accessibility
on the internet: Effects of accessible web design on
usability’, Lecture Notes in Computer Science (including
subseries Lecture Notes in Artificial Intelligence and
Lecture Notes in Bioinformatics), 5105 LNCS, pp. 482–
489. doi: 10.1007/978-3-540-70540-6_69.
Jacelon, C. S. and Hanson, A. (2013) ‘Older adults’
participation in the development of smart
environments: An integrated review of the literature’,
Geriatric Nursing. Elsevier Ltd, 34(2), pp. 116–121.
doi: 10.1016/j.gerinurse.2012.11.001.
Kelders, S. M, Kok, R.N., Ossebaard, H.C., van Gemert-
Pijnen, J.E.W.C. (2012) ‘Persuasive system design does
matter: A systematic review of adherence to web-based
interventions’, Journal of Medical Internet Research.
doi: 10.2196/jmir.2104.
Kitajima, M., Blackmon, M. H. M. and Polson, P. G. P.
(2000) ‘A Comprehension-based Model of Web
Navigation and Its Application to Web Usability
Analysis’, People and Computers XIV — Usability or
Else! SE - 24, pp. 357–373. doi: 10.1007/978-1-4471-
0515-2_24.
Kreps, G. L. and Neuhauser, L. (2010) ‘New directions in
eHealth communication: Opportunities and challenges’,
Patient Education and Counseling, 78(3), pp. 329–336.
doi: 10.1016/j.pec.2010.01.013.
Liu, C. K. and Fielding, R. A. (2011) ‘Exercise as an
Intervention for Frailty’, Clinics in Geriatric Medicine.
2010/11/26, 27(1), pp. 101–110. doi: 10.1016/
j.cger.2010.08.001.
Lyles, C. R. and Sarkar, U. (2015) ‘Health Literacy,
Vulnerable Patients, and Health Information Technology
Use: Where Do We Go from Here?’, Journal of General
Internal Medicine, 30(3), pp. 271–272. doi: 10.1007/
s11606-014-3166-5.
McEwen, B. S. (2008) ‘Central effects of stress hormones
in health and disease: Understanding the protective and
damaging effects of stress and stress mediators’,
European Journal of Pharmacology, 583(2–3), pp.
174–185. doi: 10.1016/j.ejphar.2007.11.071.
Morey, S. A., Barg-Walkow, L. H. and Rogers, W. A.
(2017) ‘Managing heart failure on the Go: Usability
issues with mHealth apps for older adults’, Proceedings
of the Human Factors and Ergonomics Society, 2017–
Octob, pp. 1–5. doi: 10.1177/1541931213601496.
Melenhorst, A.-S., Rogers, W. A., & Bouwhuis, D. G.
(2006). Older adults’ motivated choice for
technological innovation: Evidence for benefit-driven
selectivity. Psychology and Aging, 21(1), 190–195.
https://doi.org/10.1037/0882-7974.21.1.190
Narasimha, S., Madathil, K.C., Agnisarman, S., Rogers, H.,
Welch, B., Ashok, A., Nair, A. and McElligot, J. (2017)
‘Designing Telemedicine Systems for Geriatric Patients:
A Review of the Usability Studies’, Telemedicine and e-
Health, 23(6), pp. 459–472. doi: 10.1089/tmj.2016.0178.
Ng, T., Feng, L., Nyunt, M., Feng, L., Niti, M., Tan, B., Chan,
G., Khoo, S., Chan, S., Yap, P. and Yak, K. (2015)
‘Nutritional, Physical, Cognitive, and Combination
Interventions and Frailty Reversal among Older Adults:
A Randomized Controlled Trial’, American Journal of
Medicine. doi: 10.1016/j.amjmed.2015.06.017.
Peek, S. T. M., Luijkx, K.G., Rijnaard, M.D., Nieboer,
M.E., van der Voort, C.S., Aarts, S., van Hoof, J.,
Vrijhoef, H.J.M. and Wouters, E.J.M. (2016) ‘Older
Adults’ Reasons for Using Technology while Aging in
Place’, Gerontology, 62(2). doi: 10.1159/000430949.
Salive, M. E. (2013) ‘Multimorbidity in older adults’,
Epidemiologic Reviews, 35(1), pp. 75–83. doi:
10.1093/epirev/mxs009.
Theou, O., Stathokostas, L., Roland, K.P., Jakobi, J.M.,
Patterson, C., Vandervoort, A.A. and Jones, G.R.
(2011) ‘The Effectiveness of Exercise Interventions for
the Management of Frailty: A Systematic Review’,
Journal of Aging Research. 2011/05/18, 2011, pp. 1–
19. doi: 10.4061/2011/569194.
van Velsen, L., van der Geest, T., & Klaassen, R. (2011).
Identifying usability issues for personalization during
formative evaluations: A comparison of three methods.
International Journal of Human-Computer Interaction,
27(7), 670–698. https://doi.org/10.1080/10447318.
2011.555304
de Vette F., Tabak, M. (submitted). The 6D Framework: An
Evidence-Based Tool for Designers of Serious Games.
de Vette, F., Tabak, M., Dekker- van Weering, M. and
Vollenbroek-Hutten, M. (2015) ‘Engaging Elderly
People in Telemedicine Through Gamification’, JMIR
Serious Games. doi: 10.2196/games.4561.
Wildenbos, G. A., Peute, L. and Jaspers, M. (2018) ‘Aging
barriers influencing mobile health usability for older
adults: A literature based framework (MOLD-US)’,
International Journal of Medical Informatics. Elsevier,
114(December 2017), pp. 66–75. doi: 10.1016/j.
ijmedinf.2018.03.012.
Why My Grandfather Finds Difficulty in using Ehealth: Differences in Usability Evaluations between Older Age Groups
57
