
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach
to Understand the Antecedents of Attitudes towards mHealth
Applications
Luisa Sophie Vervier, André Calero Valdez and Martina Ziefle
Human Computer Interaction Center, RWTH Aachen University, Campus Boulevard 57, Aachen, Germany
Keywords:
mHealth, Privacy Concerns, User Diversity, Attitude, eHealth Literacy.
Abstract:
Mobile health apps are a solution to make people more self-sufficient with their health in relation to their
lifestyle or medical needs. The mobile health landscape is growing, but still its usage rate is rather low. Since the
attitude towards mhealth apps has not been extensively studied so far, we conducted a multi-method approach
study in Germany. To understand people’s needs, preferences and attitudes towards mhealth applications
on the one hand and the antecedents of people’s attitudes towards mhealth applications on the other hand,
we chose a user-centered approach. To get first insights into users’ needs and attitudes, we conducted two
focus groups (N=11). Topics such as privacy concerns, data sharing and app functions have emerged as key
issues. Quantitatively, we operationalized the collected key topics as well as users’ attributes and personal
health attitudes. We collected 132 complete responses from originally 180 responses. We used partially-least
squares structural equation modeling to identify the antecedents of attitudes towards mhealth applications.
Results indicate that time saving and daily life facilitating functions are favored app features. Further, we found
advantages (e.g. drink reminder) and disadvantages (e.g. data collection). Gender and age effects could be
detected regarding health literacy, privacy concerns, and data sharing. Older participants are more cautious and
reserved with the usage of health apps. Women in general show a higher health-literacy. eHealth literacy and
intention to share data were identified as being the strongest influence on a positive attitude towards mhealth
apps. To ensure that mhealth apps further enjoy a rising popularity, it is important to meet the users’ concerns
about privacy and help them to acquire eHealth literacy.
1 INTRODUCTION
Mobile applications are commonly used and affect
daily lives. Especially in the health care sector, the
development of health apps for lifestyle reasons is
increasing. The “quantified self” movement is one ac-
tuator for people’s interest in using mhealth apps (Lup-
ton, 2013). Moreover, people in general are becoming
more interested in taking an active role in their own
health care. They have become eager to take health
care decisions on their own. Especially, ever since the
physician-patient relationship has turned into a shared
decision-making relationship (Ernst et al., 2014). A
further aspect which gives a special importance to the
mhealth topic is the societal challenge of demographic
change. People will increasingly depend on techni-
cal support in the future (Lupton, 2013). Therefore,
there can be no better starting point than using and
developing existing and well known techniques fur-
ther, such as smartphone apps (Bhavnani et al., 2016).
Mobile health apps are an advanced form of eHealth.
As smartphones enjoy a rise in popularity especially
with versatile software, apps have great potential for
revolutionizing the health-care services. However, the
quality as well as the users’ acceptance of such systems
is still questionable (Powell et al., 2014). Thus, there is
a growing urgency to understand peoples’ needs, pref-
erences, and attitudes towards mhealth applications.
What kind of functions are important for an mhealth
app from a users’ perspective? And on a meta-level,
what are important topics that appear when looking at
peoples’ attitude towards mhealth apps? As the atti-
tude shapes the willingness to use mhealth apps, it is of
special interest to identify such aspects and to consider
them when defining guidelines for mhealth app devel-
opment. In this study, we investigate this topic. The
aim of the study is to explain the antecedents of the
attitude towards mhealth apps and to derive guidelines
for digital health care actors.
Vervier, L., Valdez, A. and Ziefle, M.
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach to Understand the Antecedents of Attitudes towards mHealth Applications.
DOI: 10.5220/0007720002130221
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 213-221
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
213

2 STATE OF THE ART
In the following section, we present an overview of the
different aspects that play a role in trying to understand
the attitude towards mhealth applications.
2.1 mHealth
The aim of mHealth is to contribute to the health care
of users through the use of mobile devices (Conway
et al., 2016). Mobile devices such as a smart phone or
tablet provide a platform for maintaining motivation,
defining goals, and receiving feedback (Appelboom
et al., 2014). They have a number of characteristics
that are considered to have “(...)great potential for the
healthcare sector” (Matusiewicz et al., 2017).
The most important characteristic of smartphones
is that they are part of everyday life (Gehring et al.,
2014). Since smartphones are highly valued by users
(Dennison et al., 2013) and have a size that makes
them transportable, users usually carry them along
all day long when switched on. That way users are
reachable regardless of time and place. Moreover, it
enables to address all kind of user groups. It offers an
optimal opportunity to disseminate information and
applications on the subject of health in a target-group-
oriented, effective and independent manner, regardless
of time and place.
This is not least due to two other important features
of smartphones: built-in sensors and networking (Den-
nison et al., 2013). The built-in sensors make it possi-
ble to automatically measure health-related data such
as a user’s physical activity. Thus, individual needs
can be met. The interconnection of smartphones also
allows users to share their health data with friends,
acquaintances or even their physicians and health in-
surers.
These numerous advantages of mHealth result in
a great potential for improving and promoting health
care, which could possibly fundamentally change the
health market and the health system. Although many
advantages are present, the attitude towards health
apps is very different. Individual needs are often not
covered to the satisfaction of users. So, there are many
immature health app versions on the market that are
questionable regarding security and privacy. These
aspects, as well as the individual ability to use health
apps, present great challenges for developers. With
our study we want to shed light on the users’ need and
preferences as well as on the main aspects people deal
with when considering health app usage.
2.2 Online Privacy in the Context of
mHealth Apps
Data protection and user privacy are central aspects in
the health care context. The explanation for this lies in
the way health apps work. They can constantly collect
information about the user’s health in real time (Gao
et al., 2015). Since this information is usually per-
ceived by users as sensitive, data protection is a topic
of great importance. Users’ worries include above all
the concern for the protection of privacy and the pro-
tection against unauthorized use of the data (Bansal
et al., 2010). As soon as users disclose information
about their health online, there is a risk that it may be
misused or illegally used by third parties. Thus, when
using an app, the user runs a risk that is directly related
to the concern for the security of personal data (Milt-
gen et al., 2013). Nevertheless, users are often willing
to take the risk and disclose their personal data in an
app in order to gain a personal advantage. In such
cases the perceived advantage must be greater than the
perceived risk for the user to be willing to pass on his
data (Li et al., 2014).
2.3 eHealth Literacy
The consideration of users’ prior knowledge is often
neglected in the development of mHealth offerings. It
is assumed that the user has the necessary knowledge
to deal with it (Norman and Skinner, 2006). However,
studies indicate that this assumption is not necessarily
true. In order to be able to use mHealth services for
their own benefit, however, users must have certain
skills which are summarized under the term “eHealth
Literacy”. These include: “the ability to seek out, find,
evaluate and appraise, integrate, and apply what is
gained in electronic environments toward solving a
health problem” (Norman and Skinner, 2006). Users
must therefore be able to independently search, find,
evaluate, and apply health information. The prerequi-
site for the success of this process is that users can deal
with the corresponding technology and the countless
sources of information. They must be able to critically
question the information and the media they provide
in order to form trust (Vervier et al., 2018). Only in
this way users can make so-called informed decisions
for their own health. In order to be able to develop
mHealth services that are tailored to the needs and abil-
ities of users, these abilities must first be surveyed. For
this purpose, Norman and Skinner have developed the
so-called eHealth Literacy Scale (eHEALS). The scale
is based on elements of socio-cognitive learning theory
and self-efficacy expectations. It combines six subject
areas or basic skills: “traditional literacy, health lit-
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
214

eracy, information literacy, scientific literacy, media
literacy, [...] computer literacy” (Norman and Skinner,
2006). To understand in what extend health literacy
has an impact on the positive attitude on mhealth apps,
we considered this phenomenon as an important aspect
in our study.
3 RESEARCH METHODOLOGY
This study aims at exploring two perspectives regard-
ing the attitude towards mhealth applications. In a first
step insights of people’s experience and ideas about
functional aspects as well as barriers and motives of
mhealth apps are collected qualitatively. In a second
step, based on the results of the focus group, all key
factors were included in an online survey and opera-
tionalized quantitatively. Moreover, dimensions such
as personal health attitude implying eHealth literacy
and health orientation, online privacy perception, in-
cluding privacy concerns, as well as the intention to
share data and last but not least user attributes (i.e.,
age, gender) were taken into account in order to under-
stand the attitude towards mhealth applications. This
two-way multi-method approach seemed to be the best
method to identify, evaluate, and quantify these fac-
tors. Two focus groups were run with two different
age groups. Based on the results an online survey was
designed (see figure 1). The most important research
questions leading the investigation were:
1.
Does gender or age have an impact on user’s pref-
erences (features, disadvantages, advantages)?
2.
How strong do personal health attitudes (health
orientation and eHealth literacy) and online pri-
vacy perception (privacy concerns) as well as the
intention to share data explain the positive attitude
towards mhealth applications?
3.
Do further user factors such as age and gender
have an additional impact on the positive attitude
on mhealth apps?
3.1 Focus Group Study
The aim of the focus group approach was to identify
and discuss young and old adults’ ideas of mobile
health applications, its usage options, functions, ad-
vantages and disadvantages. For this purpose, two
successive focus groups were carried out with 11 (8
female and 3 male) participants with an age range
from 19-57 (
M = 35.6
years,
SD = 16.6
) years. The
younger group was aged between 19 and 25 years and
the older group between 48 and 57 years. In the be-
ginning participants were encouraged to brainstorm
about mobile health apps they know or even use. In a
free discussion, participants shared their experiences
and previous knowledge of mhealth applications. In
a further step topics such as functions of health apps
as well as motives for use and non-use were discussed
and ranked. As main topics privacy concerns, data
sharing, and app functions have emerged as key issues
in both groups. Older participants stated a stronger
privacy concern about their personal data than younger
participants.
3.2 Online Survey
To understand which factors influence the attitude to-
ward mhealth applications, we conducted a question-
naire study with 132 participants. The survey data was
collected in Germany in summer 2017 via an online
questionnaire. Participants took part in the study vol-
untarily without any compensation. At the beginning
of the survey, detailed information was given on the
purpose and objective of the study. We also stressed
that participants were welcome to express their views
on the subject and exchange their opinions openly. Ad-
ditionally, in accordance with data protection standards
in empirical studies, we informed the participants that
none of their responses could be traced back to them
personally. The survey consisted of four parts starting
with user attributes in part one.
User Attributes.
We assessed age, gender, and self-
rated app experience (“I consider myself a very experi-
enced user of apps” to be answered on a 6-point-Likert
scale). Moreover, we assessed general usage frequency
of health apps (i.e. nutrition app, lifestyle app, fitness
app, disease control app, app for medical service) on a
6-point-Likert scale from never to several times a day.
Variables regarding the personal health attitude were
assessed in a second part.
Personal Health Attitude.
We used the health con-
sciousness scale by Dutta Bergmann (Dutta-Bergman,
2004). The respective items (five of a kind; e.g. I do
everything I can to stay healthy. or Living life in best
possible health is very important to me.) were added
after having checked the scale reliability (Cronbach’s
α = .773
). The data amounted to an AVE of .528.
Additionally, we measured eHealth literacy with the
eHeals literacy scale by Norman and Skinner (Nor-
man and Skinner, 2006) consisting of 7 items such
as I know how to find helpful health resources on the
Internet among others. Cronbach’s alpha for the scale
was .93 and the average variance extracted (AVE) was
.632.
Privacy Attitude.
We used three items adapted by
Li (Li et al., 2014) as the online privacy concern scale
as e.g., I am concerned about threats to my personal
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach to Understand the Antecedents of Attitudes towards mHealth
Applications
215
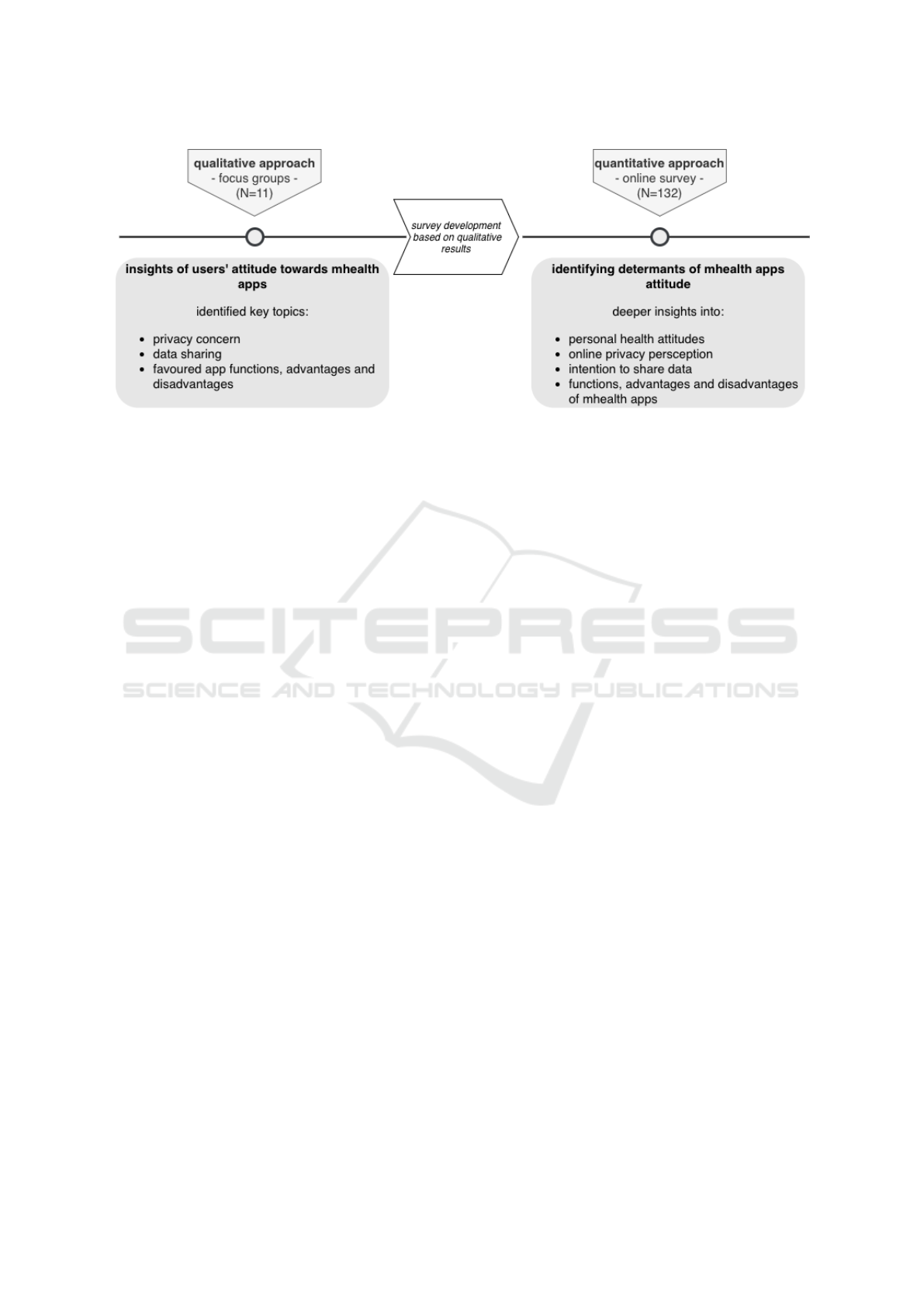
Figure 1: Overview of research process showing both qualitative and quantitative measures to address our research questions.
privacy today. The scale showed a good reliability of
Cronbach’s α = .817 and an AVE of .719.
In the privacy attitude section we additionally
added a scale called intention to share with 3 items
created by the authors. I am willing to provide my
health data to a doctor of my choice., I personally
see an advantage in sharing my health data with my
physician. and By sharing my health data with my
physician, a better health care is guaranteed for me.
with Cronbach’s α=.843 and AVE=.762.
Attitude Towards Health Apps.
Last but not least, the
attitude towards mhealth (3 items, developed by au-
thors: The usage of health apps is fun., The usage of
health apps is a good idea. and I like the idea of using
a health app.) were measured (
α = .871
;
AV E = .795
).
All items in the scales had to be answered on a 6-point-
Likert scale from I do not agree at all to I totally agree.
Finally, as generated result from the previous focus
group, advantages and disadvantages were also con-
sidered in the last part. Participants had to rank the
aspects in order of individual importance.
3.3 Statistical Method and Procedures
To understand our data, we used descriptive statistics
and report 95%-confidence intervals on all point esti-
mates. When using null-hypothesis-significance test-
ing, we set our level of significance to
α = .05
. In this
study we used partial least square structural equation
modeling (PLS-SEM) in Smart-PLS 3.0 (Hair Jr et al.,
2016) to understand the causal relationship of the an-
tecedents mhealth attitude. The benefit of PLS-SEM
lies in the possibility of causal inference in model-
ing. We report the path-coefficients, the
r
2
was ad-
justed for the predicted variables in the inner model.
We designated the significant relationships from the
bootstrapping procedure. Cronbach’s alpha and the
average explained variance as quality measures of our
model are reported (see section 3.2 Online Survey).
As PLS-SEM is used for exploratory approaches, the
following assumption were made: We assume that
with increasing age, privacy concerns increase. The
opposite we assume with health orientation. It will
decrease with increasing age. Female participants will
have a higher health orientation and a higher eHealth
literacy. We assume the stronger the privacy concerns
the lower will be the intention to share data. Moreover,
we assume that a higher health orientation and eHealth
literacy enhances the positive attitude towards mhealth
apps. However, the online privacy perception might
influence the positive attitude negatively. Figure 2 por-
trays the research model and the underlying theoretical
framework where the latent constructs are assigned to
two thematic topics: personal health attitude and pri-
vacy attitude. Personal health attitude includes health
consciousness and eHealth literacy. Privacy attitude
covers privacy concern and intention to share data. The
arrows symbolize the assumed influences among the
constructs on the positive attitude towards mHealth
apps. Age and gender are depicted underneath the dia-
gram as two factors which might affect the particular
constructs in general.
3.4 Sample Description
Our sample consisted of 132 participants who com-
pletely answered the online survey from originally
180. 62% were female and 38% were male. The age
range was between 18 and 63 years with
M = 35.9
(
SD = 23.5
, see also Table 1 and Table 2). The sample
was divided into age groups (youngest group 18 to 25
years (39%); middle-aged group 26 to 40 years (28%)
and older group 41 to 63 years (33%)). The educa-
tion level was rather high. 39% had completed a high
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
216
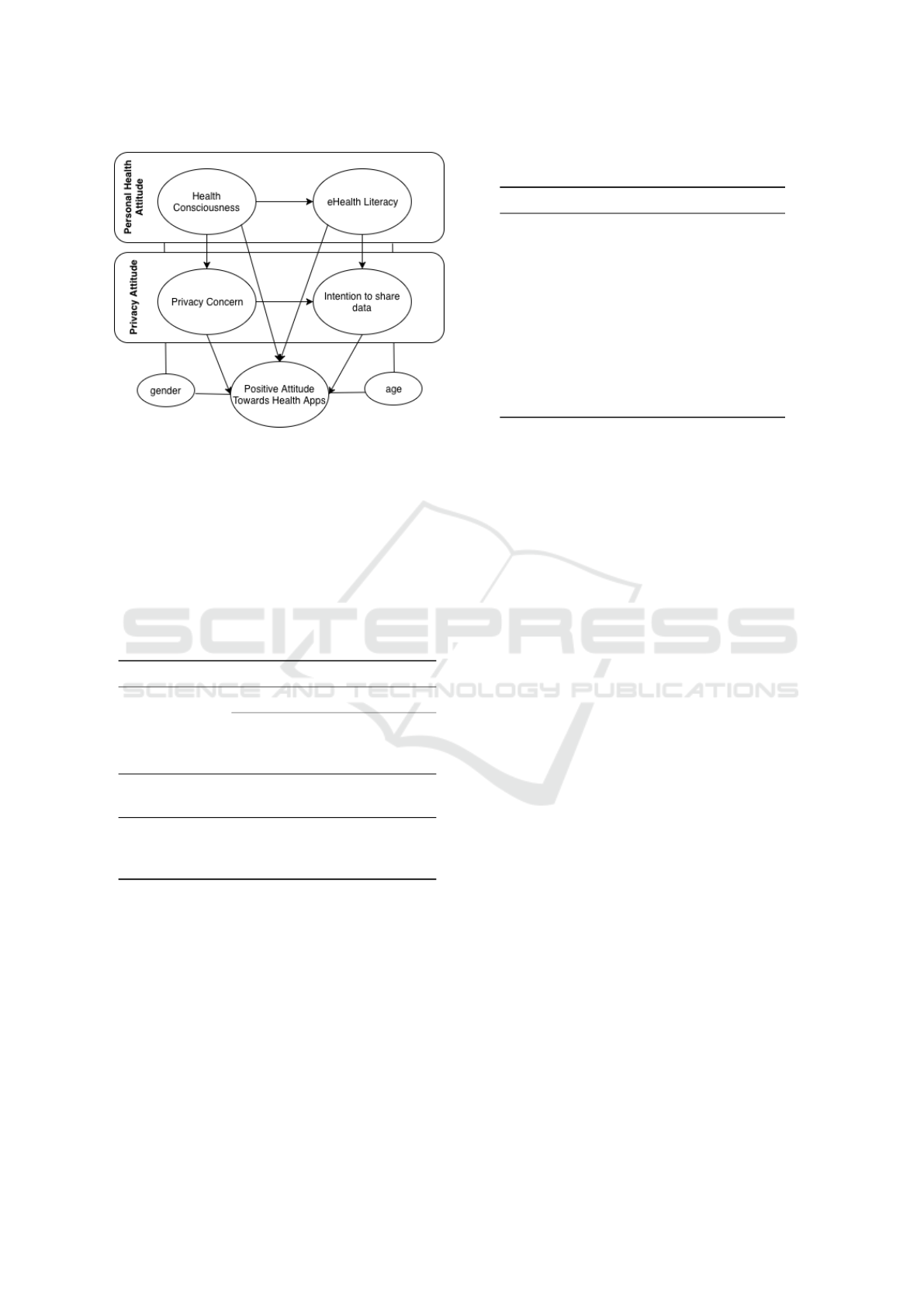
Figure 2: Overview of theoretical framework of our research
model.
school degree and 38% held a university certificate, in-
dicating the heterogeneity of the sample’s educational
level. Most of the participants (30%) allocated their
current activity in the commercial area, 29% in a tech-
nical area, 14% allocated it to the social field, 8% to
a medical field, 8% to an artistically field and 8% to
other areas.
Table 1: Demographic characteristics of aggregated sample
(N=132).
Demographic characteristics Percentage
Age
mean (SD) 35.9 (23.5)
18-25 years 39%
26-40 years 28%
41-63 years 33%
Gender
women 62%
men 38%
Education level
university 38%
high school degree 39%
other 23%
Participants rated themselves as rather experienced
app users with
M = 4.25
(
SD = 1.3
; scale from 1 to 6).
The experience decreases significantly (
F(2, 129) =
17.529, p < .001
) between the youngest and mid-
dle age groups (
M
younger
= 4.86
;
SD
younger
= 1.05
/
M
middle
= 4.38
;
SD
middle
= 1.29
), but increases sig-
nificantly with the older participants (
M
older
= 3.44
;
SD
older
= 1.16
). When asked about general usage fre-
quency, the participants generally seemed to use few
health apps down to none. Fitness-apps (
M = 2.45
;
SD = 1.58
) are still used the most, followed by nu-
trition (
M = 1.80
;
SD = 1.58
), lifestyle (
M = 1.69
;
SD = 1.18
), medical service (
M = 1.38
;
SD = .69
) and
Table 2: Mean (M) and standard deviation (SD) values of
our measured variables.
Variable M SD
age 35.90 23.50
app experience 4.25 1.30
usage fitness app 2.45 1.58
nutrition app 1.80 1.58
lifestyle app 1.69 1.18
medical service app 1.38 0.69
disease control app 1.28 0.91
health consciousness 4.09 0.90
eHealth literacy 3.94 0.93
privacy concerns 4.07 1.13
attitude towards mhealth app 3.52 1.13
disease control apps (
M = 1.28
;
SD = .91
). In general,
the sample constituted a rather healthy group with a
health consciousness value of
M = 4.09
(
SD = 0.9
; 6
points max.). The eHealth literacy level was averagely
high with
M = 3.94
(
SD = 0.93
). In this context, a
significant gender (
F(1, 112) = 6.37; p = .013
) effect
could be detected. Female participants (
M = 4.08
,
SD = 0.80
) rated their competence to evaluate digi-
tal health information higher than male participants
(M = 3.68, SD = 0.97) participants.
Participants reported a rather high privacy con-
cern measured at
M = 4.07
(
SD = 1.13
; 6 points
max.). Again, a significant difference in age was ob-
served (
F(1, 115) = 13.108; p < .001
). The concern
for online privacy in general was significantly stronger
among older participants (
M = 4.67
,
SD = 0.93
; 6
points max.) than among younger participants with
a mean of
M = 3.56
/6 points (
SD = 0.92
). A similar
picture emerged in the personal attitude to share data
(
M = 3.84
,
SD = 0.12
;
F(2, 107) = 7.439, p < .001
).
Young participants (
M = 4.17
,
SD = 0.91
) perceived
a significantly higher advantage in this and show
a greater willingness to transmit their health data
digitally to their physician than older participants
(
M = 3.84
,
SD = 1.27
).The attitude towards health
apps was averagely high with a mean of
M = 3.52
/6
points (SD = 1.13).
4 RESULTS
The presentation of the results is guided by our re-
search questions. We first look at the impact of user
diversity towards mHealth before looking for causal
explanations. Lastly we include age and gender into
our models.
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach to Understand the Antecedents of Attitudes towards mHealth
Applications
217
4.1 Impact of User Diversity on Users’
Preferences Towards mHealth Apps
In order to identify the importance of specific func-
tions and features of health apps, participants were
asked to rank six options which were characterized as
central aspects in the focus groups for each preference.
As a most important function user-friendly operation
was mentioned, followed by support for the develop-
ment of health awareness, reminder for e.g., eating,
information about health topics as well as tracking
e.g., steps. On the last place of the ranking, agreement
of consultation hours with physicians were mentioned.
No age or gender effects could be detected.
Table 3 shows the results of the ranked advantages
and disadvantages of health apps. Also in the forma-
tion of these rankings, no statistically significant user
diversity influences could be detected. So far a very a
homogeneous picture emerged when taking user diver-
sity such as age and gender into account when looking
at different aspects of preferences.
4.2 Explanation of Attitude Towards
mHealth Apps with Personal Health
Attitudes and Online Privacy
Perception
To find out what determinants influence the attitude
towards mhealth apps we used the structural equation
modeling using partially-least-squares algorithm. In
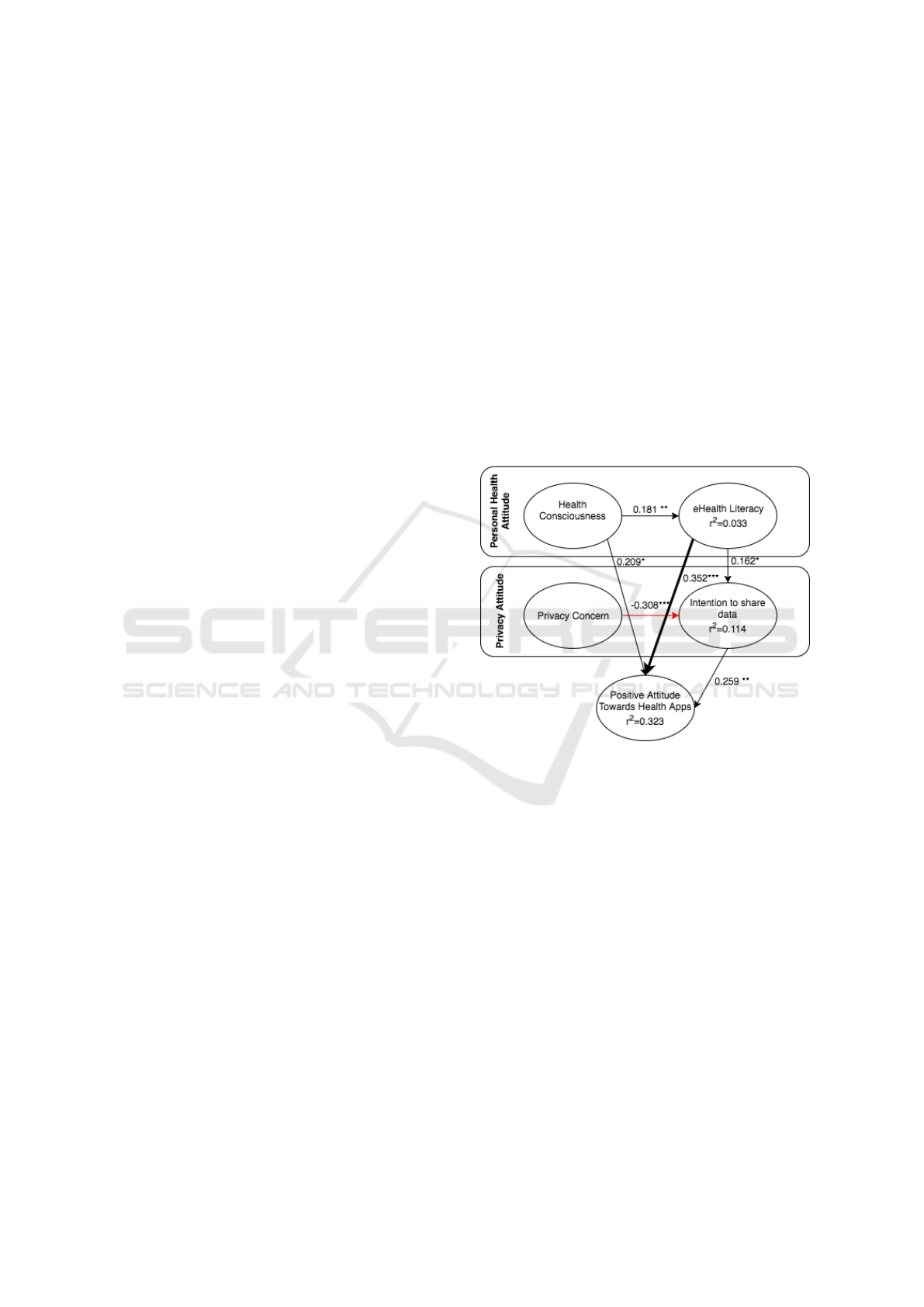
figure 3 the inner model of positive attitude towards
health apps is depicted which we introduced earlier as
the theoretical framework of our study (see figure 2) .
Due to readability we decided not to present the outer
model. The majority of path coefficients for the items
reached a value of 0.7, and 0.8 in most cases. Only the
health orientation items included two of totally five
of a kind with over 0.6 (scale reliability Cronbach’s
α = .773
,
AV E = .528
). Path coefficients are written
on the arrows which connect the latent constructs. Neg-
ative influence is colored red. We identified significant
correlations by annotating the test values with aster-
isks. The adjusted
r
2
indicates the extend the variable
is influenced by others. At a first sight, the bold arrow
shows the main determinant of the latent construct of
the positive attitude towards mhealth apps. In the sam-
ple eHealth literacy had the biggest positive impact
as previously assumed. Participants who are familiar
with their smartphones and in general with digital de-
vices and who are able to independently search for
and and find health information, evaluate and apply it
according to the definition of eHealth literacy. Further,
they seem to be open-minded towards mhealth.
Being health conscious also influences the attitude
positively, however, by far not as strong. It seems
that being interested in leading a healthy life does not
include being interested in electronic services which
might support the way of life. Looking at the privacy
attitude area, privacy concern itself did not influence
the positive attitude significantly at all. It had a nega-
tive impact on the intention to share data. The higher
the personal privacy concerns were the less people
were willing to disclose data in the context of mhealth
apps. Still, looking at the second latent construct of pri-
vacy attitude, the intention to share data correlates pos-
itively with the positive attitude towards mhealth apps.
To sum up, according to the sample, determinants of
the positive attitude of mhealth apps are eHealth liter-
acy and the willingness to pass the required data via
an mhealth app.
Figure 3: Results of the PLS-SEM Algorithm. Only sig-
nificant paths (after bootstrapping) are shown. Red arrows
indicate negative path coefficients.
4.3 Impact of User Diversity on
Antecedents of Attitude Towards
mHealth Apps
Taking a deeper look at our data, age and gender had
different effects on the investigated model. User diver-
sity played an important role. Starting with gender, the
positive attitude is described best by highly health con-
scious male participants (
β = 0.340, p < .05
). Attitude
is further significantly influenced by intention to share
(
β = 0.334, p < .05
). A further negative significant
influence was detected between privacy concern and
intention to share data (
β = −0.328, p < .05
). Looking
at the model through the “female glasses” only one
significant impact could be found. However, this one
was very strong between eHealth literacy and positive
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
218

Table 3: Ranking (#) of mHealth app advantages and disadvantages (N=132).
advantages # disadvantages #
constant availability of own health data 1 lack of data protection 1
interesting features 2 monitoring by third party 2
check compatibility of drugs 3 lack of personal contact 3
time saving (medi order) 4 no direct questions possible 4
road-saving 5 constant data collection 5
overview of pharmacy nearby 6 dependence on smartphone 6
attitude with a path coefficient of
β = 0.472(p < .001
).
Age showed effects in the middle-aged and older age
group. Similar to female participants, a significant
influence was found on eHealth literacy and attitude
(
β = 0.513, p < .001
), a negative one on privacy con-
cern and intention to share (
β = −0.337, p < .005
)
and finally on health orientation and eHealth literacy
(
β = 0.404, p < .001
). The one and only significant
influence in the older age group was detected on in-
tention to share and attitude with a path coefficient of
β = 0.546(p < .001
). To conclude, user diversity such
as age and gender play a dominant role regarding the
attitude towards mhealth apps.
5 DISCUSSION & GUIDELINES
Discussion.
With our paper “Attitude” we wanted to
investigate on people’s ideas and position relating to
the mobile health services or rather health apps. To
understand people’s needs, preferences and attitudes
towards mhealth applications on the one hand and
on the other hand to understand the antecedents of
people’s attitudes towards mhealth applications on a
meta-level, we chose a user-centered approach. That
way, we could gather more robust results and deal
with the research question in detail. In a first step
focus groups were run, in which we analyzed users’
ideas of mobile health applications, its usage options,
functions, advantages and disadvantages.
In a second step, an online questionnaire was sent
out in which the results of the focus groups were quan-
tified as well as the attitude of health apps and its
antecedents were explored. To do so, we formulated
a model with two thematic topics: personal health
attitude consisting of two latent constructs, namely
health orientation and eHealth literacy. The second
topic dealt with privacy attitude, operationalized by
online privacy concern and willingness to share data.
Last but not least user attributes (age, gender) were
taken into account in order to understand the attitude
towards mhealth applications.
Users’ insights won from the focus group study
showed that users favored app features were aspects
which improve and facilitate daily health life routines
and save time. Thus, arranging appointments via app
were highlighted. Also functions, which allow keep-
ing track on and documenting health topics were men-
tioned. In this respect, our results are consistent with
those of Mendiola (Mendiola et al., 2015). The ideas
about functions were in line with the current trend of
the “quantified self” movement. Moreover, privacy
concerns have emerged as important topics. Partici-
pants considered good data encryption and the protec-
tion of their personal data as very important as well
as the desire for a serious provider (Wilkowska and
Ziefle, 2012). Besides privacy aspects, simple and
user-friendly operations were essential features. In
general, participants could see many advantages in
using a mhealth apps which could offer an overview
of pharmacies and physicians close by. Reminders of
different kinds such as a drink reminder were also con-
sidered as an important advantage, especially by older
participants. Not surprisingly, communication with
physicians were mentioned among others. Participants
seemed to be very reflected. Among all great features
an app could offer, they also were aware of possible
negative aspects such as smartphone addiction and the
feeling of uncontrolled and unclear data collection. Fi-
nally, lack of personal contact as the fear of feeling
socially alone were mentioned.
When looking at the outcomes in the questionnaire
study, again, it was corroborated that users indepen-
dent of age or gender attached high importance to
the same features, advantages and disadvantages as
discussed above and also portrayed in table 3. In-
terestingly, that the advantage of having a constant
overview about own health data goes hand in hand
with the disadvantage of perceived lack of data pro-
tection. As assumed the topic of the so called privacy
calculus (Li et al., 2014) appears in the context of
mhealth app usage. It seems that the appreciated fea-
tures of mhealth apps might outweigh the perceived
risk (data protection and privacy) as long as the ad-
vantages of facilitating daily life and saving time are
predominant as well as user can trust the provider.
In our study we also tried to shed light on the an-
tecedents of a positive attitude towards mhealth apps.
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach to Understand the Antecedents of Attitudes towards mHealth
Applications
219

In advance, we prepared assumptions based on lit-
erature but also on the results of the focus groups.
We could make note that with increasing age, privacy
concerns increase as well. The results of the focus
group already gave a hint, that older people are more
concerned about their online privacy. The results are
consistent with other studies on the subject as e.g.,
Zeissig et al. (Zeissig et al., 2017). No significant
results could be found according to the assumption
that health orientation rises up with decreasing age.
That might be due to the fact that the sample in gen-
eral represented a rather healthy one. Another reason
might be attributable to the lower validity of items as
described in the research methodology. The assump-
tion that female participants will have a higher health
orientation and a higher eHealth literacy could empiri-
cally be proven at least for eHealth literacy. The model
showed that females eHealth literacy had the biggest
influence on the positive attitude towards mhealth apps.
In other words, in our study, women in general were
more familiar with the usage of digital devices and
the health topic. We also learned from this study, that
the extent of privacy concerns represented the biggest
motive or barrier in the same way for the willingness
to share data.
Guidelines.
Our findings show needs and prefer-
ences of participants who are rather healthy and could
imagine a mhealth app for lifestyle reasons. Therefore,
our ideas will give guidance to developers of lifestyle
health apps. In general, mhealth apps should offer
a user-friendly operation. As people are becoming
more interested in taking an active role in their own
health care, features which improve and facilitate daily
health life routines, save time are appreciated most.
The challenge however occurs right here, where ap-
preciated functions by users collide with individual
privacy concerns and data protection worries. At this
point, mhealth app providers must assure and be able to
let the user use the app with all security and encryption
possibilities of the users sensitive data which are on
the highest standard. As we learned from the study, pri-
vacy concern influences the willingness to share data
negatively. In other words, as long as the privacy con-
cern can be taken by offering highly secured mhealth
apps, the intention to share data will rise. Thus, people
will benefit from a better personalized service accord-
ing to their needs. Moreover, being eHealth literate
increased the positive attitude and thus possible usage
of a mhealth app enormously. Implementing learning
opportunities in a mhealth app for improving and keep-
ing one owns health behaviour skills up-to-date would
be an interesting further feature.
6 LIMITATION & FUTURE
RESEARCH
As studies always need to fit time and content frame-
work conditions, there are limitations that occur nat-
urally. Since the study was conducted in the authors
and students surrounding at a university, a rather tech-
nically affine sample was measured. Future studies
have to focus on conducting more representative stud-
ies as well as bigger samples to make representative
statements. Moreover, different cultural aspects of dif-
ferent countries might deliver interesting results. So
far, this study aimed at gaining general attitudes to-
wards mhealth applications. At this point it would
be of interest to develop a possible mhealth app and
evaluate it with e.g., the unified theory of acceptance
and use of technology model (UTAUT) in the health
care sector (Slade et al., 2013). That way the intention
of using such a mhealth app could be explored more
in detail. As the phenomenon of eHealth literacy oc-
curred to be a very important result in our study it is
important to pay close attention to this topic. In this
study, we entered the validated item scale by Norman
and Skinner (Norman and Skinner, 2006) who can be
seen as the pioneers of the first eHealth literacy model.
However, in course of time different theoretical ap-
proaches have been made, regarding current digital
standards (Griebel et al., 2018) who also questioned
Norman and Skinner’s approach according to its lack
of usage context and the missing fit with interactive
Web 2.0 contents. The digital health literacy instru-
ment (DHLI) by Rosalie van der Vaart for instance
represents a new approach with a validated item bat-
tery which operationalizes seven different constructs
such as operational skills, navigational skills, informa-
tion searching, evaluation reliability, determining rele-
vance, adding content, and protecting privacy (van der
Vaart and Drossaert, 2017). Another interesting and
validated model which should be considered in a fur-
ther empirical investigation with the same research
question is the e-HLS Instrument by Secking (Seçkin
et al., 2016) who takes a three factor solution into
account (behavioral, communicational and attitudinal
components of health literacy). With the decision and
usage for one of the current theory approaches, a gold
standard could also be set as a side effect which is
still missing in the research of eHealth literacy. A fur-
ther future research idea would be to subject the same
research question to a sample with sick people. Addi-
tionally, needs and preferences should also be explored
for people who need to use such an app for medical
or more severe healthy reasons in form of monitoring
their health. Questions which occur especially in an
individual usage context of health monitoring could
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
220

be the way of personalization of health information
in the conflict situation of personalization preferences
and privacy concerns (Calero Valdez and Ziefle, 2019).
The research field of mhealth apps, eHealth literacy
and privacy concerns in the healthcare context is still
wild and huge and offers many empirical research op-
portunities which need to be seized.
ACKNOWLEDGEMENTS
The authors thank all participants for sharing their
thoughts and opinions. We would also like to thank
the reviewers for their valuable feedback. A special
thanks goes to the research support of Kathrin Kohl.
REFERENCES
Appelboom, G., LoPresti, M., Reginster, J.-Y., Sander Con-
nolly, E., and Dumont, E. P. (2014). The quantified
patient: a patient participatory culture.
Bansal, G., Gefen, D., et al. (2010). The impact of personal
dispositions on information sensitivity, privacy con-
cern and trust in disclosing health information online.
Decision support systems, 49(2):138–150.
Bhavnani, S. P., Narula, J., and Sengupta, P. P. (2016). Mo-
bile technology and the digitization of healthcare. Eu-
ropean heart journal, 37(18):1428–1438.
Calero Valdez, A. and Ziefle, M. (2019). The users’ per-
spective on the privacy-utility trade-offs in health rec-
ommender systems. International Journal of Human-
Computer Studies, 121:108–121.
Conway, N., Campbell, I., Forbes, P., Cunningham, S., and
Wake, D. (2016). mHealth applications for diabetes:
user preference and implications for app development.
Health informatics journal, 22(4):1111–1120.
Dennison, L., Morrison, L., Conway, G., and Yardley, L.
(2013). Opportunities and challenges for smartphone
applications in supporting health behavior change:
qualitative study. Journal of medical Internet research,
15(4).
Dutta-Bergman, M. J. (2004). Health attitudes, health cog-
nitions, and health behaviors among internet health
information seekers: population-based survey. Journal
of medical Internet research, 6(2).
Ernst, J., Brähler, E., and Weissflog, G. (2014). Patient
involvement in medical decision making–an overview
on patient preferences and impacting factors.
Gao, Y., Li, H., and Luo, Y. (2015). An empirical study of
wearable technology acceptance in healthcare. Indus-
trial Management & Data Systems, 115(9):1704–1723.
Gehring, H., Pramann, O., Imhoff, M., and Al-
brecht, U.-V. (2014). Zukunftstrend "Medical
Apps". Bundesgesundheitsblatt-Gesundheitsforschung-
Gesundheitsschutz, 12(57):1402–1410.
Griebel, L., Enwald, H., Gilstad, H., Pohl, A.-L., More-
land, J., and Sedlmayr, M. (2018). ehealth literacy
research—quo vadis? Informatics for Health and So-
cial Care, 43(4):427–442.
Hair Jr, J. F., Hult, G. T. M., Ringle, C., and Sarstedt, M.
(2016). A primer on partial least squares structural
equation modeling (PLS-SEM). Sage Publications.
Li, H., Gupta, A., Zhang, J., and Sarathy, R. (2014). Ex-
amining the decision to use standalone personal health
record systems as a trust-enabled fair social contract.
Decision Support Systems, 57:376–386.
Lupton, D. (2013). Quantifying the body: monitoring and
measuring health in the age of mhealth technologies.
Critical Public Health, 23(4):393–403.
Matusiewicz, D., Pittelkau, C., and Elmer, A. (2017). Die
Digitale Transformation im Gesundheitswesen. Medi-
zinisch Wissenschaftliche Verlagsgesellschaft, Berlin.
Mendiola, M. F., Kalnicki, M., and Lindenauer, S. (2015).
Valuable features in mobile health apps for patients and
consumers: content analysis of apps and user ratings.
JMIR mHealth and uHealth, 3(2).
Miltgen, C. L., Popovi
ˇ
c, A., and Oliveira, T. (2013). Determi-
nants of end-user acceptance of biometrics: Integrating
the “big 3” of technology acceptance with privacy con-
text. Decision Support Systems, 56:103–114.
Norman, C. D. and Skinner, H. A. (2006). eHEALS: the
eHealth literacy scale. Journal of medical Internet
research, 8(4).
Powell, A. C., Landman, A. B., and Bates, D. W. (2014). In
search of a few good apps. Jama, 311(18):1851–1852.
Seçkin, G., Yeatts, D., Hughes, S., Hudson, C., and Bell, V.
(2016). Being an informed consumer of health infor-
mation and assessment of electronic health literacy in a
national sample of internet users: validity and reliabil-
ity of the e-hls instrument. Journal of medical Internet
research, 18(7).
Slade, E. L., Williams, M. D., and Dwivedi, Y. (2013). An
extension of the UTAUT 2 in a healthcare context. In
UKAIS, page 55.
van der Vaart, R. and Drossaert, C. (2017). Development
of the digital health literacy instrument: measuring
a broad spectrum of health 1.0 and health 2.0 skills.
Journal of medical Internet research, 19(1).
Vervier, L., Calero Valdez, A., and Ziefle, M. (2018).
"Should I Trust or Should I Go?" or What makes health-
related websites appear trustworthy?—An empirical
approach of perceived credibility of digital health infor-
mation and the impact of user diversity. In ICT4AWE,
pages 169–177.
Wilkowska, W. and Ziefle, M. (2012). Privacy and data
security in e-health: Requirements from the user’s per-
spective. Health informatics journal, 18(3):191–201.
Zeissig, E.-M., Lidynia, C., Vervier, L., Gadeib, A., and
Ziefle, M. (2017). Online privacy perceptions of older
adults. In International Conference on Human As-
pects of IT for the Aged Population, pages 181–200.
Springer.
“Attitude”- mHealth Apps and Users’ Insights: An Empirical Approach to Understand the Antecedents of Attitudes towards mHealth
Applications
221
