
Development of Diagnostic Skills in Dentistry Students using Gamified
Virtual Patients
Sneyder J. Sanchez M.
1
, Juan E. G
´
omez-Morantes
1,∗
, Carlos Parra
1
, Angela Carrillo-Ramos
1
, Adriana
I. Camacho
2
and Gloria C. Moreno
2
1
Systems Engineering Department, Pontificia Universidad Javeriana, Bogot
´
a, Colombia
2
Dental System Department, Pontificia Universidad Javeriana, Bogot
´
a, Colombia
{camacho-adriana, gcmoreno}@javeriana.edu.co
Keywords:
Virtual Patients, Serious Games, Dentistry Education, Endodontics, Diagnostic Skills.
Abstract:
The use of serious games, virtual patients, and other forms of digital learning technologies are starting to
emerge in dentistry schools around the world. However, because of their novelty, there is still a need for lit-
erature discussing the different challenges of computer-supported education in this field. This paper presents
the design, development, and pilot validation of a serious game for the development of diagnostic skills in
dentistry students. Called RealTeeth, this game puts the student in a job interview context and asks him to
diagnose 10 endondontic cases. Each case allows the student to follow 5 different diagnostic routes with dif-
ferent information and resources. At the end of the 10 cases, the student will receive a job offer in accordance
with his or her performance on the cases. This game was tested with a cohort of student of the pre-clinic course
of endodontics in the Pontificia Universidad Javeriana in Bogot
´
a, Colombia. The results of this pilot valida-
tion were positive in terms of user acceptance and attitude, reinforcing the potential of computer supported
education in the field of dentistry.
1 INTRODUCTION
Endodontics is a dentistry specialty that focuses on
the study of dental pulp and dental pulp diseases.
In the case of the Pontificia Universidad Javeri-
ana, endodontics is taught as part of the dentistry un-
dergraduate program with two obligatory pre-clinic
courses
1
and one emphasis course
2
. The two pre-
clinic courses are seen in the third year of the five-
year dentistry program, while the emphasis course is
seen in the fourth or fifth year of the program.
The three endodontics courses are structured fol-
lowing Miller’s pyramid (see Figure 1). The first
course is dedicated to what Miller calls knowledge
assessment, understood as “some assurance that a stu-
dent, a resident, a physician knows what is required in
order to carry out those professional functions effec-
∗
Corresponding author.
1
Pre-clinic courses are those that the student have to
complete before his or her clinic internship
2
Emphasis courses are optional courses that deal with
advance topics on the different disciplines of dentistry. Stu-
dents can select emphasis courses according to their per-
sonal o professional interests.
tively” (Miller, 1990, p. S63, emphasis in original).
For endodontics this includes all the knowledge re-
lated to tooth and dental pulp anatomy, endodontics
conditions (the 11 basic diagnosis
3
), the signs of the
11 basic diagnosis, and the tests needed to reach any
of the 11 diagnosis.
The second course is aimed at the competence as-
sessment level of Miller’s pyramid, defined as the one
that evaluates that “graduates must also know how to
use the knowledge they have accumulated” (Miller,
1990, p. S63, emphasis in original), and is devoted to
semiotic competences.
Semiotic competences are related to interpretation
of data and symbols, which, in the case of endodon-
tics, are related to communicating with patients and
interpreting the data provided by them. These semi-
otic competences are intimately related to diagnostic
skills and include, “among other things, the skill of
3
There are 11 basic diagnosis in endodontics, which are
covered in the first pre-clinic course. However, there are
other conditions that could include endodiotic signs or dis-
eases. For example, a periodontic condition could result in
an endodontic disease. Those associated conditions are not
covered in the first pre-clinic course nor in RealTeeth.
124
M., S., Gómez-Morantes, J., Parra, C., Carrillo-Ramos, A., Camacho, A. and Moreno, G.
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients.
DOI: 10.5220/0007708001240133
In Proceedings of the 11th International Conference on Computer Supported Education (CSEDU 2019), pages 124-133
ISBN: 978-989-758-367-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Knowledge
Competence
Performance
Action
Figure 1: Miller’s pyramid: Framework for clinical assess-
ment. Adapted from (Miller, 1990).
acquiring information from a variety of human and
laboratory sources, to analyze and interpret these data,
and finally to translate such findings into a rational di-
agnostic or management plan” (Miller, 1990, p. S63).
Finally, the third course is an elective course with
advanced semiotic and clinical competences for stu-
dents with a special interest in endodontics.
Students start their clinic internship to put in prac-
tice and further develop the knowledge and skills ac-
quired in the pre-clinic courses. Since this is where
they put their skills into practice and get access to real
patients, this is where performance and action assess-
ment takes place (Miller, 1990).
This teaching structure, based on a pre-clinic com-
ponent and a clinic internship, is commonplace in
medical education (Miller, 1990; Brailovsky et al.,
2001; Brailovsky, 2001). However, climbing Miller’s
pyramid is a considerable challenge. In the assess-
ment front, there is a tendency to believe that knowl-
edge should be the core of medical education assess-
ment. As Miller says, “there are many who appear to
believe that this knowledge base is all that needs to be
measured” (Miller, 1990, p. S63, emphasis in origi-
nal). This view could be attributed to the difficulties
of assessments at the competence or performance lev-
els without including real patients.
The training front faces similar challenges. Since
the development of real-life skills is difficult from
a classroom, most teaching efforts are geared to-
wards the knowledge level of Miller’s pyramid. How-
ever, since knowledge does not necessarily translate
to skill, competence and skill building remains elu-
sive. Some teaching methods like problem-based
learning have been explored as a possible solution
for this issue, but they have shown mixed results at
the pre-clinic level (Hartling et al., 2010). More re-
cently, and due to moderm technological advance-
ments included in medical education, simulation el-
ements have been introduced as a way to facilitate
the competence building process and its assessment
(Gaba, 2004; Issenberg et al., 2005).
It is clear, then, that new skill and competence
building methods should be explored in pre-clinic
endodontics education to avoid the shortfalls of a
knowledge-centric medical education. With that in
mind, this research proposes a simulation approach
materialized in a serious game in which pre-clinic stu-
dents have to act as dentists for virtual patients and
reach an adequate diagnosis. The objective behind
this technology introduction is twofold; first, there is
the objective of providing a tool for students to ex-
ercise and develop their diagnostic skills. Second, it
can be used to asses the knowledge and competence
levels of Miller’s pyramid.
This paper starts with a brief overview of the rel-
evant literature in section 2. The methodology fol-
lowed in this research is presented in section 3. Af-
terwards, section 4 presents more details about Real-
Teeth and the pilot validation performed during this
research. Finally, the paper concludes in section 5
with a discussion about the lessons learned during this
project and outlines a research agenda based on these
lessons.
2 RELATED WORK
Computer supported education is a strong trend that
has permeated more and more disciplines as time goes
by. Endodontics, or dentistry at a more general level,
is no stranger to this trend and there is already a strong
body of work exploring the intersection between dig-
ital technologies and dentistry education. The cur-
rent literature in this domain can be classified in three
groups; the adoption of digital technologies among
dentistry students, teachers, or schools; the use of dig-
ital technologies as an educational tool; and the edu-
cation and training in digital technologies specific to
the dentistry profession.
The literature on adoption of digital technologies
among students, teachers, or schools follows a tra-
ditional adoption studies approach to evaluate ac-
ceptance, adoption factors, or likelihood of adop-
tion of digital technologies among the aforemen-
tioned groups. In general, there seems to be an ad-
equate set of adoption factors like previous experi-
ence with digital technologies (e.g. the Internet, smart
phones, personal computers) by students and teaches
(L
´
opez Jordi et al., 2016; Mari
˜
no et al., 2012), and
positive attitudes towards the use of digital technolo-
gies as a teaching aid (L
´
opez Jordi et al., 2016; Mc-
Cann et al., 2010; Ren et al., 2017; Amer et al., 2011).
However, there are warnings against purely virtual
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients
125

models. In this sense, (McCann et al., 2010) indi-
cates that most students see digital learning tools as
complements to face-to-face teaching rather than a re-
placement. This is consistent with the work of (Reiss-
mann et al., 2015) that demonstrates a high accep-
tance of blended models and the use of digital learn-
ing tools by dentistry students.
There are, however, few studies that focuses ex-
plicitly on the adoption rate of digital learning tools
among dentistry schools. This is a big gap in the liter-
ature because, as (Ren et al., 2017) shows, acceptance
and intention to adopt does not necessarily lead to ac-
tual adoption of digital technologies in the classroom.
The literature on the actual use of digital learning
tools in dentistry education is more diverse, covering
the development of virtual patients or serious gam-
ing for dentistry students, the development of learn-
ing platforms (Bravo-Torres et al., 2017; MacPherson
and Brueckner, 2003), and the evaluation of impact of
digital learning tools in the performance of dentistry
students.
Serious games for education, or game-based
learning (GBL), is a popular subject in computer-
supported education literature. At its core, serious
games explores the use of game technologies or me-
chanics in education applications. In this sense, and
because of the interactive nature of games, it lends
itself to support problem-based, inquiry based or
learning-by-doing methodologies (Shih et al., 2010).
In terms of technologies, virtual reality, mobile or
ubiquitous computing, digital social networks, and
adaptive systems are among the most common tech-
nologies used in the development of GBL systems
(Shih et al., 2010). Virtual reality and human-
computer interaction technologies allow for the de-
velopment of 3D systems that could be manipulated
by traditional means (keyboard and mouse peripher-
als) or more sophisticated means like Nintendo Wii
remotes, Microsoft Kinect sensors, or wired gloves.
In this sense, virtual reality in GBL could lead to an
immersive experience for students. Mobile an ubiqui-
tous technologies could be used to support location-
based learning (e.g. field works or explorations) and
uses GPS information to create an augmented reality
experience for students. Digital social networks can
be used to implement social-heavy GBL systems or
to integrate social features in other GBL tools. Fi-
nally, adaptive systems can be used in conjunction
with other technologies to create GBL tools that adapt
to different aspects of the use like preferences, learn-
ing pace, learning styles, among others.
The development of virtual patients, usually ac-
companied by gamification elements, is the most
common for of game-based learning in the field of
dentistry and is a popular theme in this literature
(Antoniou et al., 2014; Sipiyaruk et al., 2017; Van-
naprathip et al., 2016). However, as pointed out in
(Sipiyaruk et al., 2017), serious games have some lim-
itations and teachers should be cautious about the mix
up of education and gaming objectives by students.
The impact of these digital learning tools on the
performance of dentistry students has been studied
with some detail, but no consensus has been reached
in this regard. While some studies suggest a positive
impact (Busanello et al., 2015; Ratka-Kr
¨
uger et al.,
2018), other found no statistically significant impact
when comparing traditional teaching techniques with
new computer-supported teaching techniques (Amer
et al., 2011). Indirect measures of the effectiveness
of digital learning tools can also be found in the lit-
erature. One example is the work of (Jackson et al.,
2018) studying the usage patterns of self-directed dig-
ital learning tools and finding a strong tendency to-
wards heavy usage in the days leading up to examina-
tions. Given that the heavy lifting of preparation for
examinations is usually left for 2 or 3 days before the
exam, the fact that students invest such valuable time
in digital learning tools is an indicator of their value.
This discrepancy could be explained, in part, by
exploring the adequacy of digital learning tools in dif-
ferent education levels. In this sense, (Browne et al.,
2004) found that face-to-face interaction was more ef-
fective for inexperienced learners (e.g. undergrad stu-
dents), while e-learning was more effective for expe-
rienced learners (e.g. professional dentists enrolled in
a continuous professional development program).
Finally, the literature on education and training
in digital technologies specific to the dentistry pro-
fession explores the transition towards a professional
practice with increasing number of digital compo-
nents and tools (Afshari et al., 2017), and the chal-
lenges of training dentistry students in techniques
such as CAD/CAM technologies, digital radiography,
or digital microscopy (Afshari et al., 2017; Brown-
stein et al., 2015; Farah and Maybury, 2009).
The literature reviewed in this section demon-
strates 3 main things; the adequacy of computer sup-
ported teaching methods in dentistry, the predomi-
nance of blended models over purely virtual models,
and the challenges and risks of the implementation of
digital learning tools in dentistry curricula. Of partic-
ular importance for this project, this literature shows
the importance of keeping a balance between gami-
fication and pedagogical elements in serious games,
and the importance of truly integrating digital learn-
ing tools as complements to face-to-face teaching.
CSEDU 2019 - 11th International Conference on Computer Supported Education
126

3 METHODOLOGY
The methodology followed in this research had three
main phases; a learning styles diagnosis, a scenario
design, and the development of the RealTeeth online
game. Finally, a pilot validation with a cohort of pre-
clinic students was performed.
In order to determine the best kind of content to
include in the simulations, a learning styles diagnosis
among pre-clinic endodontics students was performed
based on the visual, auditory, and kinaesthetic (VAK)
learning styles (Bandler and Grinder, 1990). A ques-
tionnaire with 40 closed-answer questions
4
was dis-
tributed in a cohort of pre-clinic endodontics students,
obtaining 32 fully answered questionnaires. The re-
sults of these questionnaires indicated that most stu-
dents were predominantly kinaesthetic (42%) or vi-
sual (39%) learners, while only 19% were predomi-
nantly auditory learners.
The main objective of this assessment was to pri-
oritize the time and resources devoted to the different
kinds of materials that could be included in this type
of simulations. With that in mind, and considering
that only 19% of students are predominantly auditory
learners, no auditory elements will be included in the
simulation. Visual learners, on the other hand, rep-
resent 39% of students. Hence, the simulation will
be rich in visual aids like x-rays and photos from
real cases to guide the user experience. Kinaesthetic
learners are a challenge because kinaesthetic learn-
ing implies movement and usage of tools. However,
since this project is focused on semiological compe-
tences, which have little intersection with movement
in the case of endodontics, no real kinaesthetic ele-
ments will be included in the simulation.
The scenario design phase focused on the design
of user experience and the learning experience for the
students. This included a case model, an evaluation
model, and a gamification context design. This was
done in conjunction with the current teachers of the
pre-clinic endodontics courses. These designs were
later used for the development of RealTeeth, which
was done following a Scrum software development
lifecycle to allow for constant validation and feedback
from the endodontics teaching team. For a pilot vali-
dation, RealTeeth was then deployed and tested with
a cohort of 19 dentistry students and 3 domain expert
(see Figure 2).
Since this paper reports only on the initial devel-
opment of RealTeeth, the results from the pilot valida-
tion phase are commented in section 4.3, but haven’t
been included nor implemented at the time of writing.
4
The questionnaire was taken from (De la Parra Paz,
2004, p. 85)
Figure 2: Pilot test of RealTeeth.
4 REALTEETH
RealTeeth could be described as a patient simulator
that was designed and developed as an answer to the
challenges for endodontics education in the Pontificia
Universidad Javeriana (see section 1). It covers the
two pre-clinic courses and the elective course; and
contributes to the knowledge, competence, and per-
formance levels of Miller’s pyramid. Furthermore, it
includes gamification elements to facilitate and stim-
ulate usage and learning from endodontics students.
To facilitate it’s deployment and usage, it is built as a
web application.
RealTeeth puts the student in the place of a newly
graduated dentist looking for a job position at a big
dentistry practice. In order to get the job, the student
has to show his or her endodontics skills by diagnos-
ing 10 patients (see Figure 3). Once the 10 virtual
patients are diagnosed, the student will be classified
in a basic-intermediate-advanced scale. Students with
an advanced classification will be offered the position
of Chief Endodontist. Students with an intermediate
classification will be offered the position of Junior En-
dodontist. Finally, students with a basic classification
will see their job application rejected.
Every student starts at a basic level and will be
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients
127
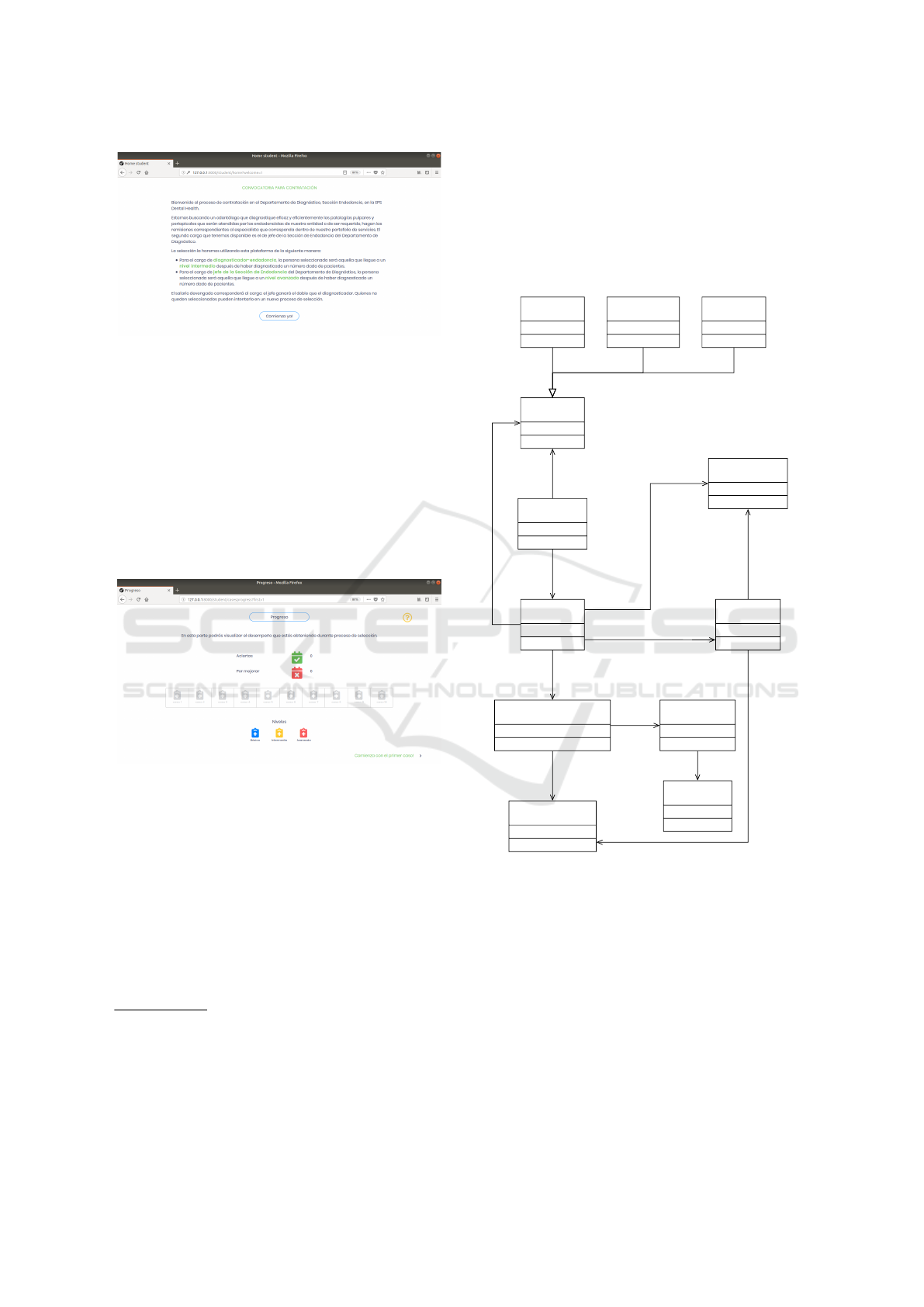
Figure 3: RealTeeth welcome screen for students.
presented with basic-level cases until he or she ad-
vances to the intermediate level. In order to do this,
the student has to get three consecutive basic-level
cases right. Once this happens, the student will be
presented with intermediate-level cases. If the student
is capable of getting three consecutive intermediate-
level cases right, he or she will move to the advanced
level and will be presented with advanced-level cases
(see Figure 4). The student will be demoted to the
previous level if he or she fails a case.
Figure 4: RealTeeth dashboard screen for students.
The cases are structured around the standard diag-
nosis protocol in endodontics (see Figure 5). Cases
have 5 possible diagnostic routes; pain assessment,
clinical exam, periapical tests, sensibility tests, and
x-rays. The student can choose any of the 5 diagnos-
tic routes to start his diagnosis. Each diagnostic route
will give different information, and some of them (e.g.
x-rays or clinical exam) will show images or photos
(see Figure 6). Additionally, each diagnostic routes
allow the student to ask questions and RealTeeth will
provide answers
5
. At the end of a diagnostic route the
5
The nature of the questions and answers depends on
the nature of the diagnostic route. The clinical exam, for
example allows the student to ask additional questions to
the patient and RealTeeth will show the answer given by
the patient. X-rays, on the other hand, allow the student to
ask questions about the x-ray and RealTeeth will provide
expert answers.
student has to reach a conclusion based only on the
information provided by the route (see Figure 7). Af-
ter completing the 5 diagnostic routes the student can
finally provide a diagnosis (see Figure 8). Based on
the conclusions of the 5 diagnostic routes and the fi-
nal diagnosis, the case is evaluated using a rubric and
provides feedback to the student (see Figure 9).
has a
has a
answers
10
offers
5
1..*
reaches a
reaches a
evaluated by
considers
considers
Case
Diagnostic route Question
Student
Level
High Medium Basic
Answer
Rubric
Conclusion
Diagnosis
Figure 5: Case model.
The use protocol is as follows (see Figure 10).
The student starts by seeing an introductory screen ex-
plaining the rules of the game. The student then starts
with the first case in basic level. A case introduction
is shown at the beginning of each case with informa-
tion regarding the reason for consultation given by the
patient. Later, the student can choose one of the five
diagnostic routes and follow it until a conclusion is
reached on that route. When the student completes
the 5 routes, a diagnosis must be given. The case will
be evaluated using a pre-defined rubric and the stu-
dent will be informed if the case was passed or not.
Based on previous performance, the student will be
CSEDU 2019 - 11th International Conference on Computer Supported Education
128

Figure 6: Main screen of the x-ray examination diagnostic
route.
Figure 7: Analysis screen of the x-ray examination diagnos-
tic route.
promoted or demoted. This process will be repeated
until the student completes 10 cases. Once this hap-
pens, the result of the game session will be shown to
the student.
The interaction between the student and RealTeeth
throughout this process is form-based and gives a
great deal of control to the student. In this sense, the
student can choose where to start (i.e. the order of the
diagnostic routes) and the order in which to ask ques-
tions to the system. The student can also go back to
previous diagnostic routes to double check informa-
tion or change his or her diagnostic. After the final
diagnosis is made, the student is shown if this diag-
nosis is correct or not. Additionally, the details of
the evaluation (i.e. the full rubrics for every diagnos-
tic route) is shown (see figure 9) in order to allow the
student to analyze his or her performance and identify
any weaknesses that should be addressed.
4.1 Case Design and Teacher-oriented
Features
This initial version of RealTeeth offers 4 features for
teachers: case creation, case editing, case search, and
case removal.
The case creation feature allows teachers to create
a complete case, including case description, basic in-
formation for the 5 diagnostic routes, uploading of x-
rays and other images used in the case, the questions
and answers of each diagnostic route, the conclusions
for each diagnostic route, the right diagnosis for the
case, and the evaluation rubric.
The case editing feature allows teachers to modify
the information and structure of a pre-defined case.
This was proven to be of key importance during our
pilot validation of RealTeeth since even though the
cases were designed by experts on the field, some mi-
nor errors where discovered in the cases. These errors
where detected when too many students were fail-
ing the same case, when students capable of reaching
an advanced level were consistently failing the same
lower-level case, or when differences of opinion about
a case level arouse among the teaching team.
The case search feature allow teachers to find
cases based on the difficulty level.
Finally, the case removal feature allow teachers to
delete one or multiple cases.
4.2 System Architecture
RealTeeth was developed using a traditional web-
oriented architecture following the Model-View-
Controler (MVC) pattern. The backend was devel-
oped in PHP using the Symfony 2.7 framework. The
frontend was developed using Javascript, HTML 5
and CSS 3. Finally, MySQL was used as DBMS. The
system was deployed using Amazon Web Services.
Specifically, AWS EC2 was used to host RealTeeth,
and AWS RDS was used to handle the database (see
Figure 11). It is important to note, however, that Real-
Teeth can be deployed in any linux-based server with
Apache Web Server, PHP, and MySQL installed.
4.3 Pilot Validation
Two kinds of tests were done in RealTeeth: functional
testing and usability testing.
The functional testing was done using the
PHPUnit testing framework and following the Clean
Code (Martin, 2009) and SOLID principles (Arora,
2017). Additionally, RealTeeth has been tested in
the latest versions (at the time of writing) of Google
Chrome, Mozilla Firefox, and Safari web browsers.
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients
129
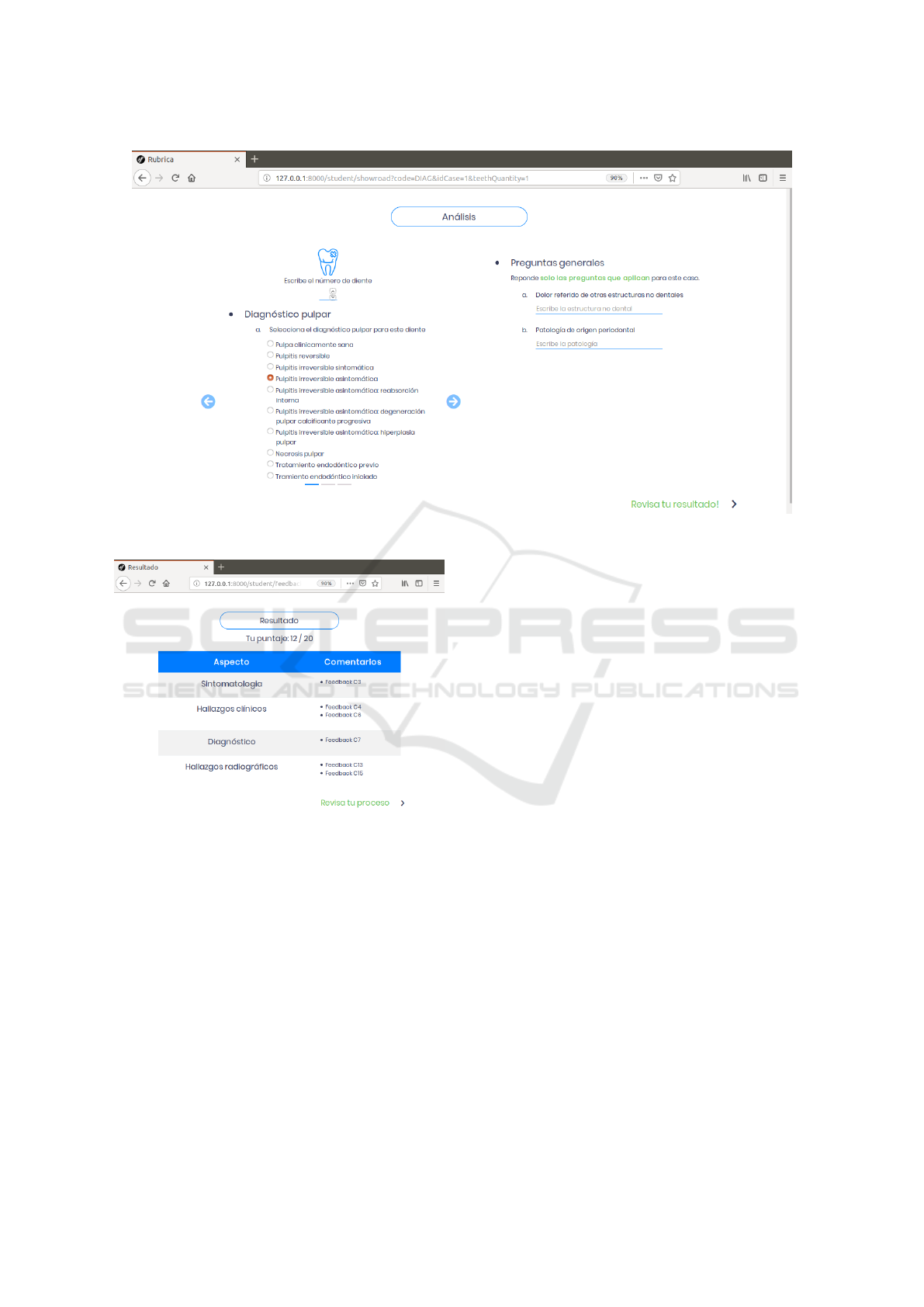
Figure 8: Case diagnosis screen.
Figure 9: Results and feedback screen.
The usability test was done using a survey handed
to the 19 students that participated in the pilot test
of RealTeeth. This usability test evaluates the effec-
tiveness, efficiency, and user satisfaction of RealTeeth
following the ISO 9241-11 and ISO/IEC 9126-4 stan-
dards. The main results from this usability test are
that the gamification elements included in RealTeeth
were well understood and accepted by the students.
However, a general comment was that these gamifica-
tion elements should be further developed to increase
the motivation of the student. Some ideas gathered
in the questionnaire included stating different salaries
for the different job positions offered at the beginning
of the game, or including different perks associated
with each job position. This highlights the importance
of gamification to ensure user engagement in digital
learning tools.
Regardless of some user interface problems (e.g.
button placement, text size and fonts, confusing nav-
igation at especific points, etc.), the pilot validation
could be considered a success. Furthermore, and re-
gardless of these navigation issues, the students seem
very satisfied with RealTeeth, with 100% stating that
the information provided in RealTeeth was close to
real-life cases and 81% stating that they would like to
use RealTeeth frequently. Finally, some of the com-
ments made by the students include “this is something
new in pre-clinic and would be interesting to use it
during the semester”, “this was an interesting exer-
cise and we’ve never done anything like this before”,
and “this helps to close the gap between theory and
practice”. This shows that RealTeeth was capable of
fulfilling the objective highlighted in section 1.
5 LESSONS LEARNED AND
FUTURE WORK
The pilot validation of RealTeeth suggests that it has
high acceptance levels from both students and fac-
ulty. Additionally, there seems to be a high percep-
tion of usefulness coming from students and faculty.
But regardless of this positive attitude towards Real-
Teeth, or digital learning tools in general, this expe-
rience yielded valuable lessons for future versions of
RealTeeth.
CSEDU 2019 - 11th International Conference on Computer Supported Education
130
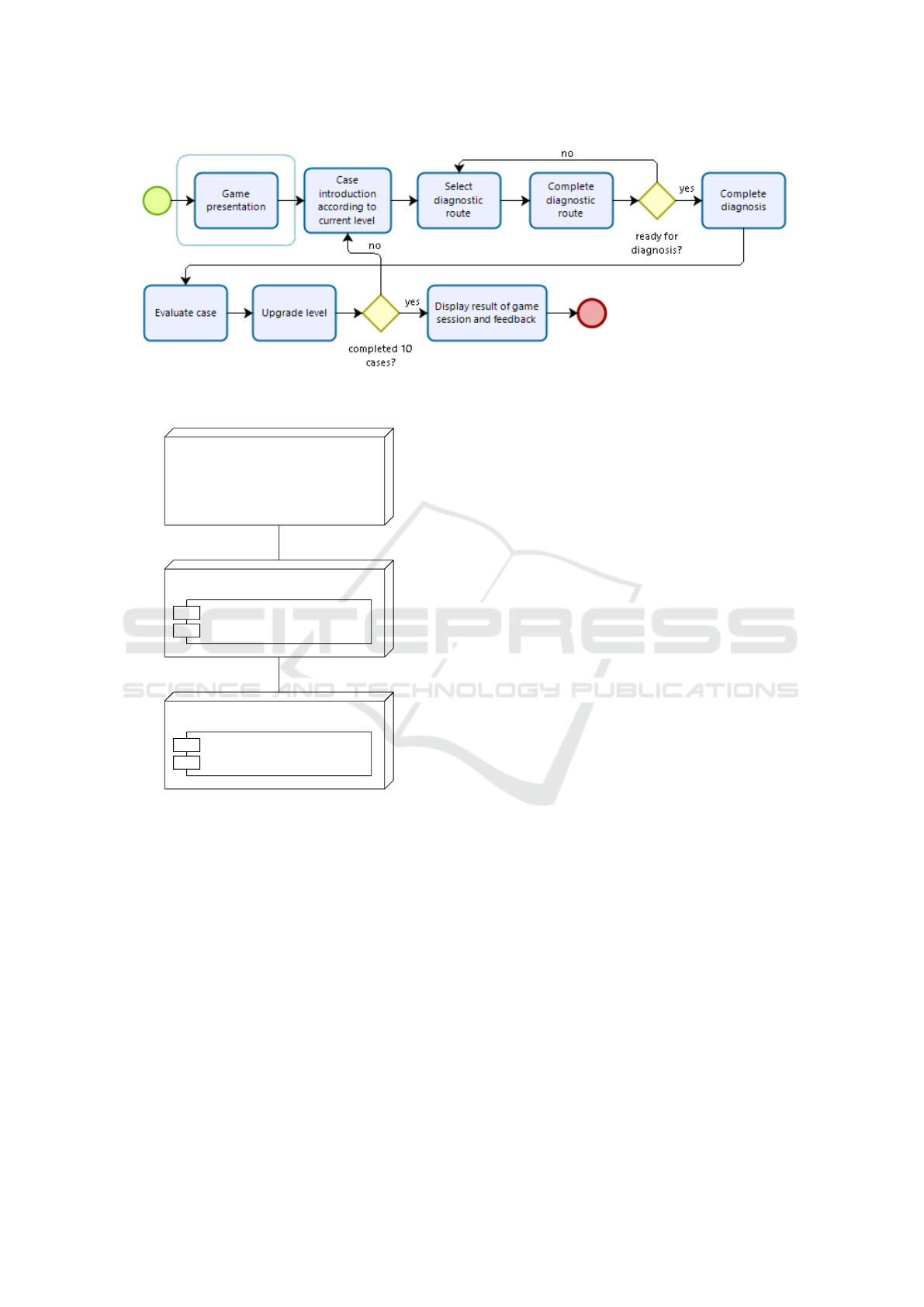
Figure 10: RealTeeth use protocol.
User Device
Amazon EC2
RealTeeth
Amazon RDS
MySQL
+HTTP
+Doctrine/ORM
Figure 11: Deployment diagram for the RealTeeth system.
The first lesson is that digital learning tools should
be designed for classrooms and not for individual stu-
dents. This was evident in the case creation-process,
especially when it came to assigning a difficulty level
to the cases. The current version of RealTeeth relies
on expert opinion (i.e. faculty member) as the only
input to assign the difficulty level to cases. However,
since case difficulty is subjective, some difference of
opinion did arise during this process. Having more
input sources, such as the historical performance of a
good amount of users, will allow for a more objective
and dynamic assignment of difficulty levels. In this
sense, future versions of RealTeeth should be able to
consider the performance of several students in each
case to provide information usable for, for example,
assigning the difficulty level of cases in a dynamic
and objective manner, flagging cases with incomplete
or inconsistent information (e.g. cases in which even
high-performing students fail consistently), and dis-
covering topics that should be revisited in class or in
external tutoring sessions (e.g. topics that are heavily
present in cases in which a particular set of students
are showing an atypical failure rate).
Additionally, this would allow for the inclusion of
further gamification elements like students leagues or
leaderboards.
A second lesson was the importance of deep per-
sonalization of the user experience according to pre-
vious performance. In its current version, RealTeeth
only uses the difficulty of previous failed/passed cases
in order to select the next case for the student. How-
ever, since diagnosis skills are multidimensional, fac-
ulty member expressed their desire for cases to be se-
lected not only based on difficulty level but also on di-
agnosis dimension. In this sense, a student with prob-
lems in one diagnosis dimension will be shown cases
that focus on that particular dimension (i.e. cases in
which the most important information is in the x-ray
evaluation or cases in which the most important infor-
mation is in the periapical test). The student can also
be given the option to select a diagnosis dimension to
use in a particular RealTeeth session. This will allow
students to identify and work on their weaknesses or
to focus their preparation for specific examinations.
Beyond these lessons, this experience, coupled
with the literature review shown in section 2, can be
used to inform the research agenda on computer sup-
ported education in the field of dentistry.
The first and perhaps more important area of fur-
ther research is the impact of digital learning tools in
dentistry education and the factors that determine this
impact. As shown in section 2, there is no consensus
on the impact of digital technologies on the perfor-
mance of dentistry students or professionals. Addi-
tionally, there seems to be external factors (i.e. fac-
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients
131

tors that are not within the boundaries of the digital
learning tool) that determine the impact of these tools
on the performance of students (Browne et al., 2004).
More research on this area is imperative not only to
determine if digital learning tools do indeed have a
positive impact on student’s performance (hence mak-
ing them worthy of attention by researchers on the
field and dentistry schools) but also under what con-
ditions (hence triggering changes in course design, in-
structional design, curricula, or classroom material).
The second area of further research is inspired by
(Bravo-Torres et al., 2017), and (Jackson et al., 2018)
and has to do with the adoption and usage pattern of
digital learning tools by students, faculty, and schools.
Key questions on this regard include what are the
adoption factors of digital learning tools in the field of
dentistry?, what is the pattern followed by this adop-
tion?, what usage is given to digital learning tools by
dentistry students and faculty members?, and what is
the relationship between digital learning tools and tra-
ditional training in the filed of dentistry?. Addition-
ally, for the case of serious games, and following the
findings of (Sipiyaruk et al., 2017), it is important to
do more research on the prevalence of learning objec-
tives over gaming objectives of serious games.
Finally, it is important to note that most research
on the field is centred on students and there is little
work centred on faculty members or schools. More
research tackling the role, challenges, and impacts of
this set of actors in computer supported education in
the field of dentistry is much needed.
REFERENCES
Afshari, F., Sukotjo, C., Alfaro, M., McCombs, J., Camp-
bell, S., Knoernschild, K., and Yuan, J.-C. (2017). In-
tegration of digital dentistry into a predoctoral implant
program: Program description, rationale, and utiliza-
tion trends. Journal of Dental Education, 81(8):986–
994.
Amer, R., Denehy, G., Cobb, D., Dawson, D., Cunningham-
Ford, M., and Bergeron, C. (2011). Development
and evaluation of an interactive dental video game to
teach dentin bonding. Journal of Dental Education,
75(6):823–831.
Antoniou, P., Athanasopoulou, C., Dafli, E., and Bamidis,
P. (2014). Exploring design requirements for repur-
posing dental virtual patients from the web to second
life: A focus group study. Journal of Medical Internet
Research, 16(6).
Arora, G. K. (2017). SOLID Principles Succinctly. Cre-
ateSpace Independent Publishing Platform.
Bandler, R. and Grinder, J. (1990). Frogs Into Princes: The
Introduction to Neuro-Linguistic Programming. Eden
Grove Editions.
Brailovsky, C., Charlin, B., Beausoleil, S., Cot
´
e, S., and
Van der Vleuten, C. (2001). Measurement of clini-
cal reflective capacity early in training as a predictor
of clinical reasoning performance at the end of res-
idency: an experimental study on the script concor-
dance test. Medical education, 35:430–436.
Brailovsky, C. A. (2001). Educaci
´
on m
´
edica, evaluaci
´
on de
las competencias, pages 103–122.
Bravo-Torres, W., Alvarado-Cordero, J., Cevallos-Lude
˜
na,
C., Vintimilla-Tapia, P., Bravo-Torres, J., and
Gallegos-Segovia, P. (2017). DentaLAV: A virtual
platform for dental multidisciplinary learning. In 2017
IEEE Colombian Conference on Communications and
Computing, COLCOM 2017 - Proceedings.
Browne, L., Mehra, S., Rattan, R., and Thomas, G.
(2004). Comparing lecture and e-learning as peda-
gogies for new and experienced professionals in den-
tistry. British Dental Journal, 197(2):95–97.
Brownstein, S., Murad, A., and Hunt, R. (2015). Imple-
mentation of new technologies in U.S. dental school
curricula. Journal of Dental Education, 79(3):259–
264.
Busanello, F., da Silveira, P., Liedke, G., Ar
´
us, N., Vizzotto,
M., Silveira, H., and Silveira, H. (2015). Evaluation of
a digital learning object ({DLO) to support the learn-
ing process in radiographic dental diagnosis. Euro-
pean Journal of Dental Education, 19(4):222–228.
De la Parra Paz, E. (2004). Herencia De Vida Para Tus
Hijos: Crecimiento Integral con Tecnicas PNL. Ed.
Grijalbo.
Farah, C. and Maybury, T. (2009). Implementing digital
technology to enhance student learning of pathology.
European Journal of Dental Education, 13(3):172–
178.
Gaba, D. M. (2004). The future vision of simulation
in health care. Quality and Safety in Health Care,
13(suppl 1):i2–i10.
Hartling, L., Spooner, C., Tjosvold, L., and Oswald, A.
(2010). Problem-based learning in pre-clinical medi-
cal education: 22 years of outcome research. Medical
Teacher, 32(1):28–35.
Issenberg, S. B., Mcgaghie, W. C., Petrusa, E. R., Gordon,
D. L., and Scalese, R. J. (2005). Features and uses
of high-fidelity medical simulations that lead to effec-
tive learning: a BEME systematic review. Medical
Teacher, 27(1):10–28.
Jackson, T., Zhong, J., Phillips, C., and Koroluk, L. (2018).
Self-directed digital learning: When do dental stu-
dents study? Journal of Dental Education, 82(4):373–
378.
L
´
opez Jordi, M., Figueiredo, M., Barone, D., and Pereira,
C. (2016). Study and analysis of information tech-
nology in dentistry in Latin American countries. Acta
odontologica latinoamericana : AOL, 29(1):14–22.
MacPherson, B. and Brueckner, J. (2003). Enhancing the
dental histology curriculum using computer technol-
ogy. Journal of dental education, 67(3):359–365.
Mari
˜
no, R., Habibi, E., Morgan, M., and Au-Yeung, W.
(2012). Information and communication technology
use among Victorian and South Australian oral health
CSEDU 2019 - 11th International Conference on Computer Supported Education
132

professions students. Journal of Dental Education,
76(12):1667–1674.
Martin, R. C. (2009). Clean Code: A Handbook of Agile
Software Craftsmanship. Prentice Hall.
McCann, A., Schneiderman, E., and Hinton, R. (2010). E-
teaching and learning preferences of dental and den-
tal hygiene students. Journal of Dental Education,
74(1):65–78.
Miller, G. E. (1990). The assessment of clinical
skills/competence/performance. Academic medicine,
65(9):S63–67.
Ratka-Kr
¨
uger, P., W
¨
olber, J., Blank, J., Holst, K.,
H
¨
ormeyer, I., and V
¨
ogele, E. (2018). MasterOnline
Periodontology and Implant Therapy—revisited after
seven years: A case study of the structures and out-
comes in a blended learning CPD. European Journal
of Dental Education, 22(1):e7–e13.
Reissmann, D., Sierwald, I., Berger, F., and Heydecke, G.
(2015). A model of blended learning in a preclinical
course in prosthetic dentistry. Journal of Dental Edu-
cation, 79(2):157–165.
Ren, Q., Wang, Y., Zheng, Q., Ye, L., Zhou, X., and Zhang,
L. (2017). Survey of student attitudes towards digital
simulation technologies at a dental school in China.
European Journal of Dental Education, 21(3):180–
186.
Schwaber, K. (2004). Agile project management with
Scrum. Microsoft Press, Redmond, WA, USA.
Shih, T. K., Squire, K., and Lau, R. W. H. (2010). Guest
Editorial: Special Section on Game-Based Learn-
ing. IEEE Transactions on Learning Technologies,
3(4):278–280.
Sipiyaruk, K., Gallagher, J., Hatzipanagos, S., and
Reynolds, P. (2017). Acquiring Critical Thinking
and Decision-Making Skills: An Evaluation of a Se-
rious Game Used by Undergraduate Dental Students
in Dental Public Health. Technology, Knowledge and
Learning, 22(2):209–218.
Vannaprathip, N., Haddawy, P., Suebnukarn, S., Sangsartra,
P., Sasikhant, N., and Sangutai, S. (2016). Desitra:
A simulator for teaching situated decision making in
dental surgery. In International Conference on Intelli-
gent User Interfaces, Proceedings IUI, volume 07-10-
March-2016, pages 397–401.
Development of Diagnostic Skills in Dentistry Students using Gamified Virtual Patients
133
