
Scaling-up of ICT Solutions in Active and Healthy Ageing through
Twinning Actions
Strahil Birov
a
, Christianne Lavin
b
and Veli Stroetmann
c
empirica Gesellschaft für Kommunikations- und Technologieforschung mbH, Oxfordstr. 2, Bonn, Germany
Keywords: ICT, Active and Healthy Ageing, Scaling-up Strategy, Digital Innovation, Twinnings.
Abstract: Despite an increase in life expectancy in today’s rapidly ageing society, unhealthy life years still make up a
big portion of a person’s life. Digital innovations in health and care services need to be scaled up to enable
more citizens to access and lead healthy, active and independent lives while ageing. Under the EU funded
ScaleAHA study, a twinning scheme was conducted to scale up ICT solutions in active and healthy ageing.
Forty-three organisations from thirteen European countries have successfully participated in financed
twinning actions ranging from knowledge exchange and training to full adoption and acquisition of an
innovative practice. Twinning topics included EHRs, ePrescription solutions, integrated health and social care
ICT service platforms, and homecare and telemonitoring solutions, among others. The twinning scheme was
a new concept that aimed to de-risk investment in innovative ICT solutions by financing small but concrete
ideas with high potential for replicability and scaling up. The twinnings led to benefits for the participating
organisations themselves as well as various stakeholders such as patients and their carers, healthcare providers
and regional authorities. This paper presents the results and lessons learnt from the twinning scheme and
recommendations to further refine future twinning actions.
1 INTRODUCTION
Scaling up digital innovations in health and care
services in Europe enables more EU citizens to lead
healthy, active and independent lives while ageing,
whilst improving the sustainability and efficiency of
health and social care systems and boosting and
improving the competitiveness of the markets for
innovative products and services. By scaling up
digital innovations, the EU Member States are
responding to the ageing challenge at both EU and
global level, while creating new opportunities for
businesses.
In order to successfully scale up digitally-enabled
innovative solutions, a comprehensive scaling-up
strategy at European level is needed. The European
Commission, supported by the European Innovation
Partnership on Active and Healthy Ageing (EIP on
AHA), has defined a five-step scaling-up strategy in
AHA by: building a database of innovative practices,
their viability assessment regarding scaling-up
potential, their classification for replication purposes,
a
https://orcid.org/0000-0002-4575-0492
b
https://orcid.org/0000-0001-8348-4642
c
https://orcid.org/0000-0001-8601-5307
the facilitation of appropriate partnerships, and
implementation of the innovative practices in other
regions and countries (European Commission, 2015).
Since its inception in 2010, the EIP on AHA has
shown considerable progress with regards to the first
three steps of the strategy. A repository of innovative
practices of the EIP on AHA contains more than 400
good practices across Europe. Each practice is
detailed and assessed via key performance indicators
(time for deployment, investment, maturity, available
evidence of outcomes, impact, transferability) in
order to help the more than 1,000 stakeholders of the
EIP on AHA identify collaboration opportunities.
With this foundation in place, the EIP on AHA is
in the process of implementing the good practices
through collaboration and partnership search.
Working together, stakeholders exchange knowledge
and share the experience of successful innovations to
facilitate their scaling up across Europe. One
important instrument promoted by the European
Commission to facilitate this step of the scaling-up
strategy is the use of twinning actions. In this paper,
222
Birov, S., Lavin, C. and Stroetmann, V.
Scaling-up of ICT Solutions in Active and Healthy Ageing through Twinning Actions.
DOI: 10.5220/0007722702220229
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 222-229
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

a twinning action or “twinning” refers to the transfer
of an innovative Information and Communication
Technology (ICT) solution (also referred to as the
“innovation” or “innovative practice” and can be a
product, service, methodology, or strategy) from one
region to one or more other regions.
The “Transfer of Innovation Twinning Support
Scheme” was a pilot scheme to support twinning
actions by partners of the EIP on AHA through the
reimbursement of expenses incurred in the transfer of
innovative practices. It was part of the EU-funded
“Support to scaling up of innovations in Active and
Healthy Ageing” (ScaleAHA) study (ScaleAHA
Consortium, 2016), which aimed to accelerate the
scaling-up of innovative approaches and practices in
Active and Healthy Ageing by fostering dedicated
mentoring activities and active knowledge exchange
among stakeholders of the EIP on AHA.
Two types of organisations could be involved in
the twinning scheme: an adopter organisation and an
originator organisation. The adopter is the
organisation that received the innovation, i.e.,
benefitted from the experience and know-how
developed by the originator organisation in a
particular field of intervention and aimed to deploy or
implement this innovation in their territory. The
originator is the organisation with the experience and
know-how in a particular field of intervention. It is
the organisation that transferred the innovation to the
adopter.
2 APPROACH
The twinning scheme of the ScaleAHA study limited
participation to organisations holding Reference Site
(RS) status as a result of the 2016 Call for Reference
Sites of the EIP on AHA. These “Reference Sites” are
highly inspirational ecosystems, delivering creative
and workable solutions that improve the lives and
health of older people through the collaboration of
different stakeholders. They are also able to give
evidence and concrete illustrations of the impact of
their approaches.
Applications to the scheme were possible through
a "joint request" submitted through a brief online
application form. It was filled in by the adopter and
originator organisations together, with details on the
requested twinning support, on the content of the
twinning action, (notably on which innovative
practice was planned to be transferred), and on the
level of commitment for implementing the innovative
practice within 2016-2018. The applications were
reviewed by an independent panel based on a set of
pre-defined award criteria.
Overall the twinning actions covered a wide range
of eHealth topics, which are relevant to current health
priorities. These included online health portals; ICT-
supported integration of health and social care
services; health and care needs assessment tools; ICT
tools supporting adherence to care plans; mHealth
systems; falls prevention; regional and national
Electronic Health Record (EHR) systems and
integration; ePrescription solutions; tele-mentoring
and virtual consultations; multi-disciplinary team and
care co-ordination; and age-friendly buildings,
among others. The twinning innovations were also
well-aligned with some topics related to the Digital
Single Market priorities on transforming health and
care (European Commission, 2018) such as health
data analytics (risk stratification tools, mobile
applications), citizen and patient empowerment
(online self-management hub, citizen access to data,
health data exchange and re-use, advanced platforms
and infrastructure, and prevention and patient-centred
care (innovations on telecare, home-monitoring, and
digital skills and staff training solutions, among
others).
The twinning organisations themselves were
responsible for managing and organising any activity
(e.g., study visits, translation work) needed to carry
out their twinning action and goals. The organisations
were also requested to report to the ScaleAHA study
team on the evolution of the innovative solution, the
motivation behind the healthcare problem that the
innovation addressed, any concrete plans on how the
innovation was to be transferred, the progress of the
twinning action, barriers and success factors
experienced, any possible future co-development,
benefits and new opportunities expected from the
twinning action, whether the twinning resulted in
implementation of the innovation in the adopter
region, and any other outcomes that resulted from the
twinning action. These reports were submitted twice
in the form of one interim and one final report.
The twinning scheme provided financial support
to cover the travel and accommodation of experts and
other expenses incurred by hosting meetings (such as
transport within the region). It did not cover fees for
professional services (consulting, advisory services,
moderation services etc.) and did not include the
acquisition of products and services from third
parties. The total maximum amount that could be
claimed was capped at € 5,000 for each twinning
action, irrespective of the number of adopter
organisations involved in the respective twinning.
Scaling-up of ICT Solutions in Active and Healthy Ageing through Twinning Actions
223
3 RESULTS
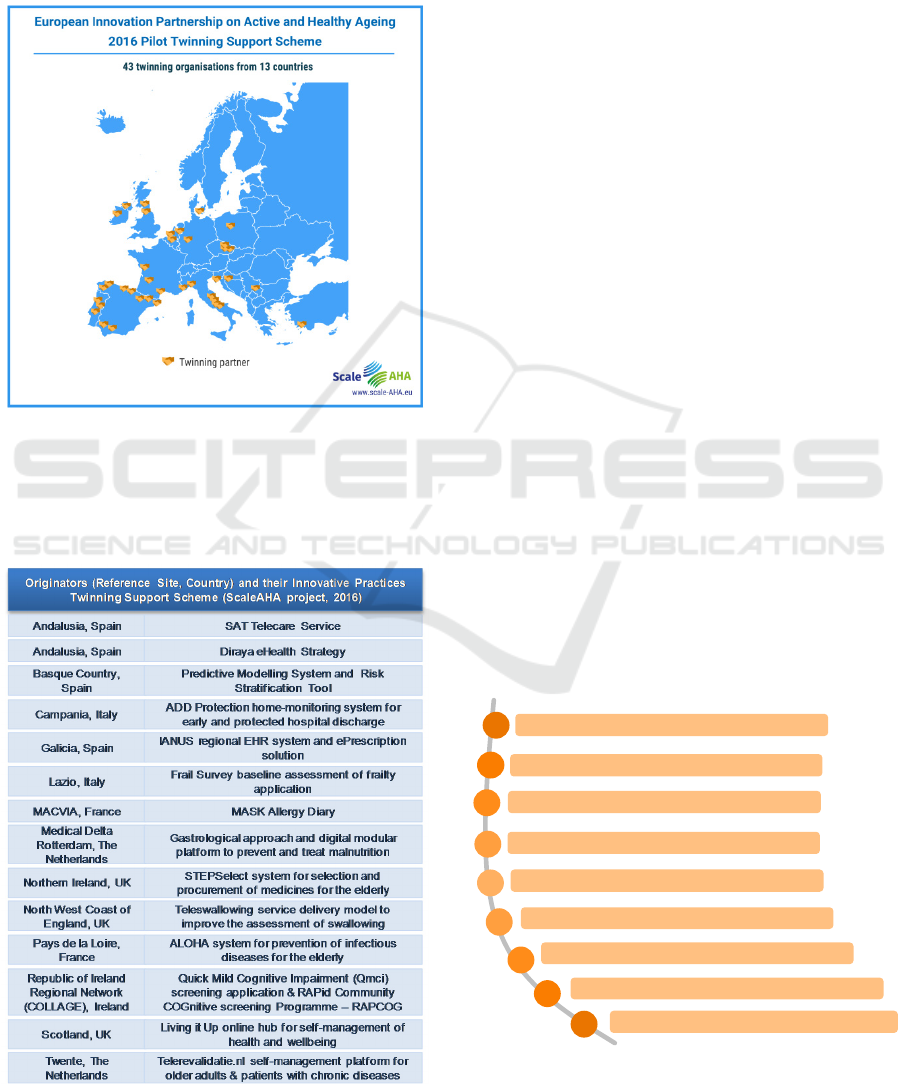
Twenty twinning proposals were accepted into the
twinning scheme, composed of 43 twinning
organisations from 26 Reference Sites in 13 countries
across Europe (Figure 1).
Figure 1: A total of 43 twinning organisations from 26
Reference Sites in 13 countries were accepted in the
ScaleAHA Twinning Support Scheme.
Table 1: Overview of innovative practices accepted in the
twinning scheme, and their respective originators.
Fourteen innovative practices were accepted in
the twinning scheme (Table 1).
The ScaleAHA study team collected and analysed
the reports on the twinnings submitted by the
originator and adopter organisations. The results of
these analyses are found in the next sub-sections.
3.1 Barriers and Success Factors to
Scaling up Innovation in AHA
The barriers and success factors to scaling up
innovation in AHA were identified and collected
based on the twinning experiences in order to present
the key elements that hampered or enabled a
smoother implementation of the innovative practice.
A lack of cooperative knowledge exchange
between professionals resulted in a delay in the
adoption of new practices, for instance, in Northern
Ireland, where clinicians initially feared that they
would lose their clinical freedom when using a new
system. There were also difficulties in convincing
stakeholders of the effectiveness of the new care
pathways, which thereby slowed down the
organisational change process. In some cases, the
implementation of a new system required clinicians
to first participate in educational programs and
training, leading to time and effort-related barriers. It
has been found to be challenging to address the target
group, i.e., present innovative eHealth systems to
those aged 80 years and above. Poor interoperability
among different health information systems and
fragmentation of software applications among
regions not only caused delays in adopting the
innovation but also caused an increase in costs related
to implementation. Technical barriers were also an
Figure 2: Overview of identified barriers to scaling up
innovation in AHA.
Lack of organisational structure
Lack of interdisciplinary communication and cooperation
Lack of interoperability and system integration
Time and effort related barriers
Financial and reimbursement problems
Resistance to change / Scepticism about effectiveness
Lack of awareness among professionals and patients
Technical barriers (infrastructure, connectivity)
Low digital literacy / Addressing the target group
Barriers to scaling up innovation in AHA
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
224

issue in several regions, in which poor internet
connectivity and multiple system crashes caused
discomfort in the users, which in turn delayed user
acceptance of the innovation.
Identifying and analysing the current state of
research in a particular target topic as well as
developing a clear vision on the use and benefits of a
new product were found to be useful initial steps in
implementing an innovative practice. Some of the
innovations were implemented quickly because they
fell in line with national strategies, guidelines and
health plans. In Andalusia and Scotland, continuous
political support helped overcome challenges in the
implementation of innovative electronic health
practices. Training and education of staff as well as
user experience design and acceptability led to more
efficient and widespread usage of the innovation.
User acceptance was particular important for
successful innovation and deployment and was
achieved by placing a focus on outcomes that were
important to the users. In Twente, the developers of
the Telerevalidatie.nl online portal supporting
rehabilitation at home were closely collaborating with
the target group, thus being able to adopt a user-
friendly and highly accepted digital solution.
Similarly, while developing the Andalusian EHR,
both technicians and the health workforce were
involved in the design and successful implementation
of the system. Financial incentives were identified to
be catalysts for change, for example, in helping
motivate doctors actively participate with other
Figure 3: Overview of identified drivers and success factors
to scaling up innovation in AHA.
stakeholders in introducing new treatment pathways.
Overall, networking, partnerships and collaboration
also played a substantial role.
More specific examples on the identified success
factors and barriers to scaling up innovation in AHA
as experienced by specific twinning organisations are
found in the ScaleAHA Final Study Report (empirica,
2017).
3.2 Twinning Archetypes and
Experiences
In terms of scaling-up scope, the twinnings can be
grouped into five archetypes: Knowledge exchange
and training, Adaptation, Partial adoption, Full
adoption, and Acquisition (described in Table 2).
Table 2: Twinning archetypes and corresponding number of
twinning actions.
The Knowledge exchange phase was usually
achieved within 3 months, and for many cases partial
adoption of the innovative practice was achieved after
6 months. Full acquisition of the innovative practice
took longer than 6 months since a pilot phase of at
least 12 months was usually required in order to study
the usability and adaptability of the ICT tools (e.g.,
assessing potential clinical effect, measuring
adherence to treatment, measuring user’s
satisfaction).
Examples of steps done within 6 months that led
to the implementation of the innovation include:
Organising various meetings for knowledge
transfer such as analysing the situation of the
Clear vision and strong political commitment
Previous research and piloting
Addressing current healthcare needs and embedding the new
system into present healthcare policies
Public and private partnerships
New business models and innovations
Product development in close collaboration with the end-users
User experience design, user acceptance
Local services, integration of the new solution into
the existing environment
Faster benefit realisation of the innovative practices
Marketing and business communication
Funding, financial incentives and investments
Networking and collaboration
Success factors to scaling up innovation in AHA
Training and education of staff
A mature innovation is being adopted by
adjusting it to local conditions (e.g. translation
into local language)
Elements or aspects of the innovation
(product, service, methodology, strategy) are
being implemented using locally available
infrastructure
The innovation (product, service,
methodology, strategy) is being implemented
in its full scope by using local infrastructure
i.e. the innovation is transferred and managed
fully by the adopter
The innovation is being implemented in its full
scope by using the originator’s infrastructure
(paid for or free of charge), i.e. the originator
still has primary ownership, but a license for
use is granted to and acquired by the adopter
Description
Focus on knowledge (know-how) exchange
and training, a central aspect of the innovation
are the required staff skills
1
8
6
4
1
Number
Adaptation
Partial
adoption
Full
adoption
Acquisition
Type
Knowledge
exchange &
training,
digital skills
Scaling-up of ICT Solutions in Active and Healthy Ageing through Twinning Actions
225

adopter site and analysing how to improve and
adjust the existing infrastructure;
Setting up working groups that analyse the
innovative solution and detect what changes or
improvements are necessary;
Translating content into the language of adopter
site (e.g., in mobile applications or portals);
Planning and designing future implementation
(e.g., creating roadmaps and study
methodologies on how to involve more citizens
and stakeholders); and
Finding sponsors for and implementing a small-
scale pilot e.g., at a hospital level.
The twinning organisations that successfully
implemented the innovative practice given the
twinning timeframe were able to do so due to the lack
of political or financial barriers even before the
twinning. In these cases, the organisations were able
to already focus on expanding their reach of potential
users (through publishing in magazines; using social
networks; using colourful, captivating icons in their
health platforms to attract a wider audience; etc.).
One of the success stories is the MASK Allergy
Diary twinning action, which was fully implemented
(full acquisition) initially by 10 adopter regions
during the twinning scheme (empirica, 2017)
followed by altogether 30 adopter regions (Bousquet,
2017). MASK Allergy Diary is a tool that enables
citizens to assess and control allergic rhinitis, and
supports pharmacists, physicians and specialists in
prescribing appropriate treatment and follow-ups.
Through the outreach of the adopter Reference Sites
(who aimed to recruit at least 50 elderly persons ≥65
years and at least 100 adults <65 years in more than
20 countries) the twinning allowed the originator to
study, compare, and analyse the differences in the
characteristics of rhinitis and asthma multimorbidity
among different age groups across different countries
(Bousquet, 2017). This twinning action not only
provided more citizens with access to a proven
allergy management tool, but also gave way to
multiple avenues of future research on rhinitis and
asthma that can be gained from the collected data.
Most of the twinnings led to an adoption of
elements of the innovation using the local
infrastructure (partial adoption). Partial adoption did
not necessarily mean an incomplete adoption. In
some cases, a partial adoption was preferred over a
full adoption since an efficient local infrastructure
was already in place in the adopter region. An
example of a success story of partial adoption is the
Andalusia-Zagreb twinning (empirica, 2017). The
adopter (Zagreb) participated in the twinning to find
digital solutions related to AHA that could be piloted
or implemented in the Zagreb RS. The twinning
enabled the Zagreb RS to co-develop workshops with
primary care physicians and ICT service providers in
order to find the best ways to implement elements of
the Diraya eHealth system (Regional Ministry of
Health Andalucia, 2016) to the Croatian healthcare
ecosystem. As a result, a set of modules was added to
the already existing health service of the adopter,
Zdravlje.net. The e-Consultation module was one of
the notable elements implemented through the
twinning. It fostered collaboration between cure and
care sectors and thus provides a multidimensional
approach to managing patients. Through this module,
each patient can receive recommendations for
managing a specific health issue based on the
multidisciplinary interaction of general practitioners
and hospital specialists. The number of citizens using
Zdravlje.net has been increasing and strongly
indicates possibilities to reach out to all current
inhabitants of Zagreb.
3.3 Benefits and New Opportunities
The adopter organisations have identified a number
of benefits and new opportunities resulting from the
adoption of digital innovations through the twinning
actions. The specific examples below are meant to
provide a better understanding of the benefits
experienced mostly by the adopter region. These
examples are not exhaustive.
Better Healthcare Service – for example, the
Basque Country Risk Stratification Tool (Orueta, et
al., 2013) enables patients with specific diseases to be
identified, selected, and precisely grouped, giving the
patient a more coordinated, proactive, and
personalised level of healthcare. The tool also collects
demographic, socioeconomic and clinical variables
from sources such as the Department of Health into
summarised, relevant information that supports
healthcare providers in their clinical decisions.
Timely Diagnosis and Better Screening – The
Quick Mild Cognitive Impairment (Qmci) screening
application (Collaboration on Ageing, 2016) has been
developed as a computerised application that reduced
paper work and data entry, and generated a more
accessible and flexible screening process. It will be
used to rapidly identify patients with Mild Cognitive
Impairment and dementia who can benefit from early
intervention.
Better Communication between Professional
and Patient/Patient's Family – The Andalusian
Telecare Service (SAT) (ASSDA, 2016) has enabled
easier and more personal communication between
doctor and patient due to its easily accessible setup: a
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
226

bracelet device that can be worn by the patient at
home and is connected to a device in the healthcare
centre that contains all patient information. The
service allowed patients to stay at their own homes,
which has also led to a bigger involvement of family
members in the patients’ care.
Improved Health Literacy – the ALOHA e-
Health platform (Gerontopole Pays de la Loire, 2016)
provides information on vaccination, nutrition, and
controlled use of antibiotics for the senior population.
Improving the patients’ awareness on such health
topics can lead to better participation in their medical
plans.
Better Resource Allocation – adopting a
transparent medicines procurement strategy using the
StepSelect system (Scott, et al., 2010) prevents the
dispensation of unnecessary medicines, which
therefore leads to cost savings that could be used to
further improve the health system.
Collection and Evaluation of Data that is by far
still Unavailable in the adopter site – the FrailSurvey
mobile app (University of Rome, 2016) enables the
collection of data and the subsequent evaluation of
the prevalence of frailty in the region. This was
beneficial for the adopter region (Porto), in which
there had not yet been data on frailty prevalence. The
possibility of including frailty status in the patient
care model was also explored.
Other benefits and new opportunities included
improved national sustainability due to massive cost
savings; reduced healthcare visits; development of
healthcare services for complex patients; new job
opportunities or roles for health professionals; patient
empowerment; the creation of new businesses,
business models and new areas of research and
development; and stronger relationships between the
Reference Sites and the possibility of future impactful
collaborations.
In some cases unforeseen benefits or “spill-over
effects” were observed. These are events that were
“inspired” by the twinning action, although not
initially planned. For example, one twinning action
involving the adoption of a telecare service had such
a positive effect on the adopter organisation’s team
that the adopters were inspired to develop another
type of service - a local call centre directed at solving
issues among the younger population. Some
twinnings also led to calls for developing other
solutions that would support the implementation of
the organisator’s innovation into the adopter region.
One of the twinnings resulted to not only in a transfer
of the innovative practice from the originator to the
adopter site but also from the adopter to the originator
site.
Furthermore, some of the twinning organisations
participated as both originator and adopter in separate
twinning actions. They reported benefits for the
originator as well, such as having an improved
internal communication, local coordination and
networking; receiving external positive feedback as
an incentive; and being able to update knowledge and
documentation of their innovative practice.
4 SUMMARY AND
RECOMMENDATIONS
Overcoming implementation barriers and leveraging
success factors for scaling up drives innovativeness in
active and healthy ageing. ScaleAHA has taken stock
of and analysed key barriers and success factors for
scaling-up of healthcare solutions in Europe. Some
barriers faced during the twinning scheme were
technical differences in infrastructure e.g., internet
access, lack of interoperability and system
integration, low digital literacy of the target group,
financial and reimbursement problems, and lack of
awareness among professionals and patients. Among
the key success factors are strong political
commitment; utilising existing networks,
partnerships and collaborations; putting the user in
the centre of the development and the overall process
to ensure acceptance; leveraging public and private
partnerships and funding mechanisms; disseminating
the benefits of the innovations; and providing
appropriate training and education to staff.
The twinnings have given rise to a number of
benefits and new opportunities resulting from the
adoption or planned implementation of the
innovation, not only for the adopter but also for the
originator. Each twinning has accomplished different
implementation steps regardless of their archetype
within the project timeframe. For many cases, a
partial adoption has been achieved after 6 months,
which generally involved organising various
meetings for knowledge transfer, creating relevant
working groups and multidisciplinary teams,
translation of ICT tools into the language of the
adopter site, and finding sponsors or even beginning
the necessary pilot phase.
Examples of lessons learnt that facilitated the
twinning actions included establishing a clear
twinning plan and identifying adopter prerequisites
early on in the timeframe; creating pilot projects to
address areas of improvement in the adopter region;
and creating more joint activities and training
sessions to enable knowledge acquisition not just for
Scaling-up of ICT Solutions in Active and Healthy Ageing through Twinning Actions
227

the adopter region but also for the originator region.
The different twinning archetypes required different
budget and financing but overall there was an own
budget of 1 million EUR invested by the adopters.
Recommendations provided by the twinning
organisations in order to further refine the
management of future twinning actions include
extending the twinning timeframe, also considering
the schedules of the different staff involved in the
twinning; making all necessary templates for
reporting available well in advance; keeping the
overall process simple (application, reporting, etc.);
increasing the twinning budget in order to extend the
scope of activities; and extending the budget to cover
other expenses such as staff participation,
development and implementation costs.
Furthermore, the following observations should
also be considered for future twinnings:
The twinning scheme should have a dedicated
online presence, which includes a list of ongoing
twinnings and regular news about their progress,
as well as information about any upcoming calls;
Provide evidence of impact and communicate the
benefits from twinning actions;
Launch Calls for Twinnings based on current and
upcoming EC priorities. Upcoming twinning
calls may be used strategically to stimulate areas
which are of priority to the EC or areas which are
underfunded but promise high impact, such as
the priority health areas described in the
Organisation for Economic Co-operation and
Development (OECD) Health at a Glance:
Europe reports (OECD/EU, 2018). Such
selective funding will allow to target digital
innovations more effectively and to close
existing gaps.
Twinnings should be placed in future European
Union funding programmes. By placing
particular requirements in the calls related to
twinning actions, the EC can further stimulate the
scheme; and
The impact of the twinnings should be captured
in a uniform way. The described twinning
scheme has delivered evidence of what works
well and can provide high impact. This evidence
was highlighted by the establishment of a clear
commitment between the twinning organisations
backed up by political support and additional
budget that was secured from local funds. The
impact of twinnings can be captured more
efficiently if assessed with a uniform impact
assessment tool.
5 CONCLUSIONS
Overall the twinning scheme carried out by the
ScaleAHA study was a new concept that aimed to de-
risk investment in digital innovative ICT solutions by
financing small but concrete ideas with high potential
for replicability and scaling up. The scheme was an
excellent instrument for targeting barriers in line with
current Digital Single Market health and care
priorities and providing digital solutions that can be
applied across Europe. Twinnings provide
inspirational organisations and ecosystems with
opportunities to learn from each other and deploy and
scale up their solutions to other regions. The twinning
actions also served as a stepping stone for further
commitment among regions to continue working
together and ensure the implementation of the
solution even after the given twinning timeframe. The
recommendations listed above were based on the
twinning experiences in the ScaleAHA study to
further refine possible future twinning actions.
Although the ScaleAHA study focused on ICT
solutions for active and health ageing, the twinning
scheme itself is replicable and can be deployed for
various other settings. Following the ScaleAHA
twinnings, the European Commission has encouraged
their use in other initiatives, including the EU project
WE4AHA (WE4AHA consortium, 2019), as well as
two new EU projects launched in January 2019.
ACKNOWLEDGEMENTS
This paper is based on the ScaleAHA study, which
was commissioned by DG Communications,
Networks Content and Technology of the European
Commission. Their support is gratefully
acknowledged.
We thank all colleagues from the ‘eHealth, Well-
being and Ageing’ Unit for their kind encouragement
and guidance, in particular, to Mr. Bruno Alves and
Mr. Arnaud Senn, for their great contributions,
enthusiasm and support.
We also thank all twinning partners for their
dedication and kind support.
REFERENCES
ASSDA, 2016. Andalusian Telecare Service. [Online].
Available at: https://ec.europa.eu/eip/ageing/reposi
tory/andalusian-telecare-service_en. [Accessed 17 12
2018].
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
228

Bousquet, J., 2017. Transfer of innovation on allergic
rhinitis and asthma multimorbidity in the elderly
(MACVIA-ARIA) - EIP on AHA Twinning Reference
Site (GARD research demonstration project), s.l.: John
Wiley and Sons Ltd..
Collaboration on Ageing, 2016. RAPid Community
COGnitive screening programme. [Online]. Available
at: https://ec.europa.eu/eip/ageing/repository/rapid-
community-cognitive-screening-programme_en.
[Accessed 17 December 2018].
empirica, 2017. Study on support to scaling-up of
innovations in Active and Healthy Ageing. [Online].
Available at: http://www.scale-aha.eu/fileadmin/
scaleaha/documents/scaleaha_d5.4_finalstudyreport.pd
f. [Accessed 13 December 2018].
European Commission, 2015. European Scaling-Up
Strategy in Active and Healthy Ageing. Luxembourg:
Publications Office of the EU.
European Commission, 2018. Transformation of Health
and Care in the Digital Single Market. COM/2018/233
Gerontopole Pays de la Loire, 2016. ALOHA, the Active and
Healthy Ageing Academy. [Online]. Available
at: https://ec.europa.eu/eip/ageing/repository/aloha-
active-and-healthy-ageing-academy_en. [Accessed 14
December 2018].
OECD/EU, 2018. Health at a Glance: Europe 2018: State
of Health in the EU Cycle, Paris: OECD Publishing.
Orueta, J. et al., 2013. Predictive risk modelling in the
Spanish population: a cross-sectional study, s.l.: BMC
Health Services Research.
Regional Ministry of Health Andalucia, 2016. Andalusian
eHealth Strategy & System (DIRAYA). [Online]
Available at: https://ec.europa.eu/eip/ageing/repo
sitory/andalusian-ehealth-strategy-system-diraya_en.
[Accessed 18 February 2019].
ScaleAHA Consortium, 2016. ScaleAHA "Support to
scaling up of solutions in Active and Healthy Ageing".
[Online]. Available at: http://www.scale-aha.eu/
home.html. [Accessed 04 December 2018].
Scott, M., McElnay, J. & Janknegt, R., 2010. Safe
Therapeutic Economic Pharmaceutical Selection
(STEPSelect): development, introduction and use in
Northern Ireland, s.l.: EJHP Practice
University of Rome, 2016. About the Baseline Assessment
of Frailty application. [Online]. Available at:
https:// ec.europa.eu/eip/ageing/repository/baseline-
assessment-frailty-application_en. [Accessed 18
December 2018].
WE4AHA consortium, 2019. WE4AHA. [Online].
Available at: https://cordis.europa.eu/project/rcn/2113
72/en. [Accessed 4 January 2019].
Scaling-up of ICT Solutions in Active and Healthy Ageing through Twinning Actions
229
