
Contact-less Vital Parameter Determination: An e-Health Solution for
Elderly Care
Christian Wiede, Julia Richter and Gangolf Hirtz
Department of Electrical Engineering and Information Technology,
Chemnitz University of Technology, Reichenhainer Str. 70, 09126 Chemnitz, Germany
Keywords:
Remote Vital Parameter Determination, Home Environments, e-Health, Contact-less, Heart Rate, Respiration
Rate, Oxygen Saturation, Blood Pressure.
Abstract:
Vital parameters are key figures for the basis functions of the human body. Without these basis body functions,
such as the heart beat, life is impossible. Therefore, vital parameters are indicators for a person’s general
medical condition. In recent years, the topic of vital parameter monitoring has been increasingly studied
in the field of e-health. Especially the contact-less determination of vital parameters, such as heart rate,
respiration rate, oxygen saturation and blood pressure, with consumer cameras brings a variety of advantages.
In this work, we present methods to determine the mentioned vital parameters in a contact-less, optical way.
Furthermore, we evaluated these methods for an utilisation in home environments with respect to elderly care.
As a result, the remote determination of heart and respiration rate show reliable measurements, which makes
the proposed methods ready for the application in home environments.
1 INTRODUCTION
e-Health has become an evolving field in recent ye-
ars. The business consultancy Roland Berger expects
that the e-health market will grow by 21 % every year
(Berger et al., 2016). Thereby, e-health is a collective
term for all applications of digital technology in the
health care sector. That comprises electronic health
records in the same way as telemedicine or consumer
health informatics. Especially self-monitoring health
care devices, such as fitness trackers, mobile apps,
blood glucose monitors or blood pressure monitors,
have shown to become of increasing interest in our
society. The devices enable persons to analyse their
own health status in an independent way.
However, all of these consumer products require
body contact. This can be obstructive for persons
with sensible skin and bears discomfort in wearing.
Moreover, elderly people tend to forget to wear these
devices because of dementia or other cognitive disa-
bilities. In order to overcome these disadvantages, we
propose to extract the vital parameters heart rate, res-
piration rate, oxygen saturation and blood pressure re-
motely in home environments. This vital parameter
data can be recorded and analysed automatically. In
case of emergencies, an alarm can be triggered. More-
over, the continuous monitoring can be a key element
for an improved evidence-based diagnosis.
In this work, we want to outline the state of the
art of remote vital parameter determination and pre-
sent own methods to solve the research tasks. Hereby,
we do not only carry out experiments in laboratory
settings, but especially in realistic home environment
scenarios. The aim is to investigate whether the single
parameters can be measured accurately in the setting
of home environments.
2 REMOTE HEART RATE
DETERMINATION
2.1 Related Work
In the past, a human’s heart rate was obtained by con-
ventional methods such as the electrocardiogram or
the photoplethysmography (PPG), which was propo-
sed by Hertzman and Spealman (Hertzman and Spe-
alman, 1937) and is based on determining the volu-
metric changes in the tissue optically.
By extending the original transmissive approach
of the PPG, it is possible to determine the heart rate
by reflective light (Humphreys et al., 2005). Ver-
kruysse et al. continued with this idea and determi-
908
Wiede, C., Richter, J. and Hirtz, G.
Contact-less Vital Parameter Determination: An e-Health Solution for Elderly Care.
DOI: 10.5220/0007682809080915
In Proceedings of the 14th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2019), pages 908-915
ISBN: 978-989-758-354-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

ned the heart rate in the visible light spectrum by an
RGB-camera (Verkruysse et al., 2008). The first au-
tomated approach in the visible light spectrum was
proposed by Poh et al. (Poh et al., 2010). Further im-
provements consist in using temporal filters (van Gas-
tel et al., 2014), autoregressive models (Tarassenko
et al., 2014) or adaptive filtering (Wiede et al., 2016).
This group of methods are considered as so-called
intensity-based methods.
The other group of methods is called motion-
based methods, because it makes use of small mo-
vements of the head that are caused by the heart bump
induced blood flow according to the the 3
rd
Newto-
nian law. Balakrishnan et al. were the first to apply
this principle (Balakrishnan et al., 2013) by tracking
this motion with optical flow.
Nevertheless, all these methods do not eliminate
the underlying artefacts or are not applicable for home
environments.
2.2 Proposed Method
As outlined in the previous section, eliminating inten-
sity and motion artefacts is the key factor for determi-
ning the heart rate robustly.
In the first step, a white balancing is necessary in
order to compensate the differences in image acquisi-
tion of different cameras. For our implementation, we
use the method presented by Garud et al. (Garud et al.,
2014). In the next step, the face is detected within
the image, because the face has both: A large amount
of skin pixels and a good detectability with standard
algorithms. We apply the face detector of Zhu and
Ramanan (Zhu and Ramanan, 2012), because it not
only provides the location of the image but as well
its orientation based on facial landmarks. Afterwards,
face regions with only skin, no hairs and less mo-
vements artefacts are selected, i. e. the forehead, the
nose and the two cheeks. By transferring all pixels of
these so-called regions of interest (ROI) to the HSV
colour space, it is possible to determine an individual
skin colour model for each person.
In the following, the video sequence can be conti-
nuously captured and the white balancing can be app-
lied to each single image. The face can be tracked by
a mixed approach of KLT tracking (Tomasi and Ka-
nade, 1991) and tracking-by-detection. Subsequently,
all pixels in the face matching the skin colour model
criteria are extracted for the further processing. These
extracted pixels are averaged in every time step for the
three colour channels red, green and blue.
The three colour channels are normalised and
bandpass filtered in order to exclude implausible fre-
quencies. An independent component analysis (ICA)
is applied to split the three filtered channels in one
wanted signal and two noise signals. The result are
three independent components. For each of them, the
periodicity is calculated to determine the wanted sig-
nal component. For this component, the dominant
frequency is computed by the Fast Fourier Transform
(FFT) within a sliding window. This dominant fre-
quency represents the heart rate. In order to prevent
this algorithm from measuring sudden changes in the
heart rate, an adaptive filtering is implemented as low-
pass.
This algorithm shows an averaged root-mean-
square error (RMSE) ranging from 1.19 bumps per
minute (BPM) to 2.93 BPM for selected lab scenarios
(Wiede et al., 2018). These results have to be verified
under realistic conditions in home environments.
2.3 Adjustments for Home
Environment Measurements
Determining the heart rate in home environments
holds some challenges in comparison to the labora-
tory scenarios. Normally, the cameras are fixed at
the ceiling in home environments, so that they do not
disturb the residents. On the one hand, a position at
the ceiling is advantageous because of less occurring
occlusion of objects and persons in the image. On the
other hand, this is accompanied by a perspective vie-
wpoint change, which leads to challenges in detecting
a human’s face. In Figure 1, such an example of per-
spective viewpoint change, with a very steep viewing
angle can been seen.
Moreover, the distance to the camera is higher
than in the lab scenarios. This goes hand in hand with
a smaller spatial resolution, which means that the face
is represented by less pixels. Furthermore, it cannot
be guaranteed that a person is always upright in an
image. Intensity artefacts strongly depend on the cer-
tain lighting in the room and can influence the mea-
surements. In addition to that, motion artefacts occur
during daily routines of the subject. To limit this chal-
lenge, we introduce the condition that measurements
are only valid if the person sits or lies. If a person
walks around, the uncertainty becomes too high, so
that no measurements are taken.
The selection of the lens is crucial at this point.
Whereas a narrow lens has less distortions and a high
spatial resolution, it is necessary to place multiple ca-
meras within one room for observation. In contrast
to that, omnidirectional cameras are equipped with
a fisheye lens, which enables to monitor the whole
room with one camera. But fisheye lenses bear the
problem of radial and tangential distortions. Further-
more, objects and persons are rotated in dependency
Contact-less Vital Parameter Determination: An e-Health Solution for Elderly Care
909
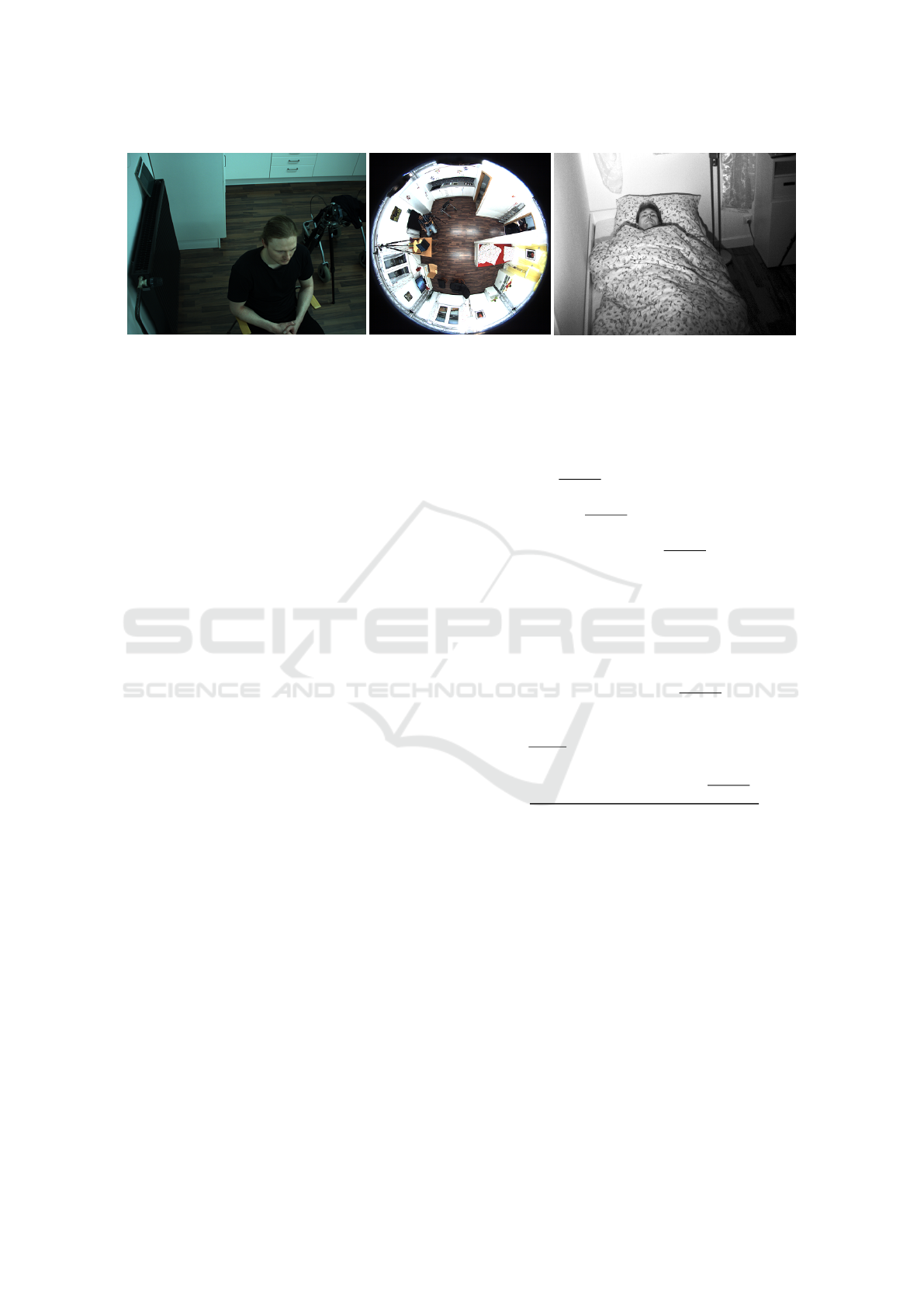
Figure 1: Different scenarios to determine the heart rate in home environments from left to right: Proband sits on a chair
recorded by narrow lens camera, proband sits on a chair recorded by omnidirectional camera, proband lies in a bed recorded
by monochromous camera.
of their position in the room, as can been seen in Fi-
gure 1. In order to overcome these issues and to still
use omnidirectional cameras, we suggest to use a vir-
tual perspective camera such as proposed by Meinel
et al. (Meinel et al., 2014). This has the advantage
that the rest of the algorithm can remain in its original
form.
Another challenge we are facing is darkness such
as in the night. Due to the fact that humans sleep a
considerable time every day, we would loose a lot of
information about vital parameters. In order to over-
come this issue, we propose to perform the measure-
ments in the IR-A light spectrum rather than in the
visual light spectrum. To that goal, external LEDs
in the near infra-red are applied. In Figure 1, such a
monochromous image is shown while a proband lies
in the bed. Furthermore, in the proposed algorithm
we exclude the parts of skin colour determination, the
ICA and the channel selection because we have one
instead of three channels.
2.4 Results and Discussion
In order to evaluate whether the heart rate can be de-
termined in home environments, different measure-
ments were carried out.
Due the fact that the camera position strongly in-
fluences the viewing angle and the lighting conditi-
ons, different scenarios were taken into consideration,
i. e. sitting on a chair or armchair and lying in a bed.
The distance to the subjects varies from 1.5 m up to
4 m. In total, six probands were recruited for these
three scenarios. All videos were recorded in a test flat
at Chemnitz University of Technology to measure un-
der realistic conditions. An Allied G201 RGB camera
with a narrow lens was mounted on the ceiling for
the measurements. For the infra-red measurements,
an Allied Prosilica GM650 monochrome camera with
external LED spotlights was used. Furthermore, the
usage of omnidirectional cameras were evaluated. A
Polar FT1 heart rate monitor was chosen as reference
system. For a quantitative accuracy analysis, the root-
mean-square error (RMSE) is chosen. The RMSE of
different videos of the same scenario can be described
by the mean RMSE.
The results are summarised in Table 1. In the sce-
nario sitting, the RMSE has a value of 1.9 BPM. The
same value is obtained for the scenario lying in the
bed. In the IR-A spectrum an RMSE of 2.6 BPM was
attained for the heart rate determination. This value
is worse in comparison to the value in the visual light
spectrum. The reason for that can be found in the
removal of the skin colour model and the ICA. Ho-
wever, this value is still accurate for the target appli-
cation field. Moreover, it can be shown that a measu-
rement of the heart rate with omnidirectional cameras
is possible, but the value of the RMSE has increased
because of the low spatial resolution.
Table 1: RMSE in BPM for different scenarios in home en-
vironments.
Scenario RMSE
Sitting 1.9
Lying 1.9
Lying (IR-A) 2.6
Omnidirectional camera 3.1
All results clearly indicate that the proposed op-
tical heart rate determination method is suitable for
usage in the field of home environments.
3 REMOTE RESPIRATION RATE
DETERMINATION
3.1 Related Work
A second vital parameter of interest is the respira-
tion rate. Pathological indicators of the respiration
VISAPP 2019 - 14th International Conference on Computer Vision Theory and Applications
910

rate such as breathlessness and hyperventilation can
be symptoms for several diseases. Conventional met-
hods in clinical set-ups are for example respiratory ef-
fort belts, nasal thermistors or pressure transducers.
However, all of these methods do not work contact-
less.
In this work, we want to focus on contact-less met-
hods working in the visible light spectrum. A first
approach was presented by Tan et al., which is based
on edge detection and frame differencing (Tan et al.,
2010). Other approaches make use of autoregressive
models (Tarassenko et al., 2014) or use Eulerian video
magnification (Sharma et al., 2015).
The largest group of methods is based on the prin-
ciples of optical flow. On the basis of works of Na-
kajima et al. (Nakajima et al., 2001) and Frigola et al.
(Frigola et al., 2002), Lukac et al. use a KLT tracking
to determine the optical flow (Lukac et al., 2014).
3.2 Proposed Method
Based on the previous work by Wiede et al. (Wiede
et al., 2017), a new algorithm was developed in the
presented work. Firstly, images is acquired by an
RGB or a monochrome camera. For the proposed al-
gorithm it does not matter whether the images are co-
loured or grey value based, because our method relies
on the lifting and lowering of the torso that is induced
by the breathing.
In order to detect these torso motions, an ROI is
placed in the image on the chest region. To that goal,
we detect the face firstly. In comparison to Wiede
et al. (Wiede et al., 2017), we suggest to use a face
detector using the normalised pixel difference (Liao
et al., 2016), which is by far more accurate. Based
on the face region, we are able to determine the chest
ROI. Subsequently, this ROI is split in four subregions
of equal size.
In the next step, suitable features, in this case mi-
nimum Eigenvalue features (Shi and Tomasi, 1993),
are detected in the subregions. The found feature
points are tracked over time using the optical flow
KLT method (Tomasi and Kanade, 1991). By obser-
ving the averaged motion of the feature points in each
of the subregions, the y-trajectory can be extracted in
a time channel. Only the y-component is considered
in the following because it has the highest contribu-
tion in the breathing motion.
Thereupon, a bandpass filtering is performed to
exclude implausible frequencies. In order to reject
motion artefacts, a PCA is applied to the four filtered
time channels of the subregions. In the following, the
principal component with the highest spectrum den-
sity is considered as the wanted breathing signal. The
final respiration rate is obtained from the dominant
peak in the frequency spectrum computed with the
FFT.
3.3 Adjustments for Home
Environment Measurements
The problems that occur while determining the he-
art rate remotely in home environments (see 2.3) are
the same as for the respiration rate. Especially the
mounting of the camera on the ceiling is challenging
because it influences the detection of the face and
consequently the ROI selection. This issue can be
overcome by using a face detector of Liao et al. (Liao
et al., 2016), which can deal with large perspective
distortions.
Avoiding motion artefacts while determining the
respiration rate is more crucial than for the heart
rate because the respiration rate algorithm is motion-
based. Especially when breathing motion and arbi-
trary motion share the same frequency band, a clear
determination is not always possible. For that reason,
the influence of motion should be evaluated.
The possibilities of using omnidirectional came-
ras for respiration rate determination were investiga-
ted. For that, virtual perspective cameras, such as des-
cribed in Section 2.3, were applied as well. A deter-
mination of the respiration rate during darkness did
not require any changes in the algorithm because the
method is motion-based. To carry out the image pro-
cessing in the IR-A spectrum, only an external illumi-
nation was necessary.
3.4 Results and Discussion
The RMSE is used once more for the quantitative
assessment. For the recordings in the visible light
spectrum, a Basler acA640-100gc industrial camera
and an Allied Prosilica GM650 monochrome camera
in the IR-A spectrum were used. In total, four diffe-
rent scenarios with six probands were recorded in the
test flat of Chemnitz University of Technology. As
described in Section 2.4, we evaluate the scenarios
sitting on chair or armchair, lying in the bed, during
darkness and with an omnidirectional camera.
In order to have a reference for these estimated va-
lues, we developed an own reference system, which
uses a piezo-electric transducer (MLT1132) to gather
information about the chest movement. The data eva-
luation is processed on an STM32F401RE embedded
board. Both the reference measurement and the video
recording are carried out simultaneously.
The results for the home environment measure-
ments are outlined in Table 2. It can been seen that
Contact-less Vital Parameter Determination: An e-Health Solution for Elderly Care
911

the RMSE for sitting and lying is relatively small with
1.8 breaths per minute and 2.0 breaths per minute re-
spectively. The differences might be explained by the
different viewing angles. The RMSE for the IR-A
spectrum is even lower than that. That could be due to
the fact that the proposed method is motion-based and
the probands performed less motion in darkness than
during normal lighting conditions. We expected pro-
blems because of the thick blanket over the torso for
the scenario lying in a bed, but this could not be con-
firmed. The usage of omnidirectional cameras was
also successful for determining the respiration rate re-
motely. We could show that a virtual perspective ca-
mera can compensate the disadvantages of an omni-
rectional camera.
Table 2: RMSE in breaths per minute for different scenarios
in home environments.
Scenario RMSE
Sitting 1.8
Lying 2.0
Lying (IR-A) 1.6
Omnidirectional camera 2.8
Under inclusion of all facts, there is evidence that
the respiration rate can be determined accurately in
home environments.
4 REMOTE OXYGEN
SATURATION
DETERMINATION
4.1 Related Work
The oxygen saturation in a clinical setting can be
obtained by a pulsoximeter. This measurement de-
vice determines the absorption of light emitted by
two LEDs of different wavelength and transmitted
through thin body parts such as fingers or earlobes.
By calculating the so-called ratio-of-ratios at the two
wavelengths 660 nm and 940 nm for the oxygenated
and deoxygenated haemoglobin, the oxygen satura-
tion can be determined.
The basic concept of using one RGB camera to de-
termine the oxygen saturation remotely was presented
by Wieringa et al. (Wieringa et al., 2005). Tarassenko
et al. used this preliminary work to determine the oxy-
gen saturation by taking the red and blue channel of
the camera instead of taking only a small bandwidth
(Tarassenko et al., 2014). Subsequently, the AC- and
DC-parts were determined. Guazzi et al. adapted this
approach and only considered regions in the face that
have a high signal-to-noise ratio (Guazzi et al., 2015).
Alternatively, the oxygen saturation can be determi-
ned by a modulation of the reflected light (de Haan
and Rocque, 2015).
In contrast to that, there exists the possibility to
use two cameras in combination with optical band-
pass filters, such as proposed by Kong et al. (Kong
et al., 2013). This approach has the advantage of a
small bandwidth, but needs to match in both of the
images to analyse the same region. Verkruysse et al.
suggested to choose rather one passband of the band-
pass filters in the infra-red spectrum than in the visible
light (Verkruysse et al., 2017).
Another method is considered as an active appro-
ach because it uses LEDs of different wavelengths to
compute the oxygen saturation (Tsai et al., 2014).
Heretofore, all of the presented methods only ope-
rate under controlled environments in lab settings
with fixed probands that are not moving and an active
lighting.
4.2 Proposed Method
In a first setup, only one camera was used. Based
on the red and the blue channel of a tracked ROI, we
determined the AC- and DC-parts. Subsequently, the
ratio-of-ratio and the oxygen saturation were calcula-
ted. This approach has the disadvantage that the co-
lour channels have a small bandwidth, which leads to
inaccurate results. For that reason, we abandoned the
single camera principle.
Consequently, we developed a concept based on
two cameras. Two monochrome cameras are placed
in a stereo setup with a base distance of 4 cm with
optical bandpass filters. The wavelengths of the op-
tical bandpass filters are 660 nm and 940 nm with a
full width at half maximum of 50 nm. This is a trade-
off between a small bandwidth with a poor brightness
and a large bandwidth, which leads to an inaccurate
calculation of the ratio-of-ratios. The images of both
cameras are recorded simultaneously by means of a
trigger cable.
In our measurements, we had the goal to deter-
mine the oxygen saturation on the arm. To that goal,
at first, a foreground segmentation was carried out to
separate foreground and background. An ROI is pla-
ced in the foreground, i. e. the arm. Subsequently,
minimum Eigenvalue features (Shi and Tomasi, 1993)
are detected and tracked with a KLT-tracker (Tomasi
and Kanade, 1991) in the video sequence. In the next
step, for each corresponding image pair, a feature ma-
tching is carried out. This guarantees that the same
ROI is considered in both images. For both ROIs one
time channel can be extracted by averaging the pixels
VISAPP 2019 - 14th International Conference on Computer Vision Theory and Applications
912

within the ROIs.
By shifting a sliding window over the time chan-
nels, the AC- and DC-parts can be computed. Hereby,
the DC value is equivalent to the mean value within
the sliding window. The gap between minimum and
maximum value in the windows represents the AC va-
lue. The ratio-of-ratio is calculated as follows:
R(φ) =
AC
660nm
(φ)
DC
660nm
(φ)
AC
940nm
(φ)
DC
940nm
(φ)
(1)
Thereby, R denotes the ratio-of-ratios and φ the cur-
rent window. Thereupon, the oxygen saturation SpO
2
can be determined.
SpO
2
= A − B · R (2)
Hereby, A and B stand for the calibration parameters,
which have to be determined during calibration.
4.3 Results and Discussion
In order to evaluate the performance of the proposed
algorithm, videos of five different probands were re-
corded. All probands were healthy and had an oxy-
gen saturation of 98-99 %. Due to the fact, that this
small range is not sufficient to perform a linear ap-
proximation between ratio-of-ratios and oxygen satu-
ration, the probands had to hold their breath, which
results in a decrease of the oxygen saturation down
to 92 % at minimum. A lower value would only be
possible for ill persons with a decreased oxygen satu-
ration.
The measurements were carried out by two Basler
A640gm monochrome cameras with disabled auto-
matic white balance and disabled automatic exposure
time control. As reference system, a Pulox Po200 pul-
soximeter was used during the measurements.
The results indicate that there is a linear depen-
dency between the ratio-of-ratios and the reference
oxygen saturation. However, a robust determination
of the calibration parameters A and B is not possible
for our sequences. There are large individual differen-
ces between the single subjects. Therefore, a usage in
home environments is impossible at the moment, so
that further work has to be carried out.
However, there is a huge potential for using a re-
mote oxygen determination system. Current systems,
such as the pulsoximeter, only provide information
about the oxygen saturation on a certain body part,
e. g. the finger. Under utilisation of an image-based
system, an oxygen saturation map on the skin is fe-
asible. With such a map, it is possible to detect lo-
cal deviations of the oxygen saturation in certain body
parts. That would be a strong indicator for abnorma-
lities and diseases.
5 REMOTE BLOOD PRESSURE
DETERMINATION
5.1 Related Work
Measuring the blood pressure remotely is the most re-
cent research topic in the field of vital parameters and
is based on the methods of remote heart rate deter-
mination. Normally, the blood pressure is measured
by means of a blood pressure cuff. This procedure is
non-invasive but not remote.
Murakami et al. proposed to use the pulse tran-
sit time (PPT) between signals extracted from a hand
and a foot ROI (Murakami et al., 2015). They used
the green channel and filtered this channel to obtain
the PTT. The blood pressure can be determined be-
cause of its linear relationship to the PTT. In a similar
way, Jeong et al. (Jeong and Finkelstein, 2016) and
Secerbegood et al. (Secerbegovic et al., 2016) calcu-
lated the heart rate but used a face and a hand region.
In comparison to that, Sugita et al. suggested to de-
termine the ROIs of the right palm, the forehead and
the left cheek manually and calculate the phase dif-
ference between the two signals by using the Hilbert
transform (Sugita et al., 2015).
Although the related works demonstrated an expe-
rimental feasibility, more work has to be carried out.
5.2 Proposed Method
A direct determination of the blood pressure by me-
ans of the magnitude of the time-varying signal is im-
possible because of the variety of influencing factors,
such as lighting, exposure time, gain factor or indivi-
dual differences of the vessels.
Hence, an indirect method is advantageous. There
is a linear relationship between the blood pressure
(BP) and the pulse wave velocity (PWV). The higher
the PWV, the higher is the blood pressure. This can
be modelled by the following equation:
BP = a · PWV + b (3)
Hereby, a and b denote individual factors, which
have to determined by calibration. The PWV can be
obtained by measuring the time t
Arm
that a pulse wave
needs to pass the distance s
Arm
between two known
ROIs.
In order to obtain the PWV, the ROIs have to be
determined on the arm. Furthermore, the distance bet-
Contact-less Vital Parameter Determination: An e-Health Solution for Elderly Care
913

ween the two ROIs has to be measured. Currently, this
is done manually but should be automatised in future.
For the detection and tracking of features, we use mi-
nimum Eigenvalue features and a KLT tracking. This
is done to reduce the influence of motion artefacts.
A time signal is extracted within a single ROI by
averaging all its pixel. By detecting identical peaks
of the two regions, the transit time can be calculated.
Hereby, the frame rate has to be high enough to detect
the peaks and to determine the time difference accu-
rately.
5.3 Results and Discussion
For the evaluation, the probands have to sit still and
should not move. A Basler acA640-100gc RGB ca-
mera is placed in 0.5 m distance to the subject’s right
arm. The frame rate is fixed to 50 frames per second.
For reference measurements, a boso medicus X
blood pressure cuff is used. Due to the fact that a me-
asurement with the reference system will influence a
camera based system, a synchronous measurement is
not sensible. Therefore, the blood pressure is deter-
mined with the reference system directly before and
after the image recording. If both values do not vary
too much, the recording is considered as relevant. Ot-
herwise, it is rejected. The probands had to rest at
least 10 min before the measurement starts to guaran-
tee a stable blood pressure.
First measurements in the lab proved the linear
correlation between blood pressure and PWV. Howe-
ver, more work has to be carried out to reduce the
influence of individual differences. An utilisation in
home environments is not given at the moment.
Nevertheless, this image-based method has some
advantages in comparison to the conventional met-
hod. For patients who have to measure their blood
pressure regularly (e. g. automatic measurement
every 15 or 30 min), a contact-less method provi-
des considerably more comfort. Furthermore, from
a medical point of view it is relevant, to determine the
blood pressure on different body parts and not only on
one arm. If the PWV is smaller only in one limb, this
can be an indicator for peripheral arterial diseases.
6 CONCLUSIONS
In our work we evaluated the vital parameters he-
art rate, respiration rate, oxygen saturation and blood
pressure concerning their remote, image-based deter-
mination in home environments. The results are sum-
marised in Table 3. The heart rate and the respira-
tion rate can be determined accurately and can be de-
ployed in the field of home environments. The met-
hods to determine the oxygen saturation and the blood
pressure have to be made more robust before evalua-
ting them in real world scenarios.
Table 3: Availability of remote vital parameter determina-
tion in home environments.
Vital parameter Availability
Heart rate Ready for usage in the field
Respiration rate Ready for usage in the field
Oxygen saturation Improvements necessary
Blood pressure Improvements necessary
Next to the field of home environments, remote vi-
tal parameter determination can be beneficial in other
fields as well. Possible application fields are the pre-
vention of sudden infant death syndrome, sleep mo-
nitoring, monitoring of a driver’s well being, monito-
ring of training in rehabilitation centres and triage in
hospitals.
REFERENCES
Balakrishnan, G., Durand, F., and Guttag, J. (2013). De-
tecting Pulse from Head Motions in Video. In Com-
puter Vision and Pattern Recognition (CVPR), 2013
IEEE Conference on, pages 3430–3437.
Berger, R., Kaltenbach, T., B
¨
osch, L., Erharter, M., Fath, S.,
Hosseini, M., and Magunia, P. (2016). Digital and dis-
rupted: All change for healthcare. Think Act, page 16.
de Haan, G. and Rocque, M. (2015). Device, system and
method for determining the concentration of a sub-
stance in the blood of a subject. US Patent App.
14/941,934.
Frigola, M., Amat, J., and Pags, J. (2002). Vision based
respiratory monitoring system. In Proceedings of the
10th Mediterranean Conference on Control and Auto-
mationMED2002 Lisbon, Portugal.
Garud, H., Ray, A. K., Mahadevappa, M., Chatterjee, J., and
Mandal, S. (2014). A fast auto white balance scheme
for digital pathology. In 2014 IEEE-EMBS Internati-
onal Conference on Biomedical and Health Informa-
tics, BHI 2014, pages 153–156.
Guazzi, A. R., Villarroel, M., Jorge, J., Daly, J., Frise,
M. C., Robbins, P. A., and Tarassenko, L. (2015).
Non-contact measurement of oxygen saturation with
an rgb camera. Biomedical optics express, 6(9):3320–
3338.
Hertzman, A. B. and Spealman, C. R. (1937). Observations
on the finger volume pulse recorded photoelectrically.
American Journal of Physiology, 119:334–335.
Humphreys, K., Markham, C., and Ward, T. (2005). A
CMOS camera-based system for clinical photoplet-
hysmographic applications. In Proceedings of SPIE,
volume 5823, pages 88–95.
VISAPP 2019 - 14th International Conference on Computer Vision Theory and Applications
914

Jeong, I. C. and Finkelstein, J. (2016). Introducing con-
tactless blood pressure assessment using a high speed
video camera. Journal of Medical Systems, 40(4):77.
Kong, L., Zhao, Y., Dong, L., Jian, Y., Jin, X., Li, B., Feng,
Y., Liu, M., Liu, X., and Wu, H. (2013). Non-contact
detection of oxygen saturation based on visible light
imaging device using ambient light. Optics express,
21(15):17464–17471.
Liao, S., Jain, A. K., and Li, S. Z. (2016). A Fast and Accu-
rate Unconstrained Face Detector. IEEE Transacti-
ons on Pattern Analysis and Machine Intelligence,
38(2):211–223.
Lukac, T., Pucik, J., and Chrenko, L. (2014). Contactless
recognition of respiration phases using web camera.
In Radioelektronika (RADIOELEKTRONIKA), 2014
24th International Conference, pages 1–4. IEEE.
Meinel, L., Wiede, C., Findeisen, M., Apitzsch, A., and
Hirtz, G. (2014). Virtual perspective views for real-
time people detection using an omnidirectional ca-
mera. In Imaging Systems and Techniques (IST), 2014
IEEE International Conference on, pages 312–315.
IEEE.
Murakami, K., Yoshioka, M., and Ozawa, J. (2015). Non-
contact pulse transit time measurement using imaging
camera, and its relation to blood pressure. In 2015
14th IAPR International Conference on Machine Vi-
sion Applications (MVA), pages 414–417.
Nakajima, K., Matsumoto, Y., and Tamura, T. (2001). Deve-
lopment of real-time image sequence analysis for eva-
luating posture change and respiratory rate of a subject
in bed. Physiological Measurement, 22:N21.
Poh, M.-Z., McDuff, D., and Picard, R. (2010). Non-
contact, automated cardiac pulse measurements using
video imaging and blind source separation. Optics Ex-
press, 18(10):10762–10774.
Secerbegovic, A., Bergsland, J., Halvorsen, P., Suljanovic,
N., Mujcic, A., and Balasingham, I. (2016). Blood
pressure estimation using video plethysmography. In
2016 IEEE 13th International Symposium on Biome-
dical Imagin), pages 461–464.
Sharma, S., Bhattacharyya, S., Mukherjee, J., Purkait, P. K.,
Biswas, A., and Deb, A. K. (2015). Automated de-
tection of newborn sleep apnea using video moni-
toring system. In Advances in Pattern Recognition
(ICAPR), 2015 Eighth International Conference on,
pages 1–6. IEEE.
Shi, J. and Tomasi, C. (1993). Good Features to Track.
Technical report, Cornell University, Ithaca, NY,
USA.
Sugita, N., Obara, K., Yoshizawa, M., Abe, M., Tanaka, A.,
and Homma, N. (2015). Techniques for estimating
blood pressure variation using video images. In 2015
37th Annual International Conference of the IEEE En-
gineering in Medicine and Biology Society (EMBC),
pages 4218–4221.
Tan, K. S., Saatchi, R., Elphick, H., and Burke, D. (2010).
Real-time vision based respiration monitoring system.
In Communication Systems Networks and Digital Sig-
nal Processing (CSNDSP), 2010 7th International
Symposium on, pages 770–774. IEEE.
Tarassenko, L., Villarroel, M., Guazzi, A., Jorge, J., Clif-
ton, D. A., and Pugh, C. (2014). Non-contact video-
based vital sign monitoring using ambient light and
auto-regressive models. Physiological Measurement,
35(5):807–831.
Tomasi, C. and Kanade, T. (1991). Detection and Tracking
of Point Features. Technical report, Carnegie Mellon
University.
Tsai, H.-Y., Huang, K.-C., Chang, H.-C., Yeh, J.-L. A.,
and Chang, C.-H. (2014). A noncontact skin oxygen-
saturation imaging system for measuring human tissue
oxygen saturation. IEEE Transactions on Instrumen-
tation and Measurement, 63(11):2620–2631.
van Gastel, M., Zinger, S., Kemps, H., and de With, P.
(2014). e-health video system for performance ana-
lysis in heart revalidation cycling. In Consumer Elec-
tronics Berlin (ICCE-Berlin), 2014 IEEE Fourth In-
ternational Conference on, pages 31–35.
Verkruysse, W., Bartula, M., Bresch, E., Rocque, M., Mef-
tah, M., and Kirenko, I. (2017). Calibration of con-
tactless pulse oximetry. Anesthesia and analgesia,
124(1):136–145.
Verkruysse, W., Svaasand, L. O., and Nelson, J. S. (2008).
Remote plethysmographic imaging using ambient
light. Optics Express, 16(26):21434–21445.
Wiede, C., Richter, J., Apitzsch, A., KhairAldin, F., and
Hirtz, G. (2016). Remote Heart Rate Determination
in RGB Data. In Proceedings of the 5th International
Conference on Pattern Recognition Applications and
Methods, pages 240–246.
Wiede, C., Richter, J., Manuel, M., and Hirtz, G. (2017).
Remote respiration rate determination in video data
- vital parameter extraction based on optical flow
and principal component analysis. In Proceedings of
the 12th International Joint Conference on Compu-
ter Vision, Imaging and Computer Graphics Theory
and Applications - Volume 4: VISAPP, (VISIGRAPP
2017), pages 326–333. INSTICC, SciTePress.
Wiede, C., Sun, J., Richter, J., and Hirtz, G. (2018). Robust
remote heart rate determination for e-rehabilitation -
a method that overcomes motion and intensity arte-
facts. In Proceedings of the 13th International Joint
Conference on Computer Vision, Imaging and Com-
puter Graphics Theory and Applications - Volume 4:
VISAPP,, pages 491–500. INSTICC, SciTePress.
Wieringa, F. P., Mastik, F., and van der Steen, A. F.
(2005). Contactless multiple wavelength photoplet-
hysmographic imaging: a first step toward spo2 ca-
mera technology. Annals of biomedical engineering,
33(8):1034–1041.
Zhu, X. and Ramanan, D. (2012). Face detection, pose esti-
mation, and landmark localization in the wild. In Pro-
ceedings of the IEEE Computer Society Conference
on Computer Vision and Pattern Recognition, pages
2879–2886.
Contact-less Vital Parameter Determination: An e-Health Solution for Elderly Care
915
